
Abstract
The prevalence of focal articular cartilage lesions among athletes is higher than in the general population. Treatment goals differ considerably between the professional and recreational athlete. High financial stakes and the short duration of a professional career influence the treatment selection for the professional athlete, while such parameters weigh differently in recreational sports. This article describes our investigation of the relation between sports and a high prevalence of focal cartilage lesions. In addition, we provide a critical review of the best available evidence for cartilage surgery and treatment selection, evaluate specific patient profiles for professional and recreational athletes, and propose a treatment algorithm for the treatment of focal cartilage lesions in football (soccer) players.
Introduction
Traumatic or degenerative focal articular cartilage lesions can cause serious reduction in sports performance. In addition, they may lead to disabilities during activities of daily living. This particularly counts for high-demanding sports such as basketball, American football, and football (soccer), where fast acceleration, deceleration, and pivoting movements are frequently executed. Related symptoms such as pain, swelling, catching, and locking make focal cartilage lesions an important reason to avoid further sports participation.1-3 Among professional athletes, where the demands of the articular cartilage are even higher, this problem is more significant. 1 After the meniscus and the anterior cruciate ligament (ACL), the articular cartilage of the knee is one of the most frequently damaged structures in football (soccer) players. In addition, injury to the articular cartilage is known as the most important cause of functional disability and may lead to early degenerative changes in the knee joint during, and after, a professional sports career. 4 Several surgical treatments for focal articular cartilage lesions in the general population have proven to be effective. Consequently, evidence-based treatment algorithms have been designed and clinically applied.5,6 However, treatment goals differ between recreational and professional sports players. Recreational players mainly hope for a relief of pain, return of functionality, and if possible, some sports participation, while professional players need a fast return to their previous, high-demanding, activity level without the blemish of having joint damage. Also, the generally short duration of the professional career makes a rapid recovery even more desirable.
The above-mentioned situation creates a delicate clinical dilemma for the responsible physician. Because of the excessive forces exposed to the regenerated cartilage and the wish for a fast rehabilitation, the treatment strategy for professional athletes might be different from those for recreational athletes. Ending contracts, high financial stakes, and commitments towards the professional sports organization could also influence the process towards an optimal patient-based treatment strategy. Therefore, understanding the need for good-quality cartilage regeneration in high-impact sports is necessary and should be the basis for a proper personalized treatment selection. Emphasis should lie on functionality during the sports career as well as quality of life afterwards.
This review describes the current ideas on why football (soccer) players have an increased risk for the development of focal articular cartilage lesions and reviews the best available evidence for treatment selection in cartilage surgery for football (soccer) athletes. Based on this, we propose a treatment algorithm suited for the individual professional and recreational football (soccer) athlete with a focal articular cartilage lesion.
High-Activity Demands and the Development of Focal Articular Cartilage Lesions
The current literature suggests that high-impact activities and thereby stresses to the articular cartilage may lead to temporary or permanent changes in cartilage and subchondral bone turnover and architecture.7-9 High-impact activities have been linked to increases in biomarker profiles as well as changes in cartilage homeostasis.10,11 Taking this into account, a pattern of repetitive exposure of the articular cartilage to mechanical stresses could slow cartilage recovery instead of improving the biomechanical resistance, which will potentially lead to the development of full-thickness articular cartilage defects.
