
Abstract
Objective:
To determine if lubricin was present in the surface layer of repair cartilage formed after autologous chondrocyte implantation (ACI).
Design:
Forty-three biopsies of repair tissue were taken from patients who had been treated with ACI 8 to 68 months previously (mean of 18.0 ± 14.4 months); 30 had flaps of periosteum and 13 of Chondro-Gide®. Cryopreserved sections were stained with hematoxylin and eosin, toluidine blue, and immunostained for lubricin and type II collagen. The quality of repair tissue was scored via OsScore, and clinical improvement in patients was assessed via change in Lysholm score. Normal/control cartilage was studied for comparison (n = 5).
Results:
Patients’ Lysholm scores improved from 48.1 ± 17 preoperatively to 69.5 ± 21.5 posttreatment. The thickness of repair tissue was 2.9 ± 1.7 mm compared with 2.3 ± 0.6 mm for control cartilage, with an OsScore of 6.7 ± 1.6 (8.9 ± 1.2 for controls). Ninety-eight percent of biopsies had staining for lubricin, with 84% having some in the surface layer (60% of periosteal treated and 100% of Chondro-Gide treated). The improvement in Lysholm score was not significantly different in patients with lubricin present at the surface compared with those without.
Conclusion:
Lubricin was present in almost all samples of repair tissue formed post ACI, often in the surface layer, resembling the distribution that is seen in normal cartilage. The presence of lubricin in the upper layer is likely to have implications for the functioning of the tissue because, via its mucin-like repeats, it appears capable of reducing the friction that could arise in articulating joints.
Introduction
Autologous chondrocyte implantation (ACI) has now been used worldwide for more than 2 decades as a means of treating chondral defects, particularly in the knee.1,2 There has been extensive interest as to the quality and morphology of the repair tissue that forms, whether it is hyaline cartilage, fibrocartilage, or how much type II collagen it contains.3-5 The premise is that the more it resembles hyaline cartilage and the more type II collagen within it, the better the quality of the repair. Other properties of the repair tissue, however, may be as important and indicative of the long-term successful functioning of the replacement tissue that forms. For example, normal articular cartilage contains a proteoglycan that is alternatively called superficial zone protein or lubricin 6 (also synonymous with PRG4, megakaryocyte-stimulating factor precursor, or CAP [or CACP] protein). These all appear to have a similar primary structure, all being encoded by the gene PRG4, but they may have different posttranslational modifications. 7 Lubricin, which was first isolated from synovial fluid, 8 is attributed with many functions relevant to its location in the superficial zone of articular cartilage, including antiproliferative effects and inhibiting protein or cell adhesion. 9 Probably one of the most important properties, however, is that it functions as an efficient boundary lubricant at low striding speeds typically seen in joints.10-12
Defects in the structure or production of lubricin are suspected to be associated with abnormal joint functioning. For example, the genetic disorder camptodactyl-arthropathy pericarditis syndrome appears to be mapped to the same locus as that encoding for lubricin. 7 Patients with this disorder have a large joint arthropathy, flexion contracture of interphalangeal joints, and synoviocyte hyperplasia, suggested to result from ineffective joint lubrication. Prg-4 knockout mice are born with apparently normal joints, but with aging, they develop abnormalities in the surface of the cartilage (abnormal protein deposition) and subsequent cartilage deterioration. 9 Animal models of osteoarthritis (OA) have reduced levels of lubricin, 13 particularly in the early stage of the disorder. 14 In vitro studies of lubricin production show it is down-regulated by several cytokines believed to be involved in OA, for example, IL1-β and TNF-α 15 ; in addition, lubricin appears to be chondroprotective and to reduce structural damage when applied in an animal model of OA. 16 To date, little is known of lubricin’s involvement in cartilage repair in humans.
