
Abstract
The goal was to examine gender differences of patient characteristics and outcome after cartilage repair based on a collective of nearly 5,000 patients. Patient characteristics, accompanying therapies, and outcome (Knee Injury and Osteoarthritis Outcome Score [KOOS], reoperations, patient satisfaction) of 4,986 patients of the German cartilage register DGOU were assessed by t test for possible gender differences. P values <0.05 were considered statistically significant. Women were older than men (38.07 ± 12.54 vs. 26.94 ± 12.394 years, P = 0.002), more often preoperated (0.30 ± 0.63 vs. 0.24 ± 0.55, P = 0.001), and had a longer symptom duration (25.22 ± 41.20 vs. 20.67 ± 35.32 months, P < 0.001). Men had greater mean leg axis malalignment than women (3.24° ± 3.26° vs. 2.67° ± 3.06°, P < 0.001), less favorable meniscal status (P = 0.001), worse defect stage (P = 0.006), and a more severely damaged corresponding articular surface (P = 0.042). At baseline (59.84 ± 17.49 vs. 52.10 ± 17.77, P < 0.001), after 6 months (72.83 ± 15.56 vs. 66.56 ± 17.66, P < 0.001), after 12 months (77.88 ± 15.95 vs. 73.07 ± 18.12, P < 0.001), and after 24 months (79.311 ± 15.94 vs. 74.39 ± 18.81, P < 0.001), men had better absolute KOOS values, but women had better relative KOOS increases 6 months (14.59 ± 17.31 vs. 12.49 ± 16.3, P = 0.005) as well as 12 months postoperatively (20.27 ± 18.6 vs. 17.34 ± 17.79, P = 0.001) compared with preoperatively, although 12 and 24 months postoperatively they were subjectively less satisfied with the outcome (P < 0.001) and had a higher reintervention rate at 24 months (0.17 ± 0.38 vs. 0.12 ± 0.33, P = 0.008). In summary, the present work shows specific gender differences in terms of patient characteristics, defect etiology, defect localization, concomitant therapy, and the choice of cartilage repair procedure. Unexpectedly, contrary to the established scientific opinion, it could be demonstrated that women show relatively better postoperative KOOS increases, despite a higher revision rate and higher subjective dissatisfaction.
Introduction
Patients’ gender plays a relevant role in orthopedic surgery. Especially in the field of cartilage repair, gender differences are under continuous investigation. The first study on gender differences in cartilage mass was in 1999, showing males having greater femoral and retropatellar cartilage volumes than females (adjusted for age, height, weight, and bone volume) and this difference even increases with age. 1 Many subsequent studies could prove women even having a greater decrease in cartilage volume of all compartments of the knee over time compared with men.2-4 This is probably a reasonable explanation for the higher risk for prevalence and increased rates of knee osteoarthritis (OA) incidence in women compared with men. Moreover, a less severe OA in the knee in men compared with women is observed with an increasing difference in age > 55 years. 5 This finding might be associated with the effects of menopause on the cartilage. Estrogen influence on the cartilage was shown by Ushiyama et al., 6 who found 2 types of estrogen receptors on human articular chondrocytes. Furthermore Jenei-Lanzl et al. 7 proved the influence of estrogen membrane receptors on chondrocytes and found a suppression of chondrogenesis via those GPR-30 membrane receptors. Even though estrogen may have a modulating effect on the cartilage, the effects of sex hormones and growth factors on the cartilage are poorly understood yet. 8
The role of quadriceps strength on the cartilage and functional outcome after orthopedic interventions has already been under investigation,9-11 but also concerning that influence, gender differences have been found: Quadriceps weakness only increased cartilage defects of the patellofemoral and tibiofemoral joint in women but not in men.12,13 Regarding patient’s outcome, some studies could show worse preoperative and postoperative outcome values in women undergoing cartilage surgery.14-16 A small study of 112 patients also revealed gender differences in the outcome after cartilage repair, showing that women achieve worse absolute postoperative outcome scores, yet relativized after standardizing patient characteristics by a matched pair analysis. 4 The same study group also showed gender differences in lesion location.
However scientific literature is lacking evidence based on big cohorts proving gender differences regarding patient and defect characteristics, as well as outcome values in patients receiving cartilage repair surgery.
Methods
Data from the German Cartilage Registry (KnorpelRegister DGOU) were used for the present analysis. The KnorpelRegister DGOU is an observational, nationwide, and longitudinal multicenter registry of patients assigned for surgical treatment for cartilage defects of the knee and aims to determine real-life treatment patterns and clinical outcomes. The registry was initiated by the Working Group Clinical Tissue Regeneration of the German Society for Orthopaedics and Trauma (DGOU) in 2013. Since then, the number of sites has increased to 120. The registry is conducted in accordance with the Declaration of Helsinki and registered at germanctr.de (DRKS00005617) and the current study was approved by the Ethics Commission of the Medical Center, University of Freiburg: EK-FR 105/13_130795.
All patients aged 18 years and older that meet the following criteria are eligible to take part in the German Cartilage Registry: surgical treatment of cartilage defects of the knee, ankle, or hip joint at a participating site, signed written informed consent, and possession of a personal email address.
Until August 2019, 4,986 patients assigned for surgical treatment for cartilage defects of the knee had been included in the registry. For the present study, data from all patients were analyzed.
Data collection is performed using a web-based RDE System “RDE-Light,” which was developed by the Clinical Trials Unit (Freiburg) as an electronic data entry interface and data management system for clinical studies and other projects in clinical research. Data are collected paperless and directly on site via an internet browser. Forms are based on HTML- and PDF-format. RDE-Light is available in various languages and validated according to GAMP 5. Furthermore, it fulfills all requirements of Good Clinical Practice (GCP). Established security standards like cryptographic security protocols (SSL/TLS), user authentication protocols, and authorization concepts are applied.
