
Abstract
Purpose
The purpose of this study was to assess the effect(s) of platelet-rich plasma (PRP) on osteochondral donor site healing in a rabbit model.
Methods
Osteochondral donor sites 3 mm in diameter and 5 mm in depth were created bilaterally on the femoral condyles of 12 New Zealand White rabbits. Knees were randomized such that one knee in each rabbit received an intra-articular injection of PRP and the other received saline (placebo). Rabbits were euthanized at 3, 6, and 12 weeks following surgery. Repair tissue was evaluated using the International Cartilage Repair Society (ICRS) macroscopic and histological scores.
Results
No complications occurred as a result of the interventions. There was no significant difference in macroscopic scores between the 2 groups (5.5 ± 3.8 vs. 3.8 ± 3.5; P = 0.13). Subjective macroscopic assessment determined greater tissue infill with fewer fissures and a more cartilage-like appearance in PRP-treated knees. Overall ICRS histological scores were better in the PRP group compared with the placebo (9.8 ± 2.0 vs. 7.8 ± 1.8; P = 0.04). Histological scores were also higher in the PRP group compared with the placebo group at each time point. Greater glycosaminoglycan and type II collagen content were noted in the repair tissue of the PRP group compared with the placebo group.
Conclusion
The results of this study indicate that PRP used as an intra-articular injection may improve osteochondral healing in a rabbit model.
Introduction
The potential for osteochondral defects to self-repair is limited in part due to the hypocellular and avascular nature of articular cartilage. 1 Osteochondral defects that fail to heal spontaneously may ultimately result in further joint destruction and osteoarthritis. 2 Numerous surgical treatment modalities have been developed, primarily focused on either repairing the damaged cartilage (e.g., bone marrow stimulation) or replacing the lesion with a viable osteochondral graft (e.g., autologous osteochondral transplantation). Regardless of whether the cartilage is repaired or replaced, the existing surgical treatment modalities are hindered by poor biology, leading to inferior quality repair tissue when compared to native hyaline cartilage. 3
In an effort to improve the repair of osteochondral defects, biological products have seen increasing interest as an adjunct to surgical treatment and as a primary treatment modality.4-7 One such biological product is platelet-rich plasma (PRP), defined as an autologous blood product derived by the centrifugation of whole blood yielding a concentration of platelets that is increased from the baseline value. 8 At the basic science level, PRP has been shown to increase chondrocyte and mesenchymal stem cell proliferation, proteoglycan production, and type II collagen deposition.9-11 Few in vivo studies have been performed to evaluate the effect of PRP alone on chondrogensis. Therefore, the objective of this study was to assess the effect of PRP on the repair of an osteochondral donor site (i.e., defect) in a rabbit model. We hypothesized that PRP would improve osteochondral healing at the donor site in the knee.
Materials and Methods
The Institutional Animal Care and Use Committee approved all surgical procedures and experimental designs. A preliminary power analysis showed that a sample size of 12 rabbits had 88% power to detect a two point difference in the primary outcome of International Cartilage Repair Society (ICRS) histological score given a standard deviation of 2 points. Therefore, 12 New Zealand White rabbits were used with a mean weight of 4 kg (range, 3.7-4.2 kg) and a mean age of 23 weeks (range, 22-24 weeks). A rabbit model was chosen for this study as the rabbit knee is large enough to accommodate the procedure and it is a well-established model that has been used previously for studies assessing cartilage repair procedures. The rabbits were held in individual cages and allowed unrestricted cage activity for 7 days preoperatively. Additional experimental results derived from this animal model have been published previously. 12
Surgical Procedure, PRP Preparation, and Cytological Analysis
Under anesthesia, 27 mL of blood was aspirated from the great aural artery of each rabbit and combined with 4 mL of anticoagulant citrate dextrose solution A (ACD-A). One milliliter of blood was then immediately dispensed into a separate syringe for cytological analysis. The remaining blood was then centrifuged using a standard, commercially available platelet concentration system (Magellan Autologous Platelet Separator, Arteriocyte, Cleveland, OH) to yield 3 mL of PRP according to the manufacturer’s protocol (centrifuge force, 1200 × g; centrifuge time 17 minutes). From this sample, one ml was reserved for cytological analysis and the remainder was allocated for surgical use. Therefore, each rabbit was treated with an autogenous sample of PRP. The whole blood and PRP samples underwent cytological analysis to measure platelet levels as well as red and white blood cell counts, as per previously published work. 12
The anesthetic protocol used for the animals involved use of subcutaneous ketamine (40 mg/kg) and acetylpromazine (0.5 mg/kg), and maintenance with isoflurane (2%) inhalation through intubation. Antibiotic prophylaxis (ampicillin 25 mg/kg) was given 30 minutes prior to surgery.
Following shaving and standard sterile preparation of both lower extremities, a 4 cm medial parapatellar arthrotomy was created in each knee exposing the medial and lateral femoral condyles. The joint was then carefully inspected to ascertain whether any preexisting cartilage pathology was present. Using a trephine with an outer diameter measuring 3.0 mm and 5 mm in depth (Smith & Nephew, Memphis, TN) an osteochondral graft was harvested on the medial femoral condyle of the left knee and lateral femoral condyle of the right knee, thereby creating a donor site. The graft harvested using the trephine was transplanted to the opposing femoral condyle for a separate study assessing autologous osteochondral transplantation that has been published previously. 12 The defects were then debrided of any remaining osseous or cartilage fragments. 13 The use of an autologous osteochondral transplant donor site as a rabbit osteochondral defect model has been widely published in the literature.14 -17 Each wound was then closed in layers using simple interrupted sutures (4-0 Vicryl), with final skin closure achieved using a running subcutaneous stitch technique (4-0 Vicryl) to obtain a water-tight seal. Prior to wound closure, the knees were randomized to receive an injection of either 0.5 mL of PRP or saline (placebo). Randomization was done through a computer-generated list, with results placed in a sealed envelope by an individual not involved with the surgical procedure. The envelopes were opened prior to wound closure so as to determine the laterality of the treatment. Therefore, following wound closure, 0.5 mL of PRP or saline was administered as an intra-articular injection.