We have examined the presence of lubricin in biopsies of repair tissue from patients who had chondral or osteochondral defects treated with ACI. In some patients, this was carried out in the traditional/original manner as described by Brittberg et al., 2 whereby autologous chondrocytes had been extracted from healthy tissue harvested from a less weight-bearing region of the knee, proliferated in vitro, and injected beneath a flap of periosteum stitched over the damaged but debrided area. In other patients, a collagen membrane, Chondro-Gide® (Geistlich Pharma AG, Switzerland), was used in place of the periosteum. This immunohistochemical study demonstrated that lubricin is present in the repair tissue after approximately 18 months of treatment in most patients using autologous periosteum and in all using a sheet of porcine collagen as the flap.
Materials and Methods
Patients and Tissue Biopsies
Forty-three full-depth biopsies were obtained from 41 patients aged 19 to 60 years at treatment (mean age, 34.8 ± 9.7 years) who had been treated with ACI for cartilage defects; 29 were treated using a periosteal flap, and 12 with a Chondro-Gide flap. As part of their follow-up assessment, patients in our institute routinely undergo an arthroscopic examination and biopsy of the graft at approximately 1 year (ranging between 8 and 68 months, with a mean of 18.0 ± 14.4 months), as approved by the local Ethical Committee. Biopsies of 1.8 mm in diameter were taken (using a juvenile bone marrow biopsy needle) from the center of the treated region and included both the repair cartilage tissue and, where possible, the subchondral bone, as detailed previously. 17 Twenty-seven biopsies were taken from the right knee and 16 from the left. The most common site of treatment was the medial femoral condyle (n = 26), with 11 biopsies taken from the lateral femoral condyle, 5 from the trochlea, and 1 from the patella. The average size of the defect area treated was 5.1 ± 3.9 cm2 (7.2 ± 5.4 cm2 for Chondro-Gide or 4.2 ± 2.9 cm2 for periosteum-treated regions). Biopsies were snap frozen and stored in liquid nitrogen until examined.
Patients were also assessed at regular intervals for clinical outcome using the Lysholm score, ranging from 0 (poor outcome) to 100 (best). 18 This was recorded preoperatively, just prior to the arthroscopic investigation, and annually thereafter. Within this score is a pain component (0 = most severe pain, 25 = no pain), which was also recorded.
For comparison to the repair tissue, “normal” control articular cartilage was examined from 5 individuals: 4 from medial femoral condyles obtained at autopsy of individuals aged 22, 30, 40, and 50 years (obtained from the UK Human Tissue Bank) and 1 lateral femoral condyle of an individual aged 10 years undergoing corrective surgery.
Histologic Assessment
Cryosections were stained with hematoxylin and eosin and toluidine blue, and cartilage morphology was determined microscopically using normal and polarized light. Quality of repair tissue was assessed using a semiquantitative score (OsScore), in which the parameters smoothness of surface, morphology, metachromasia, vascularization, mineralization, and basal integration were assessed and scored as described previously. 17 This uses a scale of 0 (worst) to 10 (best).
Immunostaining
For lubricin immunohistochemistry, 7-µm-thick cryostat sections were collected onto poly–L-lysine–coated slides and fixed with 4% paraformaldehyde. Endogenous peroxidase activity was blocked with 0.3% hydrogen peroxide in methanol and nonspecific staining blocked with normal goat serum. Sections were incubated overnight at 4°C with 10 µg/mL G35 polyclonal antibody raised in rabbits against the human lubricin peptide sequence GEGYSRDAT, from the protein region encoded by exon 2.10 This antibody detects full-length lubricin on Western blotting (data not shown). Labeling was visualized using biotinylated anti-rabbit antibody and an avidin-biotin complex (Vectastain Elite ABC kit; Vector Laboratories, Peterborough, UK) and diaminobenzadine as chromogen. Sections were counterstained with Mayer’s hematoxylin, dehydrated, cleared, and mounted with Pertex. Adjacent sections were used as controls by omitting the primary antibody and using a rabbit IgG in its place (Vector Laboratories).
Immunostaining for type II collagen was also carried out on adjacent cryosections fixed in 10% formalin and enzymatically digested with ovine testicular hyaluronidase (4800 U/mL) for 2 hours at room temperature. They were then incubated with a monoclonal antibody to type II collagen (CIICI; Developmental Studies Hybridoma Bank, University of Iowa) for 30 minutes at room temperature. Visualization was carried out as for lubricin but using an antimouse secondary antibody, with antimouse IgG used as a normal control.
