
Abstract
Objective
Tibial plateau osteochondral allograft transplantation is a promising treatment for symptomatic chondral damage of the proximal tibia due to a variety of etiologies. The purpose of this investigation is to develop an accurate and reproducible algorithm for sizing tibial plateau allografts based on recipient radiographs.
Design
A cadaveric study was performed in which radiographs of 10 fresh frozen cadaveric knees were compared to measured digital photographs of the disarticulated specimens. By comparing the average distance between standard anatomical landmarks on the radiographs to the gross specimens, a correlation factor was calculated that could be applied to recipient radiograph measurements for more accurate sizing of tibial plateau allografts.
Results
In the coronal plane there were no differences between the mean radiographic and mean morphologic measurements of either the medial or lateral tibial plateau. However, in the sagittal plane the anatomic specimens of the medial and lateral plateau were 90% and 80%, respectively, of the measurements made from the lateral radiograph.
Conclusions
This cadaveric investigation is the first to propose a sizing algorithm for tibial plateau osteochondral allografts. Based on the results, an anteroposterior radiograph can reliably measure the width of both the medial and lateral tibial plateau without any correction needed. The average morphological lengths of the medial and lateral tibial plateau, on the other hand, were found to be 90% and 80%, respectively, of the radiographically measured lengths. Without correction, this would lead to the implantation of oversized grafts that may contribute to early failure.
Introduction
Osteochondral allograft transplantation of the medial or lateral tibial plateau with the corresponding meniscus is an uncommon but important procedure in the arsenal of the cartilage restoration surgeon. This procedure was first described by Gross et al. in 1983 as a means of treating posttraumatic chondral injuries following tibial plateau fractures. 1 These authors prospectively followed their series of 65 patients, and they found long-term survival of the allografts to be 95% at 5 years, 80% at 10 years, and 65% at 15 years. 2 The 21 patients who failed were still able to avoid arthroplasty for a mean interval of 10 years. While others have also reported successful use of plateau allografts following trauma, additional indications for the procedure include reconstruction after resection of benign and malignant tumors or after infection-induced chondrolysis.1,3,4 Furthermore, as 25% of articular cartilage defects in athletes’ knees occur on the tibial plateau, allograft reconstruction of a hemi-plateau may be indicated depending on the size of the lesion and the status of the adjacent meniscus. 5
Transplantation of a tibial osteochondral allograft is a complex procedure in which many factors may influence a patient’s outcome. Among these, and similar to a meniscal transplant, accurate size matching of the donor to the recipient, while intuitively essential, remains incompletely investigated. Pollard et al. previously described the gold standard technique for size matching a meniscal allograft. 6 In a cadaveric study the authors compared anatomic specimens to standardized plain radiographs to determine a correction factor for the length and width of medial and lateral menisci allografts. However, there are no similar algorithms for sizing a tibial plateau osteochondral allograft to assist in preoperative planning. This factor alone may constitute a primary barrier to more widespread use of tibial osteochondral allografts.
This study sought to establish a preoperative sizing algorithm to be used when transplanting osteochondral allografts of the tibial plateau. The authors hypothesized that standard landmarks as identified on an anteroposterior (AP) and lateral radiograph could be used to generate an algorithm to appropriately size tibial plateau osteochondral allografts with tolerances similar to those accepted with the gold standard for sizing meniscal allografts. 6
Methods
Ten fresh frozen knee cadaveric specimens with no history of premorbid fracture, nor ligamentous or meniscal injury were used. AP ( Fig. 1A and B ) and lateral ( Fig. 1C ) radiographs were taken of each specimen. Radiographs were performed with the knees in full extension. It should be noted that radiographs were chosen as opposed to magnetic resonance imaging (MRI) as they are cheaper, easier to obtain, and do not have issues with artifact. The radiographic coronal dimension, or width, of each hemi-plateau was determined using the AP view, which was taken with a 15° caudal tilt to generate plateau views. Only images with distinct medial and lateral tibial eminences were accepted. On the medial side, 2 lines were drawn, one tangent to the medial articular margin, and the second through the peak of the medial tibial eminence. The angle tool was used to ensure that these lines were both perpendicular to the articular surface ( Fig. 1A ). The radiographic coronal dimension of the lateral plateau was measured similarly with 2 parallel lines extending from the lateral articular margin to the peak of the lateral tibial eminence ( Fig. 1B ).
