
Abstract
High-resolution 3-dimensional cartilage-specific magnetic resonance imaging (MRI) was performed at 3 T to test the following hypotheses: (1) there is a nonuniform cartilage thickness distribution both on the proximal humerus and on the glenoid surface and (2) the glenohumeral joint as a combined system is congruent with the level of the joint cartilage surface without substantial radial mismatch. Inclusion of 38 volunteers (19 females, mean age 24.34 ± 2.22 years; range 21-29 years) in a prospective study. Measurements of: cartilage thickness in 3 regions and 3 zones; radius of both circles (glenoid and humeral cartilage) for congruency calculation using 3-T MRI with 3-dimensional dual-echo steady-state sequence with water excitation. A homogenous mean cartilage thickness (1.2-1.5 mm) and slightly higher values for the glenoidal articulating surface radii both in the mid-paracoronar section (2.4 vs. 2.1 cm, P < 0.001) and in the mid-paraaxial section (2.4 vs. 2.1 cm, P < 0.001) compared with the humeral side were observed. The concept of a radial mismatch between the humeral head and the glenoid in healthy human subjects can be confirmed. This study provides normative data for the comparison of joint cartilage changes at the shoulder for future studies.
Introduction
As is well known, the shoulder joint is an almost nonconstrained joint, gaining its stability from dynamic forces rather than from structural properties. However, even small variations in the anatomy such as glenoid cartilage and bone loss can cause substantial functional changes, including instability and degeneration, which can eventually result in early osteoarthritis (OA).1,2
Since the pioneering work of Walch and Boileau that provided essential basic data about the anatomy of the proximal humerus (and its variability among individuals) and the size and orientation of the glenoid cavity, in particular in the axial plane, including patterns of morphological changes in OA, the anatomy of the glenohumeral joint as a combined system with 2 determinant parts has moved into the focus of attention.3-8 In this matter, 3-dimensional (3D) imaging and computational science have opened the door not only to a new understanding of joint relationships and kinematics but also for the treatment of altered anatomy such as glenoid bone loss.4,9,10 Yet, most imaging studies and 3D reconstruction techniques are based on data derived from high-resolution computed tomography (CT) scans, which reflect the bony anatomy rather than the cartilaginous joint surface itself, which is the domain of modern magnetic resonance imaging (MRI).4,9-20 Therefore, since the fundamental measurements of cartilage thickness and distribution, which were performed using histological slices or cadaver specimens and a rule more than 30 years ago, there is a lack of information about the particular cartilage distribution and thickness both at the proximal humerus and in the glenoid cavity.21-24
The objective of this study is to provide normative data about the thickness distribution of hyaline cartilage in healthy human subjects at the glenohumeral joint. Therefore, high-resolution 3D cartilage specific MRI was performed at 3 T to confirm or refute the following hypotheses: (1) there is a nonuniform cartilage thickness distribution both on the proximal humerus and on the glenoid surface and (2) the glenohumeral joint as a combined system is congruent with the level of joint cartilage surface without substantial radial mismatch.
Materials and Methods
Study Population
This study was approved by the local ethics committee. The principles of the study were carefully explained to all volunteers and a written informed consent was obtained prior to participation. Thirty-eight volunteers (19 females, 19 males, mean age 24.34 ± 2.22 years, range 21-29 years) were included in this prospective study (20 left and 18 right shoulders). Without exception, all participants were in good health, and no volunteer demonstrated any disorder or abnormalities of the glenohumeral joint. Subjects older than 30 years and those involved in high-level sports were excluded a priori to reduce age effects and to minimize the risk of confounding by including undiagnosed cartilage damage in our evaluation.
Magnetic Resonance Imaging
Magnetic resonance imaging of the shoulder was performed with a whole-body 3-T system (Magnetom Trio, Siemens Healthcare, Erlangen, Germany) using a flexible 4-channel body matrix phased-array coil. Examination in supine position with the arm at their side in neutral rotation in a stable position using sponges and adjustable straps. The MRI protocol included a 3D dual-echo steady-state (DESS) sequence with water excitation for morphological cartilage assessment. The DESS sequence combines 2 gradient echoes separated by a refocusing pulse into a single image that increases the signal intensity of both articular cartilage and synovial fluid. 25 Details of the imaging parameters are provided in Table 1.