For the football (soccer) player, the intensity of high stresses and pivotal movements to the knee is extreme due to the demanding training programs and, for the world-class football (soccer) players, as often as 3 competitive games a week. Therefore, the documented high prevalence (35%; range, 18%-63%) of focal articular cartilage lesions among professional and recreational athletes, compared to a prevalence of 5% to 11% in the general population, is a logical result of the high-demanding professional career. This exemplifies the need for better understanding of the impact and evaluation of treatment outcomes.1,12-14
Surgical Techniques for the Professional Athlete with a Focal Articular Cartilage Lesion
Marrow stimulation techniques, such as microfracture, and transplantation methods, such as autologous chondrocyte implantation (ACI) and osteochondral autologous transplantation (OAT), are the most frequently applied treatment options for the surgical restoration of focal articular cartilage lesions. The purpose of the microfracture technique is to create micropenetrations into the subchondral bone of the debrided focal cartilage defect in order to allow bone marrow, consisting of multipotent stromal cells (MSCs), to enter the intra-articular space. This should form a clot in the cartilage defect populated with MSCs and growth factors that eventually leads to functional fibrocartilaginous tissue.15,16 In ACI, as clinically described by Brittberg et al., autologous chondrocytes are harvested from a nonweightbearing location in the knee, expanded in vitro, and reimplanted in a second surgical procedure. 17 Over the years, this technique has evolved into several generations, all aiming at a more reliable biological response, improved ease of surgical use, and a better clinical outcome. 18 One such example is the matrix-associated chondrocyte implantation (MACI), which reduces donor site morbidity by avoiding the use of a periosteal flap. Moreover, the implantation of cultured cells in 3-dimensional matrices reduces the surgery-related morbidity and facilitates faster rehabilitation as it can be performed by a mini-arthrotomy or even arthroscopy. 19 During the OAT procedure, osteochondral plugs are harvested from nonweightbearing locations in the knee and transplanted to the osteochondral defect. 20 Although clinical efficacy has been demonstrated, the drawback of this technique is the large donor site morbidity, which occurs in at least 5% of patients. 21
Clinical Outcome after Cartilage Regeneration in the Professional Athlete
We conducted an extensive PubMed and EMBASE literature search to find the best available evidence for clinical outcome after cartilage regeneration in the athletic population. Search terms were [cartilage] AND [knee] AND [athlete OR sport(s)]. The search resulted in 198 hits (161 PubMed, 37 EMBASE). After careful consideration, 14 relevant articles could be selected and were compared to the available literature of cartilage regeneration in the general population. The results after cartilage surgery in the athletic population are described in several cohort studies for different professional sports. Microfracture showed a statistically significant improvement from baseline in functional outcome, pain scores, and Tegner activity levels after at least 1-year follow-up among professional football (soccer) players and other athletes.22-25 ACI showed an improvement from baseline in functional outcome and pain scores and an even higher good to excellent treatment success in professional football (soccer) players and adolescent athletes compared to microfracture (66%-83% for microfracture vs. 72%-95% for ACI).24,26,27 Also, Tegner activity levels were significantly higher after ACI in football (soccer) players.26,27 The OAT technique showed superior clinical results compared to microfracture in a randomized study among both professional and recreational athletes. 23 Also, prospective case series show good clinical results up to 17 years’ follow-up in a mixed athletic population. 21
The average time to return to professional sports is highest after ACI (18 ± 4 months; range, 12-36 months) compared to microfracture (8 ± 1 months; range, 2-16 months) and OAT (7 ± 2 months; range, 4-11 months). 28 For the general population, good to excellent long-term clinical results after OAT, microfracture, and ACI have been described up to 17 and 20 years, respectively.21,29,30 For the professional athlete, the longest follow-up with good clinical outcome after ACI and microfracture we found is currently 5 years. 31 For OAT, the longest follow-up, with acceptable clinical results, was 8 years and was described in a prospective case series, which partly consisted of professional athletes. 21 Although some evidence exists for the treatment of focal articular cartilage lesions in the professional athlete, good-quality evidence is still lacking.
