
Abstract
Objective
Numerous basic science articles have published evidence supporting the use of biologic augmentation in the treatment of osteochondral lesions of the talus (OLT). However, a comprehensive evaluation of the clinical outcomes of those treatment modalities in OLT has yet to be published. The purpose of this review is to provide an evidence-based overview of clinical outcomes following biologic augmentation to surgical treatments for OLT.
Design
A comprehensive literature review was performed. Two commonly used surgical techniques for the treatment of OLT—bone marrow stimulation and osteochondral autograft transfer—are first introduced. The review describes the operative indications, step-by- step operative procedure, clinical outcomes, and concerns associated with each treatment. A review of the currently published basic science and clinical evidence on biologic augmentation in the surgical treatments for OLT, including platelet-rich plasma, concentrated bone marrow aspirate, and scaffold-based therapy follows.
Results
Biologic agents and scaffold-based therapies appear to be promising agents, capable of improving both clinical and radiological outcomes in OLT. Nevertheless, variable production methods of these biologic augmentations confound the interpretation of clinical outcomes of cases treated with these agents.
Conclusions
Current clinical evidence supports the use of biologic agents in OLT cases. Nonetheless, well-designed clinical trials with patient-specific, validated and objective outcome measurements are warranted to develop standardized clinical guidelines for the use of biologic augmentation for the treatment of OLT in clinical practice.
Keywords
Introduction
Osteochondral lesions of the talus (OLT) are a commonly encountered foot and ankle disorders. In the majority of cases, patients with this pathology have a history of ankle sprains and/or fractures. 1 A recent systematic review demonstrated that as many as 50% of primary OLTs failed to resolve using conservative treatment, while operative treatment—including both reparative and replacement techniques—demonstrated good to excellent clinical outcomes in nearly 85% of cases. 2 Despite the favorable reported outcomes following operative treatment, however, inevitable deterioration of the regenerated or grafted cartilage has been documented in the literature.3-6 This observed decline has been proposed to result from a combination of mechanical and biological impairments in the injured ankle joint.7-10
