
Abstract
Objective:
This is the first report of successful allograft mosaicplasty treatment of a large osteochondral lesion of the knee caused by a blast fragment sustained during combat operations. The patient was able to return to active duty following rehabilitation.
Methods:
An active-duty infantryman sustained an osteochondral lesion of the medial femoral condyle caused by a metallic fragment of an explosively formed projectile. Initial treatment consisted of removal of the foreign body and primary closure. The patient continued to experience pain, mechanical symptoms, and repeated effusions after initial nonoperative treatment. Allograft mosaicplasty of the lesion utilizing two 18-mm-diameter fresh allograft osteochondral plugs was performed at 6 months post-injury.
Results:
At 2-year follow-up, the patient remains on active duty with marked improvement in symptoms. Two years postoperatively, his outcome scores are 72 of 100 on the Western Ontario and McMaster University osteoarthritis scoring index (WOMAC) and 60 of 100 on the Knee Injury and Osteoarthritis Outcome Score (KOOS). His follow-up x-rays and MRI demonstrate intact articular cartilage and subchondral bone incorporation.
Conclusion:
Penetrating injuries to joints are commonplace in the battlefield environment. Combat injuries to the knee are frequently associated with articular cartilage injury. While numerous cartilage restoration techniques have been used with success for the treatment of osteochondral injuries to the femoral condyles, no published reports describe the use of allograft mosaicplasty in this location for open, penetrating injuries with focal cartilage loss. This is the first documented use of allograft mosaicplasty for a traumatic osteochondral defect of the medial femoral condyle caused by a metallic projectile. The patient was able to return to active duty following rehabilitation. We demonstrate a high level of functioning is possible following allograft mosaicplasty of a large osteochondral lesion caused by penetrating ballistic trauma.
Introduction
Penetrating injuries to the knee are encountered both in civilian trauma and during military combat operations.1-9 In the military, these injuries most frequently result from explosive blasts or bullets. 10 Aside from the soft tissue involvement, these open wounds may involve varying degrees of bone and cartilage destruction. 5 In addition to irrigation, debridement, and soft tissue repair, multiple other modalities may be required for successful treatment of these injuries.
Mosaicplasty procedures have been employed to treat large, full-thickness loss of cartilage in multiple joints of the extremities. 11 Both autograft and allograft procedures have been described. While the majority of reports on osteochondral lesions of the knee describe trauma as the pathoetiology, none specifically describe the use of mosaicplasty for injuries caused by projectiles.11-15
Case Report
Permission was obtained from the patient to allow publication of his treatment history and radiological images. On the evening of 30 October 2006, a 34-year-old male U.S. Army infantry officer sustained multiple injuries after his armored troop transporter was struck by an explosively formed projectile (EFP) while on patrol with his unit just outside of Baghdad, Iraq. EFPs are a particularly lethal form of armor-penetrating improvised explosive device (IED) that have been employed by insurgent forces in Iraq. 16 Following the attack, the patient was unable to ambulate because of pain in his right leg and knee.
The patient was evacuated to the 28th Combat Support Hospital in Baghdad, where a full trauma work-up was performed. The ATLS survey finding was negative. During the secondary survey, his injuries were noted to include penetrating wounds to his lower extremities, scrotum, and perineum. The largest of the penetrating wounds was a 2-cm laceration just medial to the inferior pole of his left patella. The patient had a normal neurovascular and ligamentous examinations result in the affected extremity. Range of motion measurements of the knee were substantially limited by pain. Radiographs revealed an irregular radiodense piece of fragmentation in the anterior soft tissues of the knee ( Fig. 1 ). Because it was unclear from the imaging whether the fragment had breached the joint capsule, a 50-mL sterile saline challenge to the knee joint was performed.17,18 An open knee injury was diagnosed after injected saline was noted to be draining through the inferomedial knee wound. The patient consented for irrigation and debridement of the left knee as well as surgical treatment of his genital injuries.