Treatment Selection and Patient Profiling in the Professional and Recreational Football Player
Evidence-based treatment selection for the treatment of focal articular cartilage lesions in the general and recreational sports population is mainly based on the size of the lesion and the involvement of the bone.5,23,32-35 ( Fig. 1 ). Clinical outcomes relevant for this population, such as pain reduction and functional improvement, were taken into account when developing these algorithms.5,32-35 However, a return to the preinjury sports activity level is much more important when dealing with high-level football (soccer) players. In addition, articular cartilage repair in these patients not only requires a regenerative product that can withstand the previously mentioned excessive shear stresses and pivoting movements during the career but should also be capable of allowing a normal function after this. Saris and Vanlauwe showed that characterized autologous chondrocyte transplantation (CCI) resulted in higher histomorphometric and histological scores, and thus better structural repair, when compared to microfracture in the general population. This coincided with a higher clinical outcome as measured by the overall Knee injury and Osteoarthritis Outcome Score (KOOS) with significant improvement in the Sports and Quality of Life domains for at least 3 years.35,36 Others also reported a more fibrocartilaginous appearance of the repair tissue after microfracture compared to ACI or OAT for nonathletes.23,32,33 In addition, return to the previous professional sports activity level was higher in ACI- and OAT-treated athletes (range, 83%-100%) compared to microfracture-treated athletes (range, 44%-100%).23-27,31,37 Moreover, Mithoefer et al. showed a decline in sports performance and participation, after full rehabilitation, for microfracture-treated athletes in 47%, while at least 87% of ACI-treated professional football (soccer) players remained at their previous sports level after rehabilitation for an average of 52 months.24,27 Also, a decline in clinical results after 18 months was observed for patients in the general population when treated with microfracture, indicating a less stable regenerative product. 38
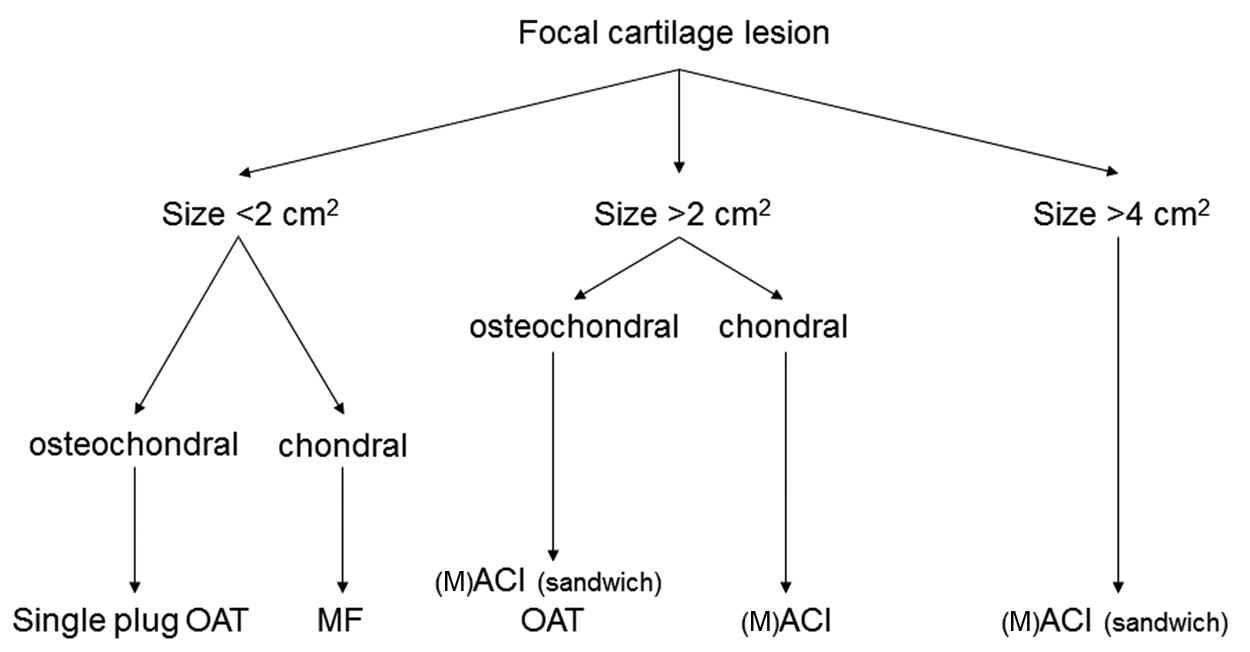
Evidence-based treatment algorithm for the treatment of focal articular cartilage lesion in the general population. (M)ACI = matrix autologous chondrocyte implantation.
