
Abstract
Objective:
The goal of this report is to describe the outcome of sequential particulated cartilage allograft and autologous osteochondral transfer treatments for an osteochondral lesion of the medial femoral condyle.
Methods:
A 44-year-old woman was treated with a particulated juvenile articular cartilage allograft (DeNovo NT) for a chondral lesion of the knee. As a result of continued pain, she had 2 further surgeries, including an autologous osteochondral transfer system procedure and finally a unicondylar knee arthroplasty. At the final procedure, the areas of the allograft and autograft tissue were biopsied for histological evaluation. The quality of the residual cartilage tissue was assessed first by equilibrium partitioning of an ionic contrast agent via micro–computed tomography (EPIC-µCT), and then by hematoxylin and eosin, Safranin O staining, and polarized light microscopy.
Results:
Despite showing good healing at 7 months postsurgery by MRI, at 28 months post DeNovo NT tissue implantation the excised cartilage tissue was heterogeneous, with some regions of hyaline-like cartilage and some regions of fibrocartilage. The later mosaicplasty may have helped maintain hyaline-like cartilage of the DeNovo NT tissue in its vicinity.
Conclusion:
This case report describes the cartilage repair tissue produced by DeNovo NT implantation and compares it with autologous osteochondral plug tissue.
Introduction
Osteochondral lesions of the knee represent a large spectrum of injuries that range from softening and fibrillation of cartilage to complete loss of cartilage and bone. Techniques such as abrasion chondroplasty, drilling, or microfracture promote lesion infilling with fibrocartilaginous scar tissue. This tissue, which is predominantly composed of type I collagen, has poorer mechanical properties than the native hyaline cartilage. 1 Newer salvage techniques such as autologous osteochondral transplant, autologous chondrocyte implantation, and particulated juvenile articular cartilage have been developed in an attempt to repair the lesion with hyaline cartilage.
This study describes the treatment performed on a 44-year-old woman who had previously undergone 2 meniscectomies and was still experiencing knee pain. DeNovo NT (Zimmer, Warsaw, IN) is a scaffold-free tissue, which can be used as a single-stage procedure for the repair of articular cartilage lesions and is typically sealed in place with fibrin glue. The tissue is procured from donors 13 years or younger since higher levels of type II collagen and proteoglycan production are typically seen in cartilage donors from this age group compared with adults. 2 To the best of our knowledge there have been no reported cases of equilibrium partitioning of an ionic contrast agent via micro–computed tomography (EPIC-µCT) analysis or histological findings from particulated juvenile articular cartilage allograft tissue treatment.
Case Report
We detail a case of an active patient who initially presented to our clinic at the age of 44 years. She had complaints of left medial side knee pain and had already undergone 2 partial medial meniscectomies that had not resulted in any pain relief and so prompted our evaluation. The preoperative workup included an MRI and a long-leg frontal hip–knee–ankle alignment radiograph. She was noted to have varus malalignment and a full-thickness chondral lesion of the medial femoral condyle (MFC) measuring 22 mm wide by 36 mm long ( Fig. 1A ). She was counseled on all surgical and nonsurgical options and elected to undergo a joint preserving salvage surgery. A high tibial valgus producing open wedge osteotomy was performed. At the same setting, the calcified subchondral layer was debrided and the chondral lesion was filled with particulated juvenile articular cartilage allograft (DeNovo NT) and sealed in place with fibrin glue.
