
Abstract
Background
Noninsertional Achilles tendinopathy affects both athletes and sedentary individuals, and its incidence is rising. Conservative management is the mainstay of treatment, but a variety of operative techniques have been described to treat recalcitrant cases. We seek to outline the current available evidence for surgical management of noninsertional Achilles tendinopathy.
Study design and methods
A systematic review was performed using the MEDLINE and EMBASE databases, and all articles were reviewed by at least 2 authors. Each article was assigned a level of evidence in accordance with the standards of Journal of Bone and Joint Surgery. The available data were reviewed and a level of evidence was assigned to each intervention of interest, based on the revised classifications of Wright.
Results and conclusion
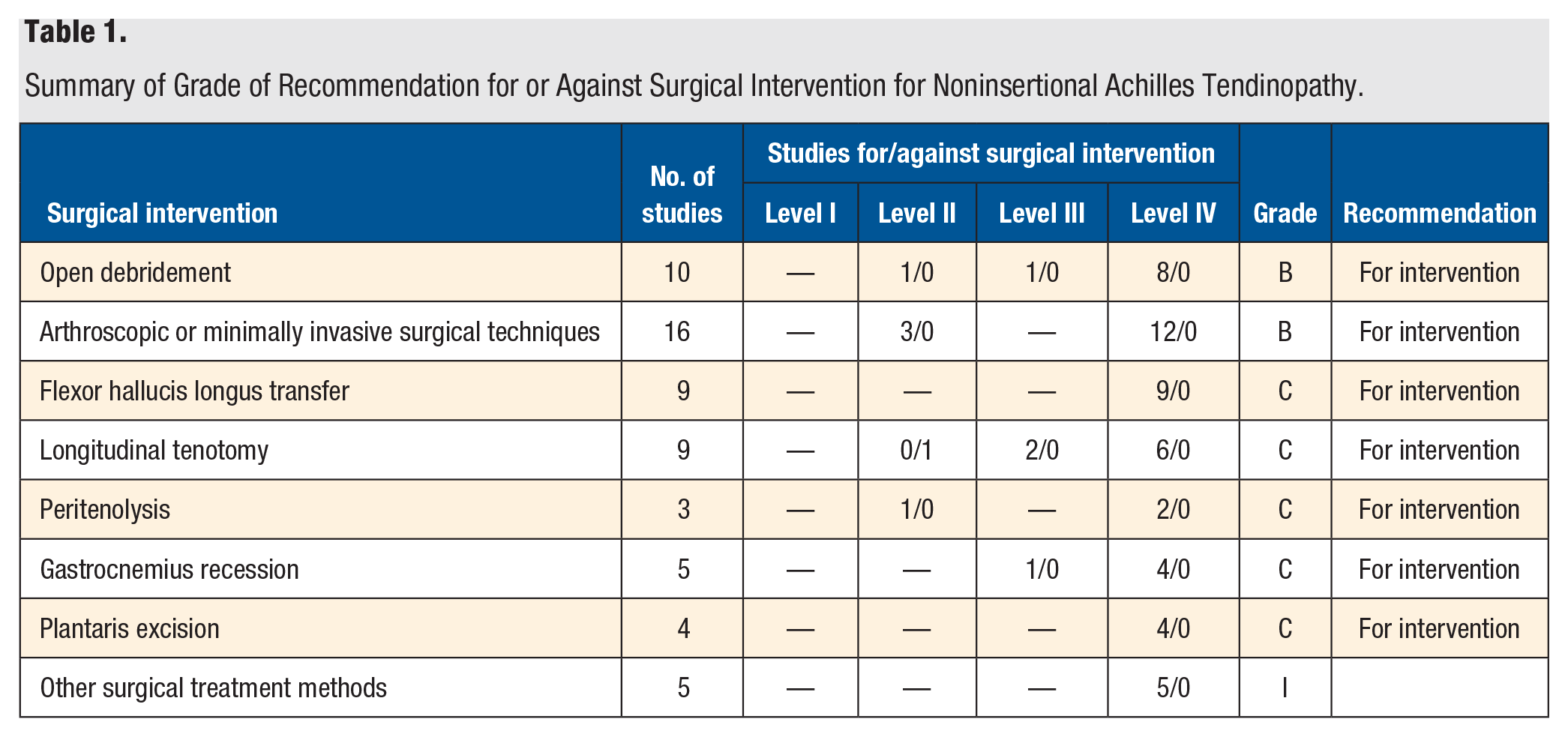
A total of 46 articles met inclusion and exclusion criteria. There is fair evidence (grade B) in support of open debridement with 1 level II study, 1 level III study, and 8 level IV studies. There is fair evidence (grade B) in support of arthroscopic or minimally invasive surgical techniques. There is poor evidence (grade C) in support of flexor hallucis longus transfer, longitudinal tenotomy, peritenolysis, gastrocnemius recession, and plantaris excision. There is insufficient evidence (grade I) to provide a recommendation about other surgical treatment methods for noninsertional Achilles tendinopathy.