Sequence Parameters.
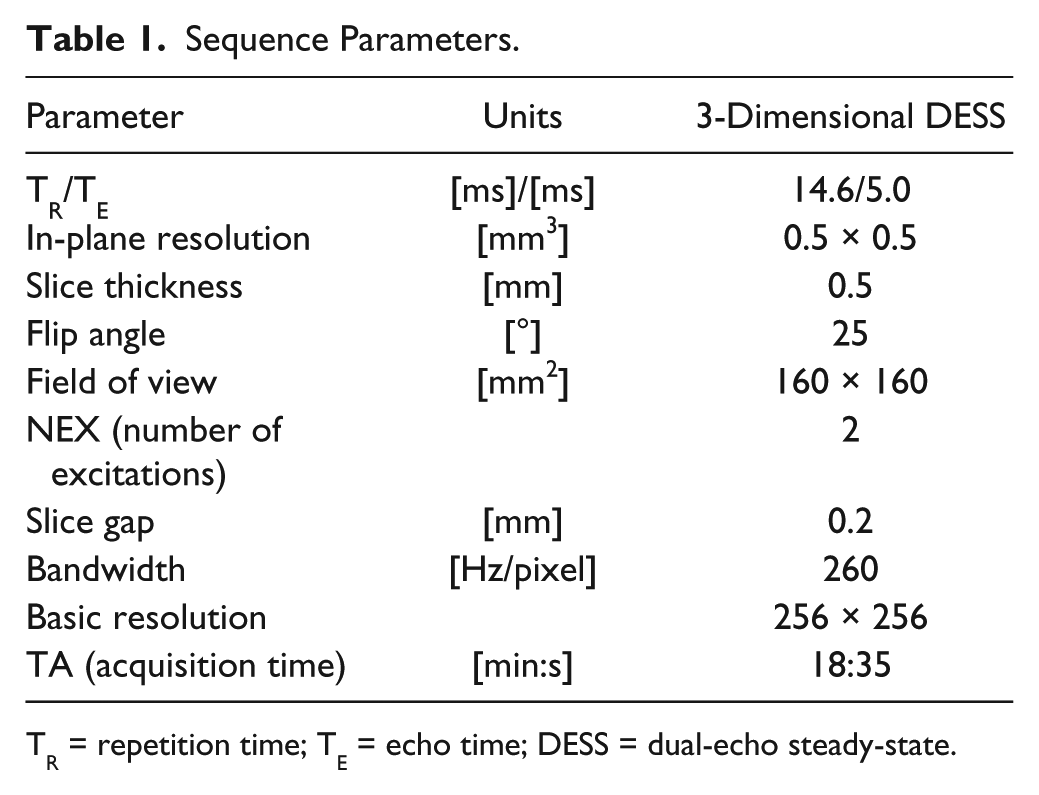
TR = repetition time; TE = echo time; DESS = dual-echo steady-state.
Image Analysis
The 3D DESS data sets were transferred to a Leonardo workstation (Siemens Medical Solutions, Erlangen, Germany) to perform further analyses. From each 3D data set, coronal oblique reformats with a slice thickness of 0.5 mm perpendicular to the glenoid surface were generated using multiplanar reconstruction (MPR; Fig. 1 ). Of these DESS reformats, 3 reformats were selected to assess the glenohumeral cartilage at 3 sections of the joint: (1) anterior, (2) middle, and (3) posterior. Within each section, cartilage thickness measurements were performed on the glenoid and humeral cartilage superiorly, centrally, and inferiorly.