After the patient signs the written informed consent, the investigator is allowed to register the patient to the database. Patient- and defect-specific parameters are reported by the treating physician at the time of surgery.
The German Cartilage Registry is supported by a grant from the “Oscar-Helene-Stiftung” and the “Deutsche Arthrosehilfe e.V.”
The baseline characteristic parameters (degree of varus, symptom duration, corresponding joint surface, defect size, defect stadium, age, body mass index [BMI], meniscus status, number of previous surgeries, defect localization, and defect etiology), type of cartilage treatment, outcome parameters (Knee Injury and Osteoarthritis Outcome Score [KOOS] total preoperatively and 6, 12, and 24 months postoperatively; delta KOOS pre/6 months, pre/12 months, pre/24 months; patients’ satisfaction 6, 12, and 24 months postoperatively; revisions 6, 12, and 24 months postoperatively), as well as accompanying surgeries were normally distributed, as assessed visually using Q-Q plots. In case of normal distribution, factors mentioned above were compared between the genders using unpaired t test. Paired values were analyzed using paired t test. P values <0.05 were considered statistically significant. SPSS statistics version 25 was used to analyze the data.
Results
Patient Selection
From January 2014 to August 2019 4,968 datasets were registered in the German Cartilage Registry (KnorpelRegister DGOU). All datasets were analyzed regarding gender differences regarding patient characteristics, accompanying surgeries and outcome. The values for males are always listed first (male vs. female).
Patient Characteristics
In comparison to men, women were older (36.94 ± 12.394 vs. 38.07 ± 12.54 years, P = 0.002), more often had a history of cartilage surgeries (0.24 ± 0.55 vs. 0.30 ± 0.63, P = 0.001), and presented with longer symptom duration (20.67 ± 35.32 vs. 25.22 ± 41.20 months, P < 0.001). Men, on the other hand, had greater mean leg axis malalignment (3.24° ± 3.26° vs. 2.67° ± 3.06°, P < 0.001), less favorable meniscal status (10.7% vs. 8.6% > 1/3 resected, P = 0.001), worse defect stage (60.4% vs. 56.3% stage IV, P = 0.006), more severely damaged corresponding articular surface (59.2% intact vs. 62.7% intact, P = 0.042), and higher mean BMI (26.73 ± 3.66 vs. 25.89 ± 4.52 kg/m2, P < 0.001) and body weight (87.78 ± 12.86 vs. 75.27 ± 13.85 kg, P < 0.001). In men, bigger defect sizes were also apparent, but the difference was not significant (356.34 ± 209.62 vs. 345.52 ± 205.33 mm, P = 0.084). There were no intersex differences in the number of previous surgeries on the joint (0.80 ± 1.13 vs. 0.81 ± 1.16, P = 0.753) or number of defects (1.21 ± 0.48 vs. 1.23 ± 0.49, P = 0.166). The patient characteristics are shown in Table 1 .
Patient Characteristics.
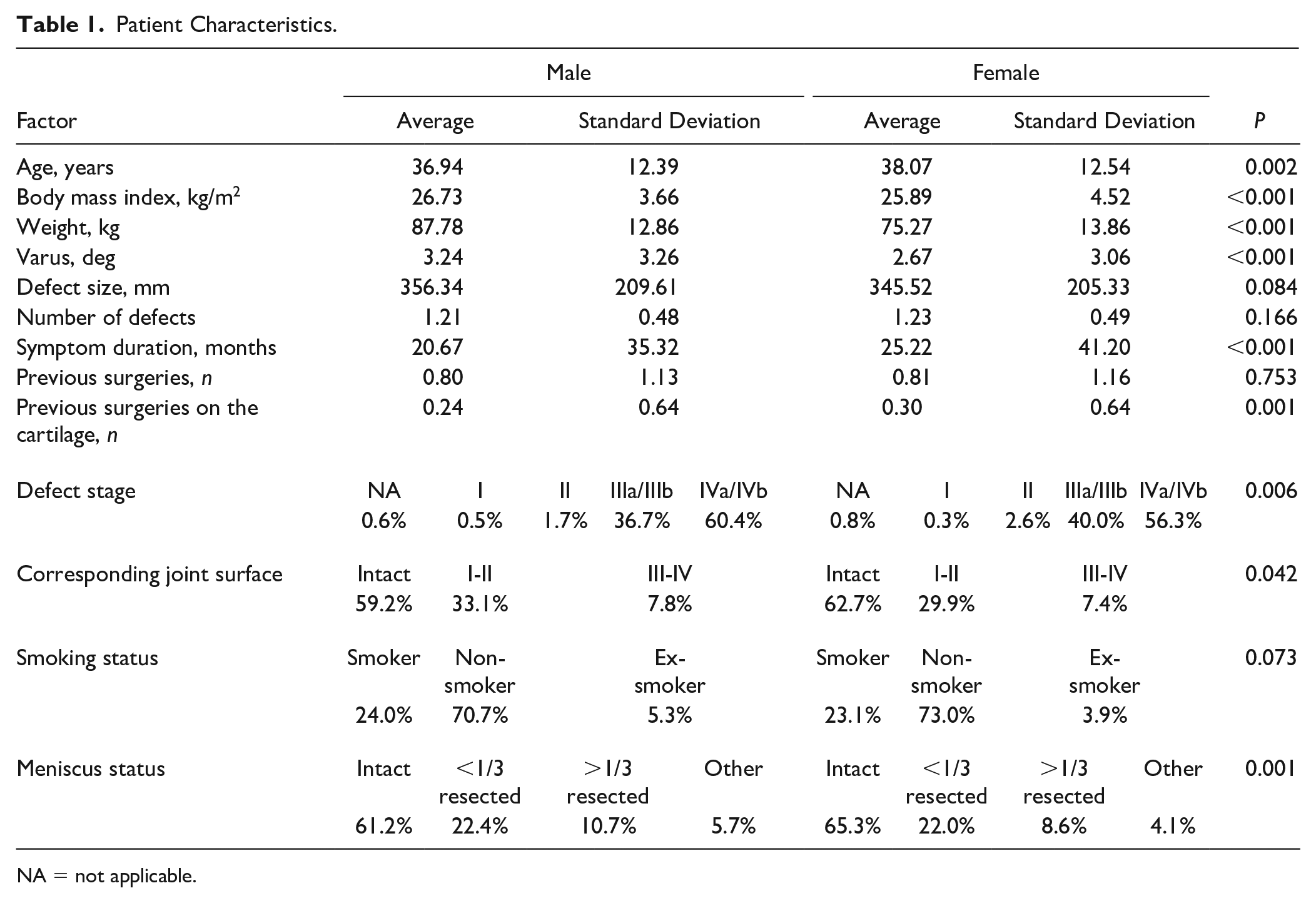
NA = not applicable.