Prior to concluding the surgical procedure, the knee was moved through a full range of motion to ensure that normal patellar tracking occurred. Postoperatively, the animals were given fentanyl skin patches (12 µg/h) and allowed unrestricted cage activity. The rabbits were euthanized using pentobarbital (100-150 mg/kg, intravenously) at 3, 6, and 12 weeks following the initial surgery, with 4 rabbits euthanized at each time interval.
Gross and Histological Processing and Scoring
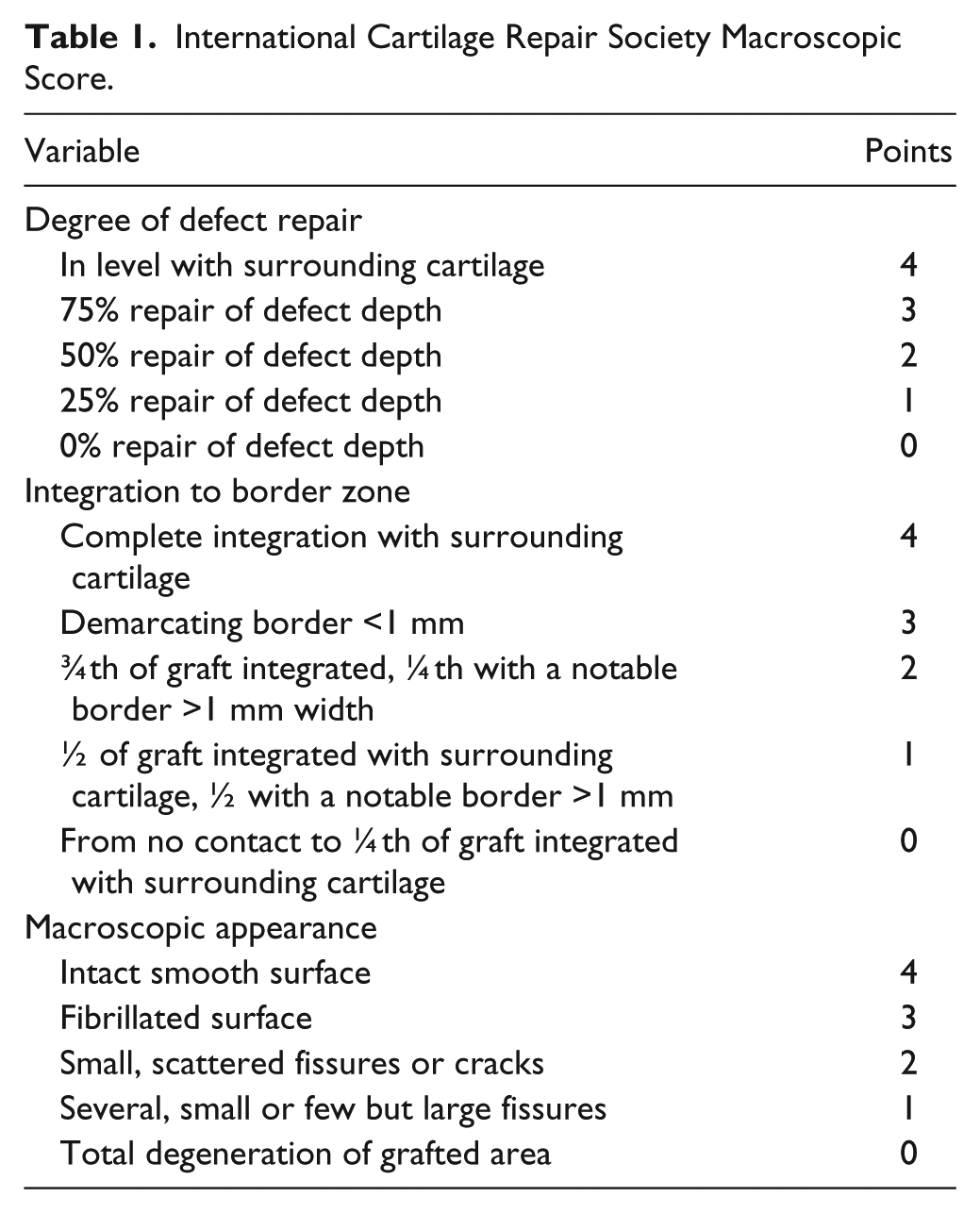
Two reviewers who were blinded to the treatment groups performed all scoring independently. Prior to assigning a final score for a given sample, the reviewers deliberated in order to reach a final consensus. The ICRS macroscopic scoring system on a scale from 0 to 12, with 12 being normal cartilage and 0 indicating severely abnormal, was used to assess the gross specimens ( Table 1 ).
International Cartilage Repair Society Macroscopic Score.