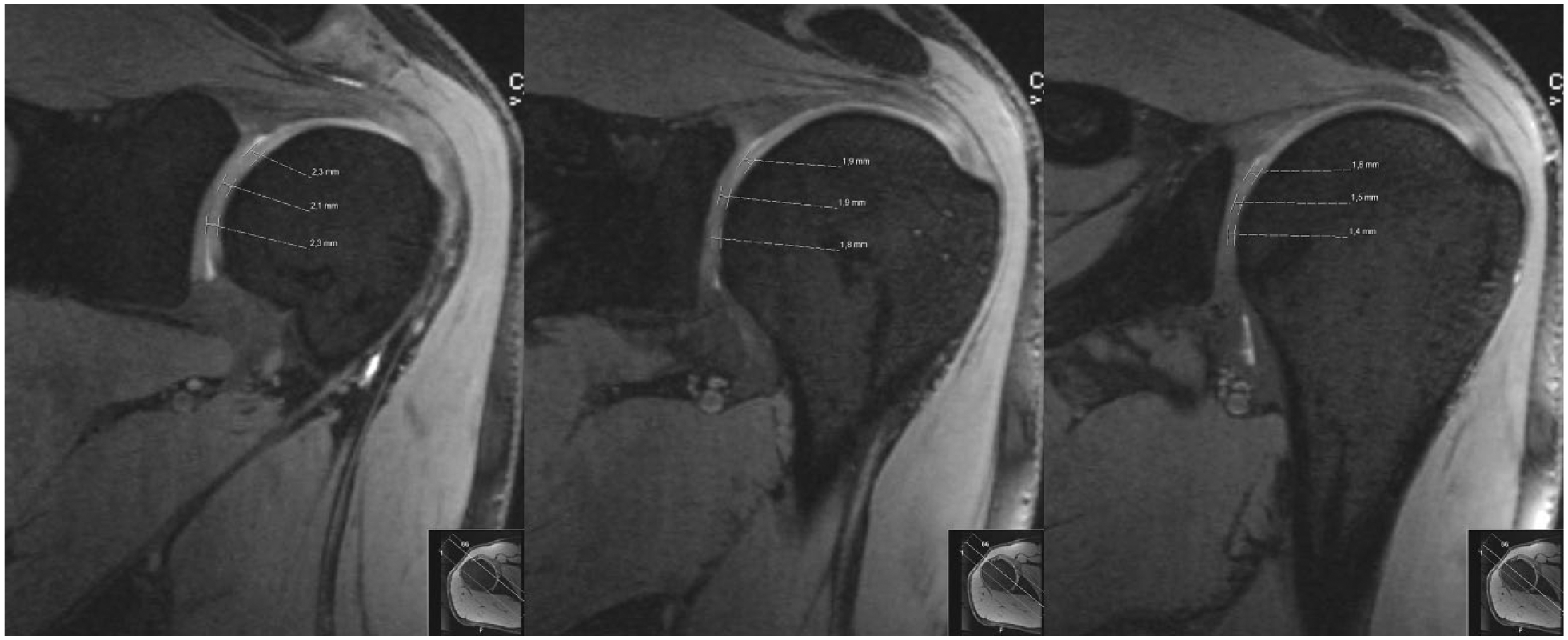
A measurement of cartilage thickness in the anterior (left), middle (middle) and posterior (right) paracoronar reformats (in this example of the humeral head cartilage). In each section, cartilage thickness was measured superiorly, centrally and inferiorly.
To analyze if the glenohumeral joint as a combined system is congruent at the joint cartilage surface level without substantial radial mismatch, a region of interest (ROI) from the head of the humerus was laid in the articular surfaces of the glenoid and humeral cartilage in the paracoronal and paratranversal reformats. Half of the diameter of the ROI was determined to measure the vertical and horizontal radius in the paracoronar and paratransversal slices. The radius of both circles, that is, the glenoid and humeral cartilage, were analyzed in the congruency calculation ( Fig. 2 ).
