
Abstract
Objective:
Platelet-rich plasma (PRP) has the capacity to improve the bone-healing process. The aim of this pilot study was to investigate the occurrence of bone healing and the time taken to achieve this in patients submitted to medial opening wedge high tibial osteotomy (MOWHTO), comparing platelet-rich plasma with bone marrow aspirate to autologous iliac graft.
Design:
Twenty-five patients who underwent tibial osteotomy were randomly divided into 2 groups: a control group, which received autologous iliac grafts (14 patients), and a study group, which received a compound of PRP and bone marrow aspirate (11 patients).
Results:
The bone-healing rates achieved were 100% in the control group and 91% in the study group. There was no difference in the time taken to achieve bone healing between the groups.
Conclusions:
The use of a combination of PRP and bone marrow aspirate, as a bone substitute, did not demonstrate any advantage over the use of an autologous iliac graft in MOWHTO.
Introduction
Autologous iliac graft is considered the gold standard among the graft materials used today and is also the most frequently used method. 1 However, patients who undergo surgical procedures to harvest iliac grafts frequently present significant donor-site morbidity. 2
Several studies have tried to obtain biologically compatible bone substitutes to avoid the complications associated with the harvesting procedure of autologous bone graft. 1 Grafting procedures using bone marrow aspirate 3 and platelet-rich plasma (PRP)4,5 have been studied, with promising results. Bone marrow aspirate is an important source of osteogenic cells,6,7 and PRP has the capacity to improve the bone-healing process through osteoinductive action.8,9
PRP has been shown to stimulate osteoblast proliferation in vitro and to enhance bone repair, presumably because of the high levels of autologous growth factors (platelet-derived growth factor, transforming growth factor–β [TGF-β], vascular endothelial growth factor) that do not induce immunological reactions.10,11
Despite the lack of clinical studies, the use of growth factors (PRP, bone morphogenic proteins, TGF-β, etc.) in several orthopedic procedures has increased in the past few years. Growth factors have been used alone or in combination to treat problems affecting bone, cartilage, ligaments, and tendons.12-14
The purpose of this article is to report on the initial results regarding bone healing with the use of a biological graft containing a combination of PRP and bone marrow aspirate, to be used in medial opening wedge high tibial osteotomy (MOWHTO), compared with autologous iliac bone graft (considered here as the gold standard among bone substitutes). It was hypothesized that in the evaluation of bone healing, this graft would be a satisfactory choice and would promote timely healing of the osteotomy site. This study therefore seeks to determine if PRP and bone marrow aspirate can be used as a bone substitute for autologous iliac bone graft in MOWHTO with comparable results in terms of the percentage of patients with bone healing and the time necessary to achieve this.
Methods
Sample and Randomization Process
This study was approved by the Ethics Committee for Research on Human Beings. All patients voluntarily agreed to participate and freely signed an informed consent form.
Patients with varus deformity of the knee that was unrelated to osteometabolic diseases and who underwent MOWHTO between August 2005 and July 2007 were included in the study, regardless of the cause (unicompartmental osteoarthritis, chronic ligament deficiencies, or lower-limb deformities). The indications for tibial valgus osteotomy established in the literature were used. 15 The patients required surgical correction, using wedges between 10 mm and 15 mm. Loss of follow-up was considered an exclusion factor.
The measurements of interest were 1) percentage of cases with consolidation 24 weeks after surgery and 2) time to achieve bone consolidation after the surgical procedure.
The patients were randomly distributed into 2 groups using random assignment with replacement. The control (iliac) group was composed of patients who underwent osteotomy with the use of an autologous iliac graft at the osteotomy site. The study group (PRP) was composed of patients who underwent osteotomy with the use of a bone substitute consisting of PRP and bone marrow aspirate. This bone substitute was called biological graft.