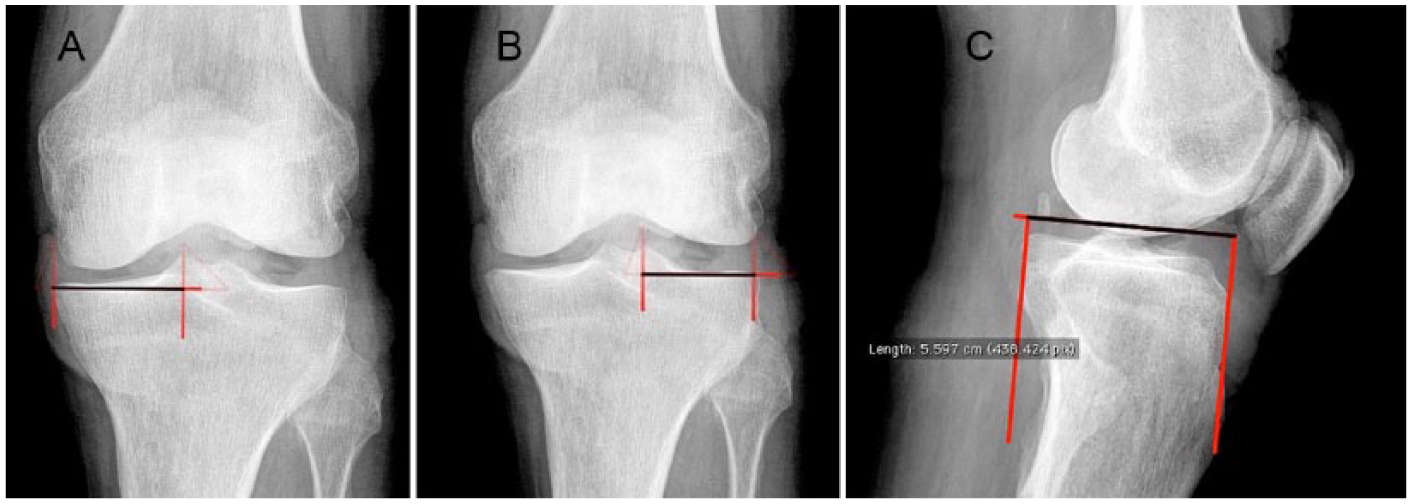
Example AP and lateral radiographs of cadaveric specimens taken in full extension. Panels
The radiographic sagittal dimension was measured from the lateral radiograph of each specimen ( Fig. 1C ). Lateral images were taken carefully to ensure superimposition overlap of the posterior femoral condyles with no more than 3 mm of mismatch accepted. Due to the overlap of the medial and lateral plateaus on the lateral radiograph, it was assumed that consistent reliable distinction of one compartment from the other would not be possible. Thus, a single measurement was taken of the sagittal dimension and applied to each hemi-plateau. This was done by creating 2 parallel lines. The first was created perpendicular to the anterior surface of the tibia, just proximal to the tuberosity. This ensured that the radiographic sagittal dimension would be measured in the same plane as the natural posterior slope of each specimen. The second line was created parallel to the first, tangential to the posterior articular margin.
Following radiographic analysis, the specimens were disarticulated and the proximal tibias were dissected free from all soft tissue except the menisci. The menisci were freed from their capsular attachments while the anterior and posterior horn insertions were left intact. High-resolution digital photographs ( Fig. 2A and B ) were subsequently taken of each medial and lateral plateau. A metric ruler was placed at the same height as the articular surface of the tibial plateau to facilitate calibration of the measurement tool in the software used to analyze the images. The photographs were taken with the respective meniscus lifted away from the articular surface, to prevent obstruction of the peripheral margin of the plateau caused by any meniscal overhang.