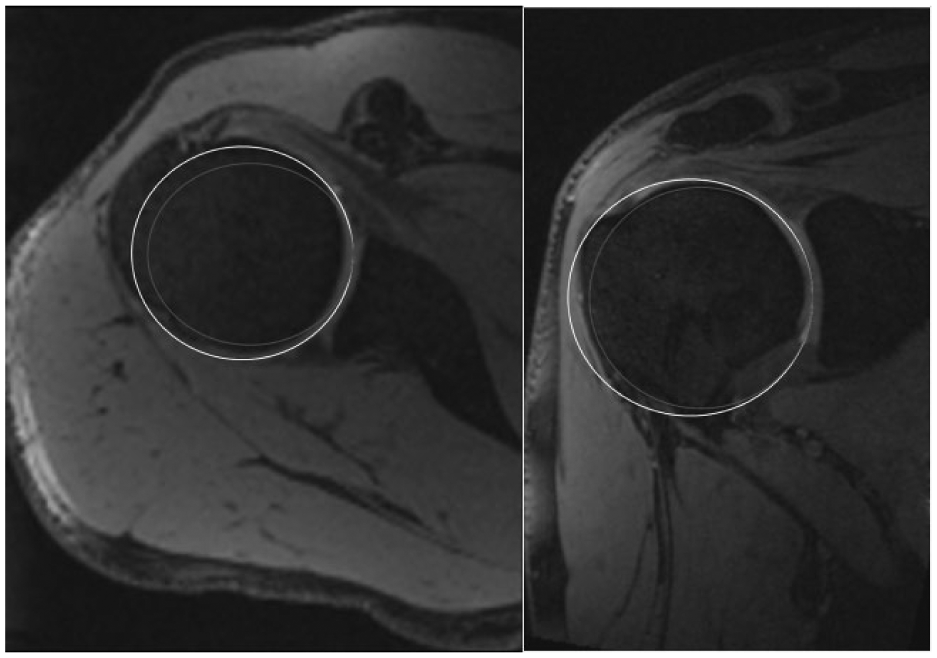
Radius measurements of glenoidal (white) and humeral (red) shoulder joint cartilage in paraxial (left) and paracoronar (right) slices.
All primary 3D DESS measurements were performed by 1 radiologist with 5 years of experience in musculoskeletal imaging, whereas for the reliability assessment, the analysis was repeated by the former and by a second observer (an orthopedic consultant with 9 years of experience in musculoskeletal imaging) in 10 randomly selected volunteers.
Statistical Analysis
SPSS software (Version 22.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. Cartilage thickness and radius values were reported as means ± standard deviations (SD), median, value range, and 95% confidence intervals. The normality of data was tested by visual inspection using boxplots and scatterplots and statistically using the Kolmogorov-Smirnov and Shapiro-Wilk tests. As the normality assumption was uncertain in portions of the data, Friedman’s test with post hoc analysis was used to identify statistically significant differences between the cartilage thickness in various regions of the glenoidal and humeral cartilage and the radius of the articulating glenoidal and humeral head surface. Interobserver reproducibility of the cartilage thickness and radius measurement was quantified with the intraclass correlation coefficient (ICC) using a pairwise correlation model with absolute agreement. P values less than 0.05 were considered to be statistically significant.
