
Abstract
Objective
To evaluate current evidence and results of cell-free scaffold techniques for knee chondral lesions.
Design
A systematic review was conducted on 3 medical electronic databases according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines, and the methodological quality was assessed with a modified Coleman Methodology Score. A meta-analysis was performed on the articles reporting results for visual analogue scale (VAS), Lysholm, and International Knee Documentation Committee (IKDC) scores. In order to investigate the clinical results improvement over time of cell-free cartilage scaffold implantation, all scores were reported and analyzed as improvement from basal scores at 1, 2, and ≥3 years’ follow-up.
Results
A total of 23 studies involving 521 patients were included in the qualitative data synthesis. The Coleman score showed an overall poor study quality with the majority of studies reporting results at short-/mid-term follow-up. Sixteen studies were included in the meta-analysis, showing a significant improvement from basal score at 1, 2, and ≥3 years’ follow-up. The improvement reached at 1 year remained stable up to the last follow-up for all scores.
Conclusions
The current literature suggests that cell-free scaffolds may provide good clinical short-/mid-term results; however, the low evidence of the published studies and their short mean follow-up demand further evidence before more definitive conclusions can be drawn on their real potential over time and on their advantages and disadvantages compared to the cell-based strategies for the treatment of cartilage lesions.
Introduction
Articular chondral lesions have always represented a challenging pathology leading to functional impairment, pain, and eventually the development of end-stage osteoarthritis. In the past decades, a variety of surgical techniques were developed aiming at restoring articular surface and preventing joint degeneration. Among these, regenerative scaffold-based procedures have emerged as a potential therapeutic option for the treatment of these kinds of lesions. 1
The rationale for using a scaffold is to have a temporary 3-dimensional (3D) structure of biodegradable polymers to allow the growth of living cells. 2 In this light, scaffolds have been introduced in the clinical practice to improve results previously achieved with autologous chondrocyte implantation (ACI), 3 while overcoming the drawback, like the periosteal overgrowth and the dedifferentiation into fibroblasts typical of 2D culture,4,5 and simplifying the procedure.2,6 ACI scaffold-based evolution (matrix-assisted autologous chondrocyte transplantation [MACT]), applied with various materials in different physical forms, 2 demonstrated equally good results in long-term follow-ups, while avoiding the complications reported for the first-generation ACI Nevertheless, MACT was still burdened by the need of a 2-step procedure and by the high costs of cell cultures. Moreover, MACT presented the same issues in terms of regulatory requirements due to the need for cell expansions. Therefore, in the past years both researchers and clinicians have been looking for solutions to overcome the aforementioned limitations and regenerate the articular surface. 6
In the past 15 years an increasing awareness of the role of scaffolds has grown: They are not considered just carrier system for cell delivery, but they also present an intrinsic ability to promote chondral or osteochondral regeneration by exploiting the self-regenerative potential of the body.6-8 Accordingly, chondral scaffolds started to be used alone or as augmentation for microfractures, providing a substrate to take advantage of bone marrow mesenchymal cells obtained through the perforation of the subchondral bone plate. Microfractures technique was demonstrated to provide good results at short-term follow-up, but a subsequent worsening of clinical score has been shown at mid-term follow-up. Consequently, the mayor concern about cell-free procedures regards the durability over time of the obtained results Thus, it would be important to document if the implant of biomaterial without cells could lead to better results and understanding if the cell-free scaffold approach could offer a positive and durable outcome in the treatment of cartilage lesions.
The aim of this study was to systematically review the current literature, in order to provide an updated insight on the potential of cell-free scaffolds, evaluating their results over time with a meta-analysis.
Materials and Methods
A systematic review and a meta-analysis were performed on the literature of cell-free chondral scaffold implantation for cartilage knee lesions. The search was conducted on PubMed, Web of Science and Cochrane databases on January 14, 2019, using of the following parameters: ((cartilage OR chondral) AND (defect OR defects OR lesion OR lesions)) AND (AMIC OR ACIC OR (cell-free AND (scaffold OR implant))). The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines were used. 9 A flowchart of the studies selection for qualitative and quantitative data synthesis is reported in Figure 1 . The screening process and analysis were conducted separately by 2 independent observers (D.R. and A.B.). In the first step, the articles were screened by title and abstract. The following inclusion criteria for relevant articles were used during the initial screening of titles and abstracts: clinical reports of any level of evidence, written in the English language, on cells-free scaffolds for the treatment of cartilage lesion of the knee. Exclusion criteria were articles written in other languages, preclinical studies, studies reporting other chondral and osteochondral not cell-free procedures such as cell-based scaffolds, autologous blood- or platelet-rich plasma–augmented techniques, and osteochondral scaffolds, and reviews. In the second step, the full texts of the selected articles were retrieved and screened, with further exclusions according to the previously described criteria. Moreover, articles not reporting clinical results were excluded. Reference lists from the selected papers and from the systematic reviews, found with the first and second screening, were also checked, and all selected studies were included in the qualitative data synthesis.
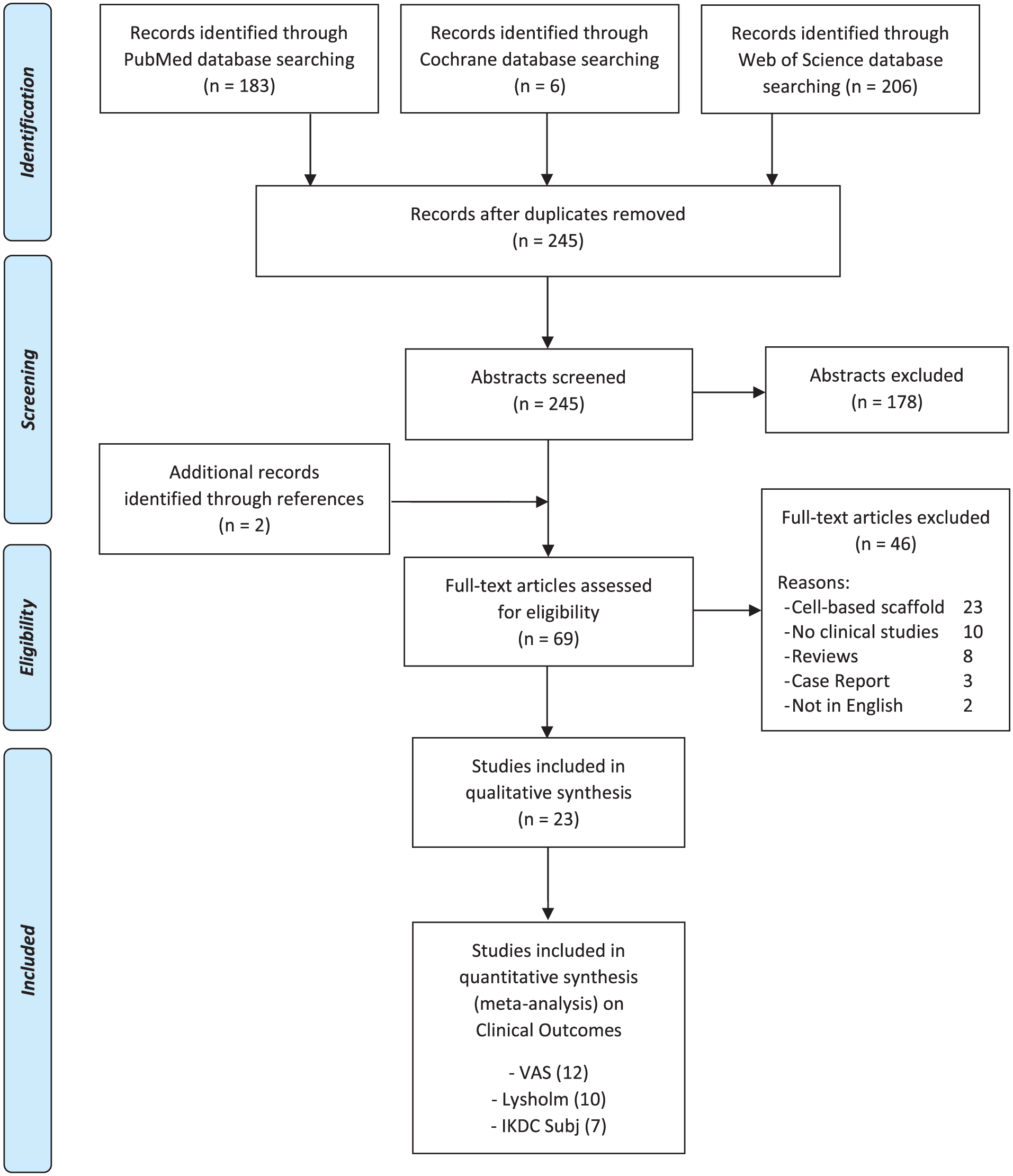
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flowchart of the systematic literature review.
