
Abstract
Sport participation is an important part of the development, both physically and mentally, of children and adolescents in the United States. Illness and injury associated with sport and physical activities may occur in the school setting. Although most sport-related illness and injury in students are considered minor emergencies, life-threatening illnesses or injuries may occur. It is important for the school nurse to recognize potential life-threatening emergencies associated with sport and physical activity, to initiate stabilization of the student with life-threatening symptoms, and to triage these students to an appropriate level of care (back to the classroom, home with their guardian with follow up at their primary healthcare provider’s office, or directly to the closest emergency department [ED] via Emergency Medical Services [EMS]). This article specifically describes the initial assessment and management of shoulder and hip injuries in pediatric athletes.
Keywords
Who is the ER Pediatrician?
Dr. Robert Olympia, MD, is a pediatric emergency medicine physician with over 20 years of experience, currently working in an emergency department in the Sweetest Place on Earth (Hershey, PA). He is a professor in the Departments of Emergency Medicine and Pediatrics at the Penn State College of Medicine. His research interests include emergency and disaster preparedness for children in the setting of schools and school-based athletics, as well as in sport-related illness and injuries. He has presented his research both regionally and nationally and has lectured on a variety of topics pertaining to pediatric emergency medicine, such as fever and infectious diseases, trauma, sports-related injuries, and disaster preparedness.
Who are Dr. Olympia’s Co-Author?
Dr. Elizabeth Brigham, MD, is currently a third-year Pediatric Critical Care fellow at the Johns Hopkins Children’s Center and will be joining the Division of Critical Care Medicine at West Virginia Children’s Hospital in the summer of 2022. Her research interests include pediatric trauma and medical education.
What is the Purpose of the “School Nurses on the Front Lines of Healthcare” Series?
The “School Nurses on the Front Lines of Healthcare” series presents cases reflecting emergencies commonly encountered in the school setting, focusing on an evidence-based approach to the initial management, stabilization, and disposition of the ill or injured child.
Special features unique to each article are Extra-credit points and Report Cards. Extra-credit points are trivia questions or clinical pearls scattered throughout the article related to the topic at hand. Report Cards are concise tables summarizing key points in each article that you can photocopy and laminate, or photograph and keep on your smart device, for easy access.
Case 1
As you are walking to the parking lot after a busy day in the school nurse’s office, you hear commotion coming from the adjacent football field. Jalen, a 16-year-old quarterback for the varsity football team, is sitting on the ground clutching his right shoulder. During drills, a defensive lineman accidentally tripped over the offensive lineman, collided into Jalen, and both were taken to the ground, with the entire weight of the defensive lineman landing on Jalen’s right shoulder. Jalen denies loss of consciousness or neck pain, but complains of right shoulder pain. After taking Jalen’s practice jersey and shoulder pads off, you perform a quick examination of the shoulder and decide to call 911 to transport Jalen to your local emergency department (ED). What do you think happened to Jalen?