Results
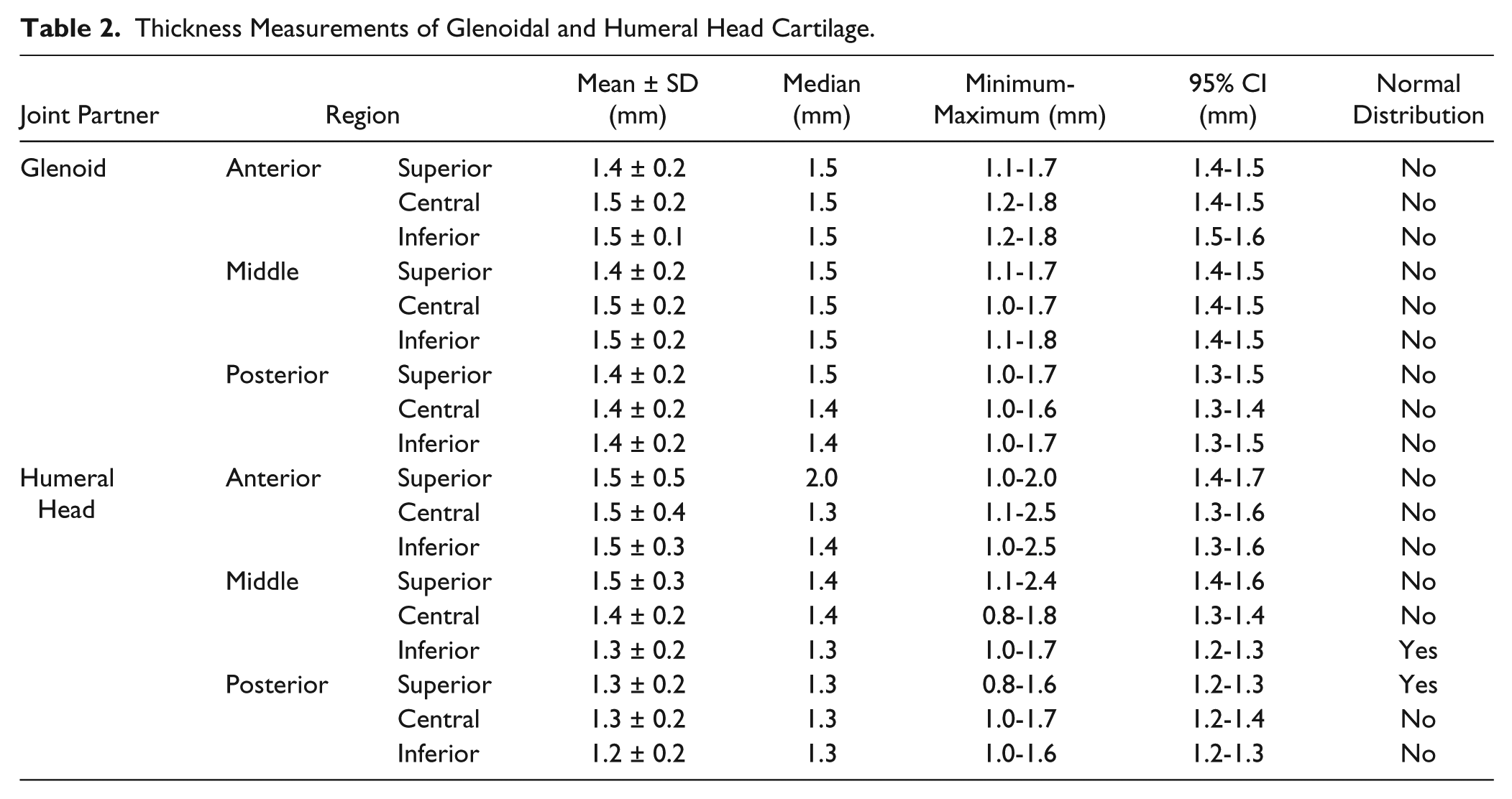
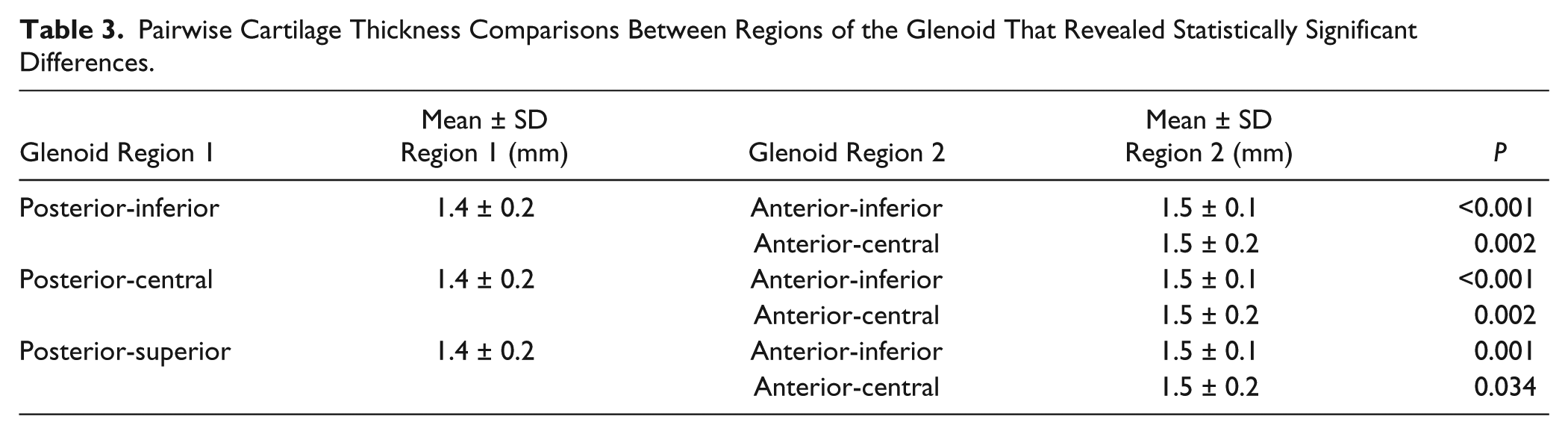
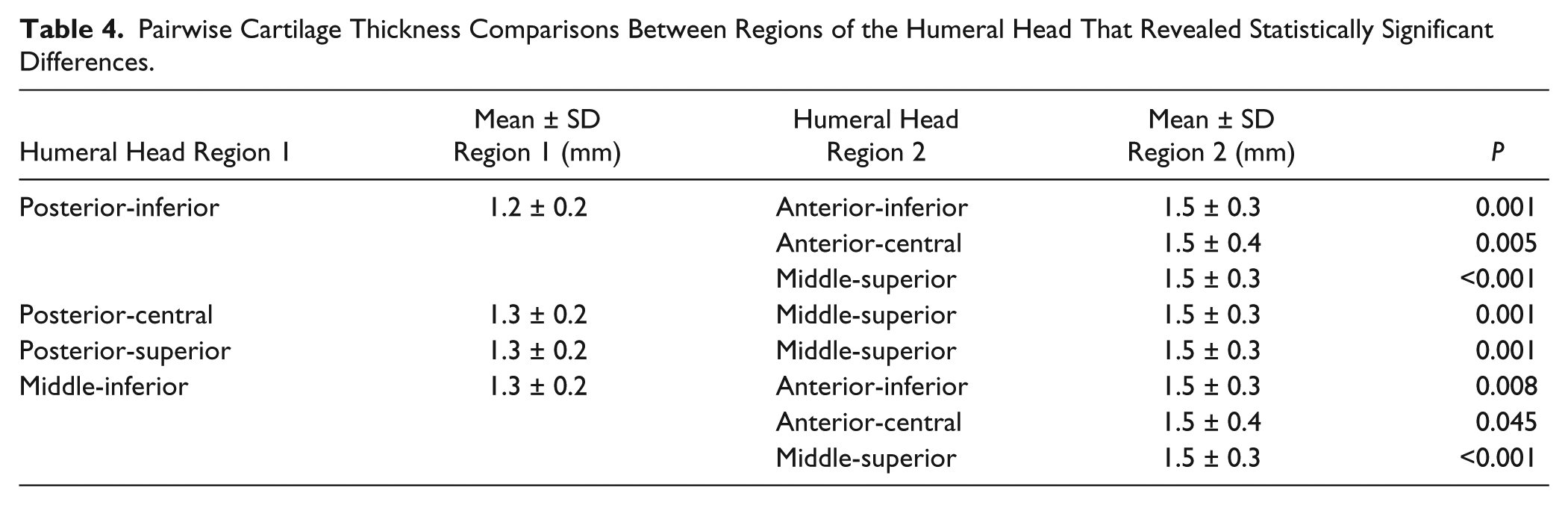
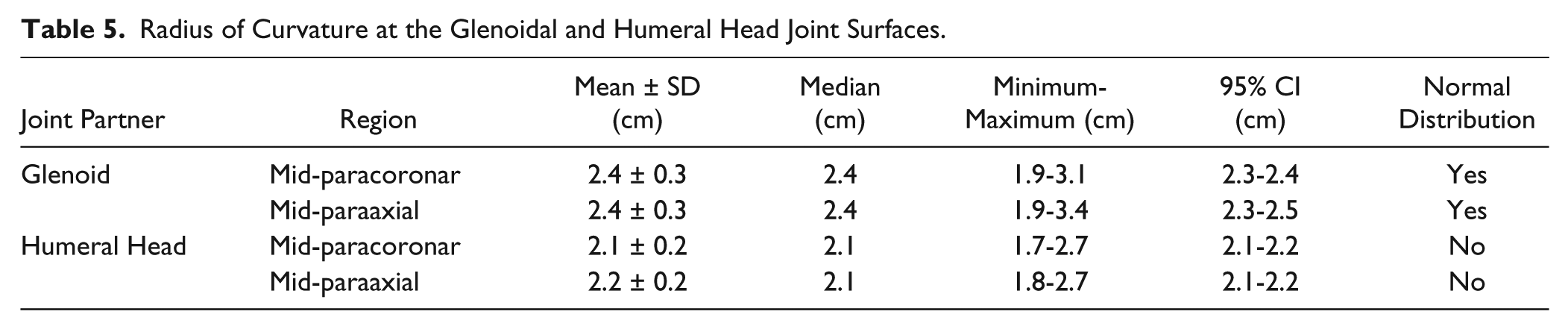
The cartilage thickness values in the posterior region of the humeral head were slightly lower when compared with those in other aspects of the glenohumeral joint (Tables 2-4). Otherwise, the difference in the cartilage thickness among various regions was clinically negligible (mean cartilage thickness ranging from 1.2 to 1.5 mm). Radius measurements (Table 5) revealed slightly higher values for the glenoidal articulating surface both in the mid-paracoronar section (2.4 vs. 2.1 cm, P < 0.001) and in the mid-paraaxial section (2.4 vs. 2.1 cm, P < 0.001) compared with the humeral side. ICC analysis indicated a high degree of interobserver reproducibility in the cartilage thickness (ICC = 0.788, P < 0.001) and radius (ICC = 0.971, P < 0.001) measurements.
Thickness Measurements of Glenoidal and Humeral Head Cartilage.
Pairwise Cartilage Thickness Comparisons Between Regions of the Glenoid That Revealed Statistically Significant Differences.