“Histopathological studies have found that tendinopathy is a result of a failed healing response, which may cause degenerative changes in the tendon.”
Introduction
Achilles tendinopathy commonly affects competitive and recreational athletes as well as sedentary individuals.1,2 Approximately 2.35 out of every 1000 adults aged 21 to 60 years suffer from pain in the midportion of the Achilles tendon. 2 Aging, overuse, obesity, and medical comorbidities such as diabetes may result in tendon degeneration. The incidence of Achilles tendinopathy is rising as people endure significant strain to the ankle as a result of an increase in participation in recreational and competitive sports and in the duration and intensity of training regimens.3-5
The hallmarks of Achilles tendinopathy are damaged, weak, and inelastic tendon tissue, presenting as pain, swelling, and impaired physical function of the Achilles tendon. Histopathological studies have found that tendinopathy is a result of a failed healing response, which may cause degenerative changes in the tendon.6-8 Achilles tendinopathy can be described as insertional or noninsertional: the insertional form is situated at the calcaneus-Achilles tendon junction, whereas the noninsertional form is located at the level of the tendon body (2-6 cm proximal to the insertion of the Achilles tendon into the calcaneus). 6
Common conservative treatments include activity modification, physical therapy, and nonsteroidal anti-inflammatory medications. When conservative treatment fails, surgical options may be pursued. The aim of this article is to provide an evidence-based literature review and assessment of the quality of evidence regarding operative interventions for chronic noninsertional Achilles tendinopathy.
Materials and Methods
A comprehensive literature review was conducted in July 2019 (Figure 1). A search of the Ovid MEDLINE and EMBASE databases was done using terms to identify operative interventions (surgery, surgical, operative, tendon debridement, flexor hallucis longus [FHL] transfer, gastrocnemius recession) for Achilles tendinopathy (Achilles, tendinopathy, tendinosis, tendonitis, paratendonitis, tenosynovitis). Search results were reviewed independently by at least 2 authors (MP, KW, CD), all of whom were junior orthopaedic surgery residents in their first 3 years of residency; discrepancies between the 2 authors were addressed by a third, independent author (AV) who is a staff orthopaedic surgeon.