Frequently, articular cartilage lesions are accompanied by other injuries in the knee like ACL ruptures or meniscal tears. A systematic review of 5 different case series calculated that the incidence of severe articular cartilage lesions in patients with an acute ACL rupture is 16% to 46%. 39 Also, Joseph et al. showed that an increasing treatment delay, up to 3 years, after an ACL injury led to a higher incidence of articular cartilage and meniscal lesions in both an athletic and nonathletic cohort. 40 Therefore, detection and direct treatment of ACL lesions in football (soccer) players are very important and should be performed as soon as possible after the trauma. If articular cartilage lesions are present during ACL reconstruction, they should also be treated directly. Their treatment selection should not differ from an articular cartilage lesion without a concomitant ACL rupture. Furthermore, Amin et al. showed that the combined treatment of articular cartilage lesions and ACL ruptures resulted in better clinical improvement compared to ACI following previous ACL reconstruction. 41
Although ACI and OAT seem to lead to a better structural repair and are more likely to result in total resumption of the previous activity level, it is not the treatment of first choice among professional athletes and their supporting medical staff. For the professional football (soccer) career, the timing of return to the preinjury level is at least as important as the remaining period to be played at the preinjury level. Also, because of the long rehabilitation time after ACI, microfracture is mainly considered the first treatment option among professional football (soccer) players. This may be incorrect given the long rehabilitation period and specific phases of tissue maturation also described for microfracture. 42 From the athlete’s point of view, microfracture is a reasonable choice as it is a safe and simple technique and allows their career to continue for at least a couple of years. However, given the shorter average rehabilitation time after OAT, compared to microfracture and ACI, this technique could also be a valuable alternative for microfracture when the lesion requires direct treatment and a short rehabilitation time is desirable. If ACI is the treatment of first choice, a surgical debridement of the acute or immediately symptomatic focal lesion with additional cartilage biopsy may be indicated to relieve symptoms during the season. Depending on the upcoming seasonal program, the reimplantation of cultured cells could be delayed to the off-season period to allow a rapid return to professional sports with the possibility of durable structural tissue regeneration.
When dealing with professional and recreational players at the beginning of their career, the responsible physician should also take the need for long-term performance of the regenerated cartilage into account. With this in mind, the better structural repair after ACI and OAT and the decrease in treatment success over time after microfracture are reasons to consider ACI or OAT as a first-line treatment option for these young sportsmen. For focal lesions >2 cm2, microfracture and OAT showed significantly worse clinical outcomes and a lower return to high-level sports when compared to lesions <2 cm2.23,24,43 For ACI, no influence on lesion size and clinical outcome or return to sports participation has been found, which indicates that for larger lesions, ACI is the treatment option of first choice for both professional and recreational sports athletes. In addition to lesion size, other patient characteristics that predict the clinical outcome after cartilage surgery in the athlete could also be helpful to develop individual, professional athlete–oriented, treatment strategies. For professional football (soccer) players and other high-level athletes with symptoms <12 months, Mithoefer et al. found a better clinical outcome and greater return to sports after microfracture as well as ACI.24,26,27 Also, when treated with OAT, the chronicity of the lesion seemed important on clinical outcome and return to sports.43,44 Similar trends are observed in the general population, where patients with symptom duration less than 2 years present better clinical scores compared to those with a symptom duration longer than 2 years.35,45 In addition, age has been found to be an important predictor in the athletic as well as general population. Football (soccer) players who successfully returned to competition after ACI were significantly younger (<25 years old), and overall better clinical results are observed in athletes and nonathletes <30 years old.5,23,27 The influences of both symptom duration and age of the athlete with a focal articular cartilage lesion are reasons to aim for early treatment.