Surgical Technique
All surgical procedures in this study were performed by the same surgeon. The technique used to perform the osteotomy was as previously described 16 : an opening wedge osteotomy, similar to the planning and surgical technique described by Puddu. 17 A nonlocking, straight wedged plate was used (Arthrex). 17 The iliac graft obtained was cortical cancellous, of sufficient amount to fill the gap created by the osteotomy. The iliac crest was used as the donor area, and the surgical technique was standardized. 18
The platelet concentrate was obtained using an automatic cell separator (MCS Plus; Haemonetics, Braintree, MA). 19 This automatic cell separator collected about 400 ml of whole blood, which resulted in 70 ml of PRP after preparation, and sodium citrate was used as an anticoagulant. The PRP platelet concentration was measured in all patients. The platelets were collected 20 minutes before surgery, immediately before anesthesia. The bone marrow aspirate was obtained from the iliac crest by percutaneous puncture, using a standardized technique with a number 14 needle guide. Six punctures were made, obtaining about 12 ml of bone marrow. 20 Sodium citrate was added to this material as an anticoagulant, with a citrate:bone marrow ratio of 1:5.
The bone graft was formed by adding the bone marrow aspirate to the PRP. Autologous thrombin and 10% calcium chloride were added to this compound to form a gel. The surgeon then placed the biological graft in the surgical site (osteotomy gap).
Radiographic Evaluation
The method used to assess bone healing was plain radiographs, similar to what is suggested by Brinkman et al. 21 The patients were evaluated every 2 weeks, to assess signs of bone healing at the osteotomy site.22,23 The evaluations were carried out by 2 observers, who were blind to the type of graft that had been used in the patient, similar to the method described by Yacobucci and Cocking. 23
The imaging method used was standard radiography in anteroposterior and lateral views (65 kV, 20 mA, with a focus film distance of 100 cm and an equivalent effective dose of <0.01 mSv within ±2%). The indicators used to assess bone union were increasing density of the graft on serial examination and bone bridging across the wedge opening.
The time to achieve bone healing22,23 was determined from this examination. The criteria used to check the occurrence of bone healing were as follows: 1) in the anteroposterior view, the presence of bone filling at least 60% of the osteotomy in the lateral-medial direction, and in the lateral view, 2) consolidation of the anterior or 3) posterior cortex. For the osteotomy to be considered united, at least 2 of these criteria had to be met (
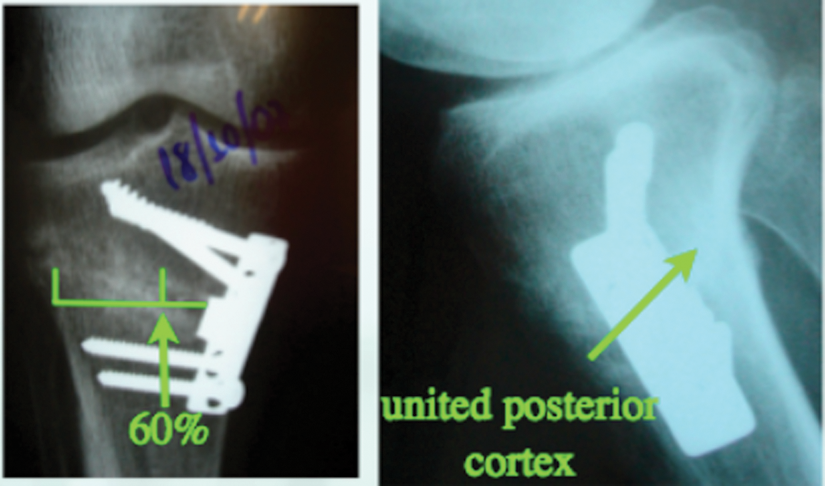
Radiographic criteria used to access bone healing.
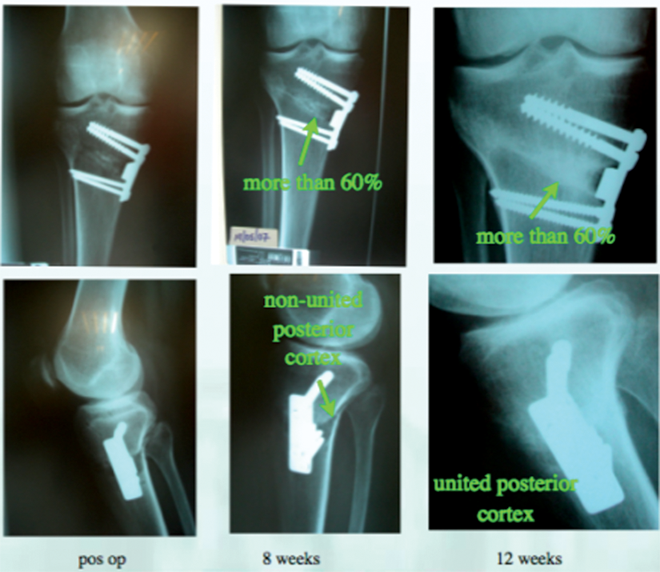
Example of union in an osteotomy performed in a 45-year-old patient with a 12.5-mm wedge, 12 weeks to bone healing.