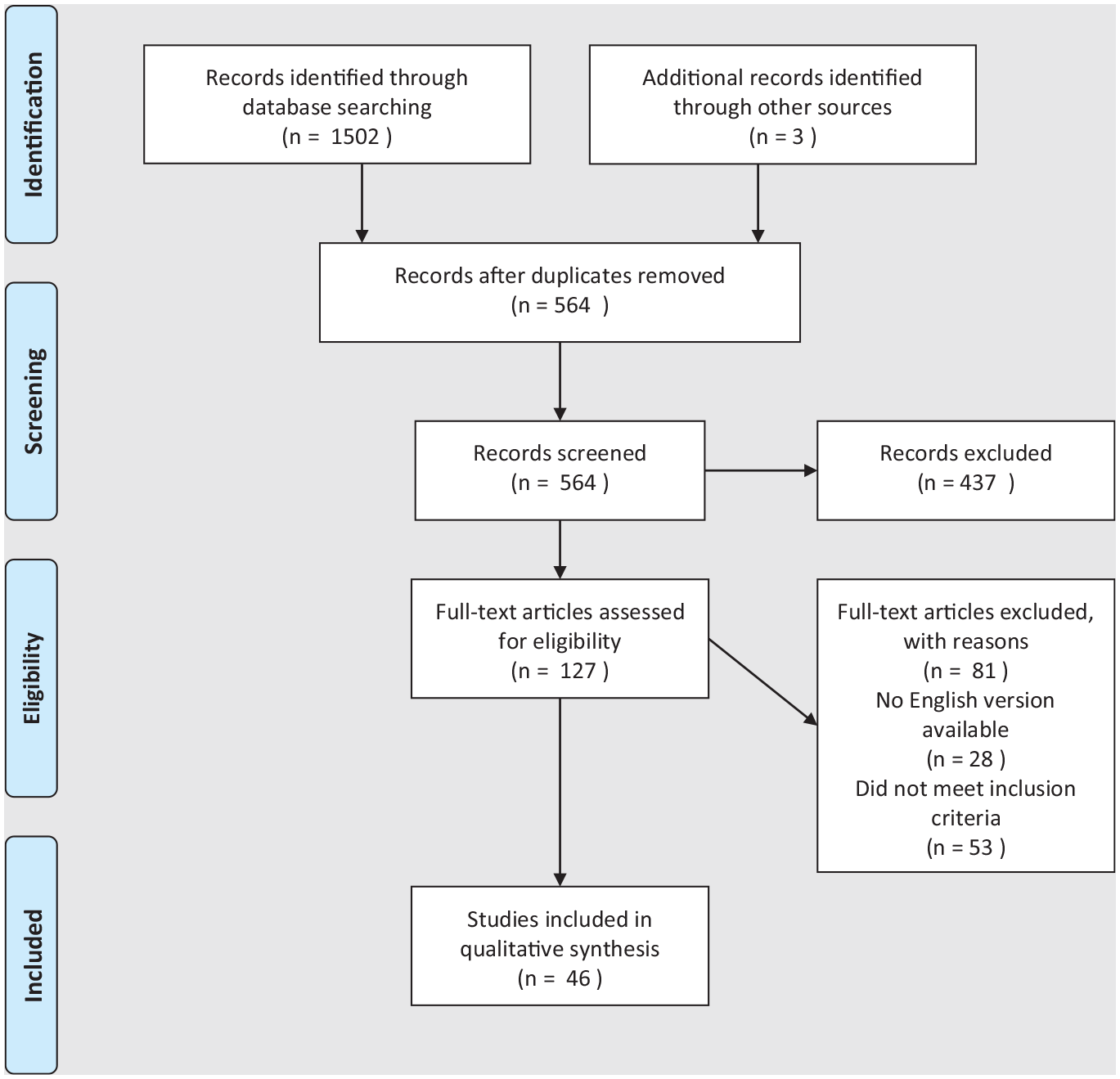
PRISMA flow diagram: The diagram illustrates the search process for the published literature meeting the inclusion criteria for this study. 40
Randomized controlled trials (RCTs), retrospective studies, and prospective studies were analyzed if they met the following inclusion criteria: (1) noninsertional or midportional Achilles tendinopathy and (2) treated by surgical means. Surgical treatments were defined as the following procedures: gastrocnemius recession (Vulpuis, Strayer, Bauman, Hoke, Silfverskiold), Achilles tendoscopy, Achilles debridement, vertical tenotomies, tendon transfer (FHL, flexor digitorum longus [FDL] or soleus), peritenolysis, and plantaris excision. Surgical treatments were grouped into open debridement, FHL tendon transfer, longitudinal tenotomy, peritenolysis, minimally invasive techniques, gastrocnemius recession, plantaris excision, and other. Surgeries were considered minimally invasive if the authors defined the surgery as such or if the surgery was described as being performed percutaneously.
Any articles that were not in English and that did not have an English translation available were excluded. Additional exclusion criteria consisted of studies describing acute ruptures, nonoperative procedures, and insertional Achilles tendinopathy.
