
Abstract
Introduction. The purpose of this study was to identify deficiencies in pediatric residents’ and pediatricians’ knowledge and confidence in diagnosing slipped capital femoral epiphysis (SCFE). Methods. Pediatricians and residents at our institution answered an anonymous 12-question survey on knowledge and confidence in SCFE diagnosis. Results. Twenty pediatricians and 30 pediatric residents participated in the survey. Of 30 residents, 22 (77%) reported low confidence ordering radiographs evaluating for SCFE in patients with hip pain. Four of 20 pediatricians (20%) reported low confidence ordering radiographs for patients with hip pain. Forty percent (8/20) of pediatricians did not feel comfortable diagnosing a SCFE based on radiographs, which was significantly different from 80% (24/30) of residents who did not feel comfortable diagnosing a SCFE based on radiographs (P = .004). There was a significant difference between residents and pediatricians in comfort ordering and diagnosing radiographs (P < .01). There was no significance between pediatrician and resident scores for knowledge-based questions (P = .50). Discussion. Despite scoring well on knowledge-based questions, more than half of pediatricians and pediatric residents felt uncomfortable ordering radiographs to evaluate for SCFE in patients with hip or knee pain. This may be one factor contributing to the continued delay in SCFE diagnosis.
Introduction
Slipped capital femoral epiphysis (SCFE) is the leading adolescent hip disease. 1 The reported incidence of SCFE in the United States is 10.8 cases per 100 000 children. 2 There have been numerous studies highlighting the significant delay to diagnosis over the past 50 years with minimal improvement.3-5 The most recent studies have reported an average delay of 17 weeks. 6 These studies also highlighted significant diagnostic errors by primary care physicians (PCPs) with 52% missed diagnosis including growing pains and flat feet.4,5 Hosseinzadeh et al found that while non-orthopedic providers see 75% of patients with SCFE initially, the average time from the first visit to diagnosis of SCFE was 94 days compared with an average of 2.9 days when evaluated by an orthopedist. 7 Vague symptoms may be misleading to non-orthopedic physicians as SCFE can present with knee or distal thigh pain. Kocher et al identified patients with a chief complaint of knee or distal thigh pain as one of the greatest risk factors for delay of diagnosis. 8 A recent study has shown that pediatricians have low sensitivity, specificity, and accuracy diagnosing SCFE on standard anteroposterior (AP) and frog lateral pelvis radiographs. 9 The result in delay of diagnosis has detrimental impact on long-term hip morbidity including pain, decreased range of motion, chondrolysis, and degenerative joint disease. 10 In Norway, pediatric hip diseases account for 9% of total hip replacements. 11 These studies underscore gaps in physician education is a potential contributing factor to the continued delay and should be a focus to improve this delay.
The purpose of this pilot study is to identify deficiencies in pediatric residents’ and pediatricians’ knowledge and confidence in diagnosing SCFE. Ultimately, we aim to use this to develop a strategy for achieving a more rapid diagnosis and preventing the devastating complications that result from these delays.
Materials and Methods
In order to investigate knowledge and confidence in diagnosing SCFE, a 12-question survey was created using the RedCap database. The survey questions were developed by the investigators, a board-certified orthopedic surgeon and board-certified pediatrician who completed a nonoperative pediatric orthopedic fellowship, respectively. Five multiple-choice questions examined the participants’ knowledge of SCFE, and 7 Likert-type scale questions assessed their clinical confidence in diagnosing the disorder. Confidence was defined as follows: scores 1 to 3 were categorized as not comfortable, and scores 4 and 5 were categorized as comfortable and very comfortable. The survey link was emailed to 90 pediatric residents (postgraduate year [PGY]—post graduate level I, II, and III) and 90 pediatricians at our institution to participate in the study. This study was approved by our institutional review board.
Exclusion criteria included completion of pediatric orthopedic, primary care sports medicine or radiology training given that this study’s aim was to focus on non-orthopedic physicians. Two pediatricians with prior orthopedic training who completed the survey and 1 radiologist were excluded. The survey was closed after 1 month online. Data were analyzed using 1-way analysis of variance and χ 2 tests to determine significant differences. The level of confidence was set at P < .05.