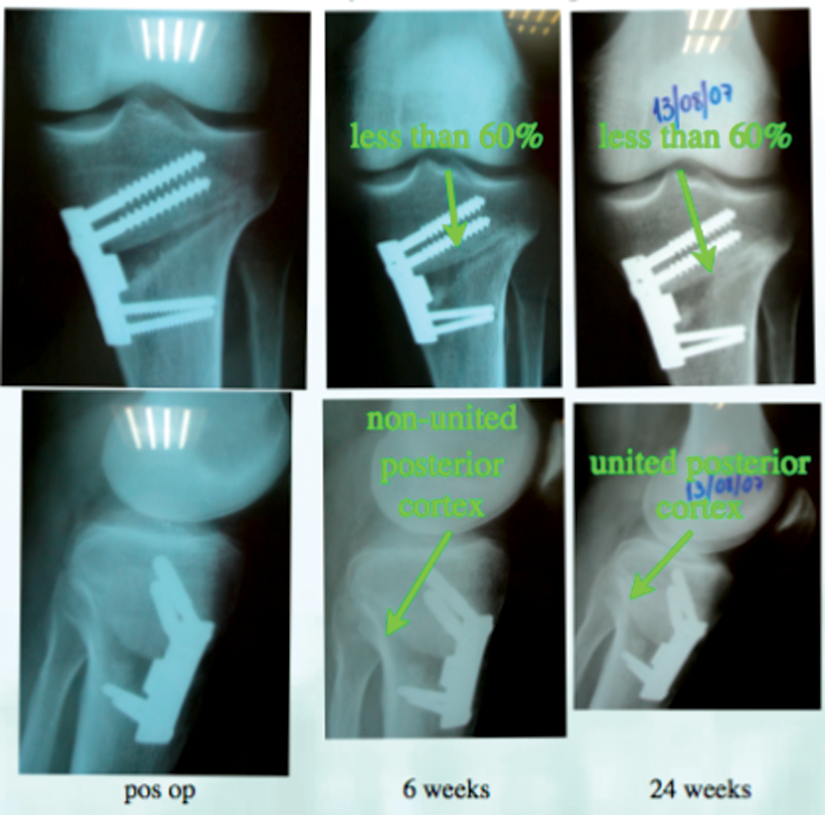
Example of nonunion in an osteotomy performed in a 37-year-old patient with a 12.5-mm wedge, 24 weeks until considered a nonunion.
In addition, to detect any signs of collapse at the osteotomy site, the angle of correction was measured right after the surgery and at the last follow-up, using a manual goniometer.
Statistical Analysis and Power
The occurrence of union was compared between the groups, by means of the Fisher exact test. The target difference was 10% between the groups.
The consolidation time (survival time) was defined as the period, in weeks, between the date of surgery and the date of consolidation, and it was evaluated by the construction of Kaplan-Meier curves. The curves for the 2 groups were compared, using the log-rank and Breslow statistical tests.
Results
During the study period, surgery was performed in 25 patients; 14 were allocated to the control group, and 11 to the study group. There was no loss of follow-up. The results of this series are described below.
Regarding the angle of correction, the mean angle of correction (initial measure) was 10.8° in the control group and 11.1° in the study group. The mean angle of correction (final measure) was 10.6° in the control group and 11.0° in the study group. Evaluating the patients separately, there was also no loss of correction.