Statistics
Nonparametric statistical analyses were performed, for example, the Mann-Whitney U test, to compare outcomes in patient cohorts with or without lubricin in the surface layer analyzing parameters such as the pain score, Lysholm score, OsScore, and thickness of repair cartilage. Similarly, comparisons were made between the 2 patient groups treated with either periosteal or Chondro-Gide patch. Statistics were carried out with a software program, Analyse-it® (Analyse-it Software Ltd, Leeds, UK). Means are quoted ±standard deviation, and a P value of <0.05 was considered to indicate significance.
Results
The average age of both treatment groups was similar, and the time post-ACI was 19.3 months for the periosteum-treated group and 14.9 months for the Chondro-Gide–treated group ( Table 1 ). Patients treated with periosteum had an average preoperative Lysholm score of 48.8 ± 17 (n = 29), which had improved to 70.3 ± 21 at 1 year. The average preoperative Lysholm score for the patients treated with Chondro-Gide was 39.1 ± 17.9 (10), which increased to 60.3 ± 21.1 at 1 year after treatment; there was no significant difference in clinical improvement between those treated with periosteum or Chondro-Gide (P = 0.17). After the 1st year posttreatment, there was little increase in Lysholm score with time for all patients ( Fig. 1a ). The pain score followed a similar trend, with little difference between patients treated with Chondro-Gide or periosteal flaps ( Fig. 1b ).
Details of Patients Entered into the Study a
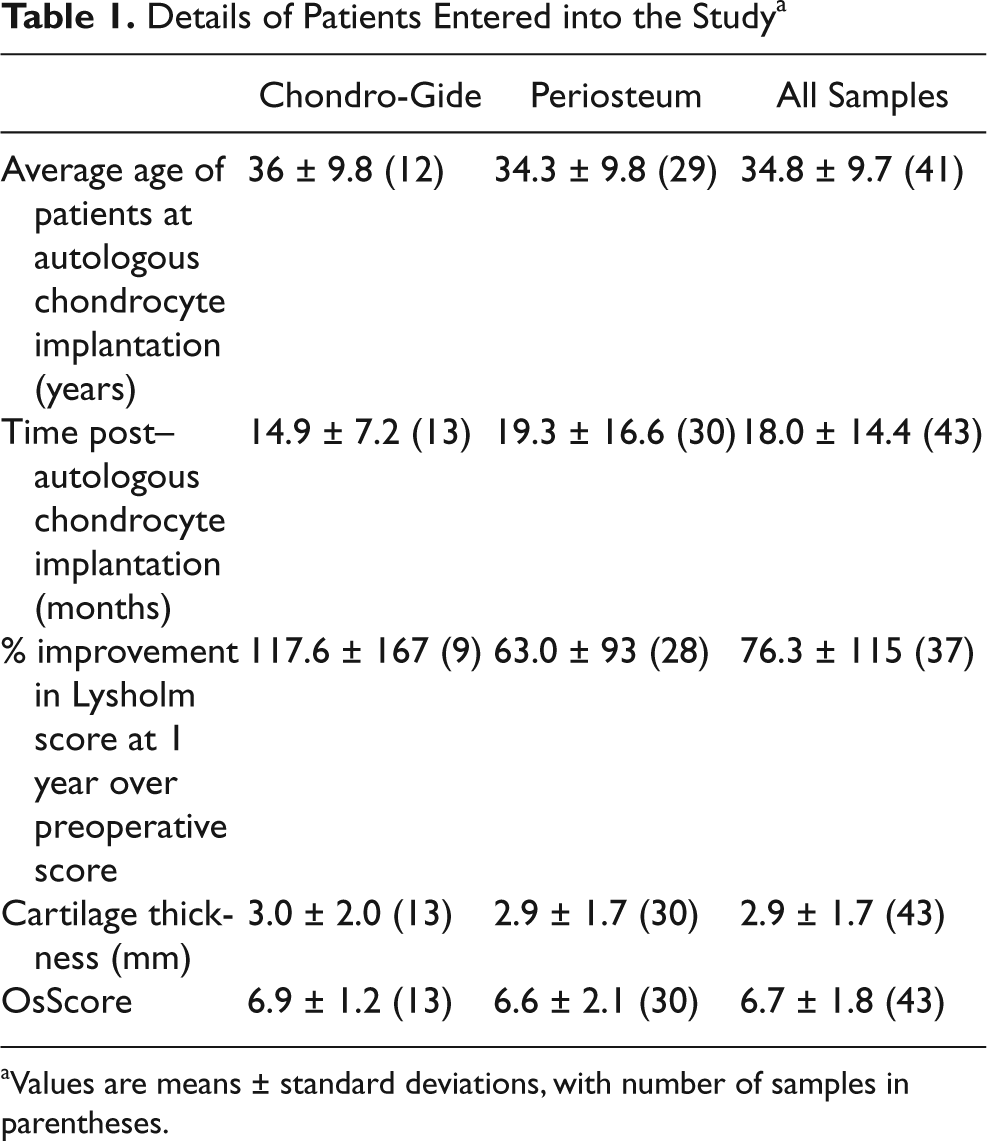
Values are means ± standard deviations, with number of samples in parentheses.
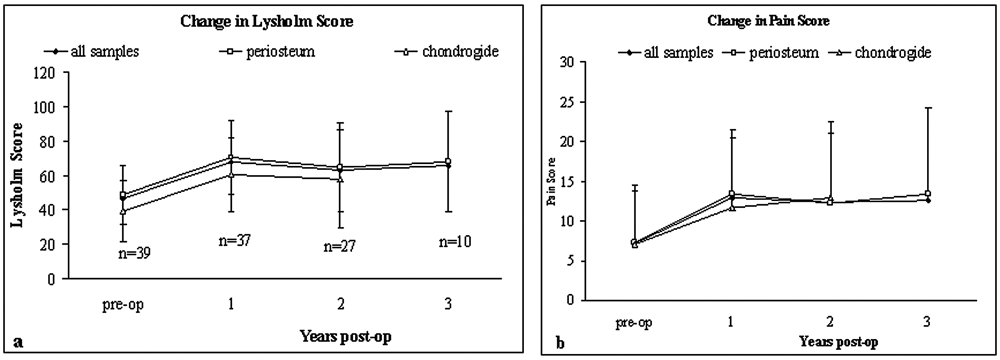
Change in (
The morphology of the repair tissue in the periosteum group was predominantly hyaline cartilage in 5 samples; 2 were a mixture of hyaline and fibrocartilage, 20 were mainly fibrocartilage, and 3 were fibrous tissue. In the Chondro-Gide–treated group, only 1 biopsy was predominantly hyaline cartilage, 1 was a mixture of hyaline and fibrocartilage, and 11 were mostly fibrocartilage. There was little difference between the groups in the thickness of repair tissue formed (2.9 mm average) or the OsScore (6.7; Table 1 ). Control samples were all classed as hyaline cartilage with an average thickness of 2.7 ± 1.1 mm and an OsScore of 8.5 ± 2.7.