Biologic agents, including platelet-rich plasma (PRP) and concentrated bone marrow aspirate (CBMA), as well as scaffold-based therapy have the potential to improve the quality of cartilage repair and prevent the long-term deterioration of the joint in OLT. While numerous basic science articles show evidence that supports the use of these biologic augmentations for the treatment of cartilage pathology,11-15 a comprehensive evaluation of the clinical outcomes of those treatment modalities in OLT has yet to be published.
The purpose of this review is to provide an evidence-based overview of clinical outcomes following biologic augmentation of surgical treatments for OLT.
Surgical Treament Modalities of OLT
Bone Marrow Stimulation
Bone marrow stimulation (BMS) is a reparative procedure that is the most common operative treatment choice for OLT. Current indication for BMS is in patients with smaller lesions up to 150 mm2 in size or 15 mm in diameter.7,8 The procedure is carried out arthroscopically in the following steps: (1) debridement of the unstable cartilage and necrotic bone, (2) debridement of the calcified layer, and (3) penetration of the subchondral bone plate (SBP) using a microfracture pick or small diameter drill ( Fig. 1 ).15,16 The procedure aims to stimulate mesenchymal stem cell (MSC) proliferation and promote fibrous cartilage repair tissue within the OLT defect. 17
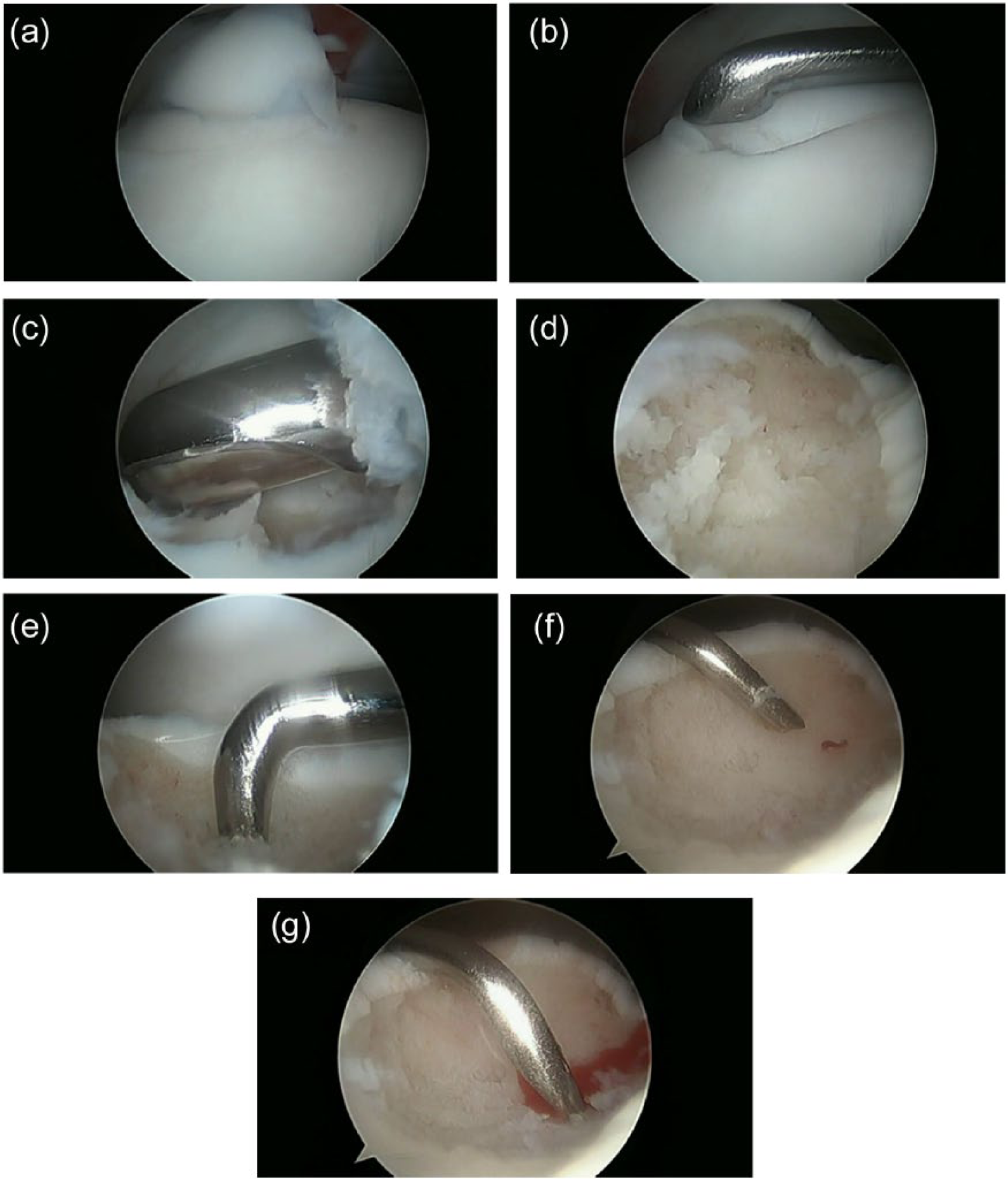
(
BMS has shown promising functional outcomes in clinical studies, with approximately 85% of patients achieving good to excellent results.2,18,19 To our knowledge, the longest follow-up after BMS was reported by van Bergen et al. 20 on the outcomes of 50 patients who were followed for a mean of 141 months. The authors reported that the mean American Orthopaedic Foot and Ankle Society (AOFAS) score for overall functional was 88 out of 100 possible points. 20 Many investigators have supported the good functional outcomes following BMS with short- to mid-term evaluations of athletic populations.21-23
Despite the successful outcomes following BMS for OLT, deterioration of the regenerated fibrous cartilage infill at the defect site produced by BMS is inevitable.3-6 Ferkel et al. 4 found deterioration in 35% of patients within 5 years following BMS. Lee et al. 5 reported that only 30% of patients who received BMS showed lesion integration during second look arthroscopy 12 months postoperatively. van Bergen et al. 20 reported that one-third of patients progressed by one grade of arthritis severity on standard radiographs, although the initial success of BMS was maintained throughout the mean follow-up period of 141 months.