The most frequent indication for surgery, in both groups, was chronic injury of the anterior cruciate ligament. The diagnoses were evaluated once and grouped into 3 categories (
Distribution of the Patients in the Autologous Iliac Graft and Platelet-Rich Plasma Groups According to Sex, Tobacco Use, and Diagnosis
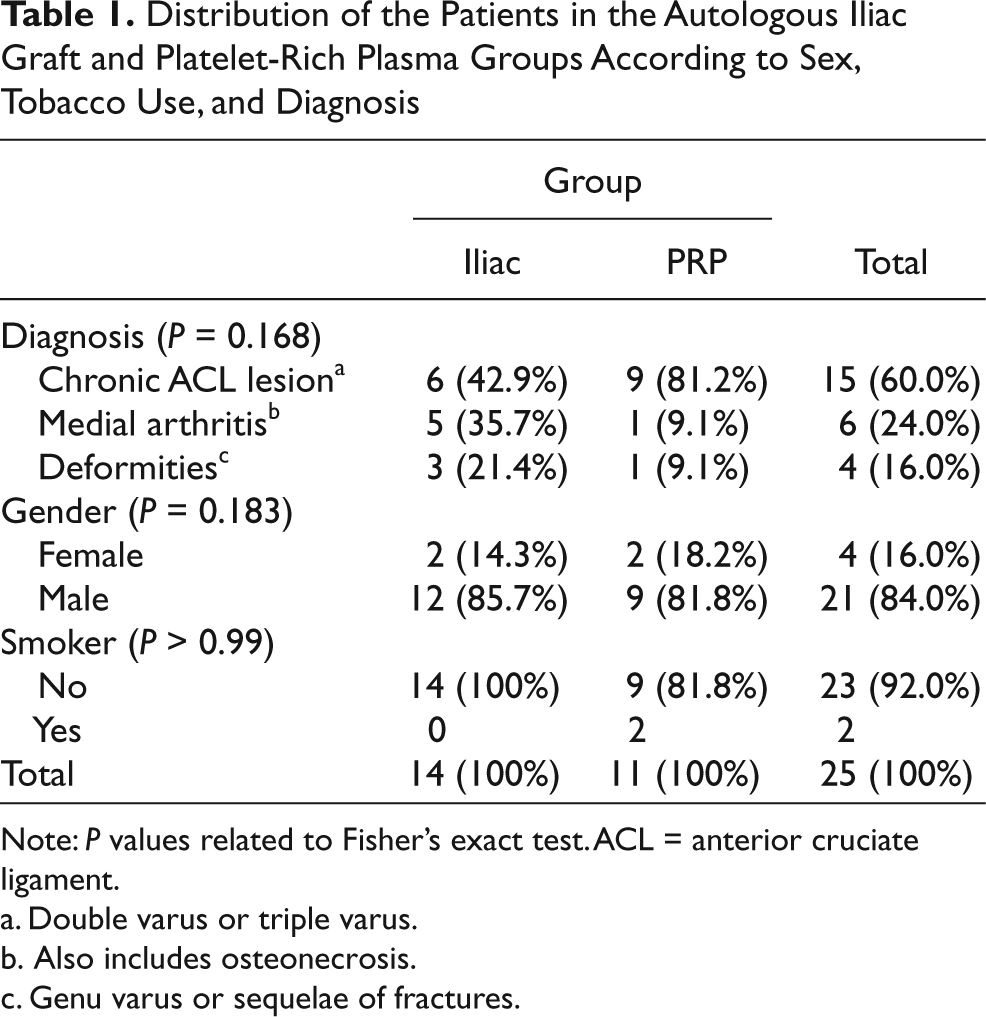
Note: P values related to Fisher’s exact test. ACL = anterior cruciate ligament.
Double varus or triple varus.
Also includes osteonecrosis.
Genu varus or sequelae of fractures.
The mean age of the patients was 42.4 years (±8.5). For the iliac group, the mean age was 45.9 years (±8.1), and for the PRP group, 37.8 years (±6.9). The mean age was significantly higher in the iliac group, with P = 0.014 (Student’s t-test). In view of the difference in mean age found between the 2 groups, a dispersion graph was constructed to correlate the consolidation time with the patients’ ages, as shown in
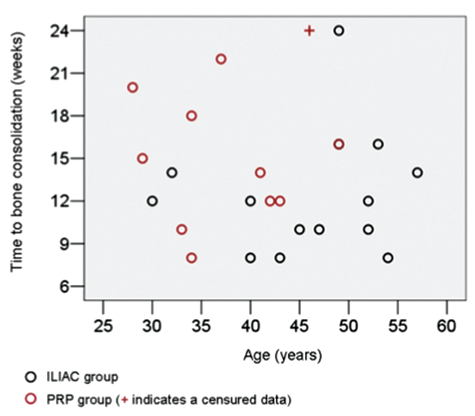
Dispersion graph showing time for bone healing versus patient age.