Pairwise Cartilage Thickness Comparisons Between Regions of the Humeral Head That Revealed Statistically Significant Differences.
Radius of Curvature at the Glenoidal and Humeral Head Joint Surfaces.
Discussion
The most striking result of our study is the remarkable difference in joint surface radii between the humeral head and the glenoid both in the frontal and axial planes. The differences in the frontal plane are 3 ± 0.3 mm and 2 ± 0.3 mm in the axial plane mean that (1) there is a radial mismatch between the flatter glenoid surface and the more curved humeral head and (2) this mismatch is greater in the frontal than in the axial plane (the ratio between the radius of the humeral head and the glenoid is 0.875 in the frontal and 0.92 in the axial plane). Although the absolute values appear to be small, they are in fact very relevant because they underline the biomechanical theory that the glenohumeral joint represents a force-locked dimeric ball-and-socket joint. 26 Early joint replacement pioneers such as Charles Neer designed their components with a high degree of conformity based on the assumption of the “ball and socket” principle that was widely accepted at that time.27-32 A quantitative analysis of Soslowsky et al. 33 in 1992 using precise stereophotogrammetry in 32 freshly frozen human cadavers found less than a 1% deviation from sphericity for both parts, which consequently lead to the conclusion that the concept of a very conformed shoulder joint with mating radii of humeral heads and glenoids such that a lack of stability rather would be attributed to the small surface area of the glenoid in comparison with the humerus. This conclusion is in contrast to the opinion and investigations of many other authors.3,19,20,34-37 Nägerl et al. 36 actually showed that, from a biomechanical point of view and based on sequential radiographs in abduction, the physiological incongruity represents a functional necessity. Most modern implant systems provide a mismatch between the humeral and glenoid component between 2 and 6 mm based on fundamental measurements on fresh specimens using a digitized measurement machine by Boileau and Walch. 3 Their ratio of humeral head and glenoid radii in the coronal plane (0.83) was very similar to that observed in our study (0.87).
