
Abstract
Objective
To compare the relative effectiveness of intra-articular N-acetyl cysteine (NAC) and hyaluronic acid (HA) on pain, function and cartilage degradation markers in patients with mild to moderate knee osteoarthritis (OA).
Design
We prospectively conducted a clinical trial with 20 patients having a diagnosis of Kellgren-Lawrence grade 2-3 knee OA, and randomly allocated to the HA or NAC groups. Groups were matched on age, sex, and body mass index. Injections of 3-mL HA (Hylan G-F 20) or 3-mL NAC (Asist ampoule) were administered as a single shot. Functional status and pain were evaluated before and after injection, using the Western Ontario and McMaster Universities Arthritis Index (WOMAC) and the visual analogue scale (VAS) scores. Pre- and posttreatment concentrations of serum C-reactive protein (CRP), synovial fluid chondroitin-6-sulfate (C-6S), matrix metalloproteinase-3 (MMP-3), cross-linked C-terminal telopeptide of type 2 collagen (CTX-II), total oxidant status (TOS), and total antioxidant concentration (TAC) were obtained.
Results
WOMAC, VAS scores, and CRP levels were comparable between groups prior to treatment. Both HA and NAC produced comparable reductions in TOS and MMP-3. NAC was more effective in reducing C-6S and CTX-II (P < 0.05). No effects on TAC were noted.
Conclusions
NAC is effective in lowering some cartilage degradation markers, with comparable outcomes to HA for pain and function. NAC could provide a cheaper alternative to HA for intra-articular injection treatment of mild to moderate knee OA. Future placebo controlled trials are warranted to evaluate effectiveness in a larger patient population with a wider range of age and OA severity.
Introduction
Osteoarthritis (OA) is a progressive degenerative disorder of cartilage, characterized by cartilage destruction, subchondral sclerosis, and the formation of osteophytes. The destruction of joint cartilage can cause joint pain, decrease joint range of motion, and cause varying degrees of impairments in function. Because of the high loads borne by the knee joint during activities of daily living and mobility, the knee is the most frequent site of OA. A range of conservative and surgical treatments are available in knee OA. 1 Most of the conservative treatment options have limited effect. Intra-articular injections of hyaluronic acid (HA) are commonly used with the aim of providing pain relief and improve functional status.2-4 Effectiveness of HA is being challenged, however, because of its limited anti-inflammatory role.
The role of free-oxygen radicals (FORs) in the pathogenesis of OA has increasingly been considered. FORs are toxic chemicals, promoting the destruction of the cartilage matrix, apoptosis of chondrocyte cells and synovial inflammation, resulting in destruction of joint cartilage and decreased viscosity of synovial fluid.5,6 As cartilage destruction causes the release of a range of biochemical markers, levels of these markers reflect the rate of cartilage turnover and, therefore, are predictive of the severity of OA, the effectiveness of a treatment and, ultimately, prognosis, as well as to inform the development of new cartilage-protecting drugs.7,8
N-Acetyl cysteine (NAC) is a strong antioxidant and anti-inflammatory agent with few side effects reported. 9 Experimental and tissue culture studies have provided evidence of the effectiveness of NAC in clearing FORs and, consequently, slowing the process of cartilage destruction, decreasing synovial inflammation and reducing pain producing cytokines.10-16 Factors involved in the pathogenesis of OA are cartilage apoptosis, release of proteases, and production of inflammatory cytokines such as interleukin (IL)-1β and tumor necrosis factor (TNF)-α. 17 Chondrocyte apoptosis has been correlated with the severity of OA and is involved in the progression of the disease. 18 Chondrocyte apoptosis has been reported to occur in response to various stimuli, including nitric oxide (NO). NO is present at high levels in OA cartilage and may play an important role in the progression of OA. 19 Studies of the mechanisms involved in these effects have indicated that cell damage occurs when NO interacts with reactive oxygen species (ROS). Exogenous NO induces ROS within cells, resulting in cytotoxicity. 20 As a result, ROS damages DNA, protein, and other molecules in the cell, finally leading to apoptosis. 21 Considering the pathogenesis of OA and the molecular action mechanisms of NAC, we hypothesized that NAC may be used therapeutically as an alternative treatment modality in the treatment of knee osteoarthritis.