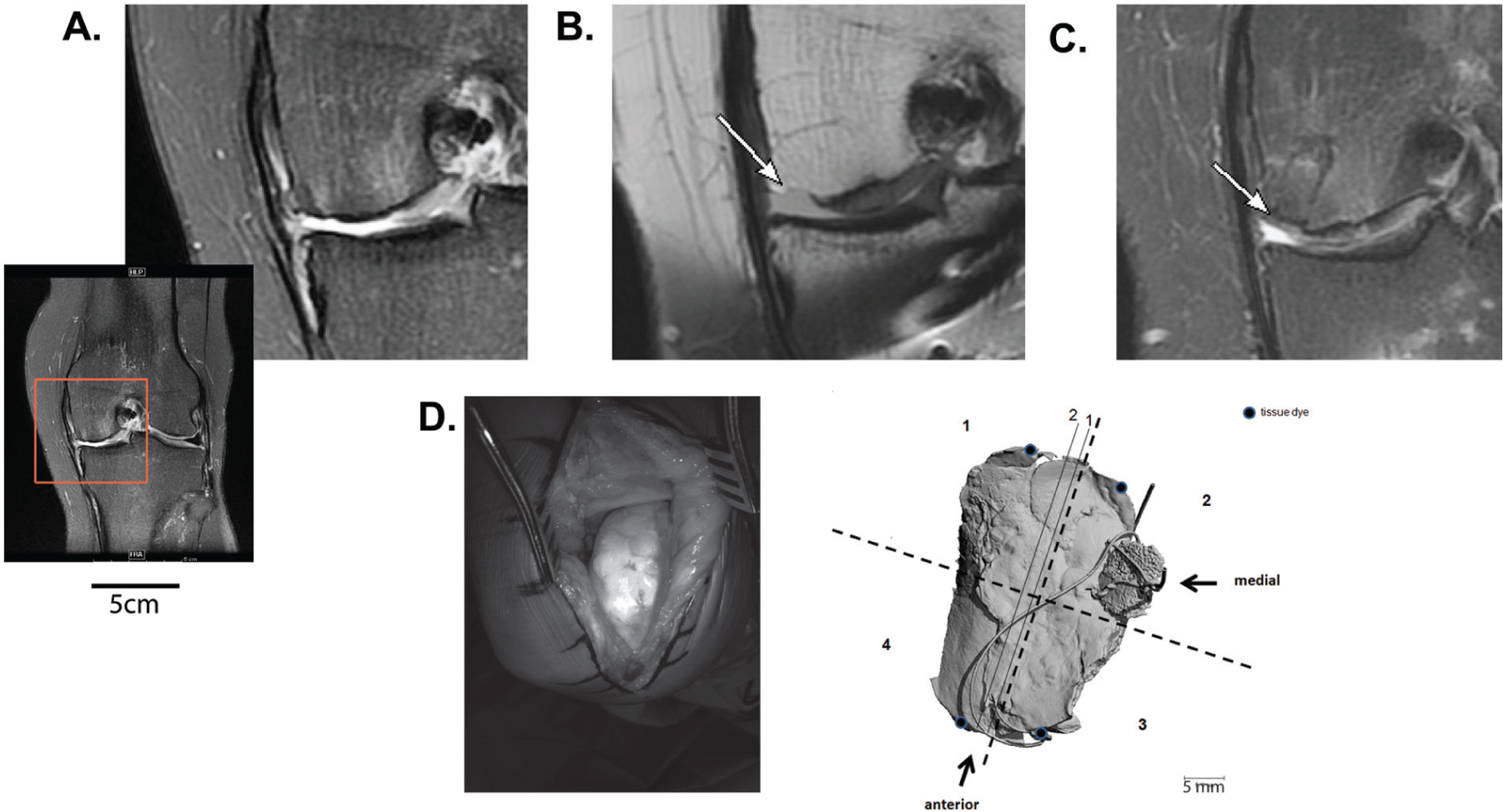
MRI and sample processing. (
The patient had improved pain after the procedure as her preoperative visual analogue scale (VAS) score was 8/10 and she had an improvement to 3/10. A routine follow-up MRI was performed at 7 months postoperation to evaluate healing which showed a residual lesion of 8 mm wide by 21 mm long on the medial aspect of the initial lesion ( Fig. 1B ). The patient returned to the clinic 13 months after the procedure with complaints of worsening of medial side knee pain with her VAS pain score increased to 5/10 to 6/10 with activity. She was also experiencing pain at the site of the hardware. Another MRI was obtained that showed no change in lesion size from the previous MRI. In an attempt to continue with the salvage effort, the patient elected to proceed with the removal of hardware followed by an osteochondral autologous transfer to address the residual lesion in the MFC. At the time of surgery, we found the residual lesion to be 6 to 10 mm wide by 28 mm long, indicating a 72% surface area reduction compared with the original lesion. The area of the DeNovo NT tissue that had healed showed stable cartilage, which had an appearance and turgor comparable to the native surrounding cartilage. The area that had a residual osteochondral lesion was directly opposite the site where the previous partial menisectomy had been performed. Two 10 mm and one 6 mm diameter autologous osteochondral plugs were harvested from the lateral trochlea and used in a mosaicplasty fashion to fill the lesion ( Fig. 1C ).