Checking for “SPASMS”
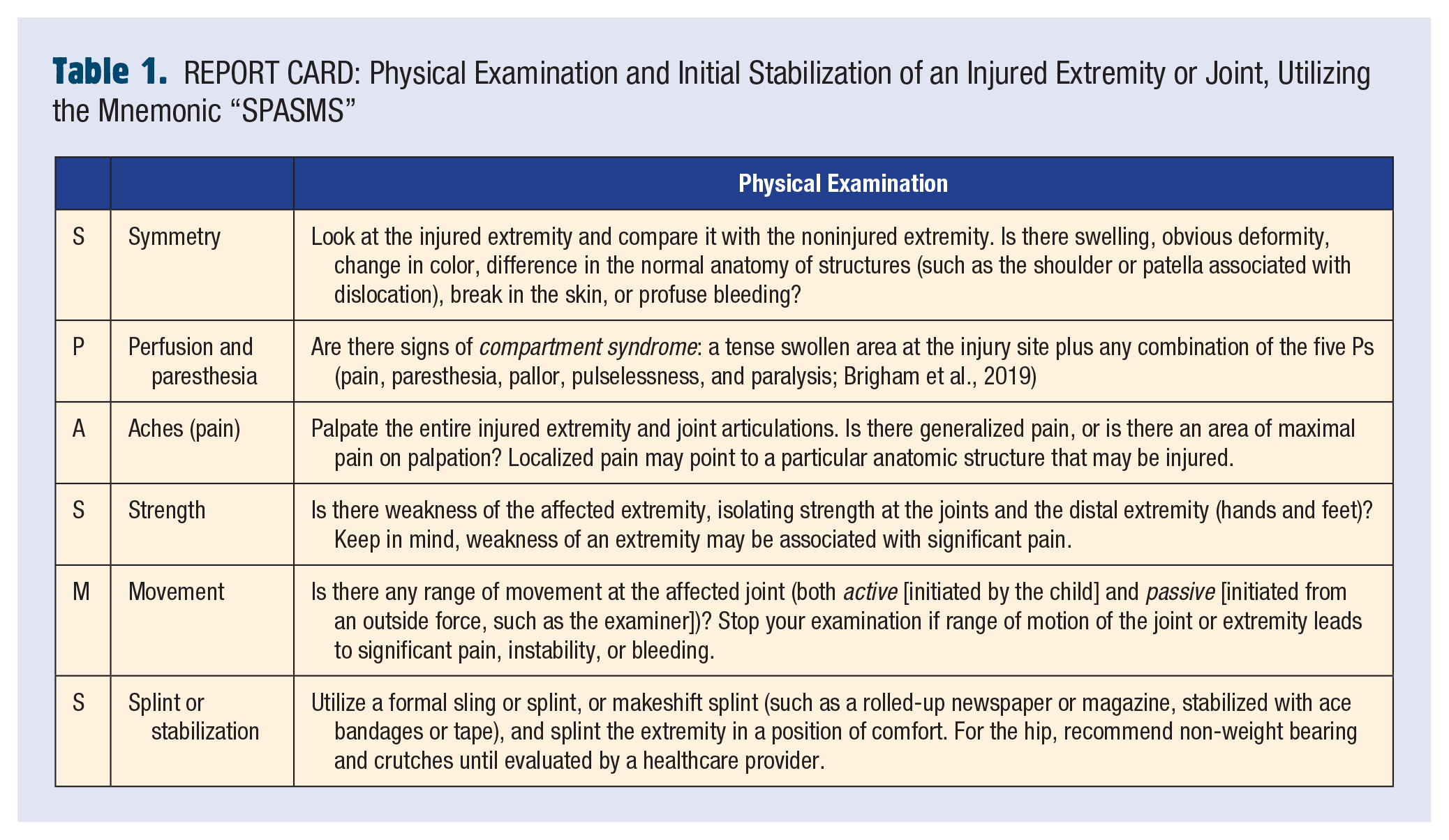
In a student who has sustained an extremity injury, it is important to perform a quick examination of the extremity and joints to determine disposition: immediate transfer to the nearest ED, transport to a local urgent care center, or follow-up at the student’s primary care physician’s office. A mnemonic developed by the authors to perform a quick examination of an injured extremity is “SPASMS” (Table 1. REPORT CARD).
REPORT CARD: Physical Examination and Initial Stabilization of an Injured Extremity or Joint, Utilizing the Mnemonic “SPASMS”
Case 1 Progression
You perform a quick examination of Jalen’s right upper extremity utilizing the “SPASMS” mnemonic:
S (symmetry)—You notice an asymmetry of Jalen’s shoulder, with a loss of the normal round contour of the right shoulder compared with the left shoulder.
P (perfusion and paresthesia)—Jalen has normal perfusion of his right upper extremity, with good radial pulses and normal color, temperature, and capillary refill of his right upper arm, forearm, and hand. On examination of his right upper extremity for paresthesias, you notice decreased sensation over his lateral shoulder.
A (aches/pain)—You palpate Jalen’s right upper extremity from his sternal notch to his fingers, and elicit tenderness to palpation over his shoulder.
S (strength)—Jalen has normal grip strength in his right hand, but has “weakness” on shoulder abduction and elbow flexion and extension. You get a sense that the “weakness” may be related to pain associated with his shoulder injury.