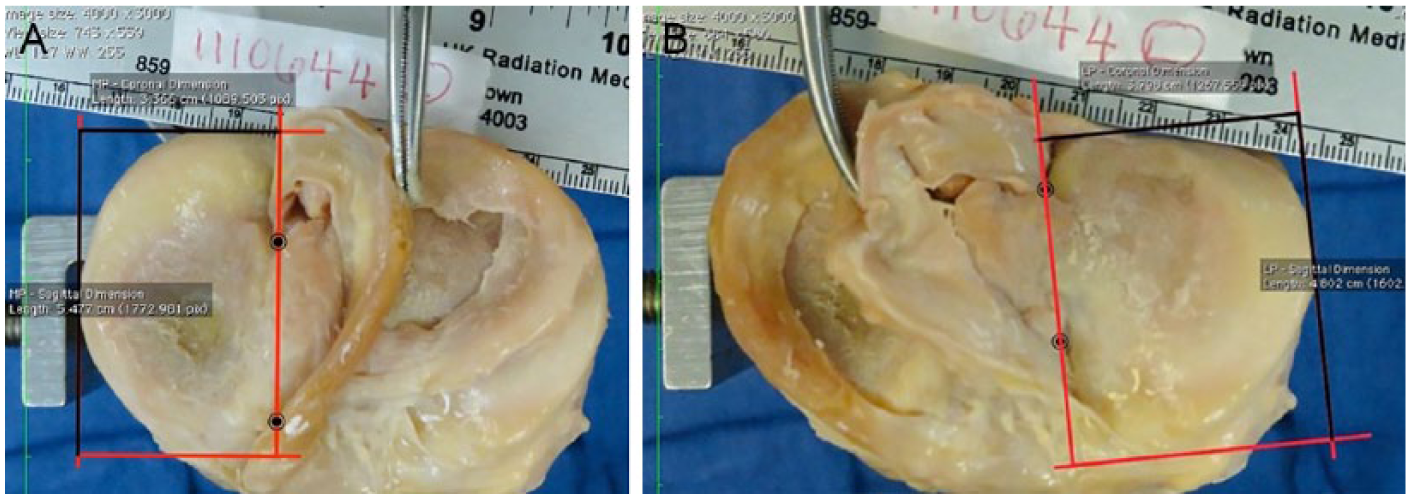
Example cadaveric specimens illustrating the method for determining the width of the medial (
In a manner similar to Pollard et al.’s investigation on meniscal allograft sizing, the photographs were used to determine the true sagittal (plateau length) and coronal (plateau width) dimensions of each hemi-plateau. 6 The collinear relationship between the insertion of the medial and lateral meniscal horns and the respective tibial eminence have previously been described. 7 As such, the lateral border of the medial plateau was established by drawing a line connecting the most central point of the anterior horn of the medial meniscus with the most central point of the posterior horn of the medial meniscus. Subsequently, the chosen lateral border of medial plateau could be correlated with the radiographic projection of the medial tibial eminence.
The anterior, posterior, and medial borders of the medial plateau were defined as the respective edges of the articular surface. An angle tool was then used to construct a series of right angles such that the medial plateau was encompassed by a rectangle with length equal to the sagittal dimension of the medial plateau, and width equal to the coronal dimension of the medial plateau ( Fig. 2A ). This was repeated for each specimen.
The anterior, posterior, and lateral borders of the lateral plateau were also defined as the respective edges of the articular surface. The medial border of the lateral plateau was established using the meniscal horns in the same manner as described above for the medial side. The angle tool was likewise used to create a rectangle with a length equal to the sagittal dimension of the lateral plateau and a width equal to the coronal dimension of the lateral plateau ( Fig. 2B ). This was repeated for each specimen.