Ethics and Informed Consent
This study was reviewed by the Committee of Clinical Investigations (institutional review board) at the authors’ institution. Waiver of informed consent was granted per 45 CFR 46.116(d).
Results
A total of 50 participants at our institution completed the survey that met the inclusion criteria (30 residents, 20 pediatricians). Sixty percent (30/50) were residents: 7 PGY-I, 14 PGY-II, and 9 PGY-III (Figure 1). On knowledge-based questions, residents scored a mean 4.4/5 (88%; range = 40% to 100%). Ninety percent (27/30) of residents were able to identify obligate external rotation as a diagnostic for SCFE. Thirteen percent of residents (4/30) did not correctly identify ordering AP and frog lateral pelvis radiographs as the appropriate initial diagnostic test when they were suspicious of a SCFE (Figure 2). On clinical confidence questions, 77% (23/30) did not feel comfortable ordering radiographs for patients with hip pain, and 87% (26/30) of residents did not feel comfortable obtaining radiographs for patients who report knee pain. There were no significant differences between the level of training and comfort of diagnosing a SCFE on radiographs (P = .50).

Participating resident demographics. Reproduced with permission from Children’s Orthoapedic Center, Los Angeles.
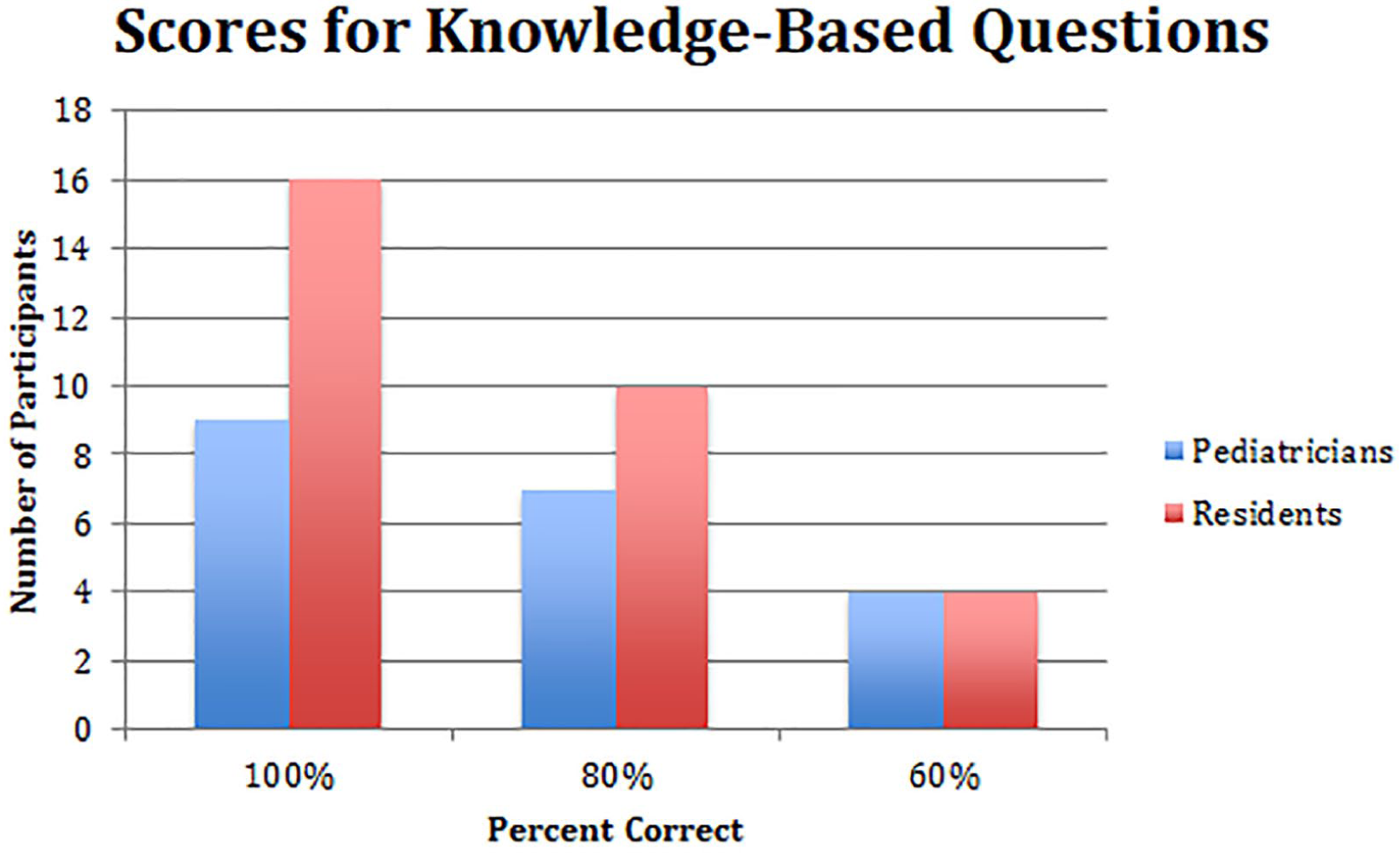
Percent of correct responses for knowledge-based survey questions among residents and pediatrician. Reproduced with permission from Children’s Orthoapedic Center, Los Angeles.