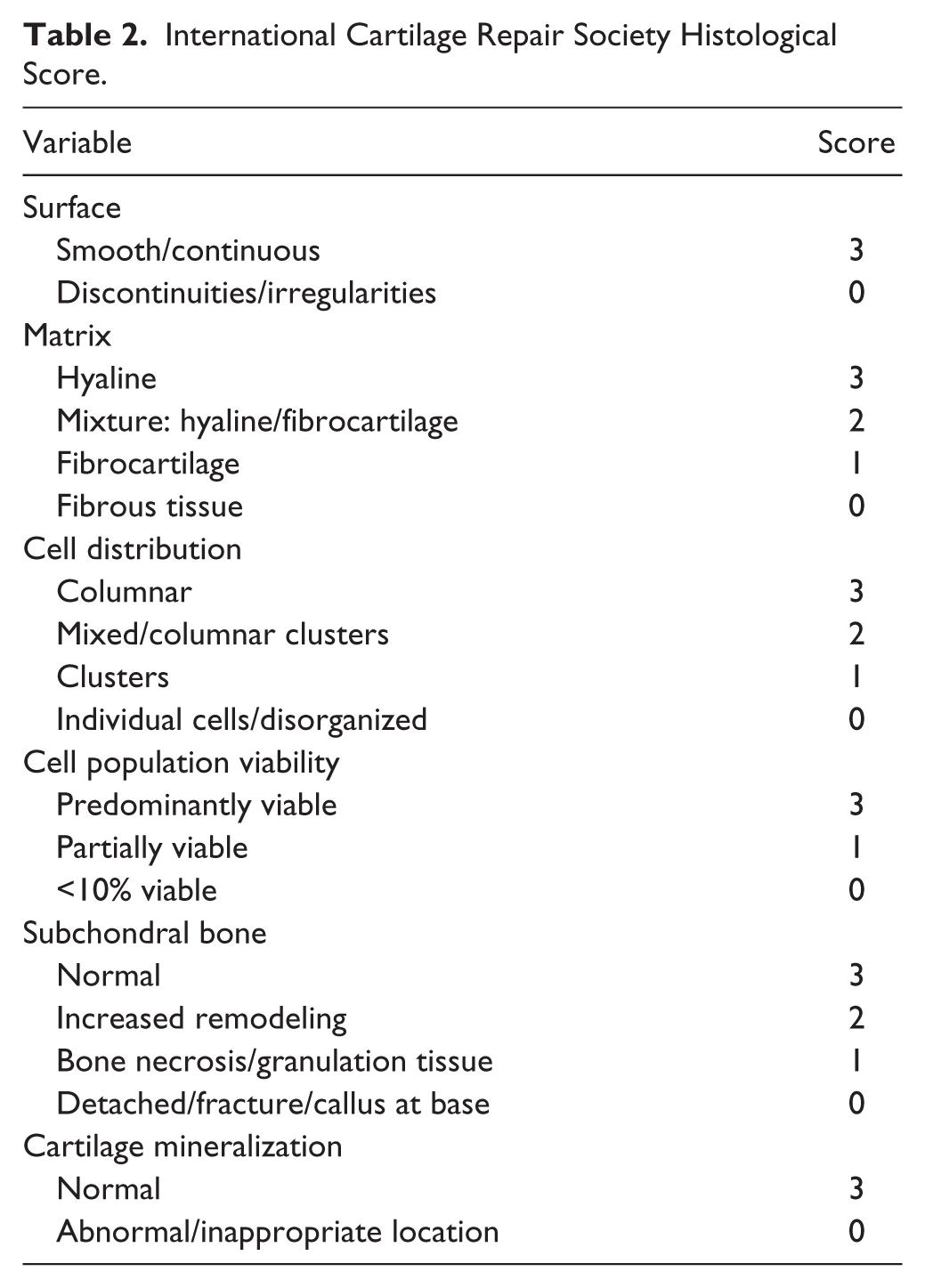
At the time of euthanasia, both knee joints were resected en bloc and placed in 10% formalin for 7 days. Following formalin fixation, the specimens were decalcified in a sodium citrate-formic acid solution for an additional 7 days prior to being embedded in paraffin wax. This is a previously published method of preparing osteochondral specimens in our institution’s laboratory. 18 The specimens were cut into 8 um sections at the posterior, middle, and anterior aspect of the osteochondral donor site, which provided a representative view of overall lesion healing. The osteochondral sections were stained with hematoxylin and eosin for ICRS histological scoring, alcian blue to assess glycosaminoglycan presence, and processed for type II collagen immunohistochemistry.1,18-20 The ICRS histological score was graded on a scale of 0 to 18 ( Table 2 ).
International Cartilage Repair Society Histological Score.
Statistical Analysis
Descriptive statistics were generated by treatment group for the overall cohort and for each time period. Comparison of ICRS macroscopic and histological scores between PRP-treated and placebo defects for the overall cohort was performed using the Wilcoxon sign-rank test. The mean difference in ICRS scores with 95% confidence interval (CI) was also calculated for each time period separately. Spearman’s rank correlation coefficients were calculated to evaluate associations between cytological variables and histological scores. All analyses were performed using SAS Software version 9.2 (SAS Institute, Cary, NC).
Results
There were no immediate perioperative complications following the surgical procedure. No rabbit exhibited any signs of lameness or developed an infection postoperatively at any time point.
Cytological Analysis
As previously reported, the mean values of the PRP produced showed a 5.1-fold increased platelet count compared to whole blood (817.6 ± 155.0 × 103/µL vs. 161.5 ± 42.6 × 103/µL; P < 0.001). 12 The PRP showed a white blood cell count 1.9 times greater than the whole blood (10.0 ± 3.2 × 103/µL vs. 5.1 ± 1.0 × 103/µL; P < 0.001). The red blood cell count of the PRP was 28% that of the whole blood (10.1 ± 1.8 × 103/µL vs. 35.6 ± 2.4 × 103/µL; P < 0.001).
Macroscopic and Histological Appearance of the Osteochondral Donor Site
The rabbits were euthanized at 3, 6, and 12 weeks following surgery and their knee joints were resected, with 4 rabbits euthanized at each time point. The mean macroscopic review of the osteochondral donor sites across all time points showed a greater mean ICRS macroscopic score in the PRP treated knees compared with the placebo group; however, this was not statistically significant (5.5 ± 3.8 vs. 3.8 ± 3.5; P = 0.13). The mean ICRS macroscopic scores for the PRP-treated group at 3, 6, and 12 weeks postoperatively were 4.0 ± 3.7, 4.5 ± 3.3, and 8 ± 4.1, respectively. The mean ICRS macroscopic scores for the placebo donor sites at the same time points were 3.5 ± 3.1, 1.5 ± 1.3, and 6.5 ± 4.2, at 3, 6, and 12 weeks, respectively. Subjective assessment of the PRP-treated donor sites determined increased tissue infill. Furthermore, the tissue in the PRP-treated donor sites appeared smoother and more hyaline like, with fewer fissures, when compared with the placebos ( Figs. 1 and 2 ).