The joint deterioration observed following BMS may be the result of a combination of both mechanical and biologic factors. Regenerated fibrous cartilage is mechanically inferior to hyaline cartilage.24,25Lesion characteristics, including lesion size (current criteria, 150 mm2 or 15 mm in diameter)7,8 and location (talar shoulder or nonshoulder) 9 may affect the rate of success of BMS for OLT. Recent attention has turned to the SBP, which provides significant joint loading support.26,27 When the SBP is diminished, either by the disease process itself or by overzealous BMS, mechanical support will be reduced compromising cartilage longevity.
Biologically, articular cartilage has poor self-repair capabilities due to the tissue’s avascularity and hypocellularity.28,29 Although the fibrous cartilage stimulated by BMS initially forms a fibrin clot that differentiates into chondrocyte-like cells that deposited type-II collagen at the site of the defect, proteoglycan depletion, chondrocyte death, and deposition of type-I collagen have been reported at 1 year postoperatively. 30 Fibrocartilage may lack the biological and structural capacity to prevent fluid ingress under hydrostatic loading, leading to the collapse of the stimulated infill. 31 Recent studies have suggested that intra-articular inflammatory cytokine levels are elevated in an injured ankle joint compared with a healthy joint.32,33 Animal studies showed that these catabolic reactions increase the risk of developing degenerative arthritis, even in mechanically stabilized joints.34,35
A biologic agent that can reduce inflammation and provide a chondrogenic biologic milieu would therefore be advantageous.
Autologous Osteochondral Transplantation
Autologous osteochondral transplantation (AOT) is a replacement, rather than reparative, treatment option for OLT. The goal of the procedure is to restore the native architecture of the chondral surface and subchondral bone plate by inserting a cylindrical autologous osteochondral graft, typically from a non-weightbearing portion of the ipsilateral femoral condyle, into the site of the defect. 17 AOT is traditionally indicated in patients with a lesion greater than 150 mm2 or 15 mm in diameter, for cystic lesions, or in cases of failed previous BMS.7,8 This technique consists of the following steps: (1) osteotomy of the malleolus to enable direct lesion visualization, (2) BMS to the surrounding healthy bone, (3) removal of the talar lesion accompanied by overdrill to create a slightly longer graft site than the harvested plug, (4) graft harvest from a non-weightbearing portion of the ipsilateral femoral condyle, and (5) insertion of the graft(s) into the recipient site ( Fig. 2 ). 36