Immunostaining for lubricin was present in all of the control samples of normal cartilage in the superficial zone; in the 22-year-old, this occurred only in the cells, but for the 10-, 30-, 40-, and 50-year-olds, it was in both cells and some matrix (
Fig. 2e
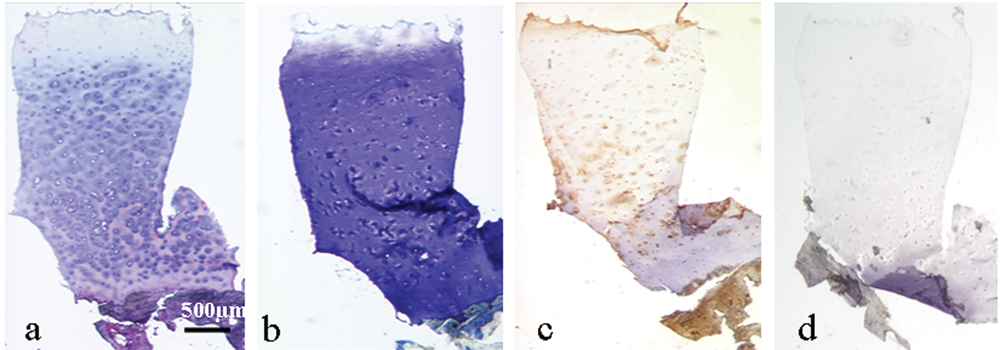
Full-depth sections of repair tissue from a 44-year-old man treated with autologous chondrocyte implantation and Chondro-Gide 15 months previously. Sections stained with (
In biopsies of repair tissue, there was immunostaining for lubricin in a very thin strip of the superficial zone in 84% of biopsy samples where the articulating surface was completely intact (33/38; Fig. 3 ); unfortunately, in 5 samples the surface was damaged or absent (probably during the process of obtaining the biopsy), so it was not possible to assess the location in these. Staining occurred either in the uppermost cells, the matrix, or both ( Fig. 2 ). In the group treated with ACI and periosteum, the superficial zone matrix was positively stained in 60% (15/25) of the samples, and 64% (16/25) had positive staining in some cells. In contrast, all the biopsies from patients treated with Chondro-Gide (13/13) showed positive staining of the cells in the superficial zone, and 83% of these samples had positive staining within the matrix here.
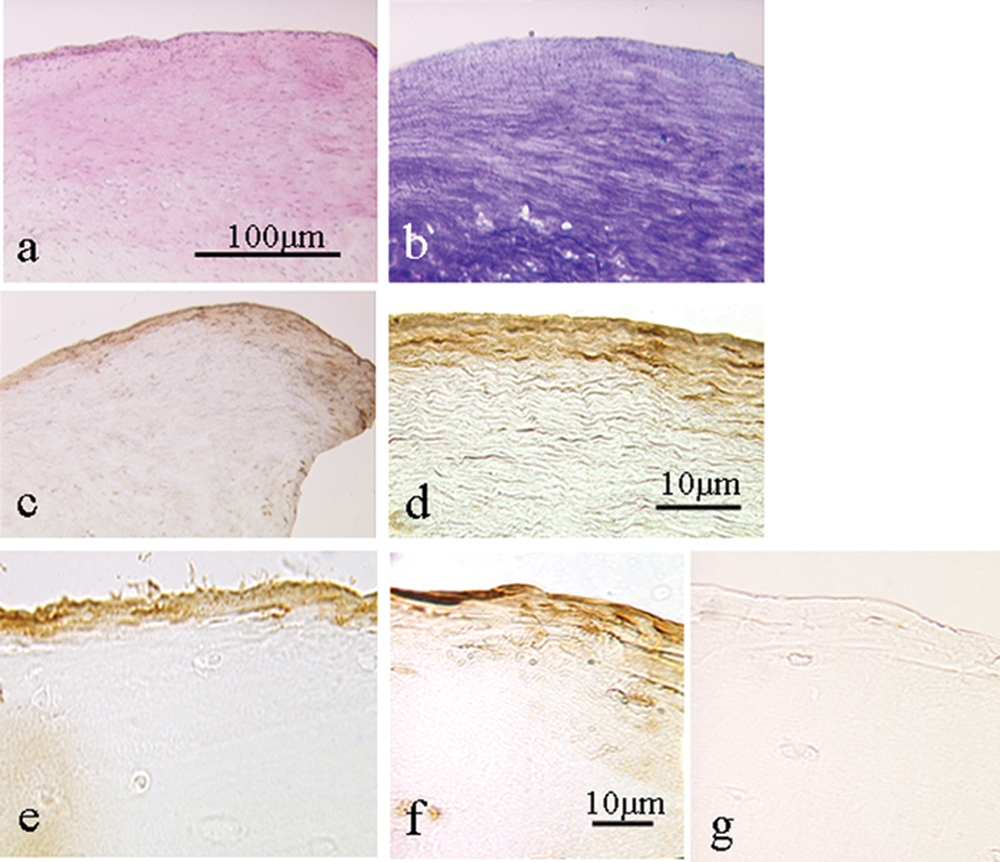
Repair tissue formed 13 months following autologous chondrocyte implantation in (
In the tissue, further from the surface, cells that stained positively for lubricin were seen in 40 samples (93%) in both the mid and the deep zones, with the strongest staining occurring in the deep zone ( Fig. 4 ). Clusters of cells were seen in 11 samples (26%), and some of the cells within the clusters were immunopositive. There was only slight (n = 8) or no (n = 35) immunopositivity seen in the extracellular matrix of the mid and deep zone of the samples. Only 1 sample from a patient (periosteal patch) was completely negative for lubricin; this biopsy was fibrocartilage throughout, with the upper surface containing very thin fibroblast-like and distorted cells.
