
Abstract
We present a case report of a previously healthy 29 year old woman who developed thromboembolic events in rapid fashion after a recent orthopedic surgery. This case highlights the importance of understanding risk factors for clot formation even in those who had no prior events, the efficacy of novel aspiration techniques to remove emboli, and how rapid triaging of acute symptoms can lead to the best outcomes. She presented to the emergency department with shortness of breath and was found to have a large bilateral pulmonary embolus. She was given intravenous thrombolysis. Shortly after, she developed aphasia and right-sided weakness and was taken emergently for mechanical thrombectomy of a left middle cerebral artery occlusion. She was later found to have a patent foramen ovale and a highly mobile right atrial thrombus which was aspirated. Further evaluation revealed right lower extremity peroneal and popliteal deep venous thrombi. She was placed on anticoagulation, made a full clinical recovery, and was discharged home. Prompt recognition of symptoms, efficient in-hospital work flow, and a multidisciplinary approach led to an outstanding outcome in this young patient.
This case highlights a unique presentation of deep venous thrombosis secondary to a recent orthopedic injury and possible hypercoagulable state that led to life-threatening embolic events in the lungs, heart, and brain in an otherwise healthy young woman.
A 29 year old female with no significant past medical history and a surgical history remarkable for a recent tibial fracture status post open reduction and internal fixation (ORIF) presented to the emergency department with sudden onset shortness of breath. On initial presentation, patient was tachypneic and anxious but was able to answer questions and provide a reliable history. She reported having mild exertional dyspnea and a cough for a few days; however, these symptoms were not debilitating. One hour prior to her presentation, she had sudden onset, severe shortness of breath for which she was taken to the emergency department. She denied significant chest pain or hemoptysis and there was not any documentation of neurological deficits including weakness, numbness, or speech disturbances. Prior to presentation, the patient was taking daily aspirin that was prescribed after her ORIF surgery 3 months prior to presentation. She also reported being on oral contraceptive pills, specifically levonorgestre-ethinyl estrad .1 mg- 20 mcg, that were stopped 1 week prior to presentation. She denied any personal or family history of premature cardiac disease or clotting disorder, however, she reported that her father had a MTHFR (methylenetetrahydrofolate reductase) gene mutation for which he was on anticoagulation. No other family or social history was significant.
Her initial vital signs were remarkable for tachycardia with a heart rate of 145 bpm, tachypnea with a respiratory rate of 26 breaths per minute, and an oxygen saturation of 58% on room air. She was started on noninvasive ventilation with a BiPAP in the emergency department (ED) and sent for a stat CT angiogram of her chest that showed acute bilateral pulmonary emboli (PE) and evidence of right heart strain. Systemic alteplase (tPA) was given in the emergency department for her massive PE and she was transferred to the intensive care unit (ICU) for close monitoring. While being assessed in the ICU, the patient was noted to have new onset aphasia and right sided weakness which was not noted in the ED. Stroke code was activated at 65 minutes after her presentation to the ED. Her initial National Institutes of Health Stroke Scale (NIHSS) was 9 (2 for questions, 1 for commands, 1 for right facial droop, 1 for right arm drift, 2 for aphasia, and 2 for dysarthria). 1 A STAT CT head without contrast was obtained at 10 minutes after the code activation and showed loss of the left insular ribbon with a hyperdense left middle cerebral artery (MCA) sign. CT angiogram of the head performed immediately afterwards showed a distal left MCA (M1) occlusion. Thrombolytic therapy was not administered as the patient already received tPA for her PE earlier that night. The patient was taken to the angiography suite for urgent mechanical thrombectomy.