Credible evidence regarding the application of NAC for the clinical management of knee OA is not currently available. Therefore, the aim of our study was to identify and compare the relative effectiveness of intra-articular NAC and HA on pain, function and cartilage degradation markers in patients with mild to moderate knee OA. NAC was chosen as an alternative modality of treatment because it has in vitro anti-inflammatory, antioxidant, and chondroprotective effects and lower cost.10-16
Patients and Methods
Prospective participants for our small, single site, pilot study were patients receiving treatment for knee OA at our institution, between April 2013 and October 2013, selected based on the following inclusion criteria: confirmed diagnosis of primary knee OA according to the American College of Rheumatology (ACR) OA criteria 22 ; ≥40 years of age; Kellgren-Lawrence (KL) grade 2 or 3 OA quantified from anterior-posterior and lateral weightbearing radiographs, obtained bilaterally; symptomatic for ≥6 months; <1 week use of painkillers, muscle relaxants, or nonsteroidal anti-inflammatory drugs (NSAIDS); <2 months’ use of oral, intravenous, or intramuscular steroids; no history of intra-articular injection or physical therapy in the previous 1 year; no history of knee trauma or surgery in the previous 6 months; no clinical findings of neurological deficit of the lower limbs; and no history of systemic disease.
Twenty patients met the inclusion criteria and were enrolled in our trial. All participants provided informed consent including all possible side effects and no previous use of NAC with a dosage that had not been tested for safety and toxicity or long-term effects on cartilage in human joints before. The study protocol received clearance from the Erciyes University research ethics board. Twenty patients were divided blindly into 2 groups by sealed envelope technique as HA injection group (group HA) or the NAC group (group NAC). Prior to the start of treatment, biochemical and radiographic assessments were completed for all study participants, including: complete blood count levels, wide biochemistry, erythrocyte sedimentation rate, C-reactive protein (CRP) levels, rheumatoid factor, and radiographs to confirm KL grading. Age, sex, height, weight, and body mass index (BMI) were recorded for all patients.
Patients in group A received intra-articular injections of 3 mL of HA (Hylan G-F 20 24 mg/3 mL) as a single shot. Group B received 3 mL of NAC (Asist ampoule 300 mg/3 mL), according to the same schedule. All injections and aspirations performed by the first author (2 years of experience as orthopedic surgeon). Aspiration of synovial fluid was performed before injections and at 6 weeks after the injections. Aspiration and injection was performed under sterile conditions, using a lateral approach with patients in a supine position under ultrasonographic guidance. A 1.7-mm cannulated dry syringe was used for all procedures. Patients were encouraged to maintain a program of isometric strength training for the quadriceps muscle and their activities of daily living.
Clinical Assessment
The Western Ontario and McMaster Universities Arthritis Index (WOMAC) (WOMAC 3.1, 11-box Numerical Rating Scale format, Turkish version) and the visual analogue scale (VAS) were completed before the start of treatment and 6 weeks after the injection, and used to evaluate patient satisfaction, decrease in pain and functional status.
Biochemical Assessment
Serum CRP levels and synovial concentrations of inflammatory and cartilage degradation biomarkers were measured before injection and at 6 weeks after the injection. Serum CRP levels were used to exclude infectious or inflammatory etiologies. Synovial fluid samples were centrifuged 10 minutes at 4000 rpm and supernatants collected. All the samples controlled for hemolysis microscopically. All supernatants were transferred to Eppendorf tubes, with a minimum volume of 0.3 mL in each tube, and maintained at −80°C until analysis.
The following biochemical analyses were conducted on samples: Enzym-linked immunosorbent assay (ELISA) test kit was used to determine levels of chondroitin-6-sulfate (C-6S) (SunRedBio, 01-12-1896 code number kit), matrix metalloproteinase-3 (MMP-3) (Boster Biological technology, EK0461 code number kit), and cross-linked C-terminal telopeptide of type 2 collagen (CTX-II) (USCN Life, E0686h code number kit); and total oxidant status (TOS) and total antioxidant concentrations (TAC) levels were determined by calorimetric test (Immundiagnostik Company KC 5100 and KC5200 code number kits). All level measurements were detected using the Epoch microplate reader. Measurements of TAC and TOS levels were performed using a colorimetric method, which was first described by Erel. 23
Statistical Analysis
All data were expressed as a mean ± standard deviation. The distribution of numeric variables was evaluated using the Shapiro-Wilk test. Between-group differences were evaluated using chi-squared test for categorical variables and Mann-Whitney U test for nonparametric variables. Wilcoxon rank test was used to evaluate change in measured variables, before and after injections. All analyses were performed with SPSS version 15 for Windows (SPSS Inc, Chicago, IL, USA), with a P value of <0.05 indicating statistical significance.