Statistical Analysis
Using the mean coronal and sagittal dimensions obtained from the photographs of the gross cadaveric specimens and radiographs, a correlation factor was calculated. Similar to Pollard et al.’s sizing algorithm for meniscal allograft transplantations, this was defined as the ratio between the morphologic and radiographic measurements. This calculation represents the correction necessary to apply to the measurements of an AP and lateral radiograph when sizing a tibial plateau osteochondral allograft. 6 The photographs and radiographs were analyzed using OsiriX software (OsiriX, Switzerland). 8
Results
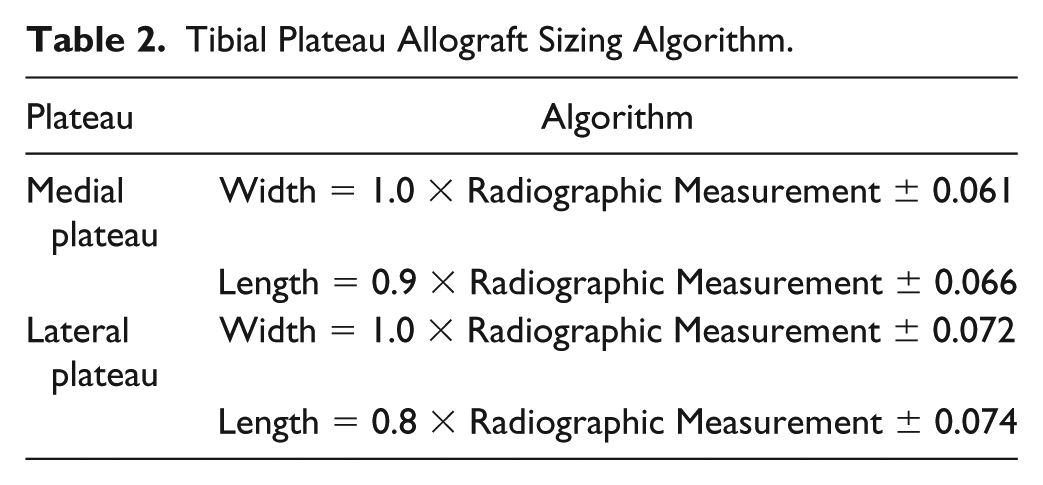
The mean radiographic and gross morphologic measurements for the width and lengths of both the medial and lateral plateaus are presented in Table 1 . Using these measurements, the average correlation factors for the width and length of each hemi-plateau were calculated. The correlation factor for the width of both the medial and lateral plateau was found to be 1.0, meaning measurements taken on AP radiographs can accurately estimate the width of an osteochondral allograft without correction. However, the correlation factors for the medial and lateral plateaus lengths were 0.921 and 0.778, respectively, meaning the radiographs overestimate the sagittal dimensions of both medial and lateral grafts. A summary of the sizing algorithm incorporating these findings is presented in Table 2 .
Mean Radiographic and Morphologic Plateau Measurements with Associated Correlation Factor.
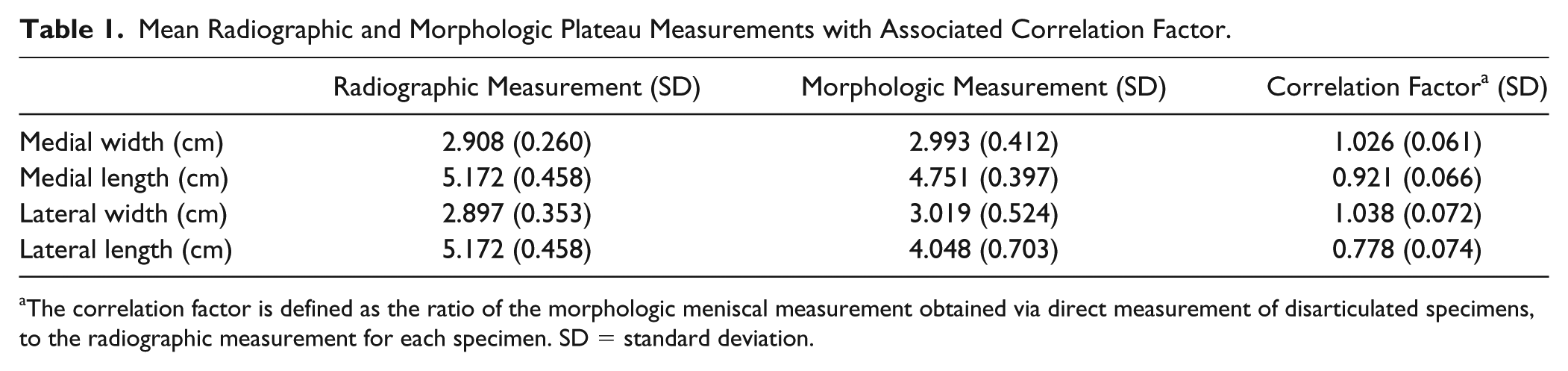
The correlation factor is defined as the ratio of the morphologic meniscal measurement obtained via direct measurement of disarticulated specimens, to the radiographic measurement for each specimen. SD = standard deviation.