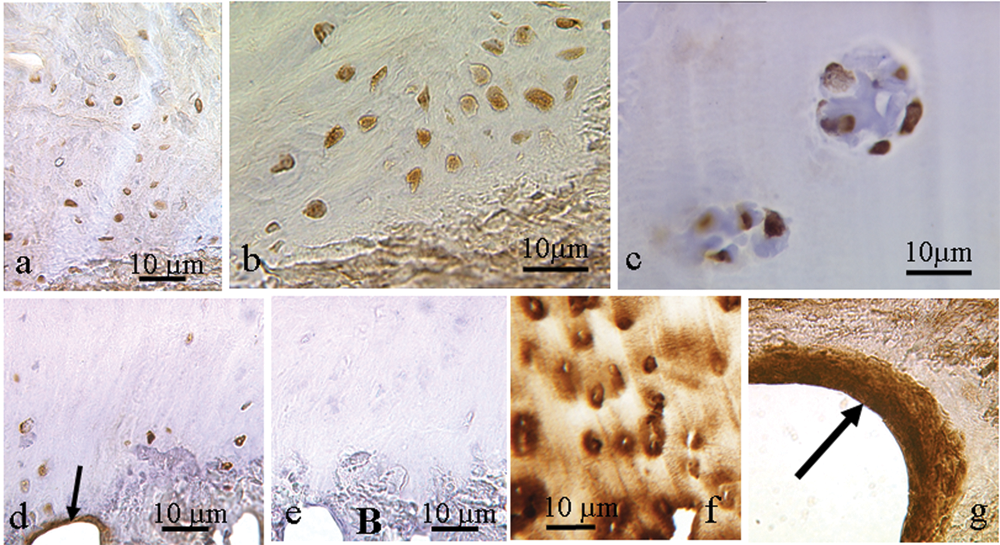
Repair tissue showing immunostaining for lubricin in cells in the deeper zones. This occurred in single cells ((
Bone was present in 40 of the biopsies (but partially detached from the cartilage in 1 sample). Positive immunostaining for lubricin was seen in either bone, osteoid, or both in all of the intact biopsies.
There was immunostaining for type II collagen in all of the samples investigated but to very varying degrees, ranging from throughout the whole depth of repair tissue to only a small region being positive. Where staining was partial, it was always the region closest to the bone that was positive, with the region toward the articulating surface being weaker or negatively stained. The distribution of staining for lubricin and type II collagen in the upper layer appeared to be completely unrelated, whereas the cellular staining for lubricin that was present in the deeper zones did occur with stronger matrix staining for type II collagen ( Fig. 4f ). There were, however, no obvious trends with the presence of or staining pattern for lubricin and the OsScore, tissue morphology, or clinical parameters investigated and no significant difference for any parameters between patients who had lubricin present in the surface layer and those who did not.