Results
The distribution of sex, age, weight, BMI, and KL grade was comparable for both groups (P > 0.05): 8 females and 2 males in each group; mean age of 54.6 ± 2.7 years for the HA group and 55.0 ± 3.6 years in the NAC group; mean BMI of 32.7 ± 1.4 kg/m2 in the HA group and 32.0 ± 1.5 kg/m2 in the NAC group; and 5 patients with KL grade 2 knee OA and 5 with grade 3 in each group. The full course of intra-articular injections was completed for all patients in both groups with no local or systemic reactions to the injections or side effects. Mean aspiration fluid volume was 1.38 ± 0.22 mL (median = 1.3, CI = 0.35-2.08). All samples had clear appearance and high viscosity. In the microscopic evaluation, mean white blood cell count was 677 ± 233 per microliter (median = 600, CI = 570-629.7) with 50% of polymorphonuclear leukocytes.
A significant decrease in VAS score was identified after the course of injections for both groups (P < 0.05) (
Changes in VAS Score Before and After Injections.
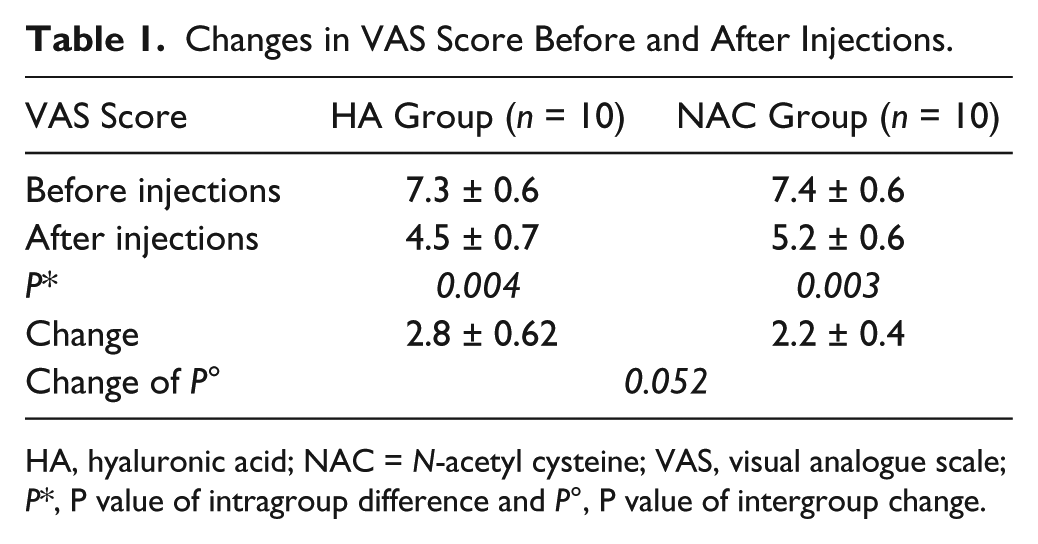
HA, hyaluronic acid; NAC = N-acetyl cysteine; VAS, visual analogue scale; P*, P value of intragroup difference and P°, P value of intergroup change.
Intra-articular injections of both HA and NAC yielded significant improvement in total WOMAC score, as well as on the WOMAC domains of stiffness and physical function (P < 0.05) ( Table 2 ). WOMAC scores were comparable between groups before and after injections.
Changes in WOMAC Scores Between the 2 Groups.