Postoperatively, the patient’s pain was decreased after the autologous osteochondral transfer, but she continued to have pain with moderate impact activities. A course of viscosupplementation injections also failed to improve her activity-related pain. At this time it was felt that joint preservation options had been exhausted. At approximately 28 months after her index procedure, the patient underwent a medial unicompartmental knee arthroplasty. At the time of unicompartmental knee arthroplasty, the area of the autologous osteochondral plugs, which was easily defined from the surrounding cartilage, appeared well healed and the cartilage appeared normal on gross examination ( Fig. 1D , photograph). The area of the DeNovo NT tissue also had good turgor, stability, and cartilage coverage. There was full-thickness cartilage loss on the MFC posterior to the area of previous cartilage repair. Samples of the tissue from the MFC, which included both areas of DeNovo NT tissue and autologous osteochondral plugs, were harvested. The tissue was subsequently fixed in 10% neutral buffered formalin at 4 °C for 48 hours. Once EPIC-µCT scanning was complete, the tissue was decalcified in Cal Ex II (Fisher Scientific, Waltham, MA) for 14 days and then divided into 4 segments ( Fig. 1D , µCT image) before paraffin embedding.
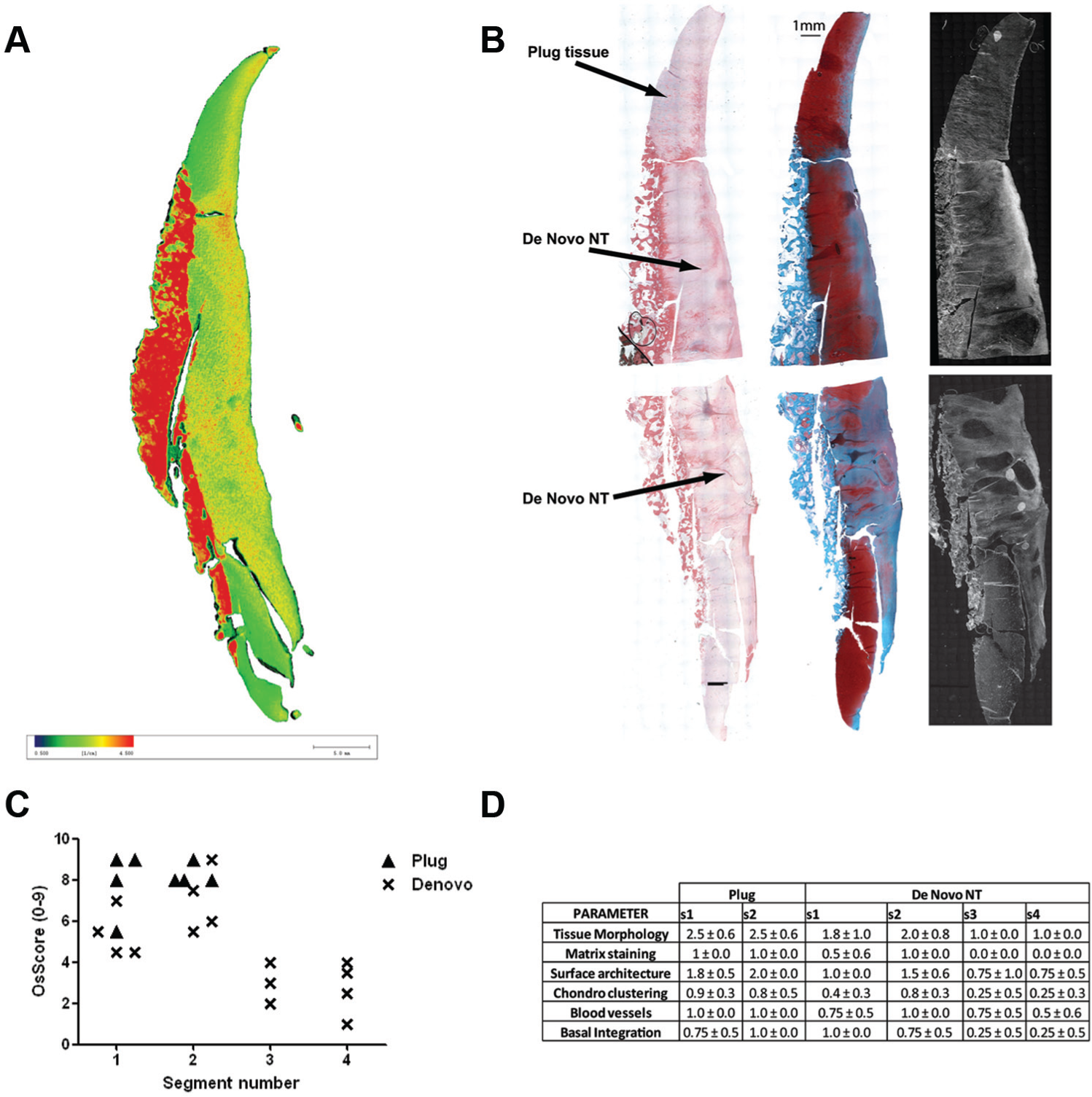
The µCT images showed a heterogeneity of signal attenuation within the DeNovo NT tissue with areas of high attenuation being indicative of low proteoglycan content ( Fig. 2A ). Histologically, the DeNovo NT tissue in segments 1 and 2 (i.e., in the vicinity of the plug tissue) stained positively for proteoglycans throughout and appeared hyaline-like under polarized light. In segments 3 and 4, furthest from the autologous plug tissue, the cartilage was metachromatic for Safranin O staining and had more disorganized areas of collagen under polarized light, suggesting fibrocartilage ( Fig. 2B ). Four blinded reviewers were asked to grade both DeNovo NT and autologous tissue in the 4 segments using a modified OsScore index 3 for histological parameters (maximum score of 9 as mineralization could not be assessed because of tissue decalcification). The results of this grading are shown in Figures 2C and 2D . There was an indication that the DeNovo NT tissue graft in segments 1 and 2, close to the autologous cartilage plugs, better maintained its hyaline nature.
(
Discussion