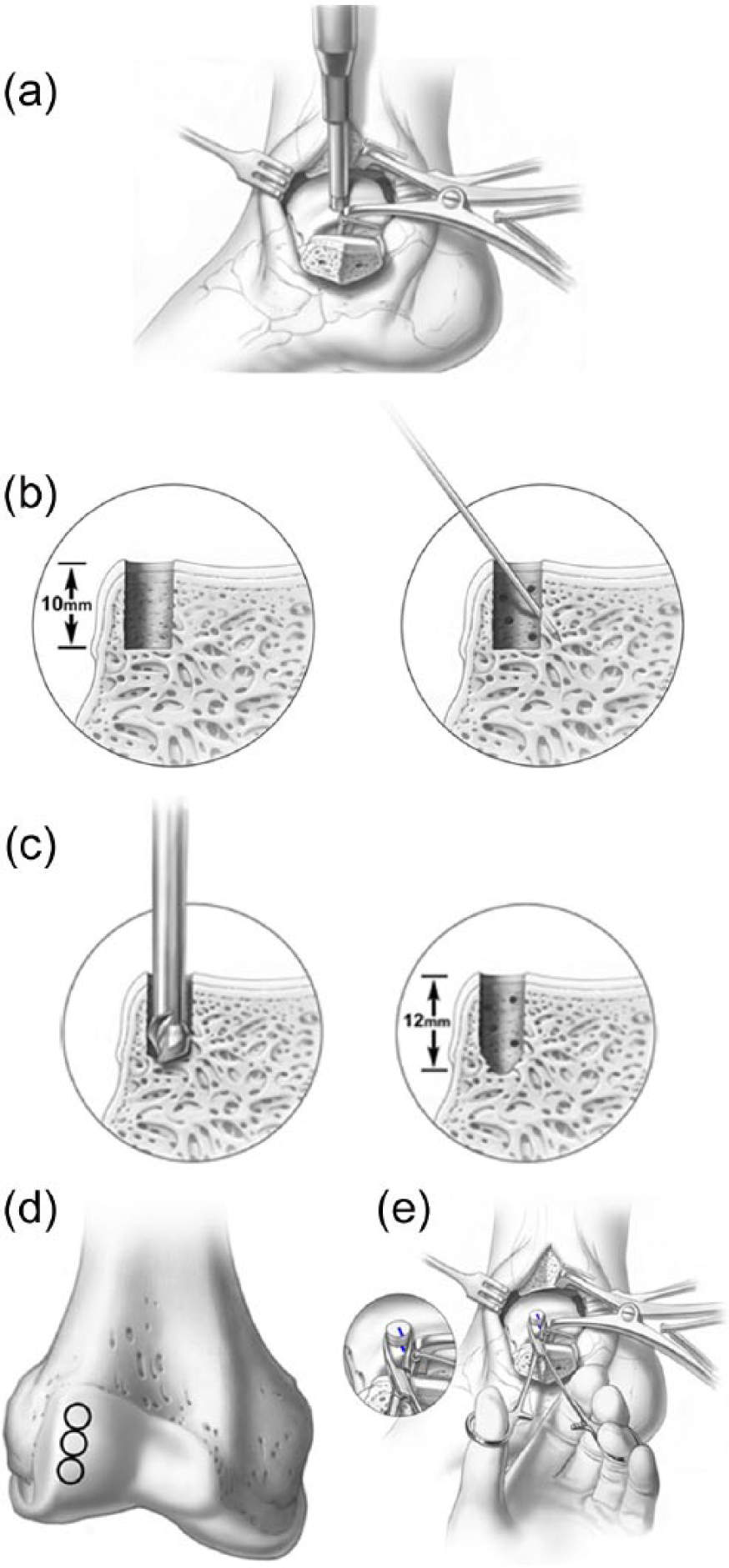
(
Several studies have reported good clinical outcomes following AOT at both short- and mid-term follow-up.36-39 A systematic review reported good to excellent outcomes following AOT in 243/279 patients (87%), 2 and several studies showed that 63% to 95% of athletes return to their previous level of activity following this procedure.36,37,40,41 Despite its apparent success and favorable short- and medium-term outcome profile; however, to our knowledge no study has described the procedure’s long-term (10+ years) outcomes.
While the reported positive clinical outcomes do not seem to significantly deteriorate over time, 36 some concerns have been raised in both basic and clinical studies.42-46 Poor integration of the graft surface with the native tissue,42,43 cyst formation around the graft site, and deterioration of the graft cartilage 46 have all been described following AOT procedure.
Like BMS, the success of AOT for OLT may be limited by a combination of mechanical and biologic factors. A biomechanical study by Fansa et al. 47 showed that a mere 1.0 mm of graft protrusion above the level of the native cartilage increased the contact pressure on the graft surface almost 7-fold. In addition, because tibial osteotomy is frequently used to enable visualization of the lesion in AOT, the procedure carries the risk of mal-/nonunion at the site of the osteotomy. 46 This inherent risk can cause mechanical abnormalities in a fixed ankle joint and accompanied by an elevated level of intra-articular inflammatory cytokines may result in posttraumatic ankle osteoarthritis.10,32,33 Furthermore, structural differences between talar and knee articular cartilage may produce incompatible mechanical properties. 48 Finally, knee cartilage contains cytokines not typically seen in ankle cartilage, including MMP-8 (neutrophil collagenase), which can produce a catabolic response in the reconstructed ankle joint and contribute to graft failure. 49 A biologic agent may therefore influence the quality of integration and longevity of the AOTS graft in the talus.