Relevant data (year, type of study, number of patients, sex, age, body mass index, follow-up, lesion size, lesion location, lesion grade, type of scaffold, scores reported, results) were then extracted and collected in a database with consensus of the 2 observers, to be analyzed for the purposes of the present study. To assess the methodological quality of the collected data, the subscales of a Coleman Methodology Score (CMS), modified by Kon et al. 10 to better suit to the cartilage repair field, were determined for each study. The articles reporting at least one of specific clinical outcomes (visual analogue score [VAS], Lysholm score, International Knee Documentation Committee [IKDC] subjective scores) were selected and included in the meta-analysis. The articles included in the systematic review were excluded from the meta-analysis in the following cases: the same survey was reported at different follow-up times and the most recent articles also reported the intermediate follow-up results; basal scores or follow-up scores (including standard deviation) not reported; results reported according to other clinical outcome measurements. All scores were reported and analyzed as improvement from basal scores at 1, 2, and ≥3 years’ follow-up, in order to investigate any clinical results improvement over time of cell-free cartilage scaffold implantation.
Statistical Analysis
The statistical analysis and the forest plots were carried out according to Neyeloff et al. 11 using Microsoft Excel. The comparisons among the follow-up times was based on the analysis of variance 12 of the difference between basal and follow-up score (MD). With no heterogeneity, the estimation of the MD and its 95% confidence interval was based on fixed effect analysis of variance; the random effect model was preferred otherwise. A P value of 0.05 was used as the level of statistical significance. Statistical heterogeneity was evaluated by t using Cochran’s Q statistic and I2 metric and was considered significant when I2 > 25%.
Results
The search identified 245 records, whose abstracts were screened and selected according to the inclusion/exclusion criteria ( Fig. 1 ): 178 abstracts were excluded and 2 articles were identified through the reference lists, which gave a total of 69 full-text articles assessed for eligibility. Forty-six full-text articles were also excluded for the following reasons: 23 articles reported on cell-based techniques, 10 articles did not report clinical results, 8 articles were reviews, 3 articles were case reports, and 2 articles did not present the full-text in English language.
Therefore, a total of 23 studies13-35 were included in the qualitative data synthesis and reported in detail in Table 1 . The scores used to assess results in these articles are summarized in Table 2 . Among the different scores used in the literature, we selected the most common ones reported at every follow-up time (VAS, Lysholm, IKDC subjective score) for the meta-analysis: 12 articles reported subjective outcome evaluated with VAS, 10 articles with the Lysholm score, and 7 articles with the IKDC subjective score.
Characteristics of the 23 Articles Included in the Qualitative Data Synthesis, with Study Quality Assessment.
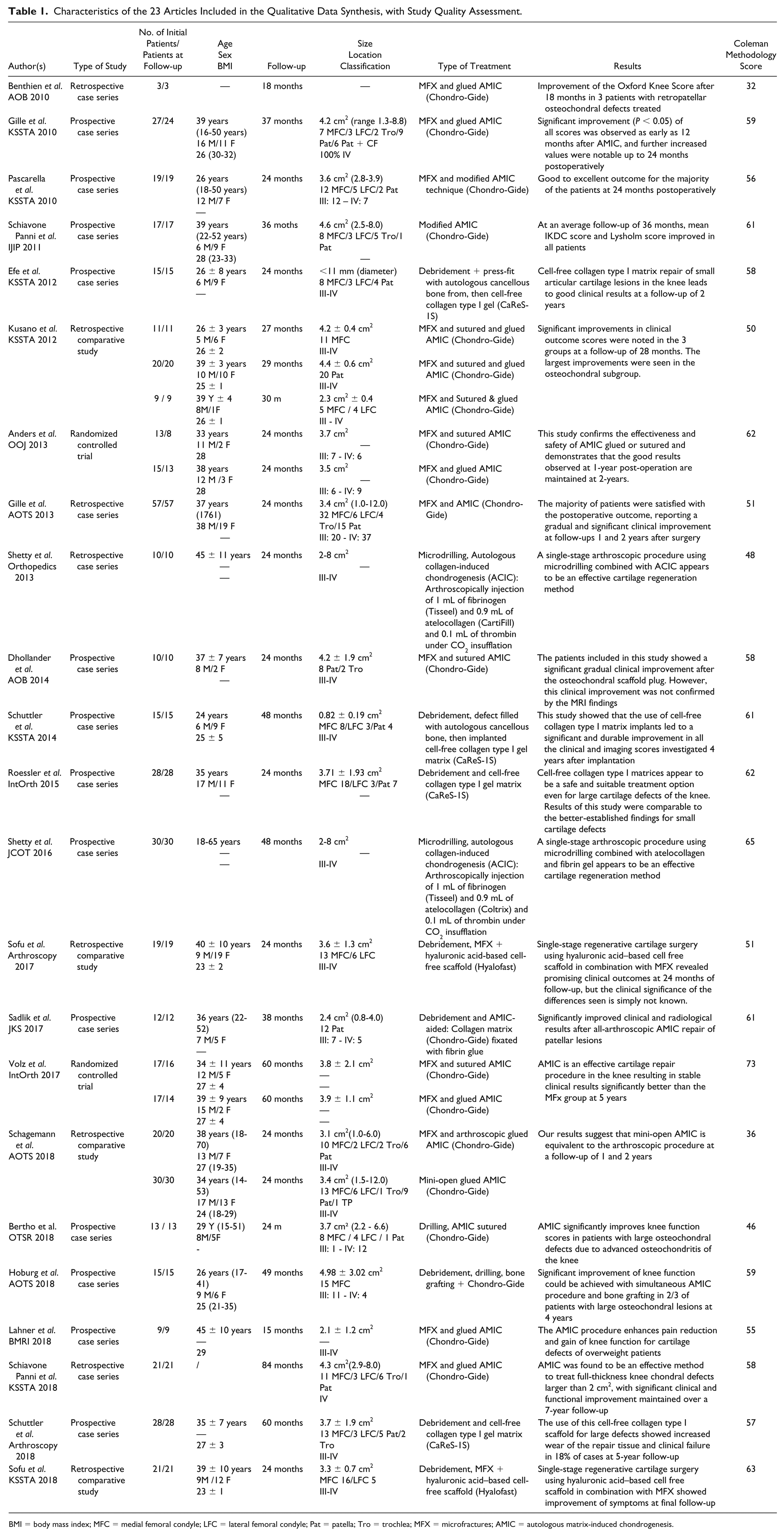
BMI = body mass index; MFC = medial femoral condyle; LFC = lateral femoral condyle; Pat = patella; Tro = trochlea; MFX = microfractures; AMIC = autologous matrix-induced chondrogenesis.