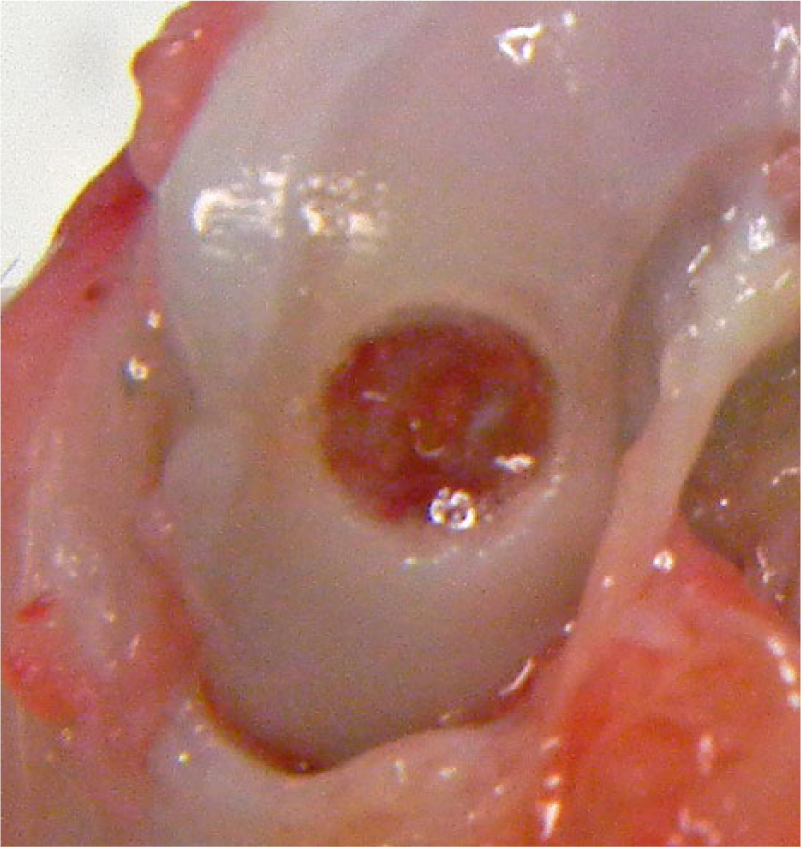
Photograph of osteochondral defect in control group at 12 weeks following surgery.
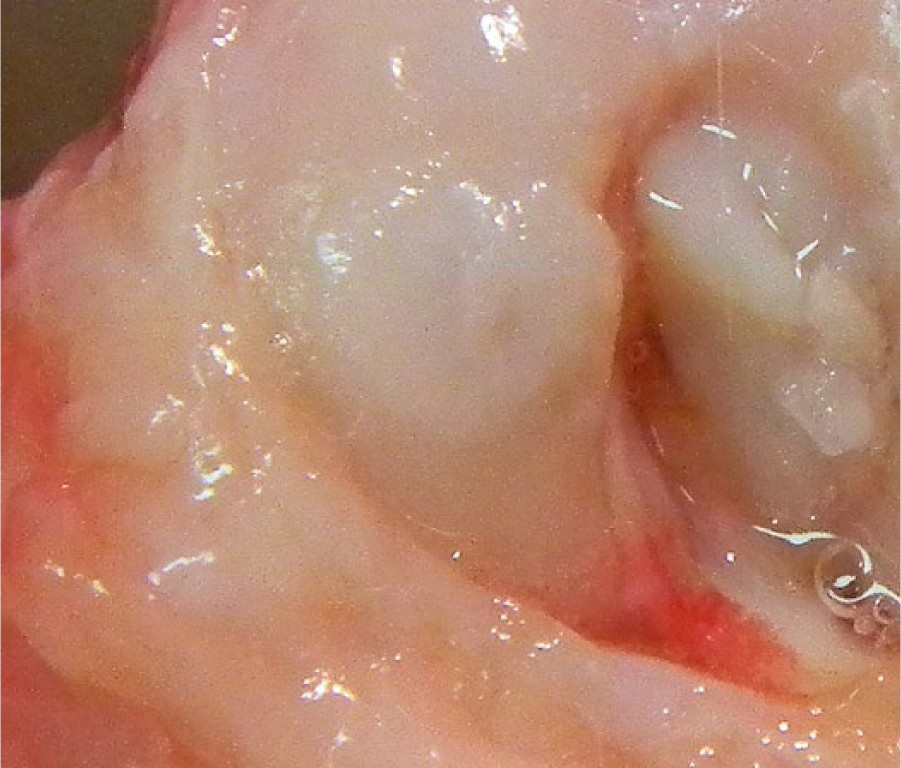
Photograph of osteochondral defect in platelet-rich plasma–treated group at 12 weeks following surgery.
The mean ICRS histological score was higher overall and at each time point for the PRP-treated osteochondral donor sites compared to the placebo group (overall mean 9.8 ± 2.0 vs. 7.8 ± 1.8; P = 0.04). The PRP-treated donor sites showed a greater amount of reparative tissue, with increased cellularity. In addition, the reparative tissue was more hyaline-like in structure in the PRP treated group when compared with the placebo. Cell viability was also noted to be more apparent in the PRP-treated group ( Figs. 3 and 4 ).