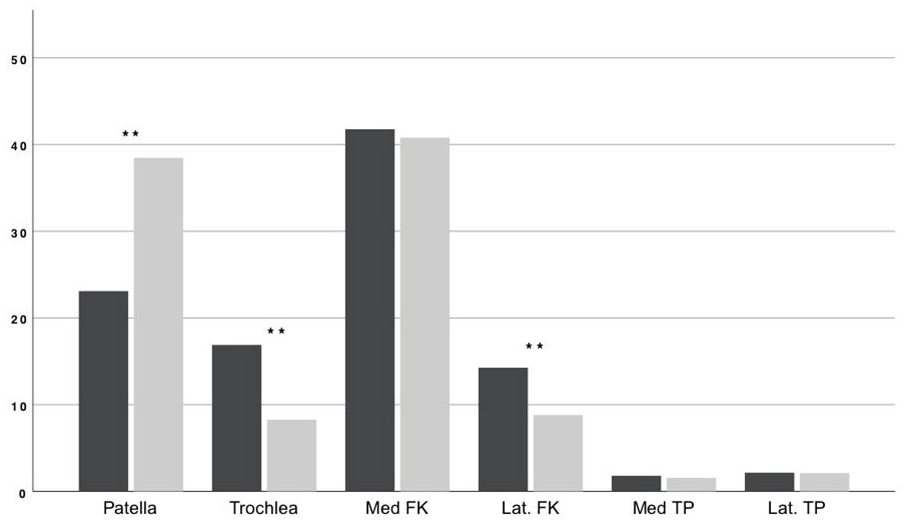
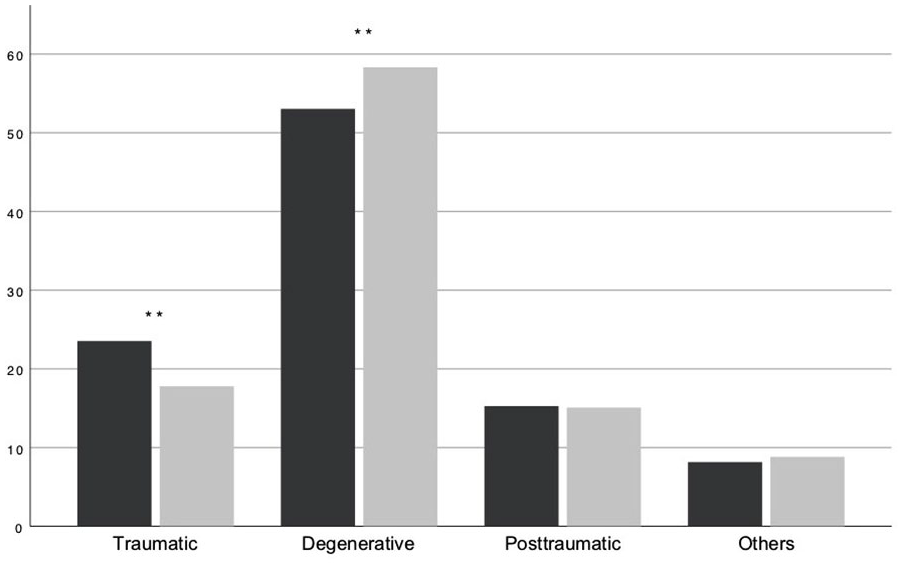
While degenerative cartilage defects (53.03% vs. 58.31%, P < 0.001) were more common in women, men were more likely to suffer traumatic defects (23.54% vs. 17.79%, P < 0.001) (see Fig. 1 ). In terms of defect localization, retropatellar defects (23.10% vs. 38.47%, P < 0.001) were more common in women, and trochlear defects (16.89% vs. 8.27%, P < 0.001) as well as defects of the lateral femoral condyle (14.27% vs. 8.81%, P < 0.001) were more common in men (see Fig. 2 ). There were no significant differences in the proportion of defects of the medial femoral condyle or the tibia plateau.
Defect etiology: Percentage of defect etiology in male (black) and female (gray) patients, ** means highly significant difference between genders with P < 0.001.
Defect location: Percentage of defects in male (black) and female (gray) patients, ** means highly significant difference between genders with P < 0.001.
Type of Cartilage Treatment
Gender differences also exist in regard to the choice of cartilage repair (see Fig. 3 ). The proportion of women treated with mBMS (matrix-augmented bone marrow stimulation) (5.04% vs. 6.68%, P = 0.045) is significantly bigger, whereas the number of men treated with ACT (autologous chondrocyte transplantation) with bone grafting (11.49% vs. 9.91%, P = 0.024) is greater. Even though the share of women treated with ACT is bigger and with BMS (bone marrow stimulation) (opposite to mBMS treatment) and ACT is smaller, there were no significant differences.