Twenty pediatricians completed the survey (12 general pediatricians and 8 pediatric emergency medicine [PEM] physicians). On knowledge-based questions, pediatricians answered a mean 4.25 out of 5 correct (85%; range = 40% to 100%). Ninety percent (18/20) of pediatricians were able to identify obligate external rotation as a diagnostic for SCFE. On clinical confidence questions, 20% of pediatricians (4/20) did not feel comfortable ordering radiographs for patients with hip pain, while 25% (5/20) of pediatricians did not feel comfortable ordering radiographs on patients who presented with knee pain. Forty percent (8/20) of pediatricians did not feel comfortable diagnosing a SCFE based on radiographs.
We performed a subanalysis of the pediatricians in 2 groups: general pediatricians and PEM physicians. On knowledge-based questions for general pediatricians, they answered a mean 4.3 out of 5 correct (86%; range = 60% to 100%). On clinical confidence, 42% (5/12) of general pediatricians did not feel comfortable ordering radiographs for patients with knee pain, while 33% (4/12) did not feel comfortable ordering radiographs on patients who presented with hip pain. Sixty-seven percent (8/12) of general pediatricians did not feel comfortable diagnosing a SCFE by radiographs (Figure 3). When evaluating data from the PEM physicians, all PEM-trained physicians reported being comfortable ordering radiographs in patients who presented with hip or knee pain and diagnosing a SCFE on radiographic X-ray. There was a significant difference between being a PEM physician and comfort level in ordering radiographs for patients presenting with hip or knee pain (P = .01).

Comfort of Ordering Radiographs with patients presenting with hip or knee pain. Percentage of survey respondents who feel comfortable with diagnosing slipped capital femoral epiphysis based on clinical examination and imaging. Pediatricians were significantly more comfortable ordering diagnostic radiographs for patient with hip or knee pain compared with residents (*P < .001). Reproduced with permission from Children’s Orthopedic Center, Los Angeles.
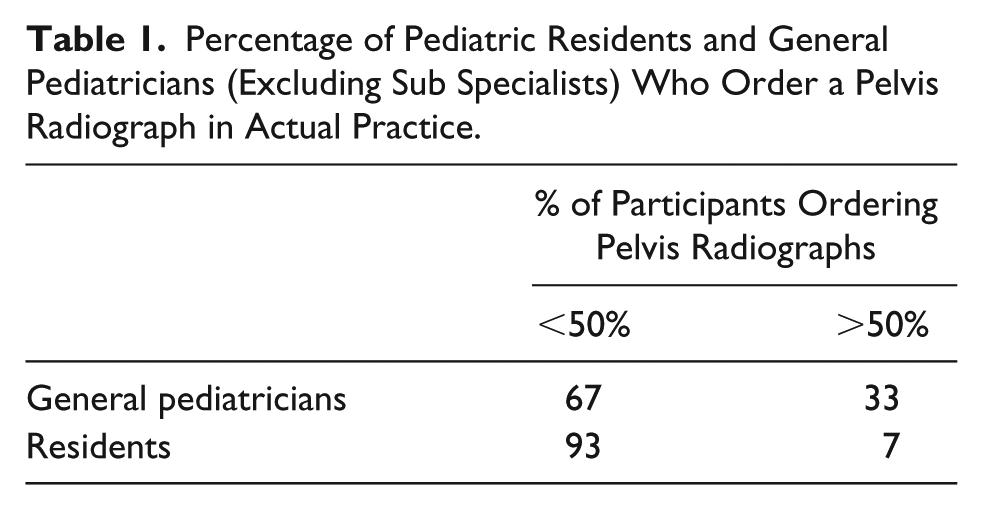
There was no significant difference in knowledge-based scores between residents and all pediatricians (P = .50). There was a significant difference between the residents’ and pediatricians’ comfort level with ordering radiographs for hip or knee pain (P < .001). Additionally, there was a significant difference between the residents’ and pediatricians’ comfort level with diagnosing SCFE by radiographs (P < .004). There was no significant difference in the comfort level and ordering radiographs for hip or knee pain in residents (P = .50) or pediatricians (P = .15). Sixty-seven percent (8/12) of general pediatricians and 93% (28/30) of residents self-reported that in their practice, they order pelvis X-rays on less than 50% of patients who presented with hip or knee pain (Table 1). There was a significant difference between pediatricians and residents with ordering radiographs in practice (P < .01).