The purpose of this study was to evaluate the medium-term histologic outcome of DeNovo NT graft, used for the repair of cartilage in the knee. Despite showing good healing at 7 months postsurgery by MRI, and the patient experiencing reduced pain at 7 and 13 months, the excised cartilage tissue was heterogeneous, with some regions of hyaline-like cartilage and some regions of fibrocartilage. Further surgical intervention was associated with the persistence of a residual chondral lesion opposite the area of the previous meniscectomy, which was resurfaced with the autologous plugs. This suggests that an intact meniscus may be an important factor in the success of this procedure. A direct comparison of the DeNovo NT tissue to the autologous plug tissue was not entirely appropriate as the plugs were only implanted for 15 months whereas the DeNovo NT was implanted for more than 2 years. It does, however, appear that the later mosaicplasty may have helped maintain hyaline-like cartilage of the DeNovo NT tissue in its vicinity. Limitations of this study include a paucity of excised DeNovo NT tissue samples. Collection of data from a larger study population with longer follow-up times would provide more information on long-term efficacy.
DeNovo NT tissue has been commercially available since 2007 and, as of March 2011, has been implanted in more than 2,200 patients in the United States. 6 Preliminary reports have shown promise. In a cohort of 4 patients reporting 24 months after DeNovo NT implantation, MRIs showed lesion infilling and pain indices were improved 7 and in a case report of a De Novo NT Cartilage implantation in the talus, 8 the patient was no longer experiencing ankle pain at 2 years postoperatively. In this case, the DeNovo NT tissue provided a stable, if heterogeneous, tissue on the lateral side of the osteochondral lesion. The differences between MRI and follow-up histology highlight the difficulties in assessment of cartilage repair surgery. This juvenile tissue graft is still offered to patients who meet the indications for cartilage repair and the multicenter DeNovo NT Longitudinal Data Collection (LDC) Knee Study ending in 2018 should provide a wealth of information on treatment outcomes.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Labib is a principal investigator on a DeNovo NT outcome study. All analysis for this study was done by nonconflicted authors.
Ethical Approval
This study was approved by the Emory University Institutional Review Board.