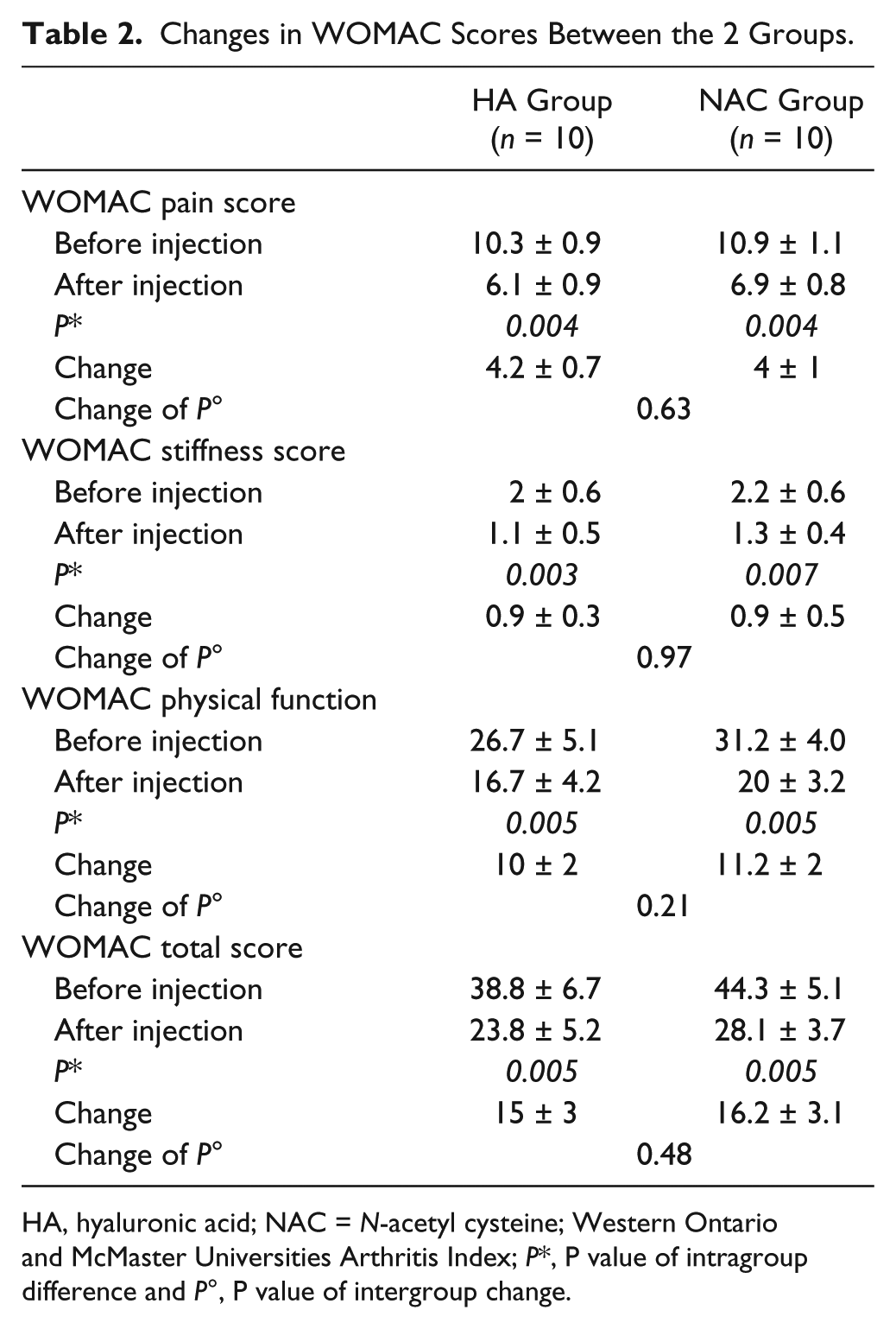
HA, hyaluronic acid; NAC = N-acetyl cysteine; Western Ontario and McMaster Universities Arthritis Index; P*, P value of intragroup difference and P°, P value of intergroup change.
Levels of CRP significantly decreased in both groups after injection (P < 0.05) ( Table 3 ). There were no between-group differences in CRP levels, before or after treatment (P > 0.05).
Comparison in CRP Level Changes of the 2 Groups.
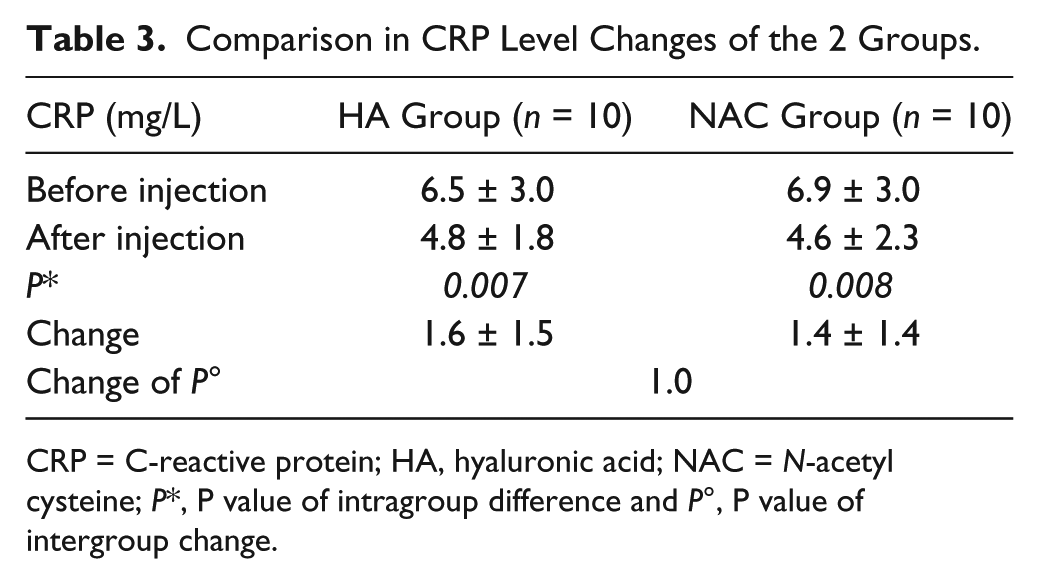
CRP = C-reactive protein; HA, hyaluronic acid; NAC = N-acetyl cysteine; P*, P value of intragroup difference and P°, P value of intergroup change.