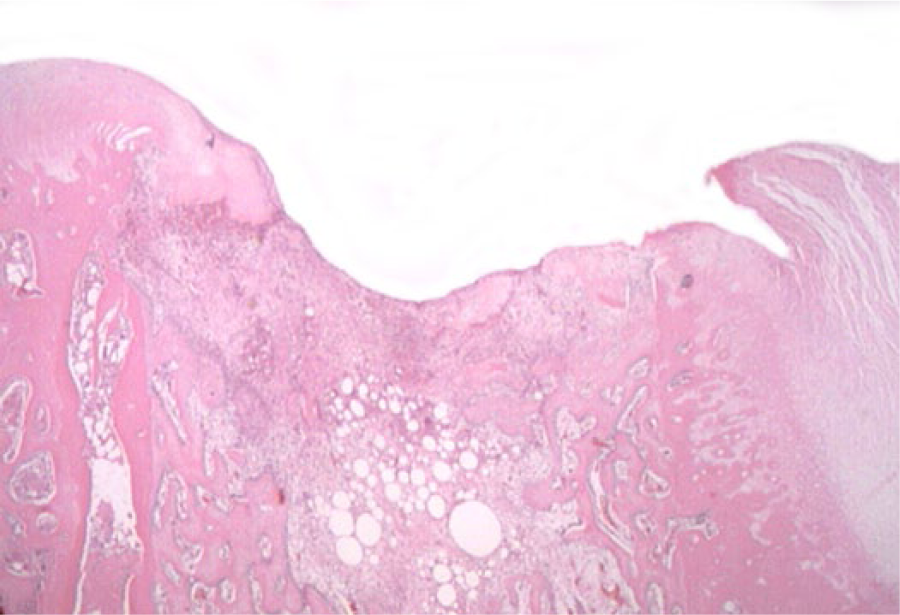
Sagittal section of osteochondral defect in control group at 12 weeks following surgery. Hematoxylin and eosin was used to stain the sections for assessment using the International Cartilage Repair Society scoring system. Image magnification 20×.
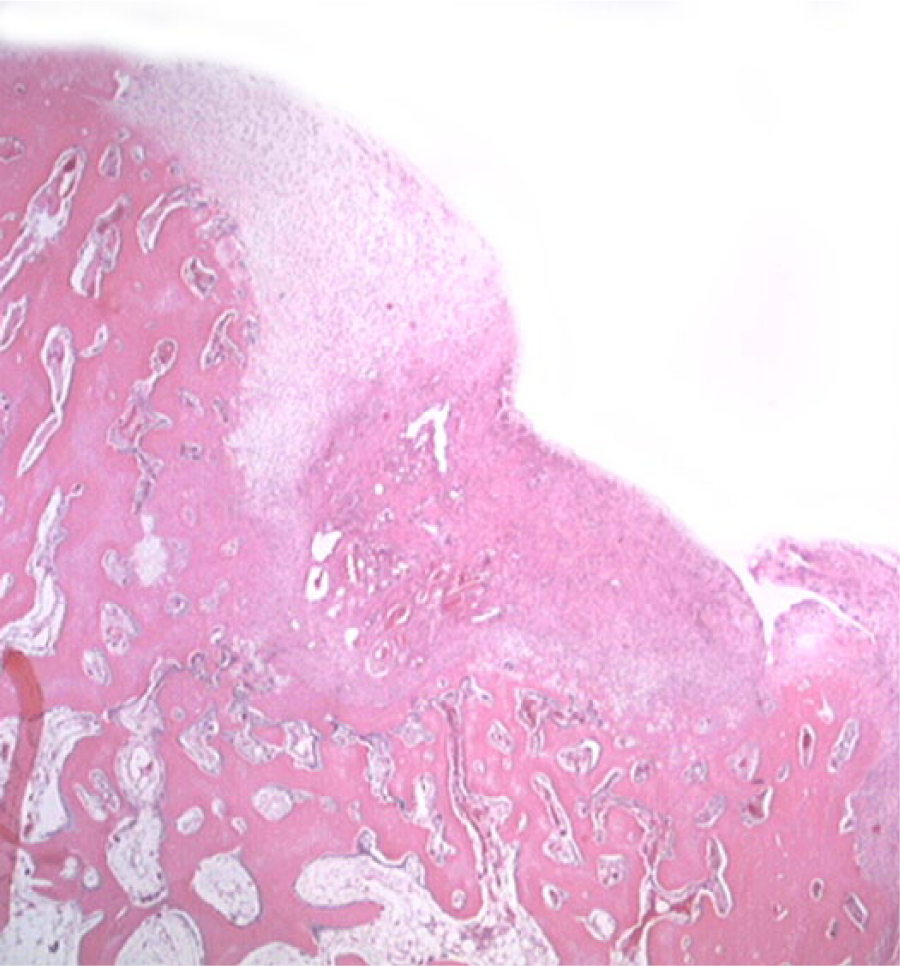
Sagittal section of osteochondral defect in platelet-rich plasma–treated group at 12 weeks following surgery. Hematoxylin and eosin was used to stain the sections for assessment using the International Cartilage Repair Society scoring system. Image magnification 20×.
The mean ICRS histological scores for the PRP treated donor sites at 3, 6, and 12 weeks postoperatively were 10 ± 0.8, 9 ± 2.9, and 10.3 ± 1.9, respectively. These were all higher than the mean ICRS histological score for the placebo donor sites at the same time points (8.0 ± 2.2, 7.5 ± 0.6, and 8.0 ± 2.6, at 3, 6, and 12 weeks, respectively). The mean difference in the ICRS histological score comparing the PRP-treated donor sites to the placebo donor sites at 3 weeks was 2.00, 95% CI = −2.68 to 6.68; at 6 weeks was 1.50, 95% CI = −2.71 to 5.71; and at 12 weeks was 2.25, 95% CI = −3.01 to 7.51. Spearman’s correlation coefficients showed no significant association between ICRS histological score and any cytological variable (white blood cells, ρ = −0.29; platelets, ρ = −0.15, red blood cells, ρ = 0.08; P < 0.05 for all analyses).