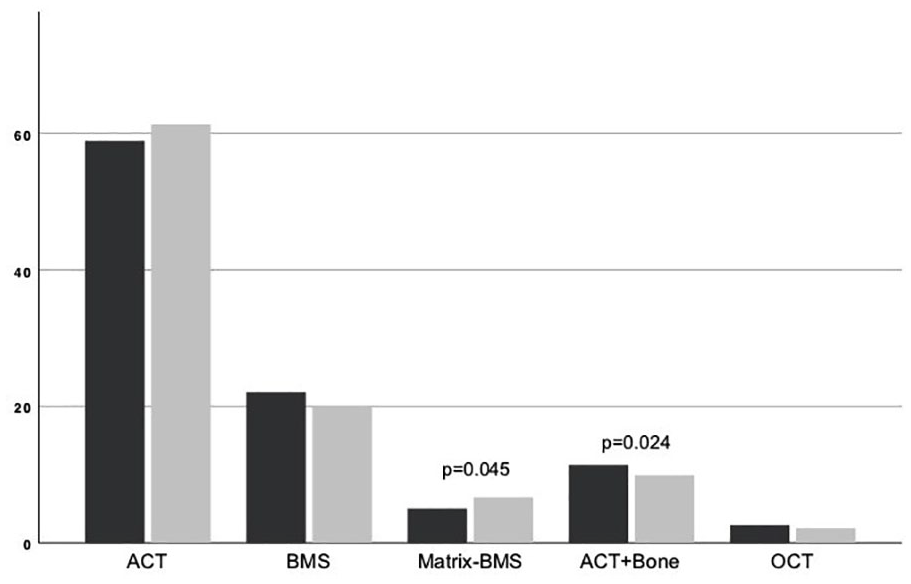
Type of cartilage treatment: Percentage of type of cartilage treatment in male (black) and female (gray) patients.
Accompanying Surgeries
In terms of surgeries accompanying cartilage treatment there are many gender differences (see Table 2 ). In women, bony (1.97% vs. 4.07%, P = 0.005) or of soft tissue (13.92% vs. 25.23%, P < 0.001) operations with the aim of patella stabilization are performed more frequently.
Accompanying Surgeries.
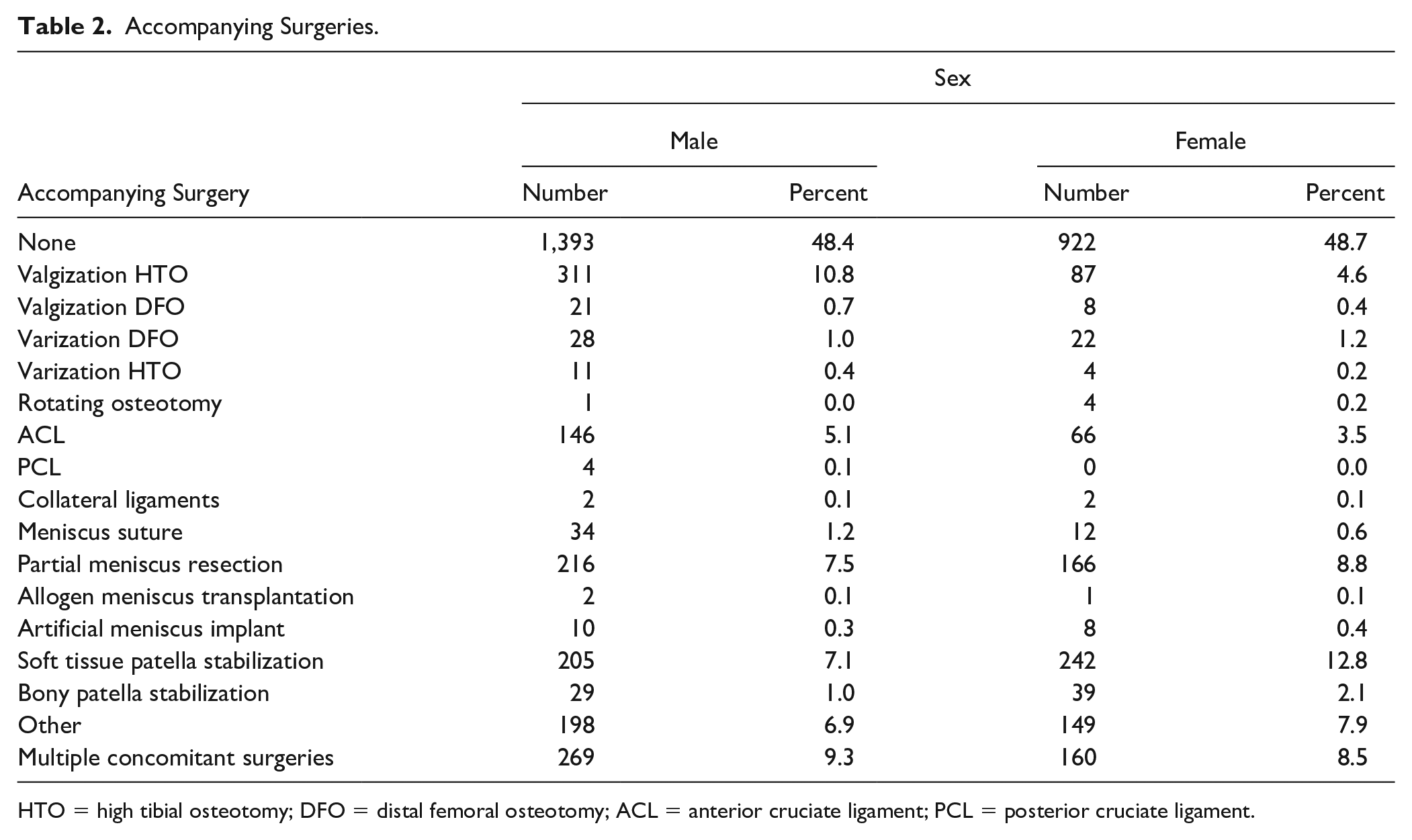
HTO = high tibial osteotomy; DFO = distal femoral osteotomy; ACL = anterior cruciate ligament; PCL = posterior cruciate ligament.