List of the Different Scores Used in the Articles Included in the Qualitative Data Synthesis.
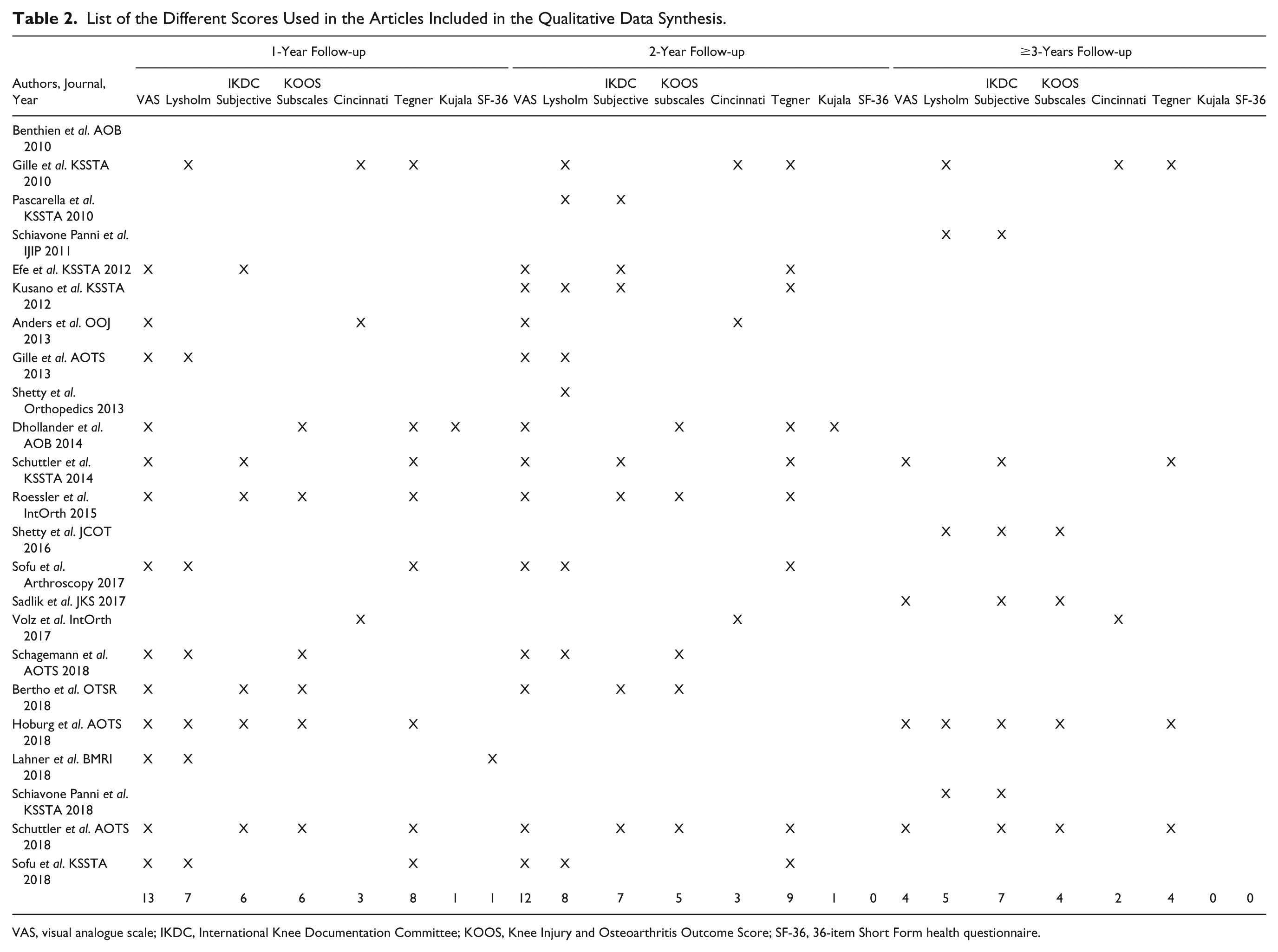
VAS, visual analogue scale; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; SF-36, 36-item Short Form health questionnaire.
Qualitative Data Synthesis
Among the 23 articles included in the qualitative data synthesis, the evaluation of study type showed 2 articles reporting the outcome of 1 randomized clinical trial (RCT), 4 comparative studies, and 17 case series (with 2 articles reporting the outcome of the same cohort at different follow-ups) ( Table 1 ). In 19 articles the scaffolds were used combined with microfractures or drilling, in 4 articles the surgical technique entailed only the debridement of the defect. Fifteen articles analyzed the results of Chondro-Gide scaffold (2 articles reporting on 1 RCT, 2 comparative studies, and 11 case series), 4 of CaReS-1S (4 case series), 2 of Hyalofast (2 comparative studies), and 1 case series each for Coltrix and CartiFill. Since the first reports in 2010, the publication trend did not significantly increase over time, with 9 articles published from 2010 to 2013 and 7 articles from 2014 to 2017, with the exception of 2018, with the highest value of 7 articles published ( Fig. 2 ).