The main advantage of this study is the reduction of selection bias because we used healthy young volunteers without relevant medical history with an average age of 24 years compared with the rather inhomogeneous groups of patient samples in comparable studies (average age between 41 and 72 years).19,20,24,35 Another relevant advantage is the fact that the reported values in this study represent in situ data of normal joints in a physiological environment, with normal lubrication by synovia and intact compression forces by the surrounding muscles, especially the rotator cuff. All cadaver studies have the inherent risk of an altered anatomy of the articular cartilage due to the absence of these physiological conditions. Even for fresh, quickly processed specimens, the effects of rigor mortis and early cartilage degeneration by the change in water content cannot entirely be excluded.
To the best of our knowledge, there is no previous study that provides data on in situ measurements of articular cartilage in healthy human subjects using high-resolution MRI. We observed a very homogenous cartilage thickness distribution at the glenoid. This is in contrast to the observations of Zumstein et al. 20 on fresh shoulder specimens with a distribution pattern of cartilage thickness between <0.9 mm and >2.8 mm at the periphery and the lower and upper glenoid surfaces, respectively. The provided radii of curvature of the glenoid (27.3-27.4mm) are slightly greater compared with our results, whereas the radii at the humeral side at 22.1 mm are comparable to our results. 40
We observed a small but significant reduction in cartilage thickness in the middle-inferior (humeral head) and the posterior parts of both the glenoid and humeral head. These areas only come into contact with the glenoid cavity in extreme external rotation. In this position, the anterior capsule with the superior, medial and inferior glenohumeral ligament (depending on the degree of abduction) and the subscapularis muscle are strained and maximally lengthened, and a smaller radius of curvature could potentially reduce contact pressure in this locked position.
Some studies have investigated the normal joint space on radiographs both in healthy subjects and in early and advanced osteoarthritis.38-40 The addition of the cartilage thickness of the humerus and glenoid at the corresponding areas in this study results in a radiological joint space between 2.9 and 2.7 mm, if close contact between both joint partners is assumed. Kircher et al.38,39 reported values of 4.3 mm at the central part on true anterior-posterior view and 6.1 mm on axillary radiographs. Therefore, our results underline that the radiological joint space at the shoulder cannot be put on a level with cartilage thickness.38,39 The provided values for cartilage thickness and radii at the shoulder joint may serve as normative data that represent a healthy adult population that future studies can compare with using modern imaging modalities such as MRI, thereby avoiding the high amount of radiation exposure with CT.11,12
Conclusion
With this study, the concept of a radial mismatch between the joint surface of the humeral head and the glenoid cavity at the cartilaginous level in healthy human subjects can be confirmed, providing normative data for use with high-resolution MRI sequences. The observed cartilage distribution was very homogenous, except for slightly smaller amounts at the posterior aspect of the humeral head. This study provides normative data for comparison of joint cartilage changes at the shoulder in various pathological conditions such as early osteoarthritis.
Footnotes
Ethical Approval
Ethical approved for this study was obtained from the local ethical committee of the Medical Faculty of the Heinrich-Heine University Düsseldorf on October 26, 2010 with the study number 3304.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant of the German Osteoarthritis-Aid (“Deutsche Arthrose-Hilfe e.V.”).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.