On the other hand, the proportion of valgization high tibial osteotomy (HTO) (21.11% vs. 9.07%, P < 0.001), meniscus sutures (2.31% vs. 1.25%, P = 0.004), as well as reconstructions of the anterior (9.91% vs. 6.88%, P = 0.007) and posterior (0.27% vs. 0.00%, P = 0.045) cruciate ligament is higher in men.
Outcome
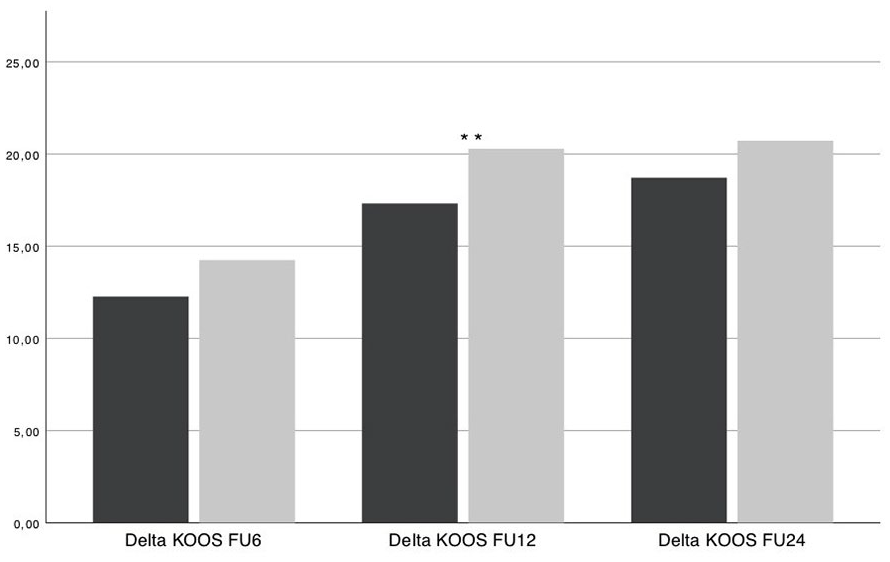
Preoperatively (59.84 ± 17.49 vs. 52.10 ± 17.77, P < 0.001) and 6 months (72.83 ± 15.56 vs. 66.56 ± 17.66, P < 0.001), 12 months (77.88 ± 15.95 vs. 73.07 ± 18.12, P < 0.001), as well as 24 months (79.311 ± 15.94 vs. 74.39 ± 18.81, P < 0.001) postoperatively, men had better absolute KOOS values (see Fig. 4 ), but women had better relative KOOS increases 6 months (12.49 ± 16.30 vs. 14.59 ± 17.31, P = 0.005) as well as 12 months postoperatively (17.34 ± 17.79 vs. 20.27 ± 18.61, P = 0.001) compared with preoperatively (see Fig. 5 ). KOOS significantly increased in men from before surgery to the 6-month follow-up (P > 0.001), as well as between 6 and 12 months after surgery (P < 0.001) as well as between 12 and 24 months after surgery (P = 0.006). In women, KOOS only increased highly significant (P < 0.001) between preoperative and 6 months and between 6- and 12-month follow-up. But there was no significant increase between the 12- and 24-month follow-up (P = 0.271).
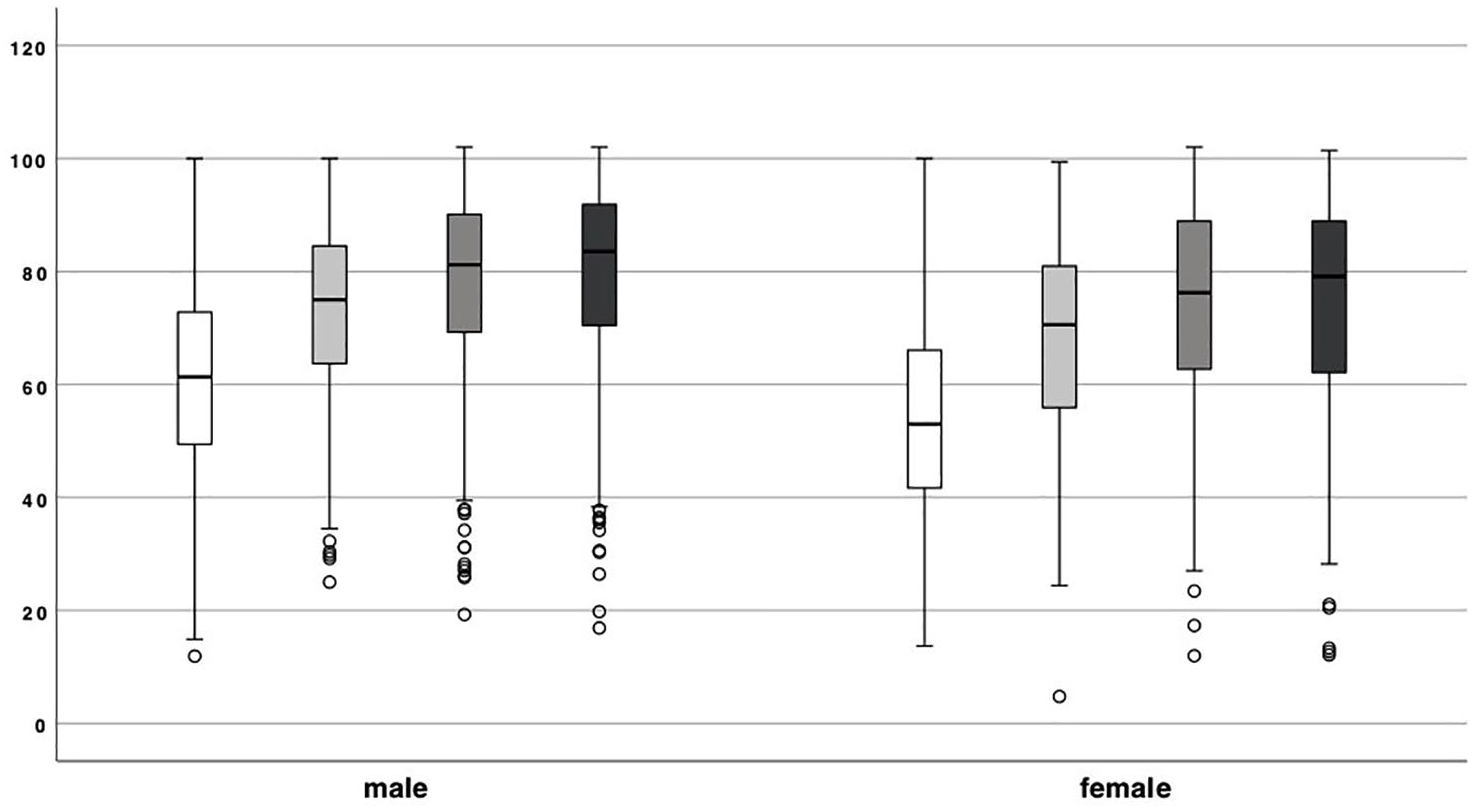
Knee Injury and Osteoarthritis Outcome Score (KOOS) values 0 (white), 6 (light gray), 12 (dark gray), and 24 (black) months after surgery. Pre- (59.84 ± 17.49 vs. 52.10 ± 17.77, P < 0.001) and 6 months (72.83 ± 15.56 vs. 66.56 ± 17.66, P < 0.001), 12 months (77.88 ± 15.95 vs. 73.07 ± 18.12, P < 0.001), and 24 months (79.311 ± 15.94 vs. 74.39 ± 18.81, P < 0.001) postoperatively, men had better absolute KOOS values than women. KOOS significantly increased in men from before surgery to the 6-month follow-up (P > 0.001), as well as between 6 and 12 months after surgery (P < 0.001) as well as between 12 and 24 months after surgery (P = 0.006). In women, KOOS only increased highly significant (P < 0.001) between preoperative and 6 months and between 6- and 12-month follow-up. There was, however, no significant increase between the 12- and 24-month follow-up (P = 0.271). ** means highly significant difference with P < 0.001.
Change in Knee Injury and Osteoarthritis Outcome Score (delta KOOS) values at 6, 12, and 24 months postoperatively compared with before surgery. Women had better relative KOOS increases 6 months (12.49 ± 16.30 vs. 14.59 ± 17.31, P = 0.005) as well as 12 months postoperatively (17.34 ± 17.79 vs. 20.27 ± 18.61, P = 0.001) compared with preoperatively, ** means highly significant difference between genders with P < 0.001.
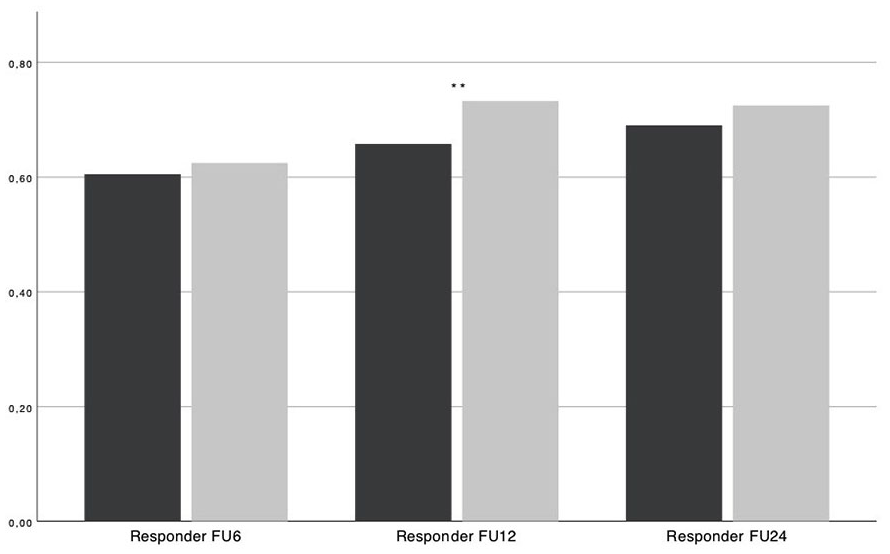
This relative increase in KOOS score is also reflected in KOOS responder rates. A patient is a “Responder” if the KOOS increase is ≥8 points compared with preoperatively. As shown in Figure 6 , women had higher responder rates 6 months (0.60 ± 0.49 vs. 0.62 ± 0.46, P = 0.208), 12 months (0.65 ± 0.477 vs. 0.72 ± 0.448, P = 0.001), and 24 months (0.68 ± 0.47 vs. 0.72 ± 0.50, P = 0.100) postoperatively compared with the preoperative values, although 12 and 24 months postoperatively, they were subjectively less satisfied with the outcome (P < 0.001) (see Table 3 ). Moreover, the satisfaction score (1 to 4; with 1 = not satisfied to 4 = very satisfied) dropped in women continuously over the follow-up time of 24 months, whereas it rose continuously in men. Although there were no significant differences in reoperation rates 6 and 12 months after the operation, 2 years postoperatively women underwent revision surgery significantly more often (0.12 ± 0.33 vs. 0.17 ± 0.37, P = 0.008) (see Fig. 7 ).