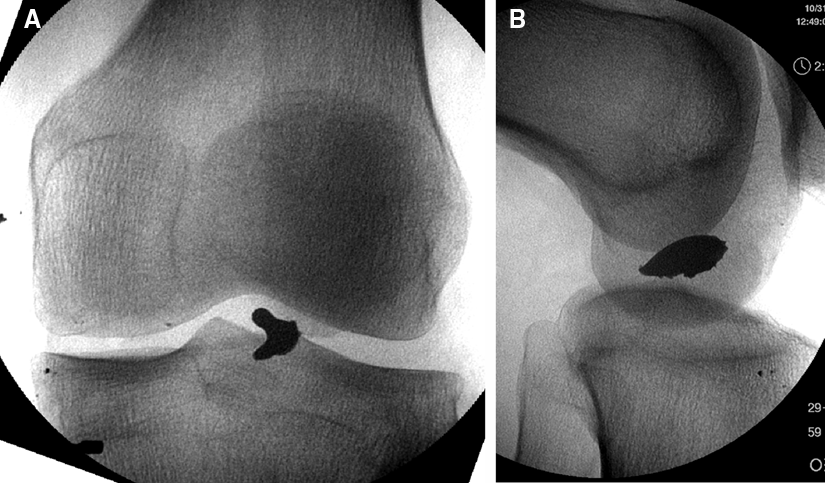
Initial anteroposterior (
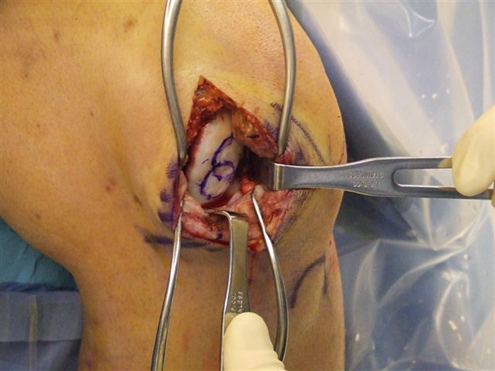
In the operating room, a limited medial parapatellar arthrotomy was performed by extending the traumatic wound. Upon exploring the wound, a large metallic fragment was found within the anterior fat pad ( Fig. 2 ). It measured 2.5 × 1.0 × 0.4 cm. The adjacent joint capsule was noted to be lacerated. This defect was extended to reveal a 3 × 2-cm area of full-thickness cartilage loss from the lateral portion of the medial condyle. In addition to the cartilage loss, a portion of the corresponding subchondral bone was noted to be denuded. The joint was further explored through the wound and irrigated with 9 L of sterile saline. No loose bone, cartilage, or additional foreign material resembling the area of osteochondral loss was found in the joint or soft tissues. A layered closure of the joint was performed after all devitalized tissue was debrided. There was no loss of integument associated with the injury. The remainder of his lower extremity wounds were irrigated and debrided followed by open management. He underwent left orchiectomy for irreparable testicular damage, and his remaining perineal wounds were debrided and treated with open management. The patient was subsequently evacuated back to the authors’ medical facility within 10 days.

Knee at time of debridement with extracted metallic fragment.
Initially, following healing of the soft tissues, the patient was treated with active range of motion of his injured knee and protected, partial weightbearing for 8 weeks. During this initial rehabilitation period, the patient complained of significant pain, repeated effusions, and mechanical symptoms, making weightbearing very difficult without the aid of crutches. He received additional imaging, including a computed tomography (CT) scan ( Fig. 3 ), which revealed a 3.2 × 1.9-cm lesion on the medial condyle. A discussion of possible treatment options was undertaken, and the patient opted to undergo allograft mosaicplasty of the lesion. Once an allograft condyle became available, the patient was taken to the operating room for arthroscopy followed by allograft mosaicplasty of the lesion at 6 months postinjury.

Sagittal computed tomography (CT) image showing the medial femoral condylar traumatic defect 4 months after injury.
Intraoperatively, the patient’s knee was ligamentously stable, and arthroscopic evaluation confirmed the dimensions of the lesion. A small horizontal cleavage tear of the medial meniscus was discovered and debrided. Following arthroscopy, a 10-cm medial parapatellar arthrotomy was performed, allowing access to the condylar lesion ( Fig. 4 ). A decision to utilize two 18-mm-diameter allograft osteochondral plugs was made. The donor plugs were obtained from a size-matched, fresh allograft femoral condyle (Allosource, Centennial, CO) using a commercially available harvesting system. These plugs were implanted into the area of the lesion after the diseased tissue had been removed using complementary sized drill bits ( Fig. 5 ).
Intraoperative image of the right knee medial femoral condylar lesion prior to mosaicplasty.

Intraoperative image of the right knee after inserting allograft plugs.