M (movement)—Jalen has no active movement of his right shoulder, likely due to pain. Passive range of motion of his right shoulder results in significant pain and discomfort.
S (splint/stabilization)—After your assessment of Jalen’s right shoulder, you place him in a shoulder immobilizer sling and place a bag of ice over his right shoulder prior to transfer to the ED.
In addition to performing a quick examination of Jalen’s right upper extremity, you assess for other traumatic injuries utilizing the information gathered from other published articles in the “School Nurses on the Front Lines of Healthcare” series, including a head injury/concussion (“Reasons for direct referral to the ER following head trauma” from Olympia, 2017) and cervical spine injury (“Predictors of cervical spine injuries in children” from Swaffield & Olympia, 2021). Based on your initial assessment, you have no concerns for significant head and cervical spine injuries.
Causes of Shoulder Pain in a Pediatric Athlete and Disposition
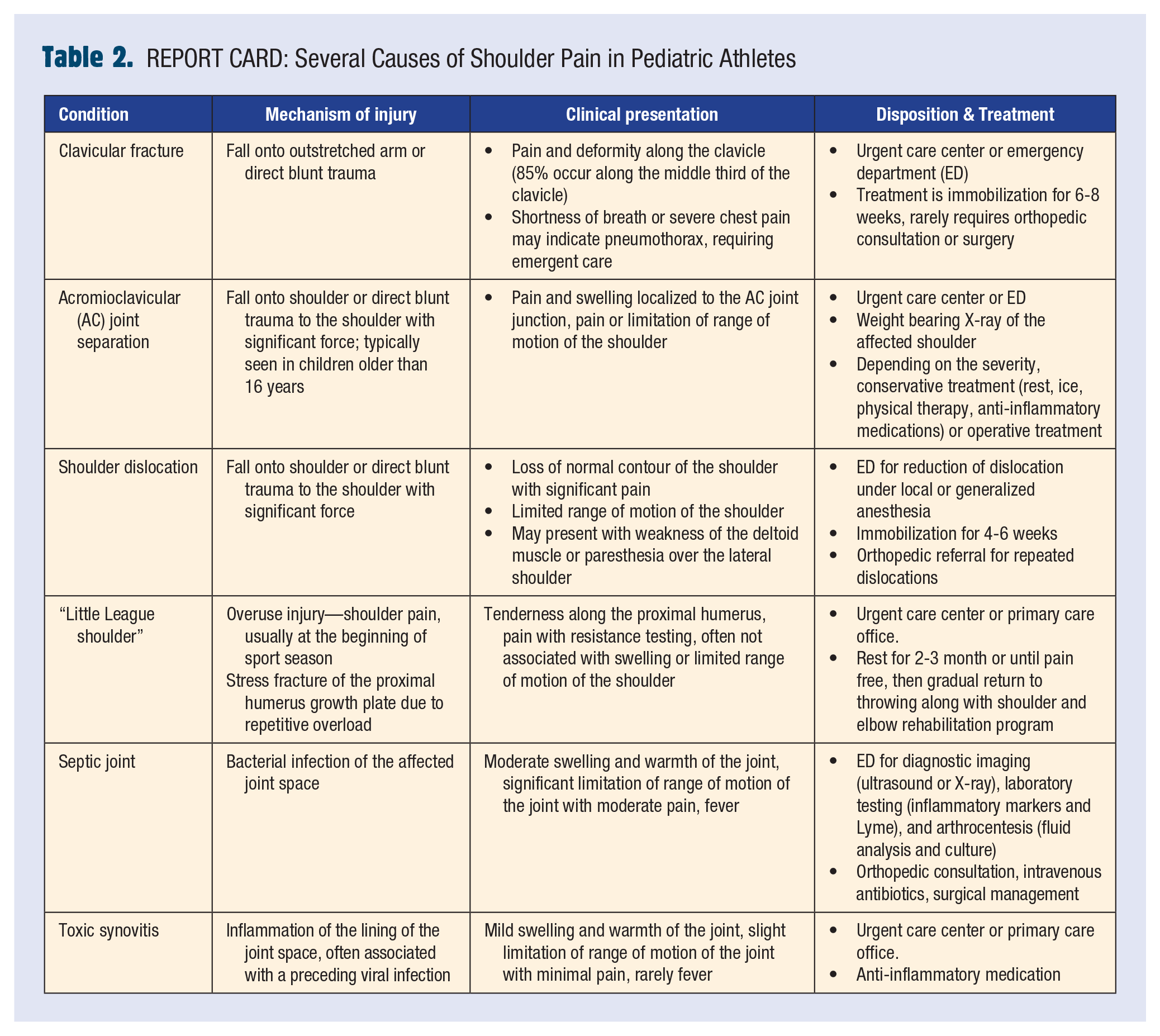
In addition to fractures, sprains, and strains, other causes of shoulder pain in pediatric athletes can be found in Table 2. REPORT CARD. After utilizing the “SPASMS” mnemonic, you remember extremity injuries that require immediate evaluation in an ED (Table 3. REPORT CARD, from Brigham et al., 2019). Based on these criteria, you make the decision to transfer Jalen to your local ED.