Biologic Augmentation for Cartilage Repair
Platelet-Rich Plasma
Platelet-rich plasma (PRP) is an autologous blood product that contains at least twice the concentration of platelets compared with baseline values, or >1.1 × 106 platelets/μL. Physiologically, platelets contain growth factors and cytokines that participate in tissue healing. 50 Platelets could also potentially attract MSCs to a site of interest. 51
PRP is produced using a simple bedside procedure: Blood is drawn from a peripheral vein and centrifuged using a commercially available centrifuge system. Several commercially available PRP centrifuge modalities, timing protocols for centrifugation of harvested blood, and activation methods of PRP have been described.50,52,53 The contents of the plasma—including platelets, cells, growth factors, and cytokines—are therefore variable, even within a single individual, 50 and no standardized PRP production method has been established to date.
Several basic science in vitro and vivo studies have examined the proposed positive effects of PRP on cartilage repair. A systematic review performed by Smyth et al. showed that 18 of 21 (85.7%) basic science articles (12 in vitro, 8 in vivo, 1 both in vitro and in vivo) described a positive effect of PRP on cartilage repair. PRP was applied as a concomitant biological adjuvant during BMS and implant, scaffold, and graft insertion in vivo. The authors reported that PRP increased chondrocyte and mesenchymal stem cell proliferation, proteoglycan deposition, and type II collagen deposition and inhibited the effect of catabolic cytokines. 11 More recently, Symth et al. 54 investigated the effect of PRP as an adjunct to AOT in a rabbit model. The authors found that application of PRP at the time of AOT improved the integration of the osteochondral graft at the cartilage interface and decreased graft degeneration. 54 Finally, Boakye et al. 55 found that TGF-β1 expression was increased in rabbits treated with AOT and PRP compared with those with AOT and saline, and concluded that PRP could have a chondrogenic effect in vivo. These studies suggest that PRP could be used as a beneficial adjunct to BMS and AOT to improve graft survival and long-term outcomes.
While the positive effects of PRP on degenerative osteoarthritis have been demonstrated in several level 1 clinical evidence studies,56-62 to our knowledge only 3 comparative studies have evaluated the use of PRP in OLT. Mei-Dan et al. 63 (level of evidence [LOE]: II) prospectively compared clinical outcomes following PRP or hyaluronic acid (HA) injection in 32 patients with a 6-month follow-up. The authors reported that PRP injection provided significantly better clinical scores than HA. Guney et al. 64 (LOE: II) performed a randomized prospective study comparing the clinical and functional outcomes of 16 patients treated with BMS with 19 patients who received BMS with PRP. At the average follow-up of 16.2 months, the authors found that all cases included in the study had significantly improved clinical outcomes, but the PRP group had superior outcomes to the BMS-only group. Finally, Görmeli et al. 65 (LOE: I) compared the effect of PRP and HA following BMS for OLT in a prospective randomized clinical trial. Among 40 patients with an average of 15.3-month follow-up, clinical improvement after PRP treatment was significantly greater than after HA or saline injection. Thus, though few comparisons are currently available in the literature, results suggest that using PRP for treating OLT may improve outcomes compared with HA or no intervention. Nevertheless, because of the noted variability in PRP content, a definitive conclusion is yet to be reached.
Concentrated Bone Marrow Aspirate
Concentrated bone marrow aspirate (CBMA) is a reservoir of MSCs, growth factors, and cytokines that have been purported to improve the quality of cartilage repair tissue. This blood product is produced by centrifuging bone marrow aspirate (BMA) harvested from the iliac crest using a trocar at the time of surgery for OLT.