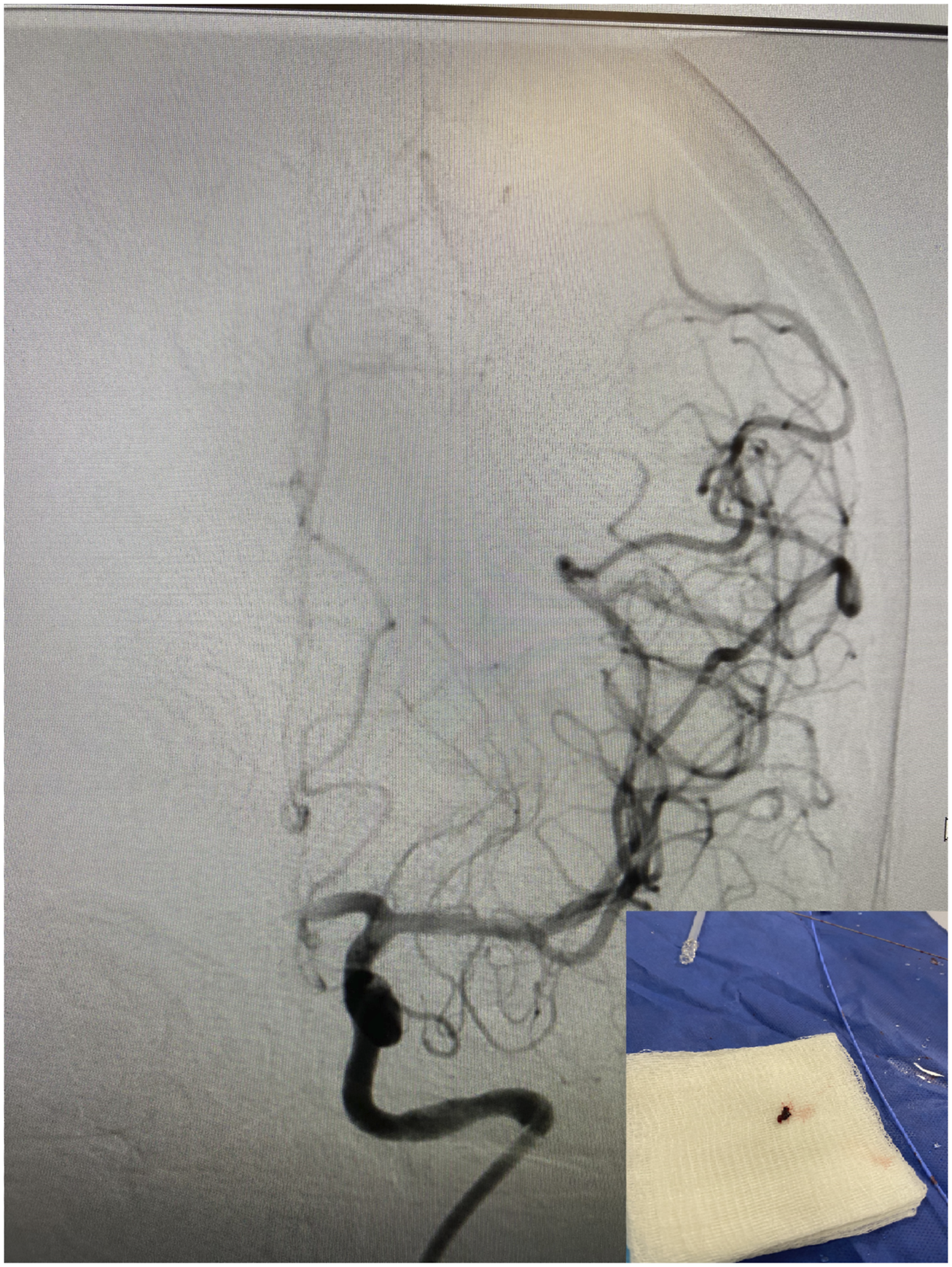
The patient was prepped and draped in the usual sterile fashion. Groin puncture was 63 minutes after stroke code activation. A 6 French sheath was advanced into the right common femoral artery. A diagnostic catheter was used to select the left common carotid artery and angiographic runs revealed an occlusion in the distal left middle cerebral artery. An exchanged length wire was used to advance into the left internal carotid artery and the diagnostic catheter and sheath were exchanged off for a 6 French 90 cm guide sheath. Then, a triaxial system of a 6 French Sofia aspiration catheter, 160 cm microcatheter, and 215 cm microwire was used to select the left middle cerebral artery. First pass was made 9 minutes after groin puncture and full Thrombolysis in Cerebral Infarction (TICI) score of 3 was achieved Figure 1 and 2.