In terms of synovial fluid analysis, TOS and MMP-3 concentrations decreased significantly in both groups after injection (P < 0.05) ( Table 4 ). Synovial fluid concentrations of C-6S and CTX-II decreased in both groups after injection, reaching statistical significance in the NAC group (P < 0.05).
Synovial Fluid Changes of Each Group.
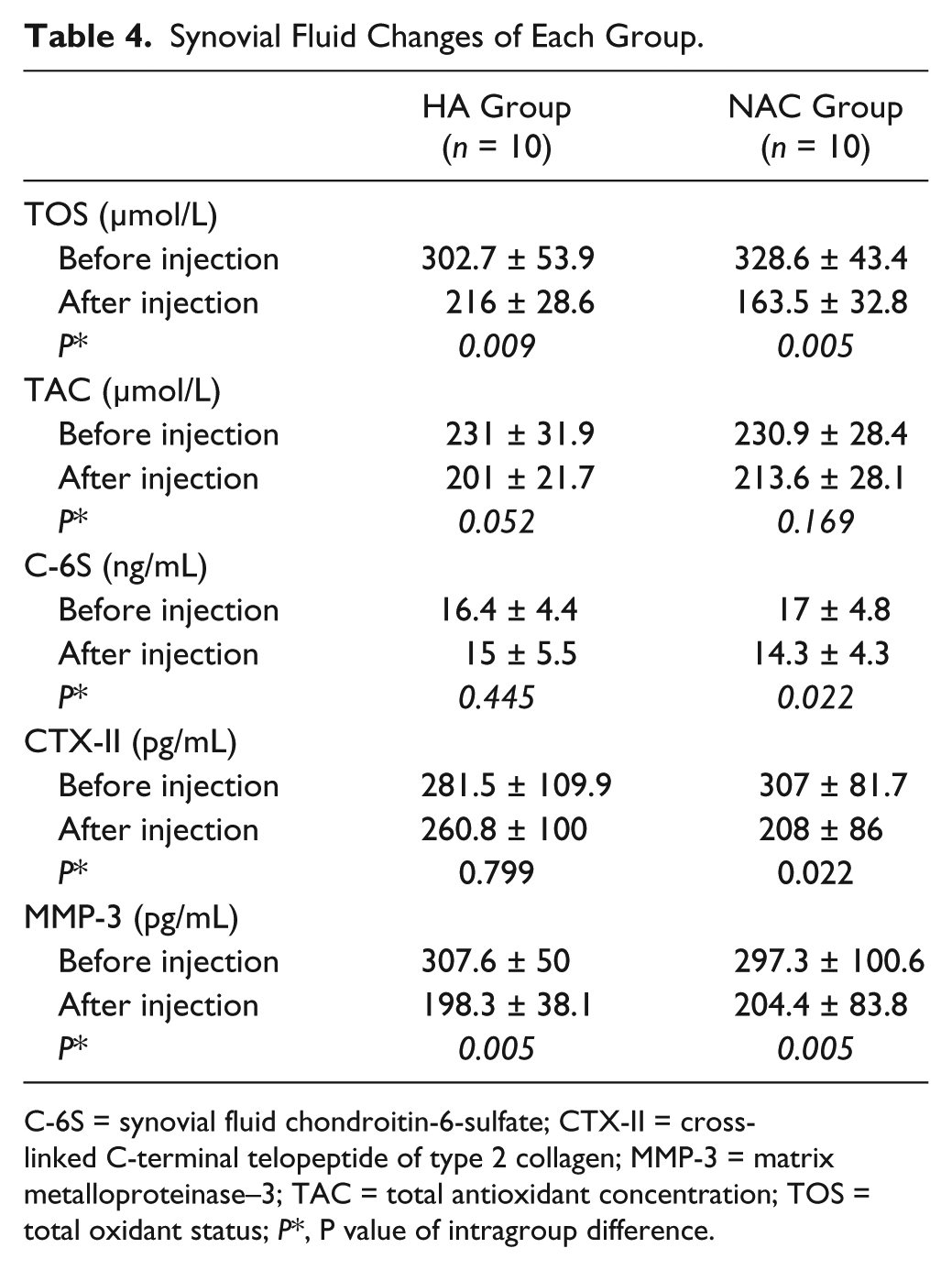
C-6S = synovial fluid chondroitin-6-sulfate; CTX-II = cross-linked C-terminal telopeptide of type 2 collagen; MMP-3 = matrix metalloproteinase–3; TAC = total antioxidant concentration; TOS = total oxidant status; P*, P value of intragroup difference.