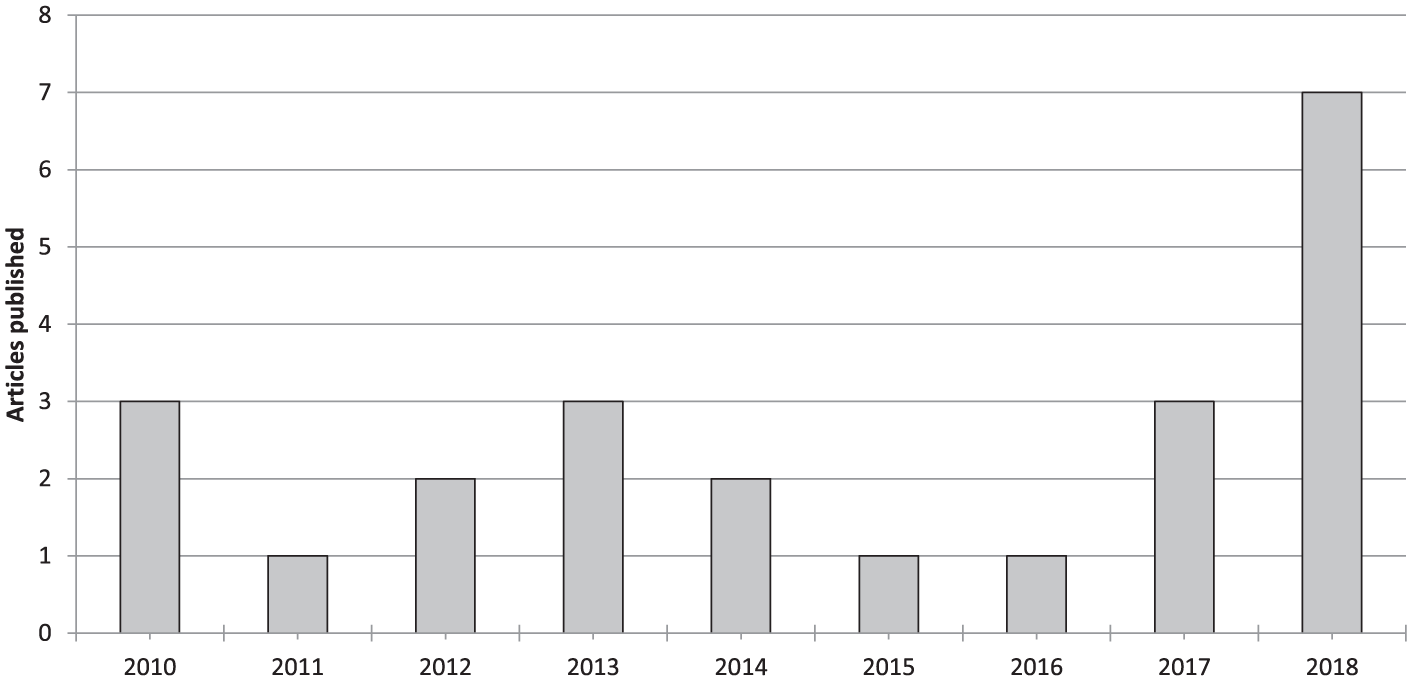
Number of articles per year dealing with cell-free scaffold techniques.
Similarly, even the level of evidence of the literature did not increase, with only 1 RCT reported in 2 articles published by the same group, the first one being only an interim analysis of the same RCT. The evaluation with the CMS showed an overall poor quality of the included studies. In fact, only 1 study scored higher than 70 and only 7 studies reached a score between 60 and 69, whereas 11 studies had a score between 50 and 59, and 4 studies obtained a score lower than 50. No improvement over time was found for CMS score ( Fig. 3 ).
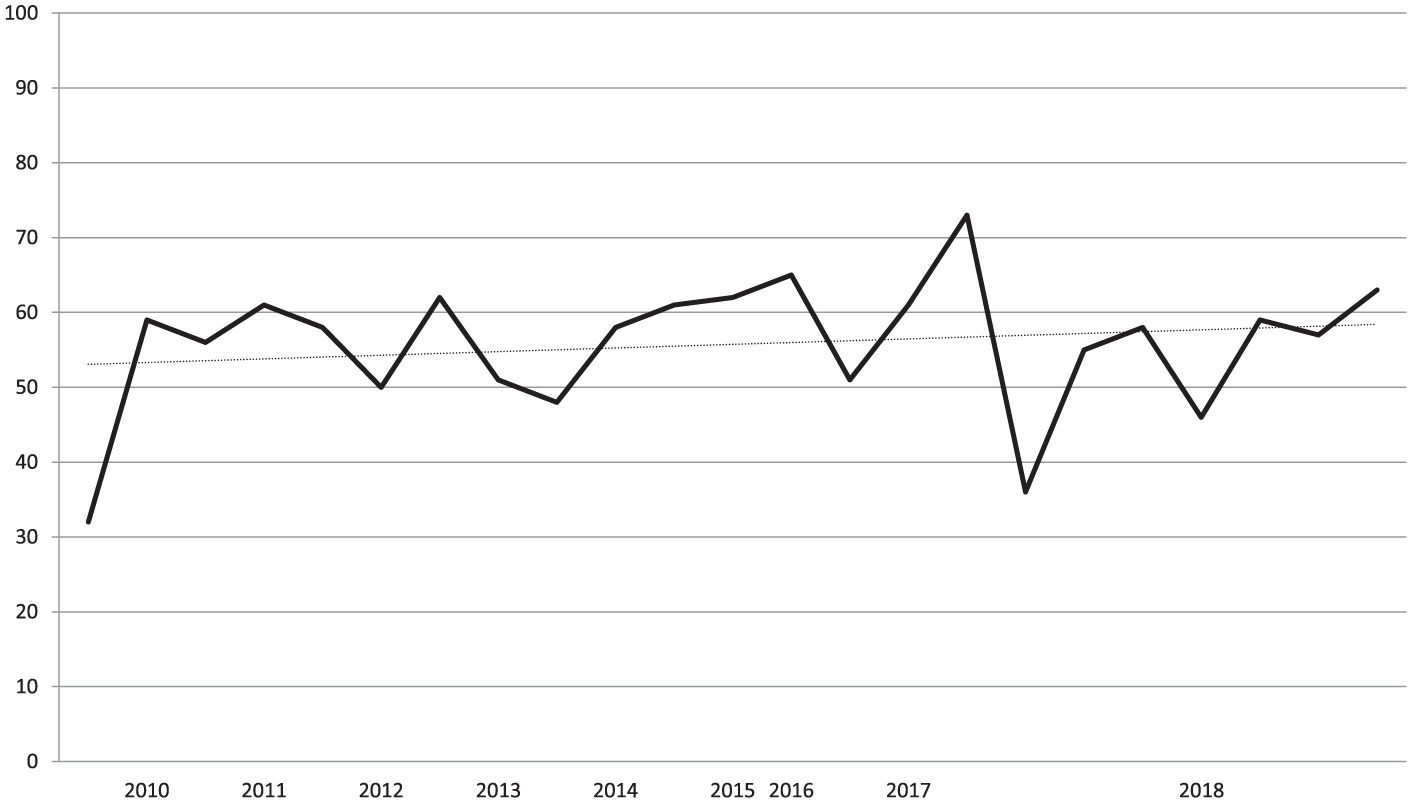
Trend over time of the Coleman Methodology Score (CMS) of the articles dealing with cell-free scaffold techniques.