2
Angiogram of left middle cerebral artery occlusion. Recanalized MCA and retrieved thrombus.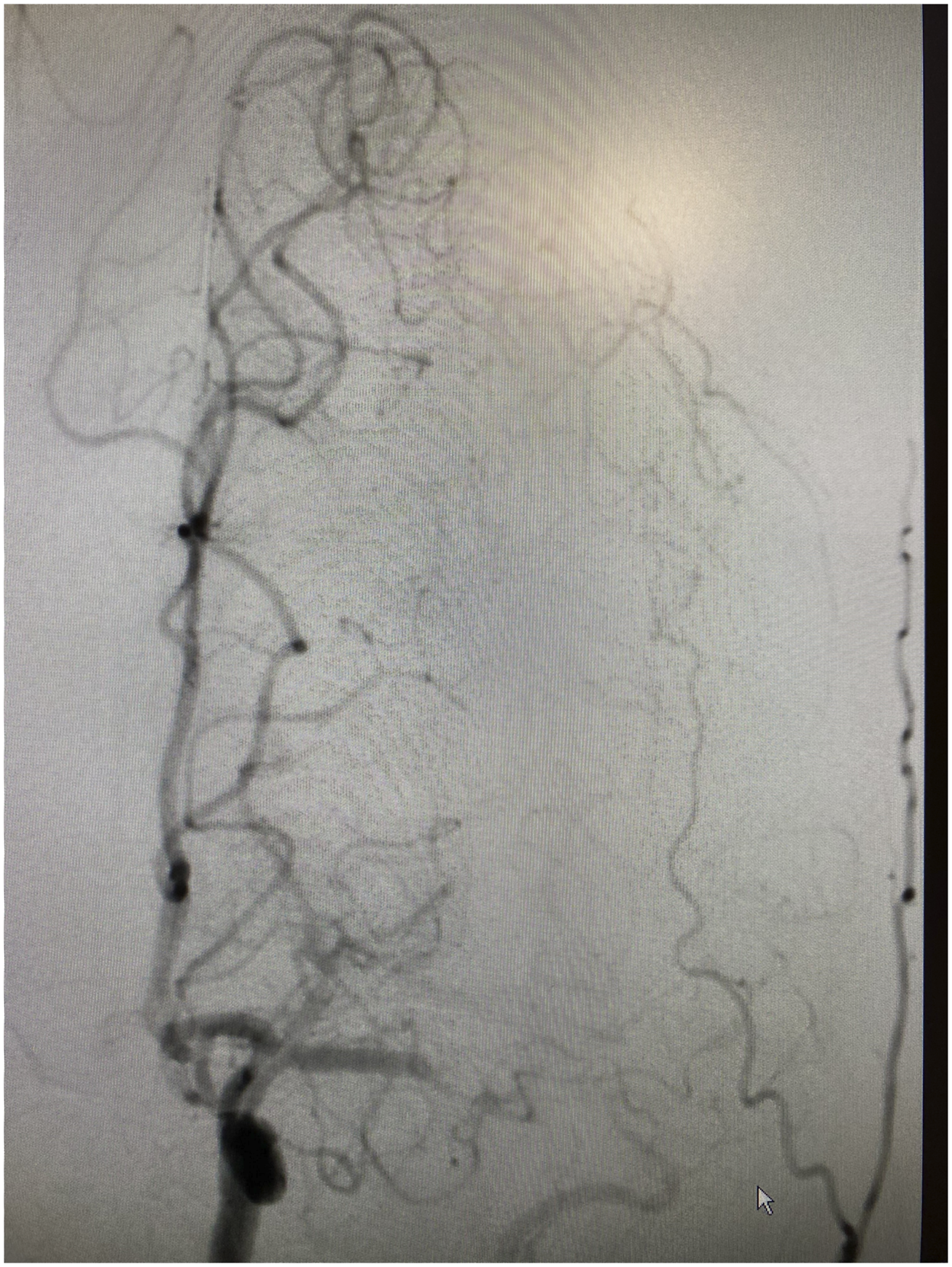
The patient was subsequently admitted to the neurological intensive care unit for further work up. Her stroke work up included a transthoracic echocardiogram (TTE) which revealed ejection fraction of 55-60%. The right ventricular size is moderately dilated. There was noted to be in echogenicity in the right atrium that was appreciable on multiple views. There was concern that this reflected thrombus in the setting of pulmonary embolism. The thrombus measured 3 cm in length. There was a bubble study that was also positive suggesting a right-to-left interatrial shunting. The off axis apical views suggested that the thrombus could be straddling a potential patent foramen ovale (PFO) or interatrial septum. Therefore, an urgent transesophageal echocardiogram (TEE) was performed. This revealed a large complex and mobile thrombus noted in the right atrium. It appeared attached along the eustachian valve and measured least 3 cm with highly mobile distal tip suggesting high risk for embolization. There was a tunneled PFO also noted. There is no thrombus at that time straddling the PFO but the right atrium clot had a mobile component in the vicinity of the tunnel. A structural heart specialist then performed an emergent trans catheter removal and debulking of the intracardiac thombus with an Angiovac aspiration system Figure 3.