TAC was comparable between groups before and after injections: HA group 231.0 ± 31.9 μmol before and 201.0 ± 21.7 μmol after injections; NAC group, 230.9 ± 28.4 μmol before and 213.6 ± 28.1 μmol after injections. There was no significant effect of either HA or NAC injections on TAC levels (P > 0.05). NAC injection, however, produced a greater decrease in TOS concentrations, compared to HA injection (P < 0.05, Table 5 ).
Comparison of the 2 Groups for Synovial Fluid Changes.
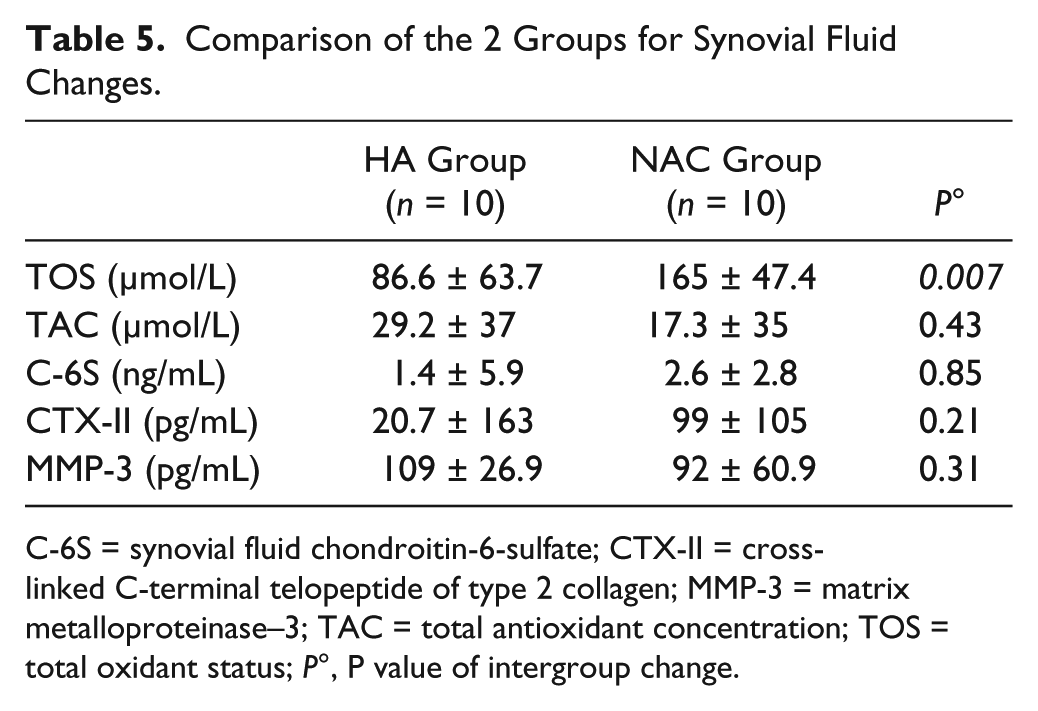
C-6S = synovial fluid chondroitin-6-sulfate; CTX-II = cross-linked C-terminal telopeptide of type 2 collagen; MMP-3 = matrix metalloproteinase–3; TAC = total antioxidant concentration; TOS = total oxidant status; P°, P value of intergroup change.