REPORT CARD: Several Causes of Shoulder Pain in Pediatric Athletes
REPORT CARD: Extremity Injuries That Require Immediate Evaluation in an Emergency Department (ED)
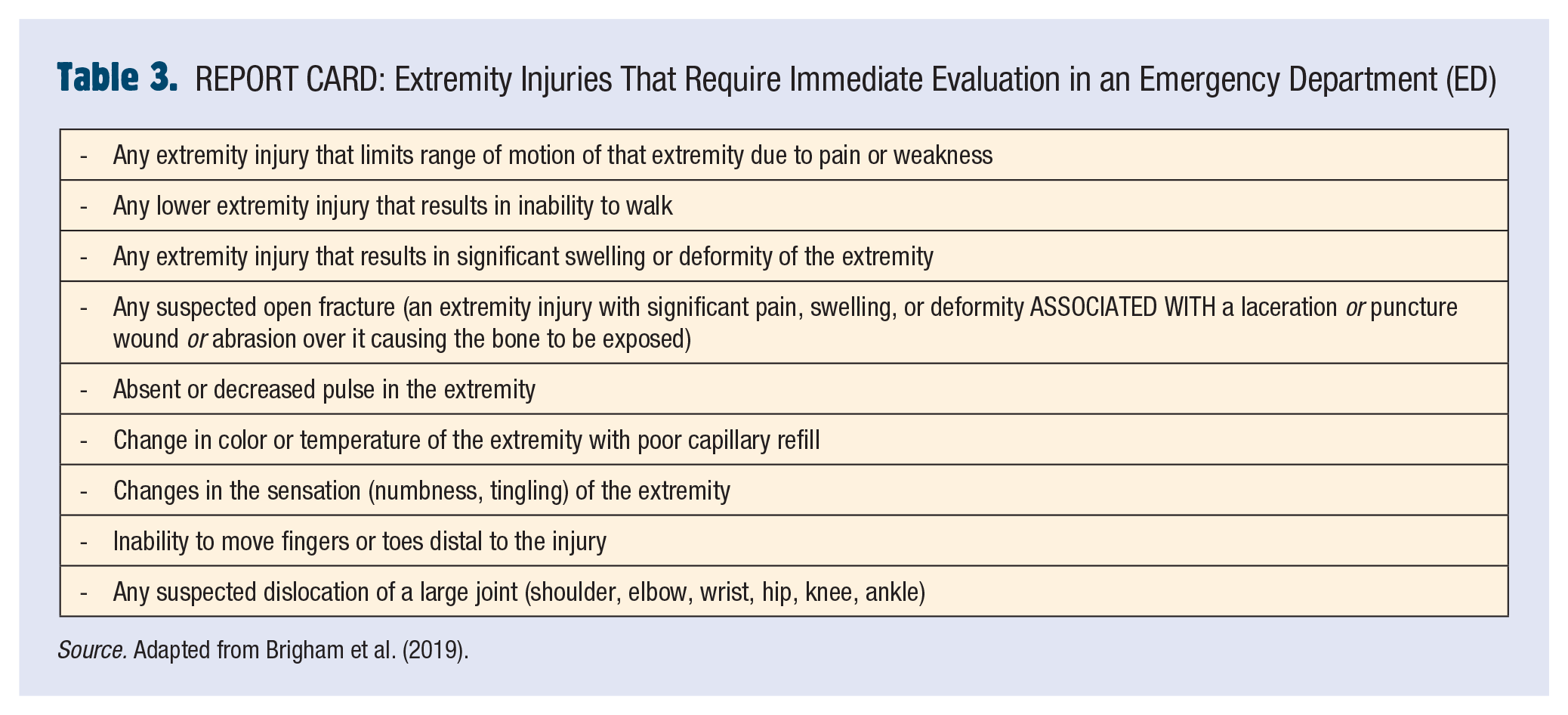
Source. Adapted from Brigham et al. (2019).