A total of 526 patients were treated with cell-free scaffolds, and the outcomes of 507 patients were reported (a detailed description of the analyzed data, with the number of patients and the specific data available is provided in Table 3 ). Patients were evaluated using a wide range of heterogeneous scores ( Table 2 ), at a mean of 34.4 months’ follow-up: 13 studies reported the outcome at short-term follow- up (≤24 months), 7 at short-/mid-term follow-up (24-60 months), and only 3 at mid-term follow-up (≥60 months), including the longest follow-up available in the literature (84 months). The study follow-up duration over the years did not show an increasing trend and in the last year only 2 mid-term follow-up studies were included in the review, with 1 short-/mid-term and 4 short-term follow-up studies ( Fig. 4 ).
Demographic Data of the Patients Analyzed in the Articles Included in the Qualitative Data Synthesis.
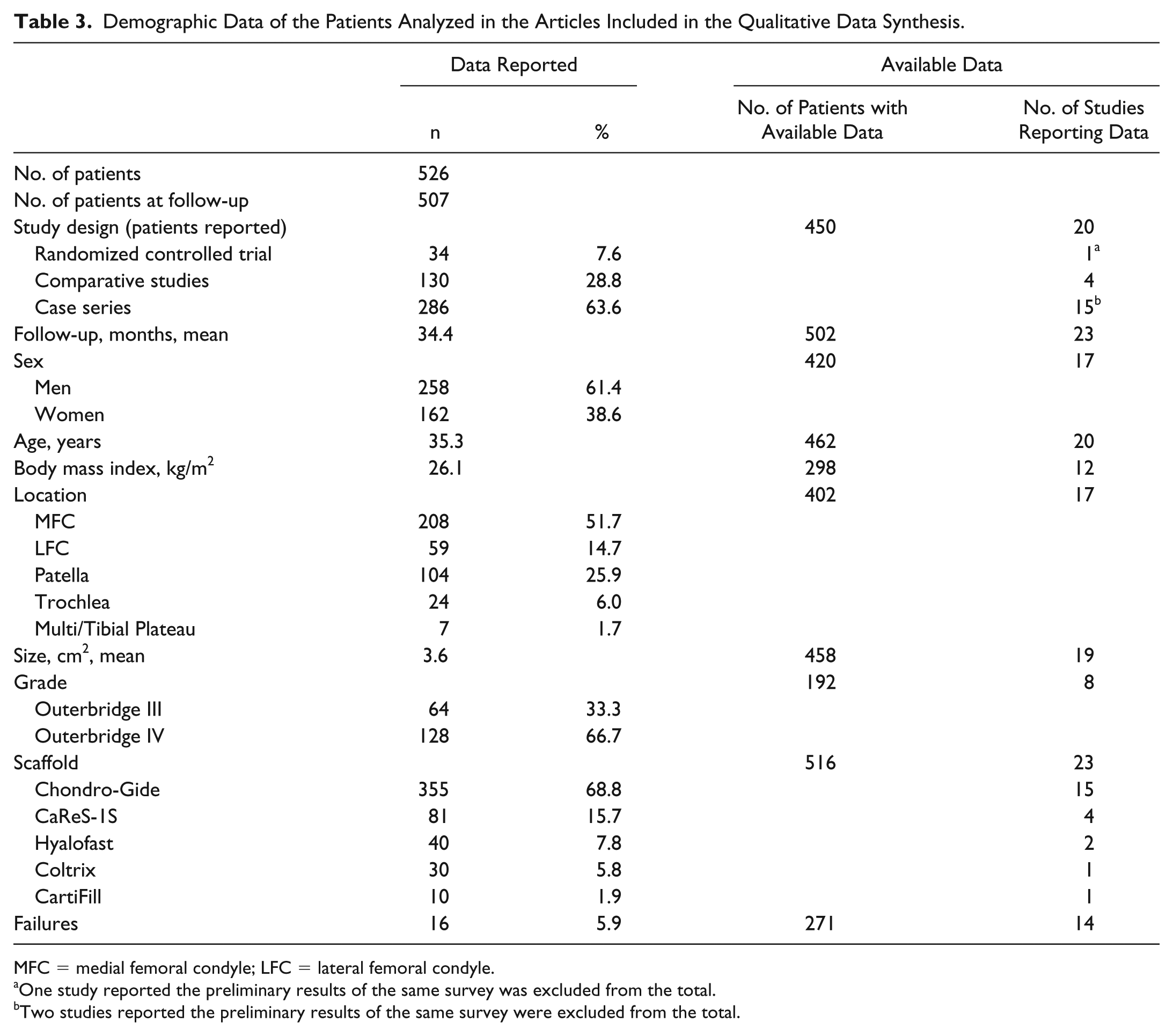
MFC = medial femoral condyle; LFC = lateral femoral condyle.
One study reported the preliminary results of the same survey was excluded from the total.
Two studies reported the preliminary results of the same survey were excluded from the total.
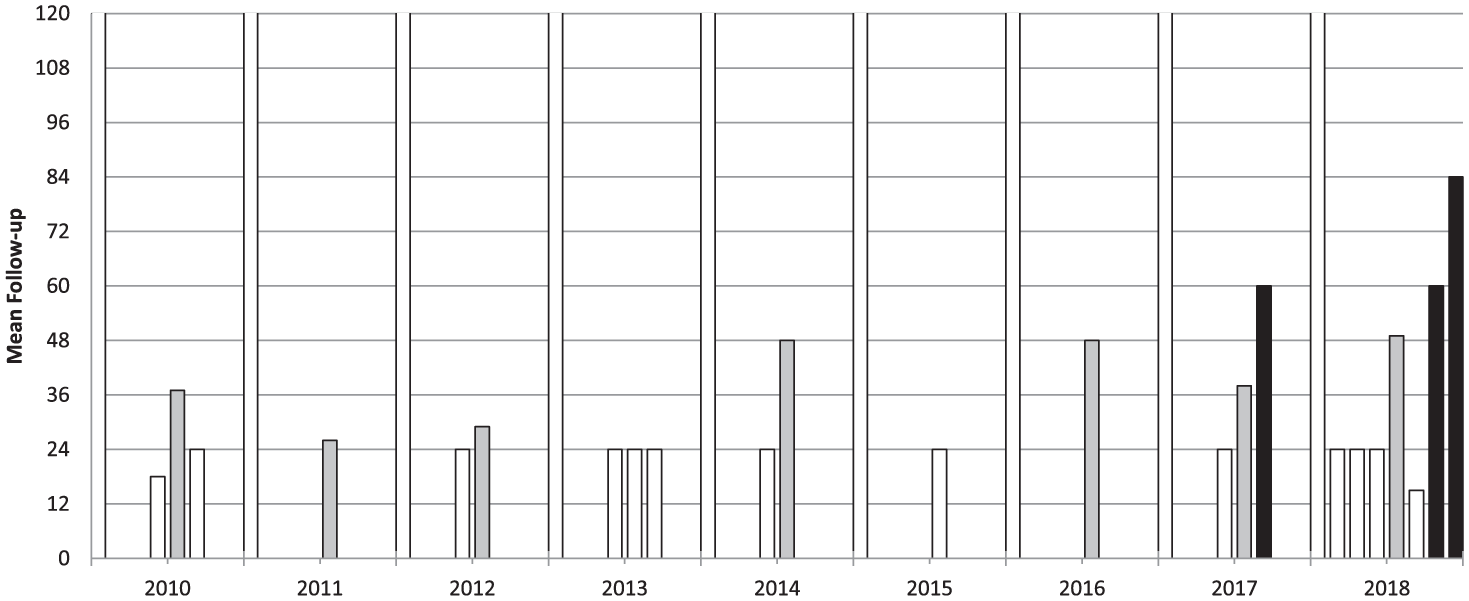
Mean follow-up of the articles dealing with cell-free scaffold techniques.