Responder rates 6, 12, and 24 months postoperatively compared with preoperatively in percent. A patient is a “Responder” if the Knee Injury and Osteoarthritis Outcome Score (KOOS) increase is ≥8 points compared with preoperatively. Male patients are visualized in black and females in gray. Women had higher responder rates 6 months (0.60 ± 0.49 vs. 0.62 ± 0.46, P = 0.208), 12 months (0.65 ± 0.477 vs. 0.72 ± 0.448, P = 0.001), and 24 months (0.68 ± 0.47 vs. 0.72 ± 0.50, P = 0.100) postoperatively compared with the preoperative values, ** means highly significant difference between genders with P < 0.001.
Patients’ Satisfaction a .
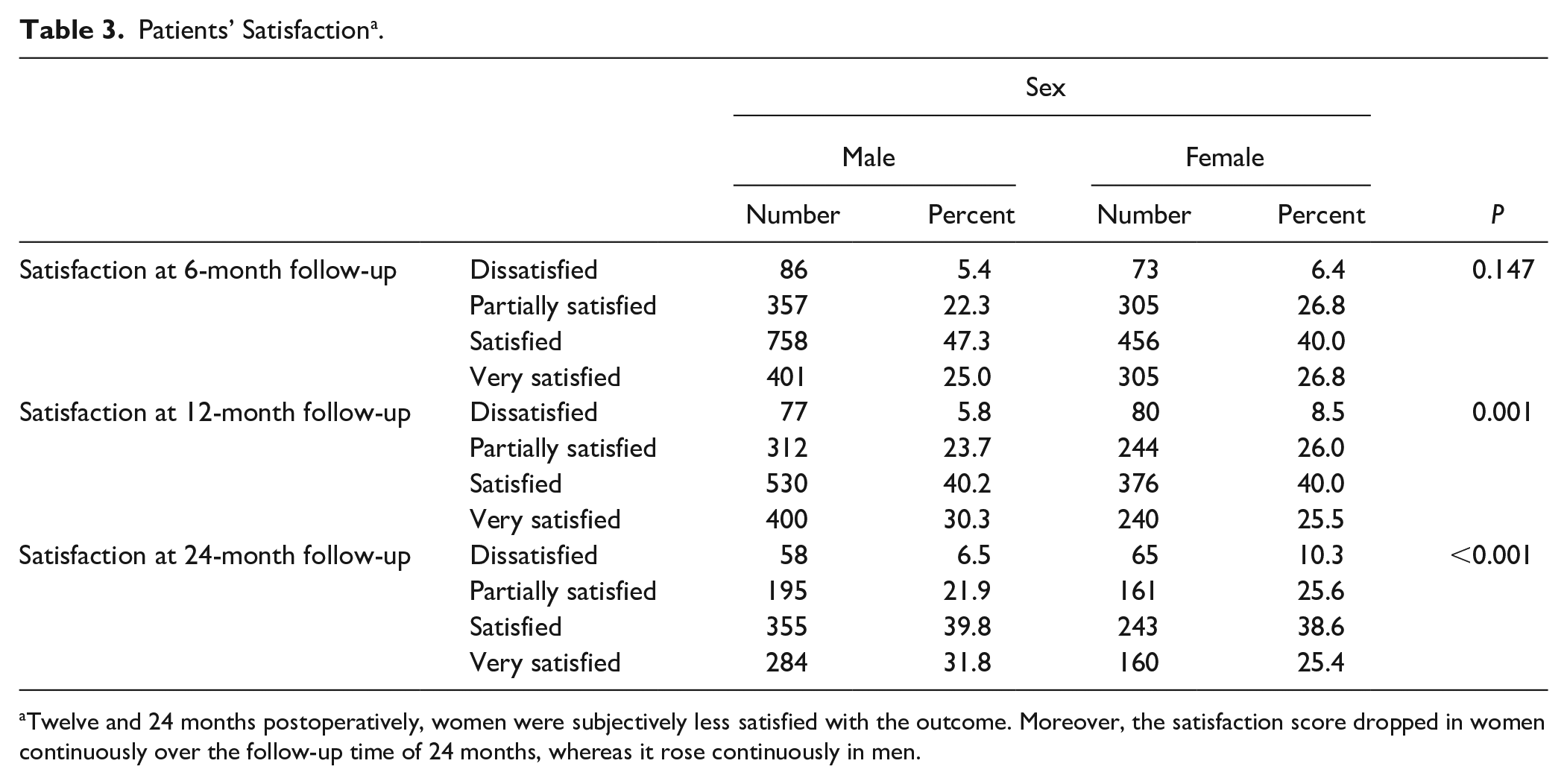
Twelve and 24 months postoperatively, women were subjectively less satisfied with the outcome. Moreover, the satisfaction score dropped in women continuously over the follow-up time of 24 months, whereas it rose continuously in men.
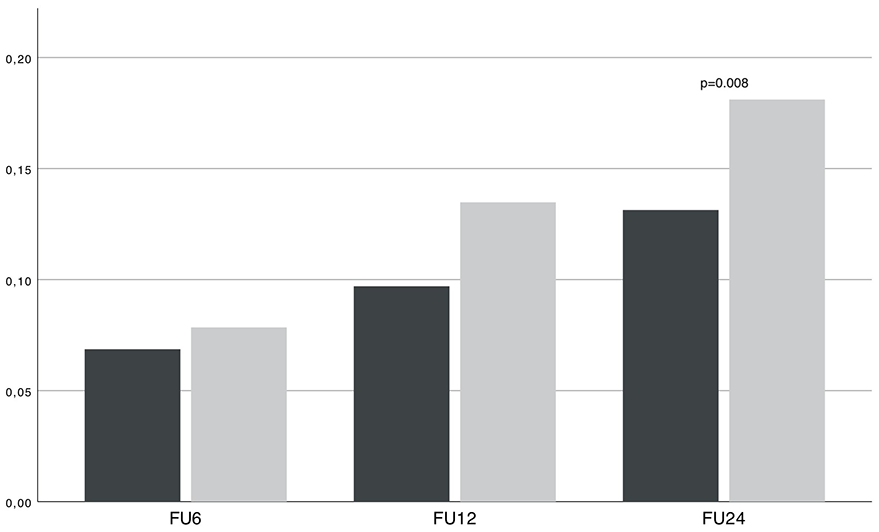
Reintervention rates 6, 12, and 24 months after surgery in male (black) and female (gray) patients. Whereas there were no significant differences in reoperation rates 6 and 12 months after the operation, 2 years postoperatively, women underwent revision surgery significantly more often (0.12 ± 0.33 vs. 0.17 ± 0.37, P = 0.008).