Extra-Credit Point: What is the Difference Between a Sprain and a Strain?
The difference between a sprain and a strain is that a sprain involves tearing or overstretching of a ligament (connect bones to bones) and a strain involves tearing or overstretching of a tendon (connects bones to muscles). The treatment of mild sprains and strains is the RICE (rest, ice, compression, and elevation) technique and physical therapy. Severe sprains and strains often require advanced diagnostic imaging (magnetic resonance imaging [MRI]), orthopedic surgery referral, and possible surgical management.
Case 1 Resolution
Based on your assessment of Jalen’s right upper extremity, you recognize a possible right shoulder dislocation. Jalen is transported to your local ED where your suspicion is confirmed by a radiograph of his shoulder. Jalen receives procedural sedation, and his shoulder dislocation is reduced by the pediatric ED physician. He is discharged from the ED with a shoulder immobilizer and instructions to follow up with a sports medicine specialist. Unfortunately, Jalen’s football season is over, but during his senior season, he leads your school to the state’s championship game and wins it all.
Shoulder Dislocations in Pediatric Athletes
Shoulder dislocations are relatively rare in school-age children, as they are more likely to fracture a bone (clavicle or humerus) than they are to dislocate their shoulder. Less than 2% of all traumatic shoulder dislocations occur in children less than 10 years of age, and approximately 20% occur in children and adolescents aged 10 to 20 years (Franklin & Weiss, 2019). The mechanism of a traumatic shoulder dislocation is often related to a fall onto a shoulder or to blunt trauma directed to the shoulder with significant force (forces applied to an abducted, extended, and externally rotated arm). Some pediatric athletes may be prone to spontaneous shoulder dislocations or dislocations due to minor trauma due to laxity of their joints. Ninety percent of shoulder dislocations are anterior dislocations of the humeral head in relation to the glenoid fossa (visualize a ball and socket, where the ball is the humeral head and the socket is the glenoid fossa).
On physical examination of a student with a shoulder dislocation, there is often loss of normal round contour of the affected shoulder, limited range of motion of the shoulder, and significant pain with attempts of movement (Lazaro & Cordasco, 2017). The student may present with weakness of the deltoid muscle or loss of sensation over the lateral shoulder due to injury of the axillary nerve. Immediate shoulder stabilization with a sling and transfer to the ED is part of the initial management.
Diagnosis of a shoulder dislocation is made with a radiograph of the affected shoulder, ruling out any fractures of the surrounding bones of the shoulder and confirming the dislocation. Although there are various techniques to relocate a dislocated shoulder (traction-countertraction, scapular technique, external rotation method, Cunningham technique, FARES method; Gottlieb, 2020), the key to a successful reduction is pain control (either from relaxation techniques, procedural generalized sedation, or local anesthesia from ultrasound guided intra-articular injections of pain medication). Following the reduction, radiographs are repeated to confirm a successful reduction and rule out complications from the reduction, such as a Bankart lesion (fracture of the glenoid fossa) or Hill-Sachs lesion (fracture of the proximal humeral head). In most cases, discharge instructions should include immobilization for 4 to 6 weeks and a referral to a sports medicine or orthopedic surgery specialist.