The reparative tissue of the PRP treated donor sites demonstrated greater alcian blue staining when compared with the placebo, representing an increase in glycosaminoglycan deposition. In addition, greater type II collagen immunoreaction could be seen in the PRP-treated group. The placebo group had sparse evidence of glycosaminoglycan and type II collagen production, particularly at the center of the donor site. In comparison, the PRP-treated group showed more diffuse staining for both glycosaminoglycan and type II collagen throughout the reparative infill. ( Figs. 5 - 8 )
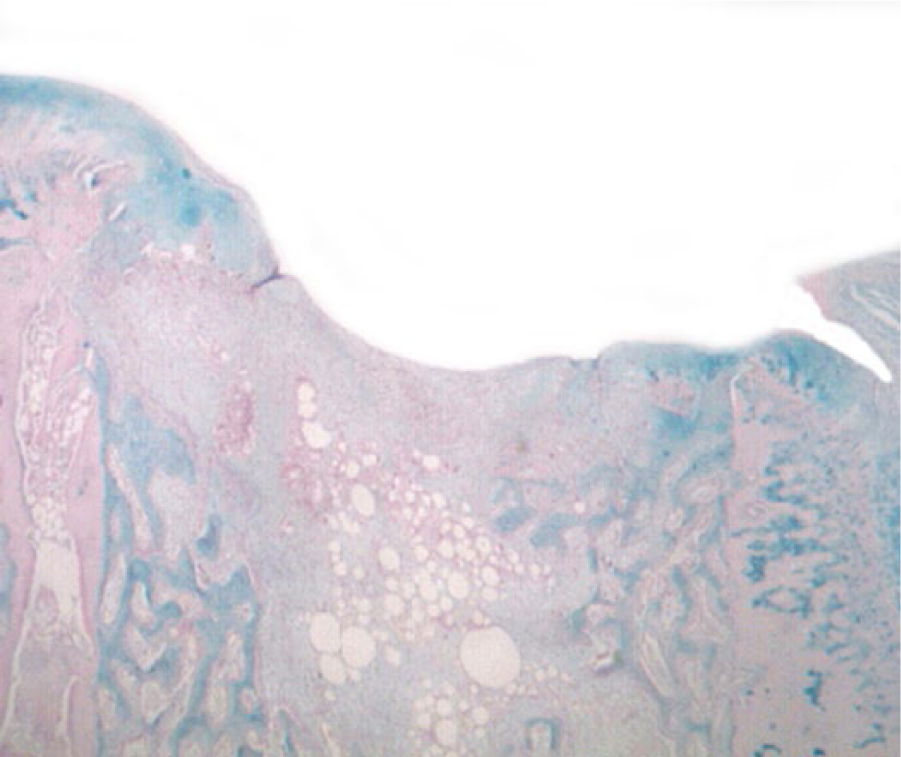
Sagittal section of osteochondral defect in control group at 12 weeks following surgery. Glycosaminoglycan content was assessed using alcian blue staining. Image magnification 20×.
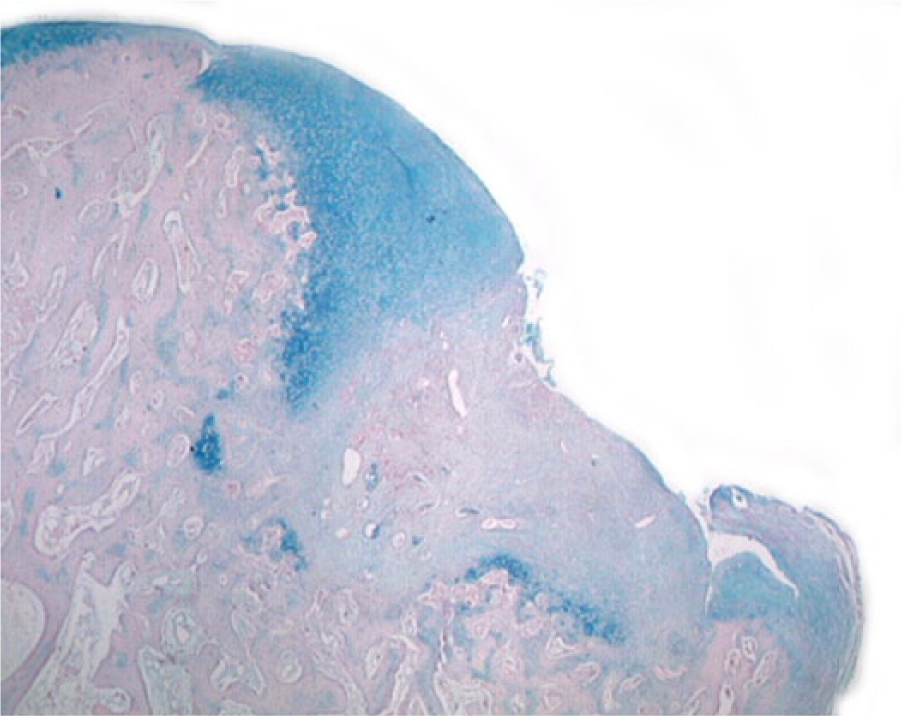
Sagittal section of osteochondral defect in platelet-rich plasma–treated group at 12 weeks following surgery. Glycosaminoglycan content was assessed using alcian blue staining. Image magnification 20×.