Rehabilitation after Cartilage Surgery in Professional Football Players
Rehabilitation of football (soccer) players after articular cartilage repair is essential for optimal function and return to preinjury game levels. Although high-level studies are lacking, this section will provide an overview of the current thoughts and evidence on rehabilitation after cartilage surgery. In general, current rehabilitation protocols can be divided into several phases aiming at protection of the graft by a gradual increase in weightbearing and active range of motion. This may enhance graft maturation, remodeling, and integration. 46
Recently, more aggressive rehabilitation protocols, with early full weightbearing after ACI, were successful, without damaging the graft.47,48 In addition, compared to the current rehabilitation protocols, less pain was reported at 3 months, while similar KOOS scores were obtained at 2 years’ follow-up.47,48 Also, the presence of low-load activities during the first 3 months after surgery seemed to positively influence the clinical outcome after 2 years. 49 The approach of aggressive rehabilitation was also described for competitive football (soccer) athletes with a focus on football-specific joint loading and an early return to on-field exercises. 50 This approach showed a return to the previous, highly active, sports level within 11 months after ACI without jeopardizing the graft. In addition, the clinical improvement achieved after 1 year remained stable for a period of at least 5 years’ follow-up. 50 Although protection of the graft is important in the rehabilitation program after cartilage surgery, a more aggressive rehabilitation program could facilitate graft maturation without risking graft damage.
Discussion
This article reviewed the best available evidence for treatment selection in cartilage surgery for football (soccer) players. We acknowledge that the majority of best available evidence consisted of cohort studies and case series while some randomized studies were also included. Therefore, careful consideration of the literature is warranted. The current lack of good-quality evidence on this topic should be a motivation to facilitate good-quality prospective cohorts and maybe, in the correct environment, randomized studies for the treatment of focal articular cartilage lesions in athletes using validated outcome instruments such as suggested by Bekkers and Hambly.51,52
A high prevalence of focal articular cartilage lesions among athletes can be explained by both acute traumatic defects and the repetitive high-impact loading of the cartilage matrix with concomitant change in chondrocyte metabolism. For this reason, regenerative cartilage surgery in the professional and recreational athletes should aim at structural repair for a long period of time to withstand the high-impact loading during return to active sports. Although protection of the graft is important in the rehabilitation program after cartilage surgery, a more aggressive rehabilitation program could facilitate graft maturation without risking graft damage. 50 The high quality of the rehabilitation facilities and the availability of experienced physicians in (professional) sport organizations creates a perfect environment for a more aggressive rehabilitation approach after cartilage surgery. With this in mind, the rehabilitation time after ACI could be reduced, supporting earlier return to competition.
Taking the above mentioned into account, ACI and OAT can be given a more prominent place in the treatment of focal articular cartilage defects in athletes because both treatments lead to higher postoperative sports activity when compared to microfracture. If direct treatment of focal lesions <2 cm2 is required, the OAT procedure should, next to microfracture, be considered. However, for lesions >2 cm2, the clinical outcome and sports resumption after ACI do not deteriorate in time, which is quite different in other treatment strategies like microfracture and OAT. Therefore, surgical debridement of the focal lesion during the season, combined with a biopsy for a possible off-season ACI procedure, may warrant a decrease in loss of playing minutes and allows faster return to competition within a single noninternational team football (soccer) season. Consequently, athletes should be re-evaluated, and indications for ACI should be reviewed during the off season. For athletes at the end of their career with a lesion <2 cm2, microfracture or OAT are suitable treatment options, both providing a fast return to competition and therefore more chance at (a remainder of) play.