Consolidation
1. Can PRP be used as a substitute for autologous iliac bone graft, with comparable results regarding the percentage of patients who achieve bone healing?
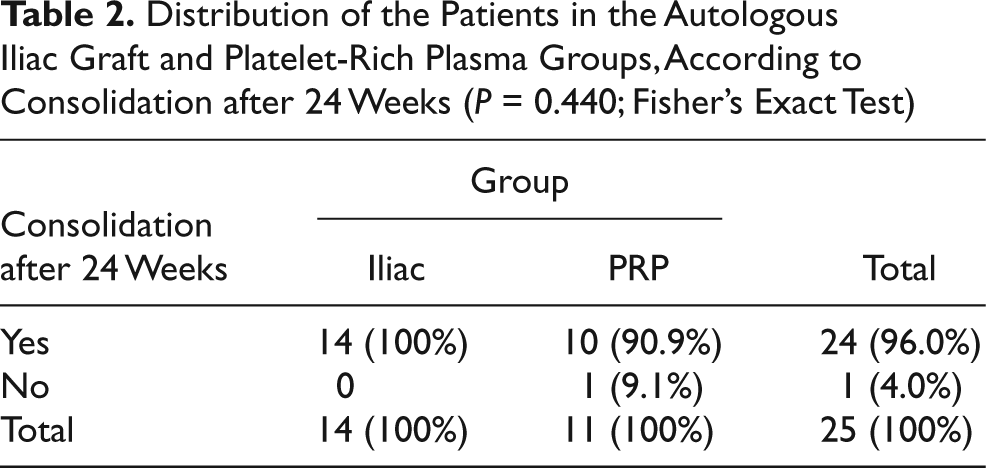
The percentages of consolidation, 24 weeks after surgery, were the same for both groups in this initial series of 25 patients: The consolidation rate reached 100% in the iliac group and 91% in the PRP group, with P = 0.440.
Distribution of the Patients in the Autologous Iliac Graft and Platelet-Rich Plasma Groups, According to Consolidation after 24 Weeks (P = 0.440; Fisher’s Exact Test)
2. Can PRP be used as a substitute for autologous iliac bone graft, with comparable results regarding the time necessary to achieve bone healing?
The consolidation time can be analyzed in
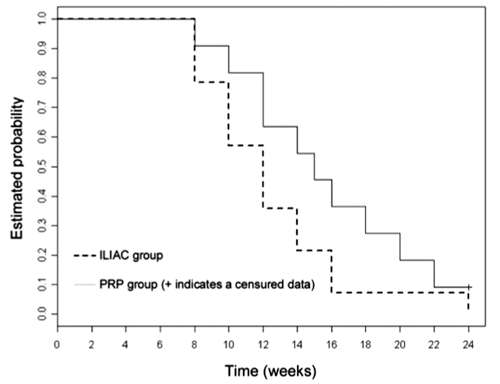
Kaplan-Meier estimates for the autologous iliac and platelet-rich plasma (PRP) groups. The + represents the occurrence of a censure.
Kaplan-Meier Estimates and 95% Confidence Intervals for the Time Taken for Consolidation (Weeks) in Autologous Iliac Graft and Platelet-Rich Plasma Groups
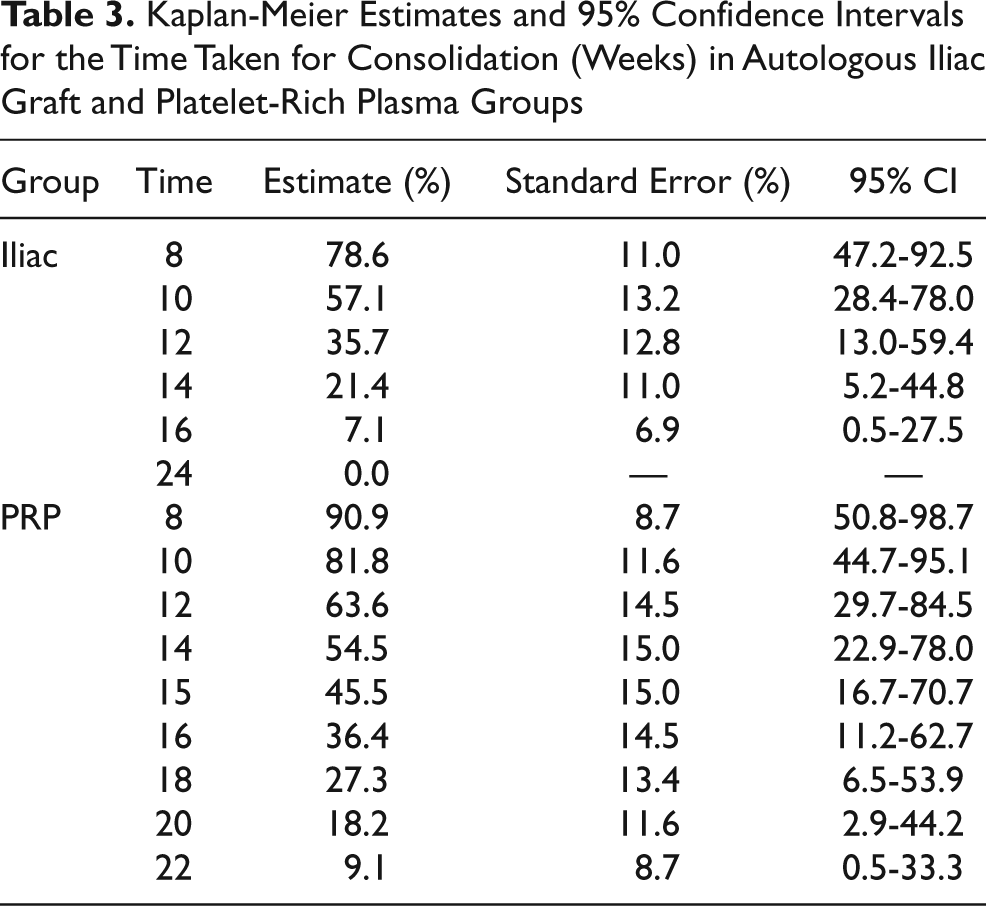