Tibial Plateau Allograft Sizing Algorithm.
Discussion
This is the first study to investigate means of improving size matching in osteochondral tibial allografts. The results have led to the development of a simple algorithm to calculate the ideal donor tibial plateau osteochondral allograft size. Accordingly, a standard AP radiograph taken with the knee in full extension and in 15° of caudal tilt can accurately measure the width of either the medial or tibial plateau without any correction. However, the radiographic length of the medial and lateral plateau obtained on the lateral radiograph should be multiplied by 0.9 and 0.8, respectively.
Chondral lesions of the tibial plateau are a challenge to treat due to the complex geometry of the proximal tibia, important nearby soft tissue attachments, association with concomitant pathologic lesions, and relatively sparse literature providing evidence-based guidelines to assist in clinical decision making.9,10 Surgical treatment options include simple debridement, marrow stimulation techniques with or without adjuncts such as micronized allogeneic cartilage and/or platelet-rich plasma, osteochondral autograft transplantation, and osteochondral allograft transplantation for larger lesions.9,11 Among the most common reasons to perform a tibial cartilage procedure is to address tibial plateau fracture malunion associated with symptomatic posttraumatic arthritis in a young patient.10,12-14
Osteochondral tibial plateau allograft transplantations have been associated with successful outcomes in the few reported case series published in the literature. For example, Ghazavi et al. published the results of 126 cases of osteochondral allograft transplantation for posttraumatic osteochondral defects of the knee, half of which involved the tibial plateau. 14 The authors reported an overall survivorship rate of 95% at 5 years and 77% at 10 years citing that the best results occurred in young patients with unipolar osteochondral defects. Gross et al. described their long-term follow-up of 65 tibial osteochondral allografts performed for failed tibial plateau fractures. 2 Survival analysis showed 95% survival at 5 years, 80% at 10 years, and 65% at 15 years. More recently, Gracitelli et al. assessed the functional outcomes and survivorship of 29 osteochondral allografts performed as a salvage procedure following a tibial plateau fracture. 12 Survivorship was 86% at 5 years and 67% at 10 years.
The above results are encouraging given that total joint arthroplasty was delayed and even avoided in the large majority of patients. As such, it can be concluded that tibial plateau osteochondral allograft transplantation is a viable treatment option for large symptomatic osteochondral lesions of the tibial plateau that are not amenable to more conservative forms of cartilage repair. However, in assessing methods to improve outcomes associated with an osteochondral transfer, proper preoperative planning and accurate size matching of recipient anatomy and donor tissue is likely critical for success. In femoral condyle osteochondral allograft transplantation, for example, it is common to use sagittal and coronal plane measurements to assess geometric matches between donors and recipients. Furthermore, a recent article by Bernstein et al. discussed a technique for evaluating the radius of curvature as an alternative criterion to improve the accuracy of size matching and restore anatomic contour. 15 The authors discuss how the radius of curvature assessment may appropriately identify instances where donor plugs from one compartment can be transplanted to the other compartment or to the contralateral side.