Percentage of Pediatric Residents and General Pediatricians (Excluding Sub Specialists) Who Order a Pelvis Radiograph in Actual Practice.
Discussion
This current study is the first to explore the comfort of pediatric residents and pediatricians in ordering and interpreting imaging to diagnose SCFE. We found there was a significant difference in physician comfort and in the actual practice of ordering radiographs between residents and pediatricians. Musculoskeletal complaints comprise 15% of outpatient general pediatric visit and 63% of graduating pediatric residents go into primary care. 12 A 2009 study in the United Kingdom demonstrated that both residents and experienced physicians in primary care and pediatrics scored lowest in self-confidence in the general pediatric musculoskeletal assessment. 13 However, scores were significantly better among PCPs if they had completed an orthopedic rotation in medical school or residency. 14 A prospective study done by Piazza et al showed a structured, 1-month, elective orthopedic rotation during pediatric residency led to increase in pretest musculoskeletal medicine examination scores and clinical confidence by the end of the rotation on the posttest examination. 15 This further supports the need for more pediatric resident musculoskeletal education.
Based on our survey responses, pediatricians appear to be more comfortable ordering imaging compared with residents. However, over half of general pediatricians reported they were not comfortable diagnosing SCFE on radiographs even if they felt comfortable obtaining initial imaging. Additionally, over 50% of the pediatricians reported that less than half the time, they actually order imaging on patients presenting with hip or knee pain. In a recent study by Lam et al, pediatricians were unable to recognize radiographs consistent with SCFE diagnosis with the lowest sensitivity (24% to 76%) compared with pediatric orthopedic surgeons and radiologists (>88%) when shown blinded AP and frog lateral pelvis radiographs. 9 One reason is that pediatricians may be relying on the radiology report instead of assessing their own imaging as many patients in a primary care setting go to an off-site imaging center for their radiographs. In the current study, there was not a question asking if pediatricians or residents looked at the actual pelvis radiographs compared with radiologist report. Another reason for less comfort with ordering imaging could be related to the implementation of the Choosing Wisely campaign, which encourages providers to be selective in the use of diagnostic imaging. 16 With an emphasis on the frontline primary care providers being more conservative about ordering imaging, they may have become less comfortable with the ordering and interpretation of imaging. The risk of missed SCFE diagnosis with consequences such as early-onset osteoarthritis and femoral acetabular impingement with significant morbidity has to be balanced against minimizing radiation to patients and cost to the system. 17 While there has been evolution in surgical techniques including the modified Dunn procedure, which has been reported to have beneficial long-term outcomes for severe slips with low rate of avascular necrosis, late or missed diagnosis continues to be an issue that affects treatment options and long-term outcomes.18,19
A clinical algorithm or decision tool may be helpful in determining when to obtain radiographs to evaluate for SCFE. For example, the Ottawa Ankle rules were developed by Stiell et al as a clinical decision tool to assist emergency department (ED) physicians deciding when to order ankle radiographs with acute ankle injuries. 20 In the future, use of decision criteria would be helpful to provide a framework for pediatricians making a clinical decision to obtain AP and frog lateral pelvis radiographs for pediatric patients presenting with hip or knee pain to evaluate at-risk patients for SCFE and to review pertinent radiographic findings such as Klein’s line though it has not been shown to be sensitive and Drehmann’s sign of obligate external rotation on clinical examination. 21
A delay or missed diagnosis of SCFE is not only clinically significant but also has economic repercussions. While pediatric orthopedic litigation only accounts for 11% of claims, misdiagnosis of SCFE is among the top 10 pediatric orthopedic conditions resulting in malpractice claims and accounts for the highest payout. In the United Kingdom, it was reported by the Medial Defense Union, there are 5 to 10 claims related to diagnostic delays in SCFE each year, which can each settle for up to £500 000 (US$ 612 000).22,23
Previous studies have focused on the identification and reporting this delay in diagnosis. Although this delay is multifactorial, with patient and physician factors, this study has allowed us to identify one of the potential contributing factors to delayed diagnosis as the lack of comfort pediatricians have with ordering and interpreting the necessary radiographs to make the diagnosis. It also serves to help identify areas to focus on in the development of a SCFE education module.