The median consolidation time (i.e., the time taken for about 50% of the patients to present consolidation) can also be observed in
Descriptive Measurements for the Time Taken to Achieve Consolidation (Weeks) for the Autologous Iliac Graft vs. PRP Groups
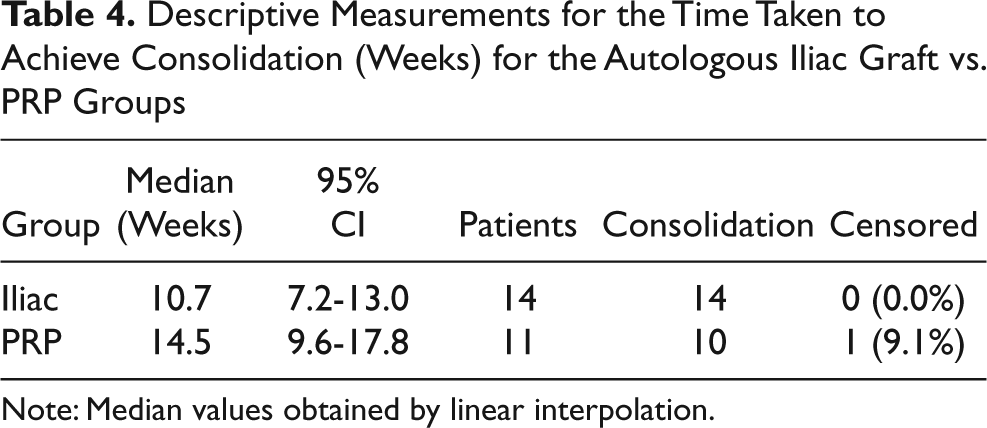
Note: Median values obtained by linear interpolation.
No strong evidence was found of any difference in the survival curves, comparing the iliac and the PRP groups; that is, there was no statistical difference in consolidation time between the groups, either by the log-rank test (P = 0.129) or by the Breslow test (P = 0.100).
Discussion
Orthopedic surgeons need to develop techniques and materials that will enable bone substitution. 1 It was hypothesized that the use of a combination of PRP and bone marrow aspirate as a bone substitute would be effective in obtaining bone healing in MOWHTO, within an adequate time, and without the morbidity associated with autologous iliac harvesting. 18
There are no reports in the literature on the clinical use of PRP together with bone marrow aspirate as a bone substitute comparing its results with that of autologous iliac graft in MOWHTO.