While there are studies that stress the importance of proper sizing of an allograft transplanted to the femoral condyles, we are unaware of studies that offer a detailed approach to matching a donor tibial allograft to a recipient. For instance, in one of the earliest reports of osteochondral tibial plateau allografts, Ghazavi et al. presented no information on how to size the donor graft. 14 Others who have published results on osteochondral tibial plateau transfers stated that donors were matched by size and morphology via measurements on standardized radiographs alone.2,16 And finally, Gracitelli et al. stated that donor and recipients were paired using the mediolateral width of the proximal tibial of the recipient as measured in an anteroposterior standing radiograph and matched to the donor plateau by using a caliper; however, there was no mention of assessing the recipient’s plateau length. 12
To address this issue, the current investigation compared measurements of standardized anatomical landmarks on radiographs and gross anatomic specimens similar to Pollard et al.’s method for sizing a meniscal allograft. 6 In their cadaveric study, standardized plain radiographs established relationships between meniscal allograft tissue and reproducible bony landmarks. With respect to the measured sagittal length of the tibial plateau, Pollard’s group determined that a correction factor of 80% for medial meniscal length and 70% for lateral meniscal length allowed for accurate size matching for meniscal transplants. This technique remains the gold standard for size matching a meniscal allograft. More recently, Jang et al. described a modification to Pollard’s method in an effort to minimize meniscal extrusion. When compared to the conventional technique described by Pollard, Jang et al.’s method reduced total graft size by 5% and found decreased rates of meniscal extrusion without any associated adverse outcomes. 17
The results of the current investigation closely mirror Pollard et al.’s findings for meniscal allograft sizing. For example, the width of an osteochondral tibial as well as an isolated meniscal graft can be accurately measured on an AP radiograph without adjustment. Both meniscal and tibial plateau allografts, however, are oversized if a direct measurement is taken from the lateral radiograph. In the case of tibial plateau osteochondral allografts, we found that the sagittal length of the medial plateau is 90% of the dimensions measured on the lateral radiograph while the lateral plateau is 80%. Given that prior techniques, as described above, failed to adjust their radiographic measurements, it is possible that grafts were oversized in the sagittal plane. Using the average length of medial and lateral plateaus in this investigation as 5.2 cm, this would result in a 5 mm and 10 mm mismatch for the medial and lateral plateaus, respectively. This is additionally worrisome as osteochondral allografts are more commonly performed on lateral than medial plateaus.12,14
This study is limited by the fact that it is a cadaveric investigation and further research will be necessary to evaluate the clinical efficacy of the proposed algorithm. Furthermore, it should be noted that the anatomy of the proximal tibia is often distorted following tibial plateau fracture malunions, which would make accurate radiographic analysis difficult. In this setting, obtaining a contralateral AP and lateral knee radiographs can be used for appropriate sizing. The strength of this study is that it is based on a prior radiographic sizing investigation with a proven track record for successful meniscal allograft transplantation. The proposed algorithm is simple to calculate and uses easily reproducible measurements on standard radiographs.
In conclusion, this is the first investigation to propose an algorithm for sizing a tibial plateau osteochondral allograft. This algorithm considers that the lateral radiograph may oversize the anterior to posterior dimension of these grafts, which could potentially result in early failure. Future prospective investigations examining the clinical effects of this algorithm will help further elucidate this important topic.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kirk A McCullough is a paid consultant to Alliqua, Arthrex, and Stryker. Dr. Christian Lattermann has stock or stock options in Cocoon, is a board or committee member of the International Cartilage Repair Society, and a paid consultant for Joint Restoration Foundation, Samumed, and Vericel. Dr. David Flanigan receives research support from Aesculap/B.Braun, Anika Therapeutics, Cartwheel, Histogenics, Moximed, Musculoskeletal Transplant Foundation, Smith & Nephew, and Zimmer, is a board or committee member for American Orthopaedic Society for Sports Medicine and Arthroscopy Association of North America, and is a paid consultant for Ceterix, CONMED Linvatex, DePuy, Vericel, and Zimmer. Dr. James Fleischli receives research support from Arthrex and Smith & Nephew. The remainder of the authors have no conflicts of interest to report.
Ethical Approval
Ethical approval was not required as this is a cadaveric study.
Informed Consent
Informed consent was not required as this is a cadaveric study.