Failures were reported only in 14 articles, with 16 failures among 271 patients evaluated at a mean 34.8 months of follow-up, for an overall 5.9% failure rate.
Clinical Scores Meta-Analysis
Seven studies of the systematic review were excluded from the meta-analysis for the following reasons: preliminary data of the same survey (3 studies),23,29,30 no clinical scores (1 study), 33 no standard deviation reported (3 studies).26,32,35 Thus, 16 studies (for a total of 20 study groups)13-22,24,25,27,28,31,34 were included in the quantitative synthesis.
Pain evaluated with VAS was available for 289 patients in 12 studies (15 study groups).13-18,20,22,24,27,28,31 In detail, 1-year VAS follow-up was available for 237 patients (11 study groups in 10 studies), 2-year follow-up for 253 patients (12 study groups in 9 studies), and ≥3-year follow-up (mean 48.8 ± 9.0 months from surgery) for 58 patients (4 study groups in 4 studies). Compared with the basal score, the meta-analysis on VAS showed a mean improvement of 37.6 (95% CI 31.8-43.4, I2 = −29%) at 1-year follow-up, 39.1 (95% CI 34.0-44.3, I2 = −64%) at 2-year follow-up, and 40.0 (95% CI 24.7-55.4, I2 = −20%) at ≥3-year follow-up ( Fig. 5 ), all significantly higher than baseline (P < 0.05), but without any significant difference among follow-up times. That is, the improvement reached in the first year remained stable up to the final follow-up, average 49 months.
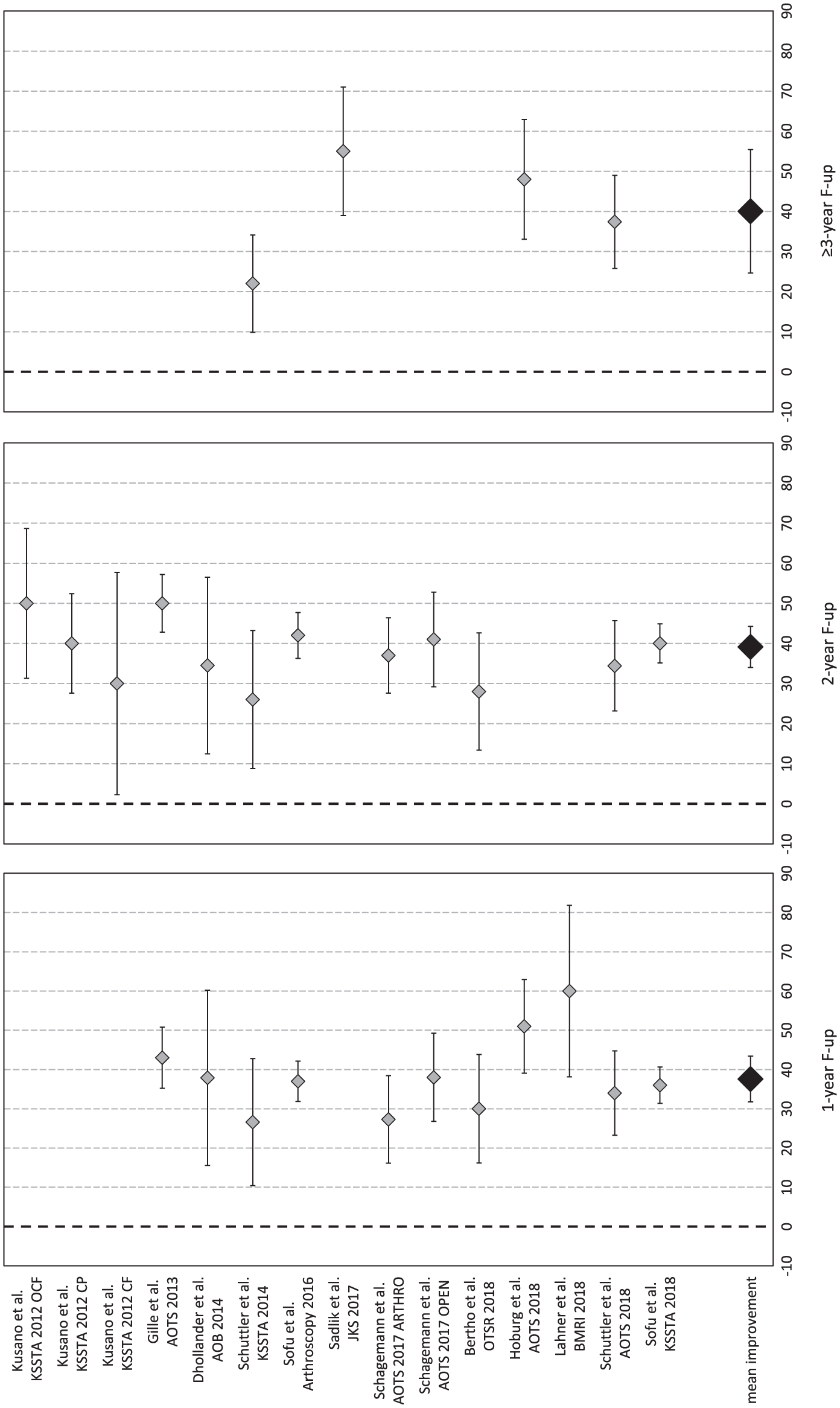
Forest plot of mean improvement of visual analogue scale (VAS) score at 1, 2, and ≥3 years’ follow-up.
The Lysholm score was available for 265 patients in 10 studies (13 study groups).14,16-19,22,25,27,31,34 In detail, 1-year follow-up was available for 194 patients (8 study groups in 7 studies), 2-year follow-up for 220 patients (10 study groups in 7 studies), and ≥ 3-year follow-up (mean 56.0±25.0 months from surgery) for 43 patients (3 study groups in 3 studies). Compared with the basal score, the meta-analysis showed a mean improvement of 35.0 (95% CI 29.8-40.3, I2 = −76%) at 1-year follow-up, 36.7 (95% CI 30.5-42.9, I2 = −48%) at 2-year follow-up, and 33.8 (95% CI 27.1-40.5, I2 = 17%) at ≥3-year follow-up ( Fig. 6 ), all significantly higher than baseline (P < 0.05), but without any significant difference among follow-up times. That is, the improvement reached in the first year remained stable up to the final follow-up, average 56 months.