The need of bone graft or bone substitute when performing MOWHTO is still debated. No prospective randomized trials have yet been published that compare the various filling materials with no filling at all. 21
Bone marrow contains hematopoietic and nonhematopoietic stromal cells, from which osteoclasts and osteoblasts, respectively, originate. The inducible osteogenic precursor cells are capable of forming osteogenic tissue in the presence of inducers or stimulatory factors such as the ones released from platelet-derived growth factors. 7
Like other authors, 24 we chose not to evaluate the clinical outcome of MOWHTO because this is already well documented in the literature16,25 and should not be affected by the choice of graft, provided the osteotomy unites and the wedge construct does not collapse. No signs of collapse were observed at the osteotomies because the initial and final measurements of the angle of correction were similar in all patients.
As shown by other studies in this field,22-27 there are some limitations in performing a study on MOWHTO, regarding the number of patients needed to achieve statistical power for the analysis of the results. The sample size needed to achieve statistical difference would be extremely high, and the frequency of the conditions that indicate the procedure are relatively low.21,23,28 Therefore, a multicenter study would be needed to reach the ideal sample size. A retrospective power analysis and an analysis of variance test were performed, and our study was found to be underpowered.22-25
There is a lack of clinical studies, especially prospective and randomized studies, comparing the use of bone substitutes with the technique that is still considered the standard for grafting (i.e., autologous iliac bone graft).1,2,22 The study presents this design with an evaluation and comparison of the performance of 2 types of grafts (iliac vs. biological) regarding bone healing in a standardized procedure: MOWHTO.
PRP has significant osteoinductive action, as demonstrated by various experimental studies.9,19,29 It has widespread clinical application in the field of oral and maxillofacial surgery and is used as a bone promotion agent in a variety of situations. 10 Its clinical use in orthopedics has been increasing, despite the absence of prospective and randomized studies evaluating the results of its use.30,31
The obtainment method of PRP is of major importance because different methods have different capacity to concentrate platelets32,33 and there is a direct correlation between the number of platelets in the PRP and the growth factor concentration. Marx et al.8,34 and Kawasumi et al. 35 suggested that the ideal concentration of platelets to be used as an enhancement factor in procedures involving bone and soft tissue should be about 1,000,000 platelets/µl. Most commercially available devices are merely modifications of laboratory centrifuges and do not have the capacity to adequately produce PRP. In the present study, an automatic cell separator was used (Haemonetics MCS Plus),19,36 and it produces PRP with an ideal concentration of platelets.
Mesenchymal stem cells are present in bone marrow aspirates, and when associated with substances with osteoinductive or osteoconductive properties, they have already proven to be an alternative to autologous grafts.7,37 In a study on canines, Yamada et al. 37 demonstrated that PRP has osteogenic capacity when used in association with mesenchymal stem cells. This osteogenic capacity was found in our study, as seen with the occurrence of consolidation of the osteotomy site, but it was not significantly different between the groups (P = 0.440).
In their work, Dallari et al. 22 demonstrated that PRP in association with mesenchymal stem cells derived from bone marrow aspirate is capable of producing consolidation at the osteotomy site in MOWHTO. However, they did not include a control group composed of patients who had received only autologous bone grafts.
Despite the excellent clinical results obtained from osteotomy with the addition of a medial wedge,21,25 one of the main drawbacks of this procedure is the length of time during which the patient must remain in a non- or partial-weight-bearing regimen until local bone healing is achieved. Any bone substitute that is to be used in this type of procedure must be compared with autologous graft, in terms of the occurrence of consolidation as well as the time required to achieve this, as in the present study. The biological graft consisting of PRP and bone marrow did not demonstrate any advantage over autologous iliac grafts (

Radiographs after bone healing of patients with anterior cruciate ligament chronic injuries submitted to tibial opening wedge osteotomy: the 1st patient (
Regarding bone healing time, the PRP group required a longer period in this study. This may be considered a great disadvantage, in view of the longer time that the patient must remain with load-bearing restrictions. However, the differences were not statistically significant (P > 0.1). But the low power of the test presented here points out that the results should be seen only as indicative.
The use of a combination of PRP and bone marrow aspirate, as a bone substitute, did not demonstrate any advantage over the use of an autologous iliac graft in MOWHTO.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article. Ethical review board statement: This study was approved by the Ethics Committee of Hospital das Clínicas, School of Medicine of the University of São Paulo.