Discussion
The present study comprising 4,968 patients shows specific gender differences in terms of patient characteristics, defect etiology, defect localization, concomitant therapy, and the choice of cartilage repair procedure, as well as outcome scores.
Concerning defect location, patella defects occur significantly more frequent in women than in men in our study cohort. This finding has also been described by Filardo et al. 4 Reasonable explanations for that finding could be the lesser retropatellar cartilage volume with a higher decrease over time in women, 1 on one hand, and the fact that quadriceps weakness only increased cartilage defects of the patellofemoral joint in women but not in men,12,13 on the other hand. Women have a higher rate of patella defects; hence women are treated highly significantly more often with patella stabilization (bony and soft tissue) than men.
Men show higher rates of anterior cruciate ligament and posterior cruciate ligament reconstruction concomitant with cartilage surgery; hence traumatic lesions are more common in the significantly younger men ( Table 1 ), whereas degenerative lesions are more common in women ( Table 2 ). The latter might be a reasonable explanation for the higher rate of mBMS treatments in women.
Another interesting fact is, that even though the proportion of defects on the medial femoral condyle is equal in men and women, valgization tibia osteotomies are performed significantly less often in women.
Worse outcome in women after orthopedic surgery is well described not only for cartilage surgery17,18 but also for osteotomies19-21 and anterior cruciate ligament surgery.22-24 But women do not only score worse postoperatively; worse preoperative scores for women have been shown earlier.14-16 Even in a healthy population, women score worse in KOOS than men.25-27 It could have also been shown that worse preoperative PROMs (patient-reported outcome measures) result in worse postoperative PROMs. 28 In our study, contrary to the established scientific opinion, we could show that women only present worse absolute outcome KOOS values, but with better relative postoperative KOOS increases. Thus, women do not only excel through higher responder rates 6 and 24 months postoperatively compared with preoperative KOOS values but are also characterized by significantly higher KOOS increases 6 and 12 months postoperatively. Filardo et al. 4 also found that the worse absolute outcome in women must be considered complex and is relativized after standardizing of patients according to the mean score typical for the corresponding age and sex category in a healthy population. And also, in a study of Kreuz et al., 18 analyzing 52 patients after ACI (autologous chondrocyte implantation) regarding sex-dependent differences, it was on one hand shown that women had significantly worse outcome after ACI especially after ACI of the patellofemoral compartment, but on the other hand it should not be overlooked that women also had worse preoperative IKDC (International Knee Documentation Committee) and Lysholm scores with a consecutive approximately equal increase of the Lysholm score in patellofemoral cases and even a better increase in Lysholm and IKDC score in tibiofemoral cases.
Contrasting the better relative outcome in women shown in the present study was the lower satisfaction, which decreased in women over the follow-up time of 24 months, whereas it increased in men during follow-up. Questionable is whether the satisfaction has a stronger correlation with the absolute KOOS or the reoperation rate than with the relative KOOS increase: The latter being better in women and the former better in men implies that the worse satisfaction in women may be based on the worse absolute KOOS values and the higher reoperation rate.
It also needs to be taken into consideration that women generally report being more sensitive of their own health in self-assessed scores; in the World Health Survey with over 250,000 participants, women reported significantly poorer on all self-reported health indicators than men. 29 Moreover, self-assessed functional knee scores have many confounders, such as preoperative mental health, 30 for which gender bias on self-reports has been proven, specifically men underrating depressive symptoms. 31 A further reason for lower KOOS values in women pre- and postoperatively may be the significantly longer preoperative symptom duration and the significantly higher number on previous cartilage surgeries in women. Both factors could be determined as strong predictors for worse outcome in multiple studies.28,32,33 Despite these 2 worse preoperative factors, women result in higher KOOS increases.
Higher complications rates in cartilage surgery in women have already been shown28,32,34 and could be confirmed by our analysis showing higher revision rates in women 24 months after surgery (0.17 ± 0.377 vs. 0.12 ± 0.327, P = 0.008). This might be related to the lower satisfaction level in women, possibly causing more complaints to the operating surgeon, who in turn decides to perform an additional operation. But the higher reoperation rate could also be the reason for the lower satisfaction in women. Further investigations on the causes of the higher revision rates and lower satisfaction rates in women is needed.
Conclusion
In summary, the present study shows gender-specific differences not only in terms of patient characteristics, defect etiology, defect localization, concomitant therapy, and the choice of cartilage repair procedure, but also in the outcome. Unexpectedly, contrary to the established scientific opinion, it could be shown that women only show worse absolute outcome values, but better relative postoperative KOOS increases, despite a worse initial situation (more previous cartilage operations and longer symptom duration). Despite the greater increase in KOOS, women have higher revision rates and higher subjective dissatisfaction. Finally, when outcome is compared between genders delta PROM-values should be used instead of absolute PROM values.
Limitations
In addition to the unfortunately expected registry input errors on the doctor and patient side, only KOOS was examined in terms of PROMs. It would be desirable for follow-up work to also examine the influence of the patient’s sex on other PROMs.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.