3
This included an intracardiac echocardiogram, inferior vena cava (IVC) venogram, and IVC filter placement using a 30 mm Cook IVC filter in the infrarenal position. Unfractionated heparin drip was started at the conclusion of this procedure which was approximately 12 hours from her mechanical thrombectomy. She had a tissue culture that was obtained from the mass which did not reveal any organisms. The patient subsequently returned to the neurological ICU in stable condition. Atrial thrombus and echocardiogram.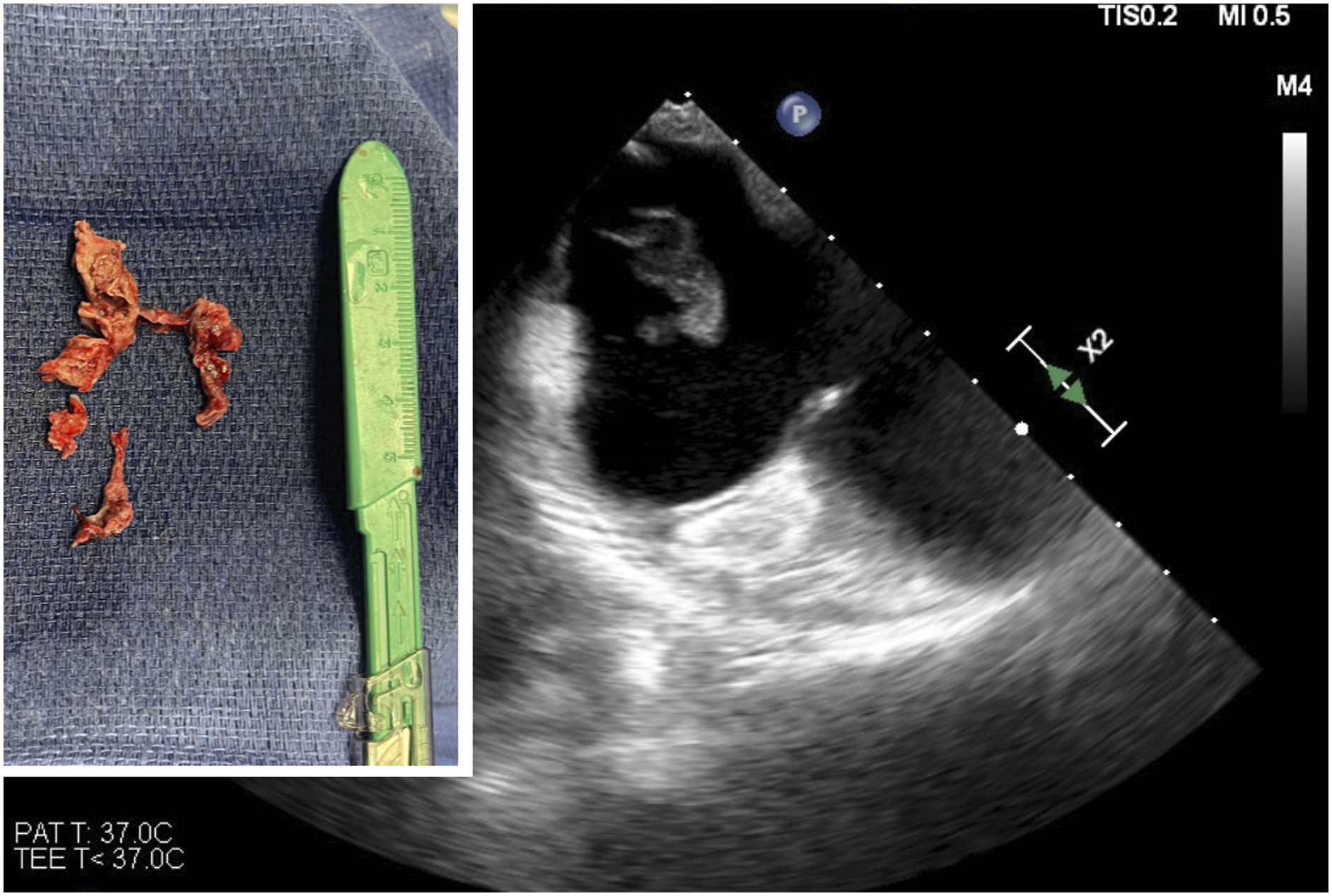
She had confirmatory testing showing a popliteal deep vein thrombosis (DVT) and peroneal DVT both of undetermined age. The patient was initiated on heparin drip with bridge to apixaban on her second day of admission after MRI showing minimal stroke burden involving left insula and frontal operculum Figure 4. Vascular medicine was consulted and performed hypercoagulable testing. This included anticardiolipin AB IgA, IgM, IgG at <2.0, <1.5, <1.6 and beta-2 glycoprotein antibodies Beta – 2 gp1IgA, Beta – 2 gp1IgM, Beta – 2 gp1IgG at <2.0, <1.5, 2.8, both of which were within normal limits. Dilute Russell Viper Venom Test (DRVVT) was negative for lupus anticoagulant. She had lipid profile that revealed a total cholesterol of 202, low-density lipoprotein (LDL) of 144, and high-density lipoprotein (HDL) of 29. Her hemoglobin A1C was 5.6. She also had a negative pregnancy test. There were no diagnostic challenges. DWI sequence of MRI brain with infarct in left insula and frontal operculum.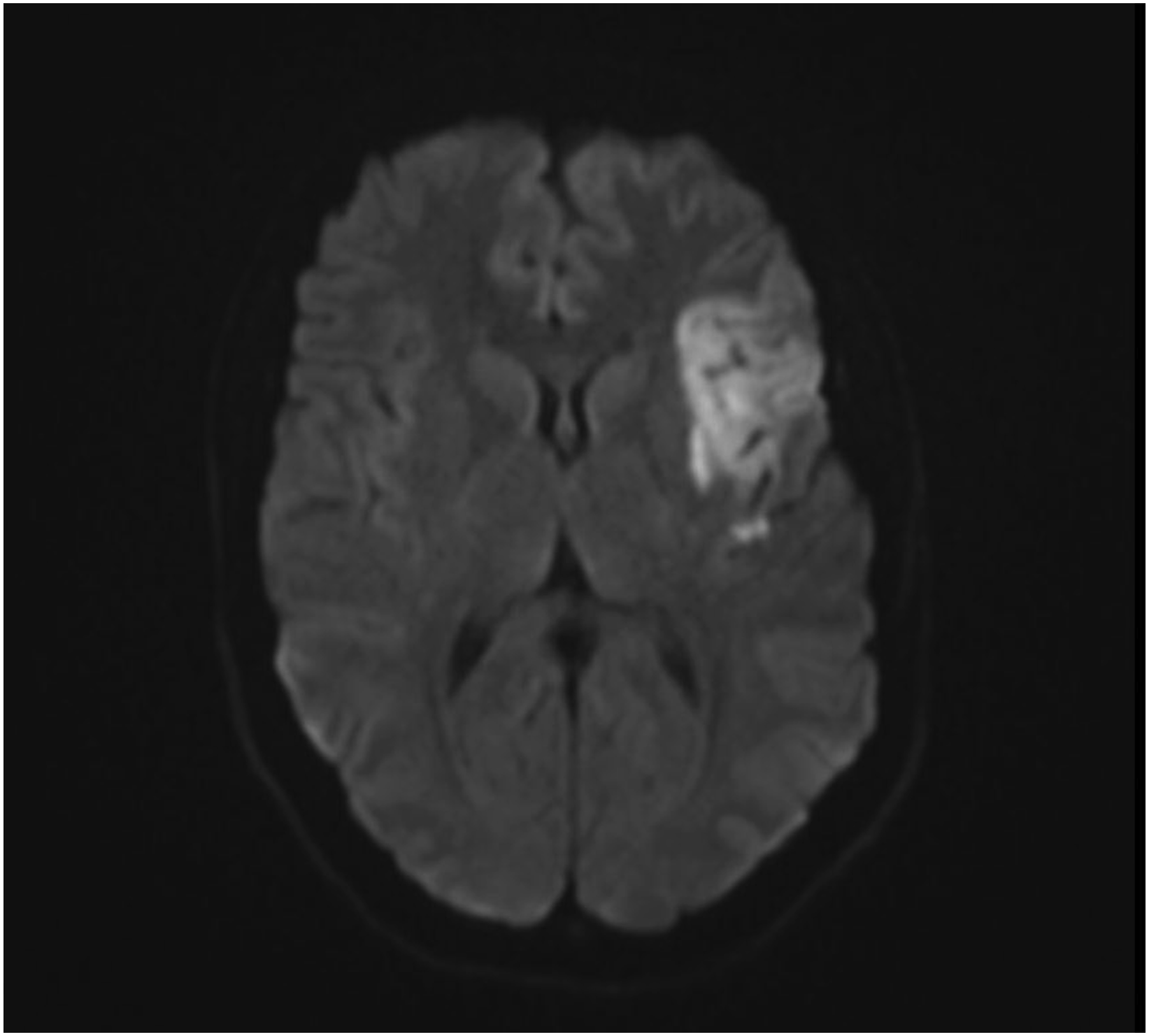