CBMA’s potential to improve the quality of cartilage repair tissue following BMS has been reported in both in vivo models and a clinical study. In an equine model, Foriter et al. 12 reported that when added during BMS, CBMA improved healing compared with BMS alone based on histological and radiological parameters. In a goat model, Saw et al. 66 described that BMS in combination with CBMA and HA showed significantly improved healing compared with BMS with HA only. In addition, the authors reported that nearly complete coverage of the defect and evidence of hyaline cartilage repair were found in the CBMA-treated group. In a clinical study, Hannon et al. 67 performed a retrospective comparative study of 22 OLT patients treated with BMS alone or BMS with concomitant CBMA. The authors reported that BMS with CBMA resulted in comparably good medium-term functional outcomes, but improved border repair tissue and less evidence of fissuring and fibrillation on MRI compared with BMS alone.
A single report on CBMA in OLT patients treated with AOT has been published (LOE: IV). 36 This showed significant improvement of clinical outcome in 72 patients at a mean follow-up of 28 months. In addition, the authors reported that magnetic resonance imaging using T2 mapping showed restoration of radius curvature and color stratification similar to that of native cartilage.
Based on current evidence, it appears that CBMA can improve cartilage repair in OLT. However, further conclusions cannot be made at this early juncture and further research, including comparative studies, is warranted.
Scaffold-Based Therapy
Scaffold-based therapy is another reparative option for treatment of OLT that has recently been gaining support by clinical evidence.
Matrix-induced autologous chondrocyte implantation (MACI) consists of a 2-stage operative procedure. In the first stage, autologous chondrocytes are obtained by biopsy and cultured ex vivo for several weeks. In the second stage, the chondrocytes are seeded in a scaffold containing type I/III collagen, hyaluronan, and polyglycolic/polylactic acid and implanted in the site of the defect.2,68,69 MACI has shown promising functional outcomes in the literature, with the majority of patients achieving good to excellent results. To our knowledge, the longest follow-up after MACI was reported by Giannini et al. 70 following 46 ankles for a mean of 87.2 months (LOE: IV). The authors reported that the mean score for AOFS was 92 out of 100 points.
Autologous matrix-induced chondrogenesis (AMIC) is a 1-step scaffold-based therapy. In this procedure, an acellular collagen I/III matrix is used to cover the lesion following BMS. AMIC attempts to stabilize the blood clot and stimulate chondrogenesis from MSCs. Wiewiorski et al. 71 (LOE: IV) investigated the outcomes of 23 OLT patients following AMIC at a median of 23 months postoperatively and reported an increase in median AOFAS scores from 60.3 to 90.9. Recently, Valderrabano et al. 72 (LOE: IV) reported a mean AOFAS score increase from 60 to 89 in patients who received AMIC. They also reported that 84% of studied patients had normal or near-normal signal intensity of the repair tissue compared with the adjacent native cartilage.
Bone marrow–derived cells transplantation (BMDCT), a combination of CBMA and scaffold material, is used to fill the defect site. Several clinical articles have shown that postoperative clinical scores improved significantly using this treatment modality.73-79
Overview
Biologic therapy to improve OLT outcomes remains a subject of debate. Based on currently available basic and clinical evidence, biologic agents and scaffold-based therapies have been shown to improve clinical and radiological outcomes in OLT. Nevertheless, variable production methods of these biologic augmentations confound the interpretation of clinical outcomes. A recent systematic review showed that most studies assessing clinical outcomes following operative treatment in OLT are of low levels of evidence and of poor methodological quality. 80 As such, well-designed clinical trials with patient-specific, validated and objective outcome measurements are warranted to develop standardized clinical guidelines for the use of biologic augmentations for treatment of OLT in clinical practice.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John G. Kennedy is a consultant for Arteriocyte, Inc; received research support from the Ohnell Family Foundation, Mr. and Mrs. Michael J Levitt, Arteriocyte Inc; is a board member for the European Society of Sports Traumatology, Knee Surgery, and Arthroscopy (ESSKA), International Society for Cartilage Repair of the Ankle (ISCRA), American Orthopaedic Foot & Ankle Society (AOFAS) Awards and Scholarships Committee, International Cartilage Repair Society (ICRS) finance board.