Case 2
You decide to stay after school to support your middle school students who are rehearsing for the school musical. One of the teachers grabs your attention and asks if you have noticed that one of the students has been limping on stage during rehearsal. Camden is a 13-year-old overweight student with no past medical history. When you ask him about his limp, he tells you that his left knee and hip have been bothering him for the past 3 to 4 weeks. He can still bear weight on his leg, but the pain associated with walking and dancing has worsened recently. He has had no fever or recent illness. Despite being a member of your school’s soccer team, he denies any particular injury to his left leg. What do you do next?
Case 2 Progression
You perform a quick examination of Camden’s lower extremities utilizing the “SPASMS” mnemonic:
S (symmetry)—There is no obvious asymmetry, deformity, or swelling noted.
P (perfusion/paresthesia)—Camden has normal perfusion and sensation of his bilateral lower extremities.
A (aches/pain)—There is no pain on palpation of his bilaterally lower extremities.
S (strength)—Camden has normal strength of his lower extremities.
M (movement)—Camden has normal range of motion of his left knee and ankle, but has mild pain on flexion and abduction about his left hip. He has a noticeable limp when walking.
S (splint/immobilization)—After your assessment of Camden’s lower extremities, you recommend non-weight bearing and crutches until evaluated at your local ED.
After performing a quick examination of Camden’s lower extremities, you assess for other possible life-threatening causes of hip pain, including appendicitis (his abdomen is soft and nontender) and testicular torsion (he denies testicular pain; Olympia & Brady, 2016).
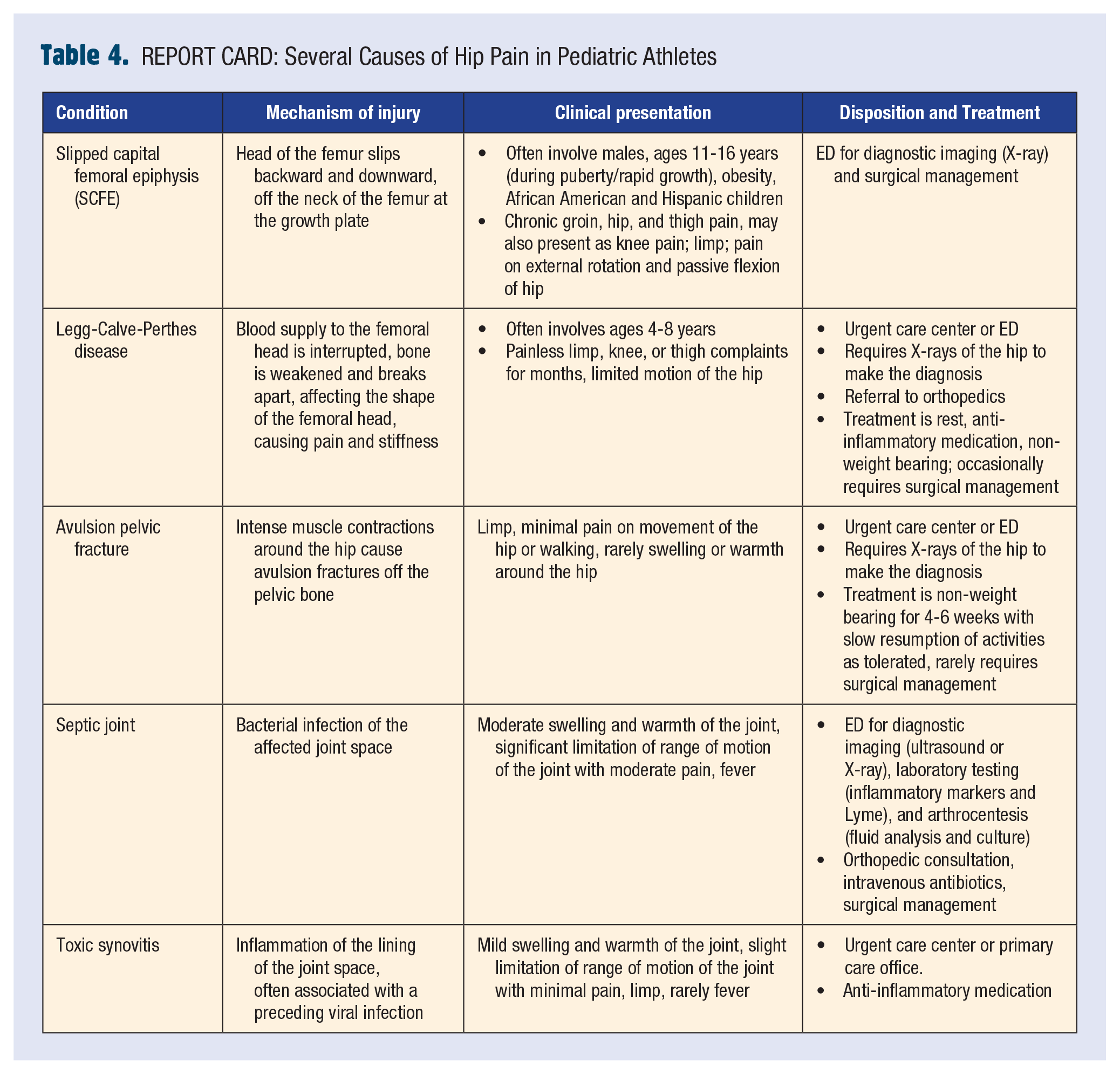
In addition to fractures, sprains, and strains, other causes of hip pain in pediatric athletes can be found in Table 4. REPORT CARD. Based on your recollection of extremity injuries that require immediate evaluation in an ED (Table 3. REPORT CARD, from Brigham et al., 2019), you make the decision to transfer Camden to your ED for evaluation.
REPORT CARD: Several Causes of Hip Pain in Pediatric Athletes
Extra-Credit Point: Pediatric Athletes With Hip Injuries or Hip Disease May Present With Anterior Thigh and/or Medial Knee Pain, Why?
Children and adolescents with hip injuries/pathology may present with anterior thigh and/or medical knee pain due to referred pain from the femoral and obturator nerves.
Case 2 Resolution