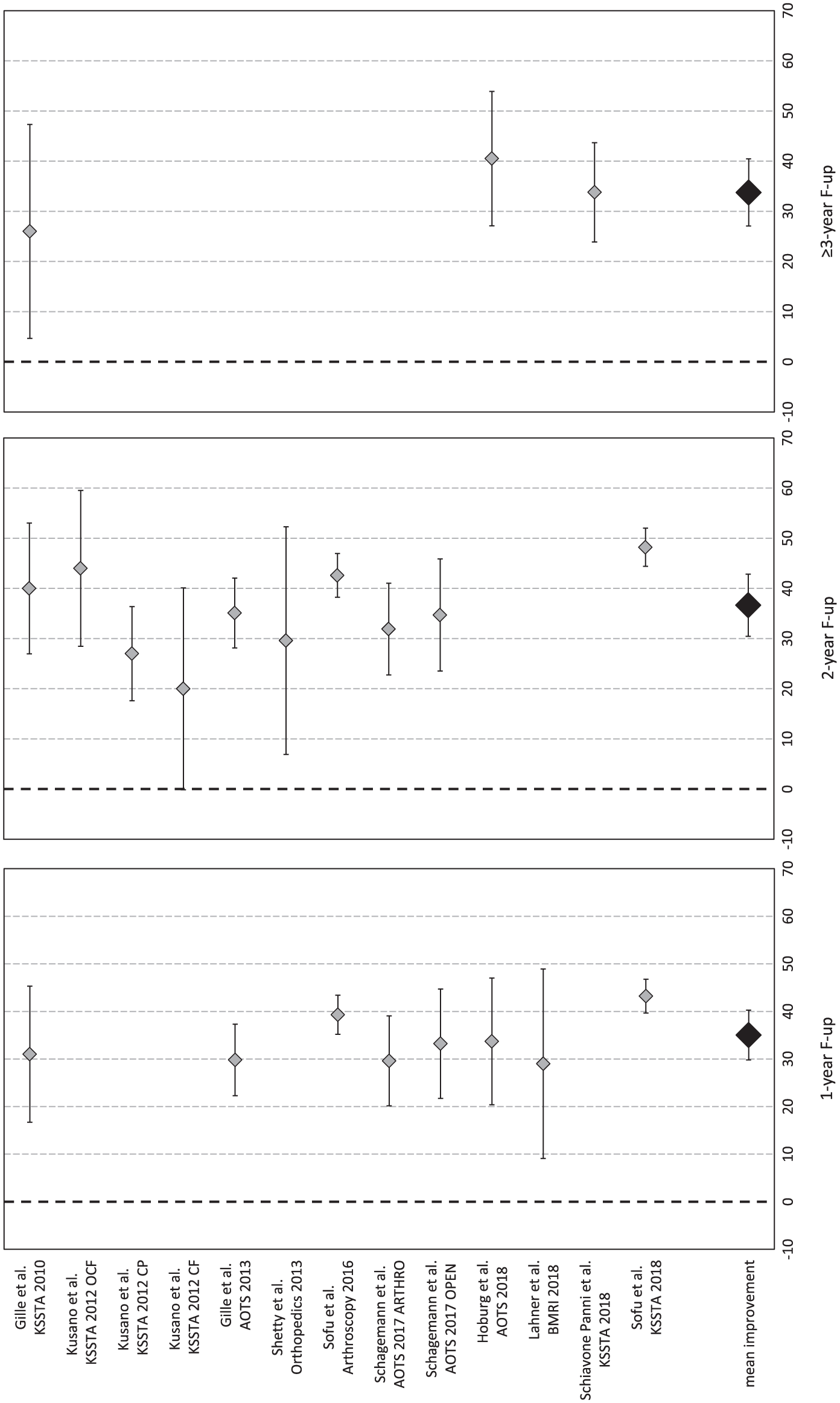
Forest plot of mean improvement of Lysholm score at 1, 2, and ≥3 years’ follow-up.
The IKDC subjective score was available for 144 patients in 7 studies (9 study groups).13,15,17,19,20,28,31 In detail, 1-year follow-up was available for 71 patients (4 study groups in 4 studies), 2-year follow-up for 96 patients (6 study groups in 4 studies), and ≥3-year follow-up (mean 56.0 ± 17.6 months from surgery) for 81 patients (5 study groups in 5 studies). Compared with the basal score, the meta-analysis showed a mean improvement of 19.6 (95% CI 9.4-29.8, I2 = −62%) at 1-year follow-up, 24.4 (95% CI 14.0-34.8, I2 = −48%) at 2-year follow-up, and 34.4 (95% CI 29.6-39.3, I2 = 92%) at ≥3-year follow-up ( Fig. 7 ), all significantly higher than baseline (P < 0.05), but without any significant difference among follow-up times. That is, the improvement reached in the first year remained stable up to the final follow-up, average 56 months.