The patient was ultimately evaluated by physical, occupational and speech therapy. Physical and occupational therapy recommended safe transition home with intermittent care giver support for higher level activities of daily living (ADL) needs. Speech therapy evaluated patient’s swallow function and she was recommended for a regular texture diet with thin liquids. At the time of discharge, patient’s speech had returned to baseline without noticeable deficits. Patient was discharged with an NIHSS of 0. Her modified Rankin scale (mRS) was graded as a 1. 4
Her etiology of stroke was thought to be secondary to a paradoxical embolus from DVT/PE through her patent foramen ovale. She will continue outpatient hypercoagulable work up including testing for MTHFR gene, Factor V Leiden, Protein C/S deficiency, Antithrombin III, and Prothrombin gene mutation after at least 3 months of anticoagulation. She was discharged on anticoagulation with apixaban 5mg twice a day with short term follow-up. Follow-up with structural heart clinic was planned to decide on need for PFO closure. She was also taken off her birth control medication regimen going forward as this has been linked to thromboembolic events. 5 There were no adverse or unanticipated events (Figures 1 and 2).
This is an unusual case of a young patient with minimal medical history who presented with a large PE and L MCA occlusion. The strengths of this case include the description of cutting edge techniques to treat thromboembolic events and the overall great clinical outcome described. Weaknesses include lack of a clear etiology of the patient’s initial thrombus as her continued anticoagulation precludes her immediate hypercoagulable testing.6-8
Due to prompt recognition of her neurological symptoms and short interval between her symptom onset and treatment, this patient made a near full recovery. A full stroke work-up revealed a highly mobile intra-cardiac thrombus that was also swiftly removed. Right atrial thrombi are associated with high mortality and there is a lack of consensus on the optimal treatment strategy with anticoagulation, surgical embolectomy, and thrombolysis all being effective.9-12 In this case, all 3 approaches were used (Figures 3 and 4).
This case highlights the need for an efficient in-hospital workflow and multidisciplinary approach in order to achieve optimal outcomes and work-up for our patients. Furthermore, identifying stroke etiologies, especially in young, healthy patients is important to prevent future catastrophic events. Close follow-up for stroke patients remains essential.
Patient Perspectives
“I came into the hospital because of extreme shortness of breath. I remember being in the emergency room and doing a CT scan, after that happened, I don't remember a lot. I don't recall having the stroke. Most of the day on my second day I do not remember until after they took the clots out of my heart. That evening I remember being more with it and started to understand what had happened to me, I slept a lot that night. Now I am back to normal except for my right leg which I have begun to bear weight on.”
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.