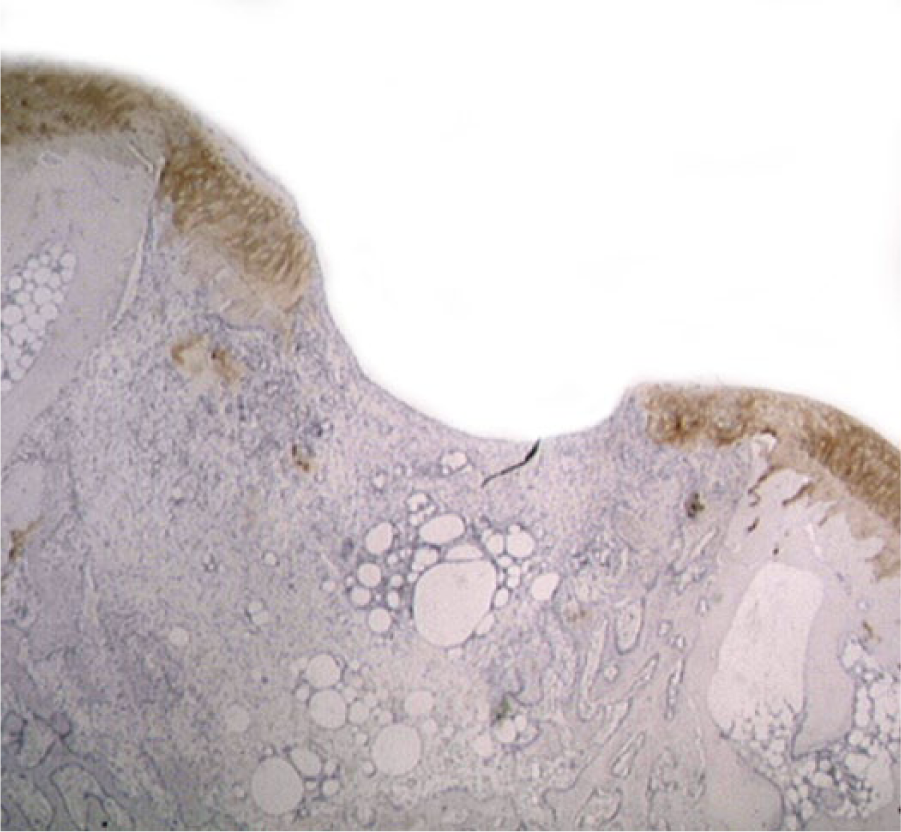
Sagittal section of osteochondral defect in control group at 12 weeks following surgery. Type II collagen content was assessed using type II collagen immunohistochemistry. Image magnification 20×.
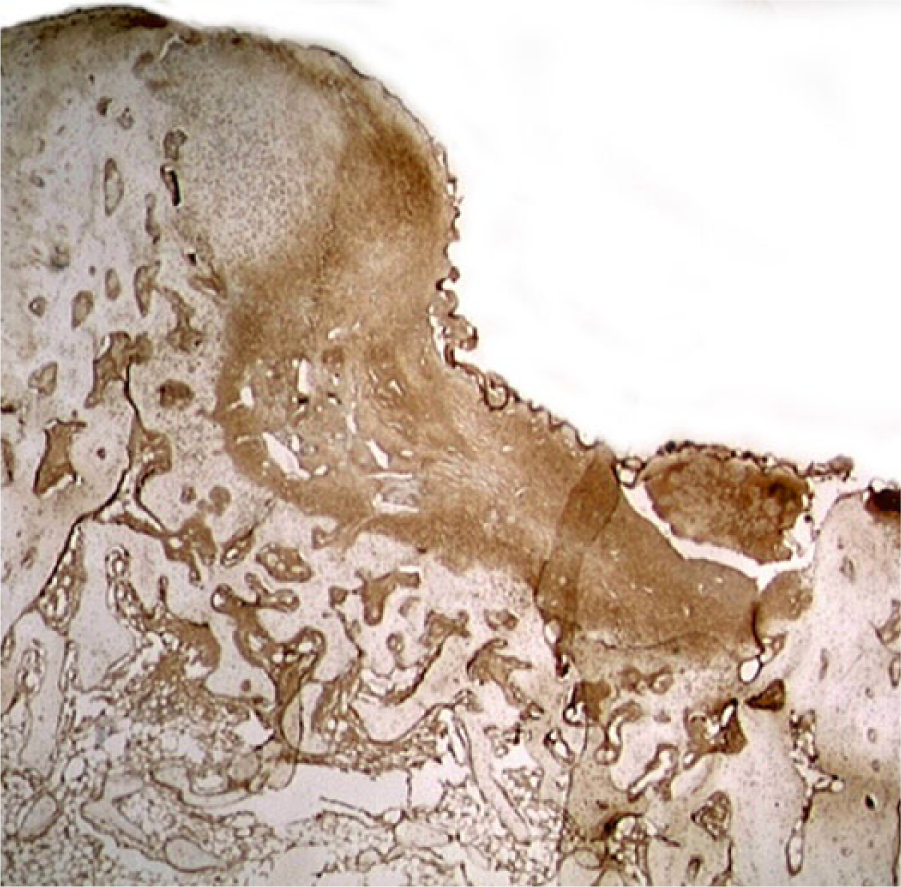
Sagittal section of osteochondral defect in platelet-rich plasma–treated group at 12 weeks following surgery. Type II collagen content was assessed using type II collagen immunohistochemistry. Image magnification 20×.
Discussion
The most important finding of this study is evidence that PRP may improve healing of an osteochondral donor site in vivo in the first 12 weeks postoperatively. While a statistically significant difference was not measured using the ICRS macroscopic scoring system, a significant improvement was quantified at the histological level. No significant detriment occurred as a result of PRP administration.
The effects of PRP on autologous osteochondral transplantation have been reported previously. 12 In contrast to the current study, the use of PRP in an empty donor defect resulted in lower ICRS scores by comparison with those seen in autologous osteochondral transplantation. While these results were expected, the tissue regeneration seen in the PRP group by comparison with the placebo is nonetheless encouraging and may prove beneficial clinically in patients requiring the harvest of an osteochondral graft from a non-weightbearing portion of the femoral condyle.