Based hereon and taking the best available evidence into account, we propose a treatment algorithm for football (soccer) athletes that takes the timing of surgery into account and can be modified to the individual needs and upcoming seasonal program of the athlete ( Fig. 2 ). Improvement in the surgical techniques with sophisticated graft biology, less surgery-related morbidity, and faster recovery, combined with new insights on rehabilitation programs aiming at an earlier load-bearing regime, will make the combination of fast return to play with good-quality cartilage repair possible on an individual basis for highly active football (soccer) athletes.
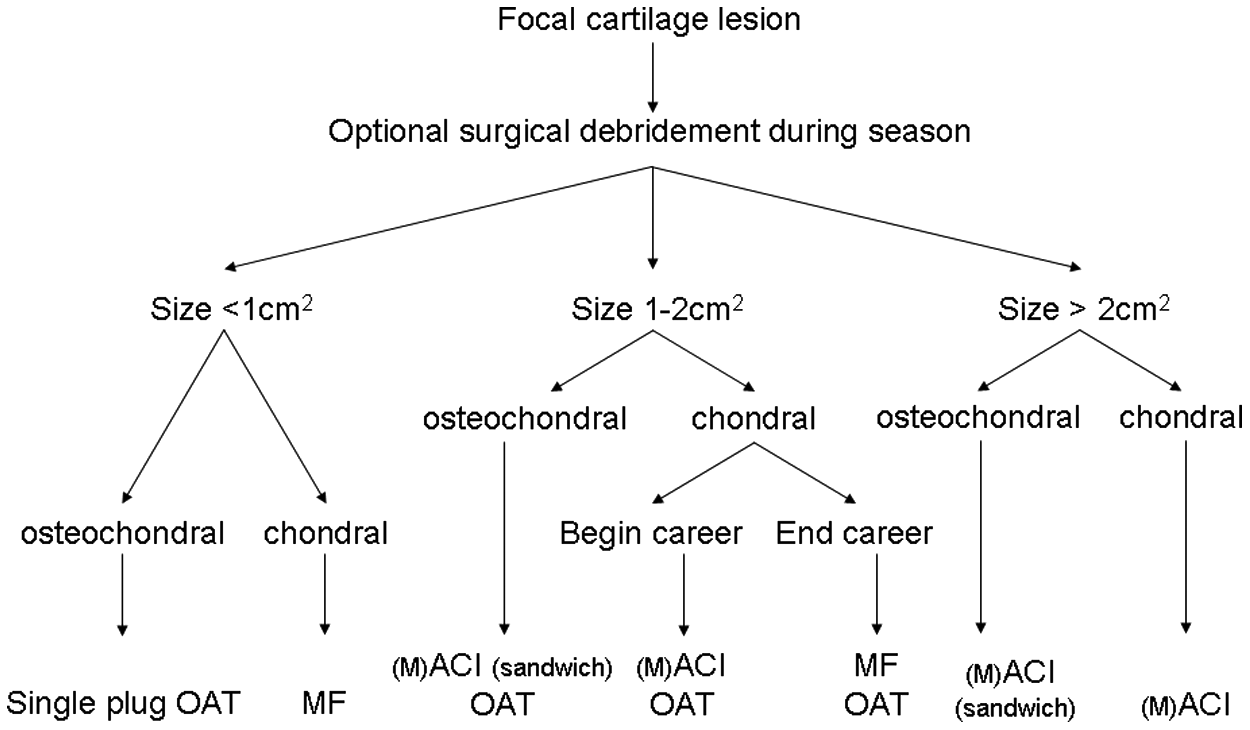
Treatment algorithm for the treatment of focal articular cartilage lesions in (professional) football players based on the best available evidence. (M)ACI = matrix autologous chondrocyte implantation.
Footnotes
Acknowledgements
The authors greatly acknowledge the support of the TeRM Smart Mix Program of the Netherlands Ministry of Economic Affairs and the Netherlands Ministry of Education, Culture and Science.
The authors received no financial support for the research and/or authorship of this article.
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.