In the ED, a radiograph of his bilateral hips confirms the diagnosis of left-sided slipped capital femoral epiphysis (SCFE). Orthopedic surgery is consulted, and Camden has surgery to place percutaneous pins in his hip to stabilize his SCFE. Camden makes a full recovery after several months of physical therapy.
Not Your Normal “Slip”
SCFE is often seen in children 11 to 16 years of age during puberty and rapid growth spurts (Castillo & Mendez, 2018). Risk factors for SCFE include being male (male-to-female ratio of 2:1.4), being from an African American or Hispanic race, or being obese. Other associated conditions include hypothyroidism, renal osteodystrophy, growth hormone deficiency, and panhypopituitarism. SCFE is described as a disorder of the head of the femur along the physis (growth plate), which leads to slippage of the head of the femur in a backward and downward direction, off the neck of the femur.
Children with SCFE often complain of chronic groin, hip, thigh, or knee pain, and the pain may be exacerbated by physical activity or during sport. On physical exam, the affected hip often lacks swelling or warmth, and there may be mild-to-moderate pain on external rotation and passive flexion of hip.
Children who may have an SCFE should be referred to the ED for diagnosis and management. Radiographs should be performed on both hips, as 10% of children with SCFE have bilateral involvement. Hip X-rays findings associated with SCFE are often described as “ice cream following off an ice cream cone.” Delay in the diagnosis of SCFE may lead to chronic painful arthritis or a limb length discrepancy later in life. Treatment is surgical (alignment of the fracture with pins), followed by physical therapy.
Conclusion
Shoulder and hip injuries are common in pediatric athletes. The assessment for concomitant injuries (such as head and cervical spine injuries) and life-threatening medical conditions (such as appendicitis or testicular/ovarian torsion in an athlete with hip pain) is important. Utilizing the mnemonic “SPASMS” and remembering extremity injuries that require immediate evaluation in an ED will help the school nurse determine disposition.
Footnotes
Robert is a physician boarded in both Pediatrics and Pediatric Emergency Medicine with over 20 years of clinical experience. His research interests include emergency and disaster preparedness for children in the setting of schools and school-based athletics.
Dr. Elizabeth Brigham, MD, is currently a third-year Pediatric Critical Care fellow at the Johns Hopkins Children’s Center and will be joining the Division of Critical Care Medicine at West Virginia Children’s Hospital in the summer of 2022. Her research interests include pediatric trauma and medical education.