In addition, both general pediatricians and emergency medicine physicians are the first-line physicians to examine and diagnose a patient with SCFE. Schur et al demonstrated in 2016 in 481 patients, the time from first evaluation to diagnosis was significantly shorter for patients evaluated at an orthopedic clinic (0 weeks) than patients seen by their primary care provider (4 weeks) or at an ED (6 weeks). 6 It was interesting in our study that all emergency room physicians reported being comfortable with obtaining imaging and diagnosing SCFE based on X-ray. There seems to be a discrepancy, given the literature supports there is a longer delay to diagnosis in those presenting in the ED of 6 weeks. Given that there has been no significant change in delay to diagnosis of SCFE in over a decade, it is time to focus on addressing the education gaps of pediatric residents, PCPs, and emergency medicine physicians. By partnership of leading organizations such as Pediatric Orthopaedic Society of North America, the American Academy of Pediatrics, American Academy of Family Medicine, and American College of Emergency Physicians, there can be a focus to not only highlighting the importance of missed SCFE diagnosis but to also development of a position statement, live and web-based continued medical education modules, and diagnostic criteria algorithmic tools to promote education.
We acknowledge that there were several limitations to this study including small sample size, poor response rate, and survey question design and validation. Our survey questions did not ask residents their career plans to go into primary care or subspecialty. The survey also did not ask about prior exposure to orthopedics such as rotations completed in medical school or residency. Additionally, there was no question about the importance of an urgent referral to an orthopedics or emergency department once SCFE is diagnosed. We did not ask about the radiographic parameters to diagnose SCFE and did not include actual pelvic radiographs of patients with SCFE to confer accuracy of respondents and compare this with perceived confidence. Pediatricians practicing in urban settings may have access to pediatric radiologists, and therefore, the pediatrician may not be reading their own radiographs or making final decisions based on their own interpretation of the X-rays. This could contribute to discomfort of interpreting radiographs given potential reliance on radiologist to read the imaging. This discomfort could be greater in rural settings where there is limited access to pediatric radiologist. Regional differences can contribute to perceived confidence. Following completion of this pilot study, we plan further investigation into the factors contributing to these results. In turn, these data can be used to implement a SCFE educational module with scores of both knowledge and confidence before and after the module. Additionally, comparing primary care/urgent care pediatricians and PEM physicians in comfort and ability to identify SCFE on radiographs would be helpful given these physicians are at the frontline to diagnose and refer a patient with SCFE. Education can then be tailored in terms of the best type, methodology, and length to those physicians practicing in both the general outpatient setting as well as in the ED.
In conclusion, both pediatric residents and pediatricians are knowledgeable regarding the physical examination findings and diagnosis of SCFE; however, this does not translate to confidence in diagnosing the disorder radiographically in those patients presenting with hip or knee pain. Further education is necessary to improve confidence in diagnosis and management of SCFE in both pediatric residents and pediatricians.
Footnotes
Author Contributions
JM, NS for drafting manuscript; MAB as PI, significant edits, corresponding author; LMA: develop question and edits; DLS: edits; RYG: edits; BRE: edits; TLZ: edits.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.