The findings of the current study reflect the general trend seen in the current literature regarding the use of PRP in cartilage pathology. Multiple systematic reviews investigating the role of PRP in cartilage pathology have been published recently with similar findings.9,10 Zhu et al. 11 concluded that the current basic science, preclinical, and clinical evidence for PRP use in osteochondral defects shows promise. The evidence for this assertion, as well as the potential explanations for the results of the present study, are multifactorial.
Platelet-rich plasma has been shown to increase chondrocyte proliferation and chondrocyte viability.21-23 There is also evidence that PRP upregulates the synthetic capacity of chondrocytes, with multiple studies citing a rise in glycosaminoglycan production and type II collagen deposition.18,24,25 The effect of PRP on mesenchymal stem cells (MSCs) is also relevant to osteochondral defect healing as the lesions in this animal model have a bleeding base, leading to recruitment of subchondral-derived MSCs. Krüger et al. 26 and others,27,28 have shown that PRP increases MSC migration, chondrogenic differentiation, and subsequent proteoglycan production. In addition, PRP may also have an effect on the joint as a whole by modifying the levels of catabolic cytokines that are seen in the presence of a cartilage lesion. These are known to include interleukin-1 (IL-1) and tumor necrosis factor alpha (TNF-α).18,29,30 In vitro evidence indicates that PRP may inhibit the degradative effects of these cytokines, such as the downregulation of type II collagen and aggrecan gene expression.23,31 Recently, Sundman et al. 32 demonstrated that human synovium taken from knees with cartilage pathology expressed decreased TNF-α levels when cultured with PRP. Furthermore, synoviocyte hyaluronan synthase expression was increased in the presence of PRP. These findings mirror the conclusions drawn by Anitua et al. 33 who determined that PRP increased the secretion of hyaluronic acid by synovium cultured from osteoarthritic patients. As PRP has been shown to exhibit an effect on the joint as whole, affecting not only cartilage but also the synovium and intra-articular cytokine levels, it was decided that PRP would be administered as an intra-articular injection in this study. This contrasts with the aim of combining PRP with fibrin glue or other biological product to limit it to the confines of the osteochondral lesion.
There are discrepancies in the literature with respect to the fact that PRP has not been found to positively influence cartilage repair in all instances. An in vivo study conducted using a goat model by van Bergen et al. 34 concluded that PRP did not improve cartilage repair of an osteochondral lesion when combined with demineralized bone matrix. Similarly, Serra et al. 35 conducted a rabbit osteochondral lesion study comparing 7 intra-articular PRP injections with saline injections and found that the evolution of the healing tissue showed no difference between the 2 groups at 8 weeks postoperatively. The results of these studies, as well as other similar findings reported in the literature, may potentially be explained by the variance of adjuncts used in combination with PRP, including demineralized bone matrix, biomimetic scaffolds, and stem cells. Another potential explanation for the varying results seen in the literature may be the different formulations of PRP used in each study. While the term “platelet-rich plasma” implies a pure mixture of platelet and acellular plasma, this may not actually reflect the true composition of the biological product used in clinical practice. PRP may in fact be leukocyte-rich, leukocyte-poor, contain varying concentrations of growth factors, or be reduced to platelet-rich fibrin.11,36,37 To further compound this issue, the majority of studies fail to adequately characterize the cytological composition of the PRP used, thus making cross-study comparisons difficult. 10 While each rabbit in our study received a PRP injection, no correlation was found between the cytological components of the PRP (platelets, white blood cells, red blood cells) and the histological score. It is likely that a larger sample size may be required to determine optimum platelet, WBC and RBC concentration on cartilage repair. Studies have also used a myriad of adjuncts in combination with PRP, and it is likely that the interaction between the biologically active components of PRP and the adjunct (e.g., synthetic scaffold) cause different results than that of PRP in isolation. Last, there is a lack of uniformity in the literature regarding the optimum number of PRP applications, further compounding comparison between studies.
A potential limitation of the study is the model used for creation of an osteochondral donor site. While this is an established model in the rabbit, it is an acutely created defect. 13 This differs from the classic clinical presentation of an osteochondral lesion, which is often more chronic in nature. Therefore, the interaction of PRP with the defect and the joint itself in the animal in vivo setting may differ from what would take place in the clinical setting with a chronic osteochondral lesion. However, PRP may play a further role in healing acutely established osteochondral defects, such as those created at the osteochondral graft donor site in clinical practice. In this regard, Nosewicz et al. 38 noted in an ovine model that osteochondral donor sites show failure of defect closure at 6 months post-operatively. Donor site morbidity is a known complication of autologous osteochondral transplantation, and PRP may have the potential to mitigate this risk in the clinical setting.39,40
While the initial findings assessing the effect of PRP on patient reported outcome measures have been reported,5,7 there is little published literature quantifying the cartilage repair tissue found following PRP treatment. Ultimately, clinical trials assessing cartilage repair in the presence of PRP, performed using second-look arthroscopy and/or advanced noninvasive imaging techniques, will determine whether the results found in the basic science literature translate to clinical practice.
Conclusion
The results of this study indicate that PRP used as an intra-articular injection may improve cartilaginous healing of an osteochondral donor site in a rabbit model.
Footnotes
Acknowledgments and Funding
This study was funded through educational grants from Arteriocyte Inc., the Ohnell Family Foundation, and Mr. and Mrs. Michael J. Levitt, given directly to Hospital for Special Surgery. This funding was used for supplies and animal costs. No author received any financial benefit from this study.
Declaration of Conflicting Interests
One of the authors (JGK) serves as a consultant for Arteriocyte Inc. This relationship had no bearing on the study.
Ethical Approval
The Institutional Animal Care and Use Committee approved all surgical procedures and experimental designs.