Discussion
The purpose of this study was to identify and compare the relative effectiveness of intra-articular NAC and HA on pain, function, and cartilage degradation markers in patients with mild to moderate knee OA. Our results showed that both HA and NAC produced comparable reductions in TOS and MMP-3. NAC was more effective in reducing C-6S and CTX-II (P < 0.05). Also, intra-articular injections of both HA and NAC yielded significant improvements in VAS and total WOMAC scores, as well as on the WOMAC domains of stiffness and physical function (P < 0.05). Both HA and NAC produced significant, and comparable, improvements in pain and functional scores.
NAC may be effective on progression of knee osteoarthritis. The aim of OA treatment is to relieve pain and increased joint, as well as overall, function. Intra-articular injection of HA is a widely used treatment for knee OA worldwide. OA is a chronic degenerative disease characterized by destruction of articular cartilage, leading to progressive pain and impairments in function.
The pathogenesis of OA is related to chondrocyte death, loss of matrix proteoglycans, and disruption of the balance between cartilage formation and resorption. 24 Primary osteoarthritis is the most common form of knee OA, with age being the most potent risk factor of its incidence. According to the ACR criteria, the lower age limit for OA diagnosis is 38 years. 25 The age of our study group conformed with this minimum diagnostic criterion for OA, with a mean age of 54.6 years of the HA group and 55.0 years for the NAC group. The prevalence of knee OA is also higher in women. 26 Again, our study group was representative of the general population with OA, with an 80% proportion of females in both groups. The relationship between obesity and OA has been well documented, with the Framingham study providing strong evidence for BMI being predictive of future OA. 25 Our study group was representative of the general OA population, with a mean BMI of 32.7 kg/m2 for the HA group and 32.0 kg/m2 for the NAC group, which is within the BMI range of 30.0 to 34.9 kg/m2 commonly interpreted as being indicative of obesity. Therefore, our study groups were homogenous and compatible with principle demographic variables of the OA within the general population.
There is evidence of the effectiveness of intra-articular HA in providing pain relief and improving function, for at least 6 months after injection. Corrado et al. 27 reported a significant decrease in pain, both at rest and with activity, 35 days after HA injection. A meta-analysis of randomized controlled trials provided evidence for decreased pain, at rest and with activity, and improved function status after HA injection. However, the effectiveness of HA has been reported to be limited in patients older than 65 years and in patients with higher grades of OA. 28 Another second meta-analysis of 76 studies provided head-to-head comparison of HA with a placebo group, as well as with steroid use, physical therapy and exercise, with results of intra-articular HA being superior to placebo. 29 Based on this evidence, the authors concluded that HA is an effective treatment method for knee OA.
HA injection treatment is a relatively expensive method in comparison with NAC injection. According to our results, NAC injection was found effective as HA injection in the treatment of mild to moderate knee osteoarthritis. But, our study population was relatively small. Future randomized controlled comparative studies with larger populations and varying OA degrees needed to assess effectiveness and cost of NAC injection therapy.
In vitro biochemical studies have shown the concentration- and molecular weight–dependent effectiveness of HA injections in inhibiting IL-1-induced prostaglandin E2 (PGE2), bradykinin, and arachidonic acid release, as well as positively modifying leukocyte function, as well as inflammatory cell function, migration, chemotaxis, and phagocytosis.30-32 The positive effects of HA in providing pain relief and improving functional status in our patients supports these mechanisms.
Intra-articular HA injection is recommended for patients with KL knee OA grades of 2 and 3. 41 High molecular weight HA is the preferred preparation with high concentration and high molecular weight HA enhancing the lubrication and shock absorption capacity of the articular cartilage. 27 In addition, high molecular weight HA induces endogen HA synthesis and reduces the concentration of cartilage damage biomarkers in synovial fluid.3,33,34 It is based on this evidence that we used a high molecular weight HA (Hylan G-F 20) in our study.
NAC, which is a glutathione precursor, is a strong antioxidant agent with thiol group, directly neutralizing FORs. In addition, NAC act as an indirect antioxidant, by entering the cell through plasma membrane and reacting with glutamic acid and glycine to generate intracellular glutathione. 10 Glutathion is the most abundant antioxidant in cells. 42 Because of its antioxidative properties, glutathione can control cell damage. Glutathione in chondrocytes also plays crucial role in their survival. 15 Several in vivo and in vitro studies evaluating the anti-inflammatory effect of NAC on human articular tissues have provided evidence of the effectiveness of NAC in neutralizing FORs by inducing a TNF-α and IL-1β downregulation and inhibiting PGE2 synthesis and COX-2 expression.10,11,35,43 We chose NAC as an alternative treatment modality because of its in vitro antioxidant, anti-inflammatory, and chondroprotective effects. Pain relief and functional status improvements in our patients after NAC injections support anti-inflammatory mechanisms. Also, decreased TOS and cartilage degradation markers after NAC injections support antioxidant and chondroprotective mechanisms. Nakagawa et al. 10 reported decreased cartilage apoptosis and cartilage degeneration in experimental OA rat models after an 8-week protocol of intra-articular, 5-mg injection of NAC. It is based on this current evidence, considering the volume of the human knee joint and possible side effects and toxicity, that we used lowest available intravenous NAC concentration of 300 mg/3 mL intra-articular (Asist ampoule).