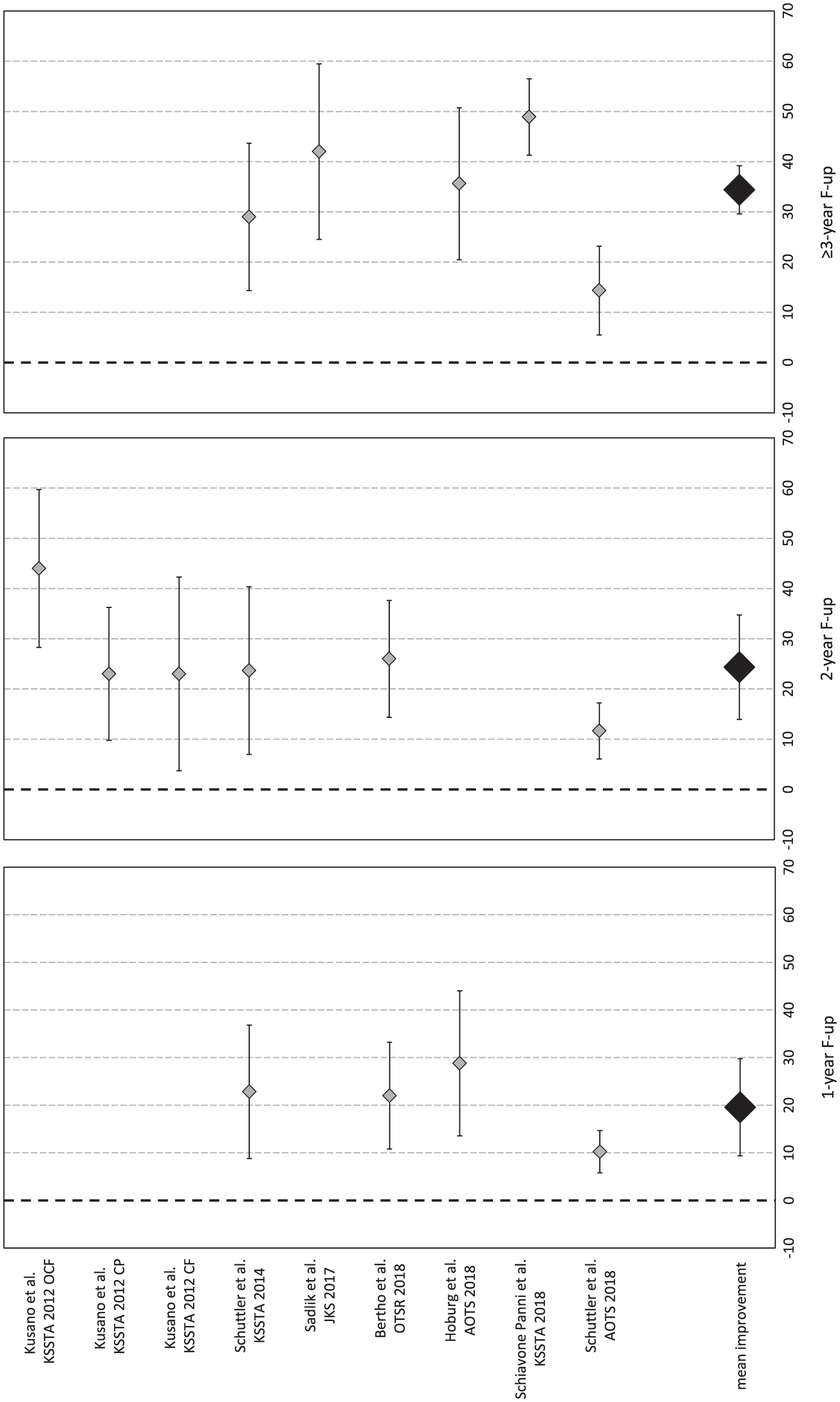
Forest plot of mean improvement of International Knee Documentation Committee (IKDC) subjective score at 1, 2, and ≥3 years’ follow-up.
Discussion
The main finding of the present study was that cell-free chondral scaffolds provided significant improvement at short-/mid-term follow-up, but the evidence level was limited and studies at longer follow-up were missing.
Surgical treatments of cartilage lesions have the main indication for young active patients, 36 where the recovery time is an important aspect; therefore, early follow-ups are useful to provide correct expectations to patients undergoing these procedures. In this light, this meta-analysis showed that at 1-year follow-up all evaluated scores improved significantly compared with the baseline scores, demonstrating the efficacy of the technique. Moreover, the evaluation at 2 years’ follow-up did not show a further improvement, suggesting that most of the benefit had already been achieved in the first year. This is in line with studies about microfractures, which led to a relatively fast recovery. 37 Interestingly, this trend differs from what reported for cell-based techniques, where a further improvement has been documented from 1 to 2 years of follow-up. 38 This shows that the scaffold-based cell-free approach presents an improvement trend more similar to microfracture than cell-based procedures, as also confirmed by the only RCT comparing MFX and cell-free scaffold approach.21,29
Another important aspect to evaluate in surgical chondral procedures is the stability of clinical results over time. Cell-based cartilage procedures have already been evaluated at long-term follow-up, and even if results are not univocal in the literature, a general trend can be depicted. ACI and MACT generally showed stable results up to a long-term follow-up.36,38-43 Microfractures, on the other hand, showed more controversial results. While short-term results are supported by good-level evidence, long-term results are not 37 : some studies reported good long-term results for microfractures,44-47 but other articles reported worst results and an increasing number of failures versus mosaicplasty.48-50 Moreover, some studies documented a worsening trend over time, with positive short-term results and a decrease at mid-/long-term.51,52 This meta-analysis showed that clinical results after scaffold-based cell-free approach remained stable for up to ≥3 years’ follow-up, and a RCT reporting mid-term results demonstrated significant better outcome for cell-free scaffold compared to microfractures at 5 years’ follow-up. 21 Unfortunately, the current literature does not allow to draw conclusions on long-term follow-ups and the reported findings on results duration have to be taken with caution. Besides the low number of studies, mainly reporting on small series at a short-follow-up, the overall study quality is limited, as evaluated with the modified CMS.
The relatively short follow-up of the published studies should be underlined, also considering that this surgical approach cannot be considered recent. The first articles included in this review are dated 2010,33-35 and the cell-free techniques had actually been already described in a report dated 2006. 53 Moreover, since 2005, patients treated with Chondro-Gide (Geistlich Pharma, Switzerland), a scaffold-based cell-free approach, started to be enrolled in the “AMIC Registry.” 27 Consequently, considering the high number of patients treated and initially followed, and the time elapsed from those documented treatments, these techniques can no longer be considered new and long-term follow-up studies are lacking to confirm the duration of documented benefits of these procedures.
The quality of the overall literature on this topic is very low, as confirmed by the CMS of the published studies and by the presence of only 1 RCT on AMIC, reported in 2 different articles included in the systematic review. This aspect has been previously underlined, 54 and the current update does not show any improvement in the evidence level of the scientific literature over time. High-level comparative studies are needed to demonstrate the advantage of implementing microfractures with a cell-free scaffold or of using cell-free scaffolds alone. Moreover, since currently cell-based therapies are the most documented regenerative techniques, comparative studies including also the economic evaluation are needed to fully evaluate advantages and disadvantages of cell-based and cell-free strategies for the treatment of cartilage lesions. The limitations of the current systematic review and meta-analysis reflect the abovementioned limitations of the literature: paucity of studies, generally of low quality, including a low number of patients evaluated at short- to mid-term follow-up with heterogeneous scores. Accordingly, a weakness of the meta-analysis is represented by the high proportion of evidence level IV studies and this is also the reason why it was not possible to perform further subanalysis (e.g., techniques with microfractures/drilling vs. cell-free scaffold alone). Moreover, the inclusion of heterogeneous surgical techniques and scaffolds (e.g., collagen scaffolds, hyaluronic acid scaffolds, atelocollagen, with or without microfractures) may weaken the results of this study. Nonetheless, all these studies use the cell-free scaffold-based approach, proposed as alternative to the cell-based one, which also includes variants related to techniques and scaffolds applied. Until comparative studies specifically focused on this issue will prove differences among the several proposed variants of these approaches, the literature will only allow a broad comparison of the 2 strategies, while it cannot demonstrate if and which techniques emerges as the most suitable cell-based or cell-free options.
In conclusion, the current literature suggests that cell-free scaffolds may provide good clinical short-/mid-term results, but the low evidence of the published studies and their short mean follow-up, demand further evidence before drawing more definitive conclusions on the real potential of this technique over time and on its advantages and disadvantages compared with cell-based strategies for the treatment of cartilage lesions.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.