Discussion
The repair tissue that formed post-ACI in this study was of a similar thickness to that of the normal control articular cartilage, even though it was mostly fibrocartilaginous rather than of hyaline cartilage morphology. In most samples, a thin layer of lubricin was demonstrated to occur in the superficial region at the articulating surface. The pattern of immunostaining was a little more widespread throughout the matrix at the surface than in the older control samples examined here and in those illustrated in some other studies (although this was in bovine cartilage). 19 There was an average of a 20-point increase in clinical benefit in both groups of patients (regardless of the type of flap used), which generally occurred within the 1st year and was sustained thereafter, as has been reported in other studies. 20
The location of lubricin at the articulating surface could arise either via lubricin within the synovial fluid binding to the upper layers (as has been shown to occur in vitro 10 ) or via production by the surface cells, particularly in response to shear stresses on the tissue and cells. Grad et al. 21 found that increasing surface motion via reciprocating sliding on tissue-engineered cartilage constructs increased the expression for and production of lubricin. The loads and strains that arose in this model were not characterized, but it is thought that fluid flow, cell deformation, or shear would occur. Lubricin production increased when shear was applied to chondrocytes cultured in alginate. 22 Lubricin has been reported on the surface of other connective tissues and at possible sites of high shear stresses, for example, in tendons,23,25 meniscus, 26 and between annular lamellae within the intervertebral disc. 27 The most intense staining for lubricin was at the surface of tendons subjected to the highest levels of compressive, shear, tensile, and frictional forces. 23
One of the most commonly suggested functions for lubricin occurring at the articular surface is that it is likely to reduce friction, possibly by virtue of its large mucin-like domain characterized by the repeat motif KEPAPTTT/P. 9 Certainly, the coefficient of friction for articular cartilage increased from 0.06 N to 0.09 N following trypsin digestion, with the increase suggested as being due to the digestion and loss of the lubricin. 28 It is also thought that lubricin might protect the cartilage surface from cell adhesion 19 and possible synovial overgrowth. 9 Down-regulation of lubricin in the superficial zone of cartilage occurs as an early event in a sheep model of OA, 14 which could reduce the chondroprotection lubricin normally offers. In the correct location, lubricin thus produces the desirable effect of preventing fusion of apposing surfaces in the articular joint. It might, however, also inhibit the lateral integration of fully formed cartilage, either in vitro29,30 or perhaps in vivo in the surgical treatment of mosaicplasty.
The significance of lubricin staining in the cells within the lower regions of the cartilage is unknown, but because the lubricin molecule has several other multifunctional motifs (e.g., somatomedin B and hemopexin-like domains), it can be involved in many distinctive biological processes other than just reducing friction. Although there is undoubtedly some lubricin in the deeper regions of the tissue, the degree of immunostaining within the matrix is less than in the surface layer; this is similar to the in vitro production of lubricin reported to be much less by mid and deep cells compared with those from the surface. 31 Interestingly, lubricin has recently been reported in the human intervertebral disc, with the greatest extent of immunostaining being seen in the central nucleus pulposus. 32 We are also unaware of the significance of results from this study reporting lubricin immunostaining within the osteoid of bone, although lubricin previously has been reported to occur in the subchondral bone of human joints, 33 particularly within cartilaginous deposits.
This study is the 1st report to our knowledge of the presence of lubricin in repair tissue formed after ACI treatment. Although it occurred in patients treated with either periosteal or Chondro-Gide flaps, it was more consistently present in the surface zone of Chondro-Gide–treated patients. This is despite these patients having larger defect areas than those treated with periosteum (and biopsies being taken on average slightly earlier posttreatment). We have not studied the degree and type of posttranslational modification of the lubricin in terms of glycosylation in the repair tissue. Variations in these could have important implications for function because they are known to influence and organize the location of water to support loading and shear stress. 34 Nonetheless, this study does demonstrate that repair tissue that forms after ACI treatment resembles normal articular cartilage in at least some of its properties, such as the occurrence of lubricin in the surface layer.
Footnotes
Acknowledgements
We are very grateful to Helena Evans for technical assistance in carrying out the immunohistochemistry and Aled Jones for provision of the G35 antibody. Work was carried out at Spinal Studies, ARC/TORCH Building, Robert Jones Agnes Hunt Orthopaedic Hospital NHS Trust, Oswestry, Shropshire SY10 7AG, UK.
Declaration of Conflicting Interests
The authors have no known conflict of interest, although C.R.F. is employed by Pfizer Inc.
Funding
The authors received no financial support for the research and/or authorship of this article.