CRP levels may be elevated in patients with OA. 36 In a study of 105 female patients with knee OA, patients with bilateral knee OA had higher CRP levels than patients with unilateral knee OA. 37 In our study, we identified a mild elevation in CRP levels in both the HA and NAC groups. (HA group, 6.5 ± 3.0 mg/L; NAC group, 6.9 ± 3.0 mg/L). Both HA and NAC injections were effective in lowering serum CRP levels. Lo et al. 36 reported decreased serum CRP levels after intra-articular HA and indomethacin injection in an experimental OA model. In their clinical study, Palmieri et al. 32 reported decreased serum CRP levels after high molecular weight HA injections in patients with KL grade 2 and 3 knee OA. In our study, we confirmed a statistically significant decrease in serum CRP levels after both HA and NAC intra-articular injections.
OA molecular predictors (OMP) provide a proxy measure of cartilage turnover and, therefore, are useful in the follow-up of patients, determination of prognosis, and development of new protective drugs.7,8 In our study, we quantified C-6S, MMP-3, CTX-II, TOS, and TAC levels to evaluate the effectiveness of intra-articular NAC injection therapy efficiency. We identified that both HA and NAC significantly decreased synovial fluid TOS concentrations. However, NAC decreased TOS concentration to a greater extent than HA (P < 0.05). As the extent of change in TAC concentration was comparable for both HA and NAC injections, we postulated that the significant effect of NAC on TOS is indicative of the antioxidant capacity of NAC.
Matrix metalloproteinase enzymes (MMPs) play an important role in cartilage matrix degradation. MMP-3 has wide substrate specificity and therefore, contributes significantly to the degradation of type 2 collagen. Several studies have reported elevated MMP-3 concentrations in synovial fluid and cartilage tissue in patients with OA.7,32,34,38 In an experimental OA model, MMP-3 levels decreased after HA injection. 11 In another clinical study, synovial fluid C-6S levels decreased after five intra-articular injections of HA. 39 Conrozier et al. 40 reported decreased urine CTX-II levels after intra-articular HA injections. Using in vivo models, Morin et al. 14 reported a downregulation of TNF-α- and IL-1β-dependent MMP-3 gene expression after NAC injection. Homandberg et al. 35 further confirmed an effect of NAC on TNF-α, IL-1, and IL-6 catabolic cytokines, as well as an indirect decrease in MMP-3 synthesis. Interestingly, in our study, we identified significant decreases in the MMP-3 concentration in synovial fluid after intra-articular HA injection (P < 0.05). HA did not decrease concentrations of C-6S and CTX-II concentrations (P > 0.05). By comparison, intra-articular NAC injections produced a significant decrease in concentrations of TOS, MMP-3, C-6S, and CTX-II concentrations in synovial fluid (P < 0.05). We could not explain why NAC decreased certain cartilage degradation and inflammation markers but not others. Based on these results, we conclude that NAC may be more effective than HA in decreasing proteoglycan and collagen degradation, which would provide favorable outcomes in the treatment of OA. Also, NAC provides a cheaper treatment alternative in mild to moderate knee OA.
This study is the first pilot study assessing the effectiveness of intra-articular NAC injection in knee OA. The main limitation of this study was relatively small number of participants because of the funding restrictions. Also there was no placebo control group. Studies with larger placebo controlled patient groups may warrant possible clinical use of NAC in the treatment of knee OA.
Conclusion
Based on the clinical and biochemical outcomes of our study, we suggest that NAC may be as an effective and cheaper alternative to HA in slowing the process of progressive cartilage destruction and improving clinical and functional status. NAC would provide a further advantage of lowering the cost of intra-articular OA treatment, compared to HA. Placebo-controlled trials are warranted to provide higher level of evidence regarding the possible clinical role of intra-articular NAC in the treatment of patients with knee OA.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Erciyes University Scientific Research Ethical Board (2013/579).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Erciyes University Scientific Research Project Committee: TTU-2013-4982