After surgery, the patient remained nonweightbearing on the operative leg for 3 months but was allowed unrestricted range of motion. Transition to weightbearing activities and resistance training ensued. The patient was able to return to weightbearing activities with minimal discomfort. Although released to full activity, he remains limited in running and marching with full combat gear (approximately 80 lb of protective gear and equipment). Two years postoperatively, his outcome scores are the following: Western Ontario and McMaster University osteoarthritis scoring index (WOMAC), 72 of 100; and Knee Injury and Osteoarthritis Outcome Score (KOOS), 60 of 100. His follow-up x-rays and MRI demonstrate intact articular cartilage and subchondral bone incorporation ( Fig. 6 ). He remains on active duty at 2-year follow-up.
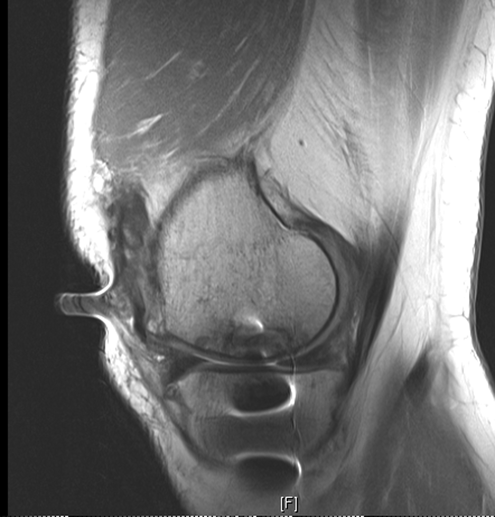
Sagittal fat-suppressed magnetic resonance image of the knee 2 years following allograft mosaicplasty.
Discussion
Penetrating injuries to joints, particularly knees, are commonplace in the battlefield environment.1,5,19,20 In one series, knee trauma accounted for 50% of joint injuries. 5 Combat injuries to the knee are frequently associated with articular cartilage injury. 20 Although less common than those caused by blunt trauma, penetrating articular injuries occur in noncombat-related incidents. In the noncombat environment, these frequently arise from gunshot wounds.16,21,22 The current conflicts have produced large numbers of knee injuries from blast mechanisms. Unfortunately, many of these injuries have large amounts of comminution, affecting limb stability and greatly complicating reconstructive efforts. Although substantially less common, we do not know the incidence of focal, nondestabilizing osteochondral lesions resulting from blast injury in the Global War on Terror.
Several case series report generally “good” outcomes in patients treated for penetrating ballistic injuries without defined follow-up periods or objective outcome measurements.5,8,20,23 These patients were treated with arthroscopic debridement of foreign and loose bodies without further procedures. Regarding focal cartilage lesions, only “drilling” of these defects has been described outside of a single report of allograft reconstruction for extensive bone loss of the medial femoral condyle following a gunshot wound to the knee. 6 No objective analysis of outcome was provided in this report.
While numerous cartilage restoration techniques have been used with success for the treatment of osteochondral injuries to the femoral condyles, no published reports describe the use of allograft mosaicplasty in this location for open, penetrating injuries with focal cartilage loss. To the best of our knowledge, this is the first documentation of allograft mosaicplasty used for reconstruction of a traumatic osteochondral defect of the medial femoral condyle caused by a metallic projectile.
Although the use of allograft mosaicplasty was successful in our patient, it is not appropriate for all patients with focal osteochondral lesions of the femoral condyles caused by penetrating trauma. Some patients may sustain osteochondral injuries that are large and amenable to reduction and fixation, while small articular lesions (less than 0.5-1.0 cm, depending on location) may be treated with debridement, microfracture, or abrasion chondroplasty. 24 For small articular cartilage lesions, it is prudent to first attempt less invasive methods such as arthroscopically assisted marrow stimulation techniques. 25 Larger lesions (measuring greater than 2.0-3.0 cm2 in area), such as the one encountered in our patient, have been treated successfully with a variety of methods including autologous chondrocyte implantation (ACI) as well as both autograft and allograft mosaicplasty.11,25,26 Given the size of this patient’s lesion and the involvement of the subchondral bone, we felt the best treatment was allograft mosaicplasty. Treatment of articular cartilage lesions is clearly dependent on several variables including patient factors, available resources, and surgeon capabilities. All factors must be taken into consideration when planning treatment. With the high percentage of penetrating knee injuries resulting in articular cartilage injury, it is important to both accurately diagnose the lesions and choose a proper method of articular resurfacing.
This case report describes successful management of a large osteochondral injury to the medial femoral condyle using allograft mosaicplasty in an active-duty serviceman. We demonstrate the utility of this technique for military as well as civilian orthopedic surgeons faced with similar scenarios.
Footnotes
Acknowledgments and Funding
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of the Army or the Department of Defense. The authors thank Allosource for their continuing support of the United States Military and its service members. The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.