Studies meeting inclusion criteria were assigned a level of evidence (I-IV) in accordance with the standards of Journal of Bone and Joint Surgery (Appendix A). 9 A grade of recommendation (A-C, I) was assigned to each intervention of interest based on the revised classifications of Wright (Appendix B). 10
Results
Initial search results produced 564 articles, after removing duplicates. Of those, 103 articles underwent a full-article review; 46 of these were found to meet all necessary inclusion and exclusion criteria. The grade of recommendation assigned to each intervention is summarized in Table 1. There is fair evidence (grade B) in support of open debridement (Tables 2 and 3) and arthroscopic and minimally invasive techniques (Tables 4 and 5). There is poor evidence (grade C) in support of FHL transfer (Table 6), longitudinal tenotomy (Tables 7 and 8), peritenolysis (Tables 9 and 10), gastrocnemius recession (Table 11), and plantaris excision (Table 12). There is insufficient evidence (grade I) to provide any recommendation regarding other surgical treatment methods for noninsertional Achilles tendinopathy (Table 13).
Summary of Grade of Recommendation for or Against Surgical Intervention for Noninsertional Achilles Tendinopathy.
Studies of Open Debridement: Levels I to III.
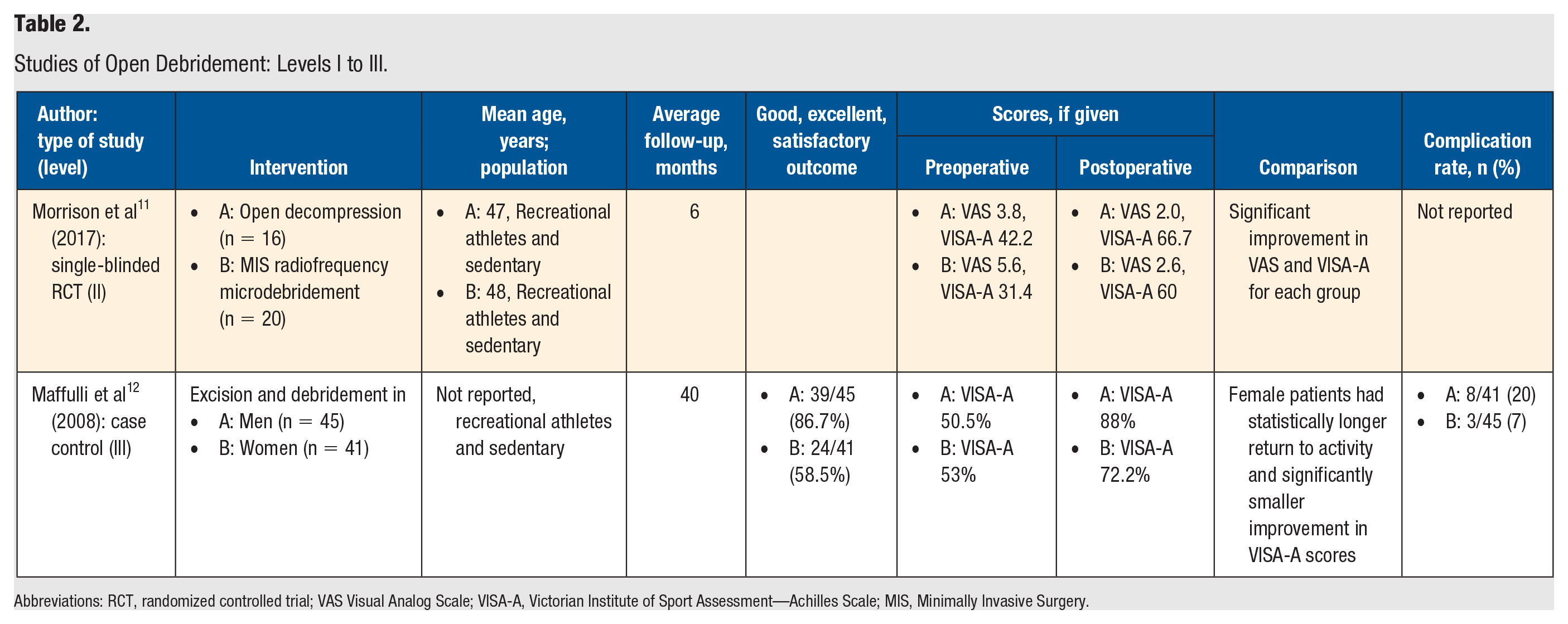
Abbreviations: RCT, randomized controlled trial; VAS Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment—Achilles Scale; MIS, Minimally Invasive Surgery.
Studies of Open Debridement: Level IV.
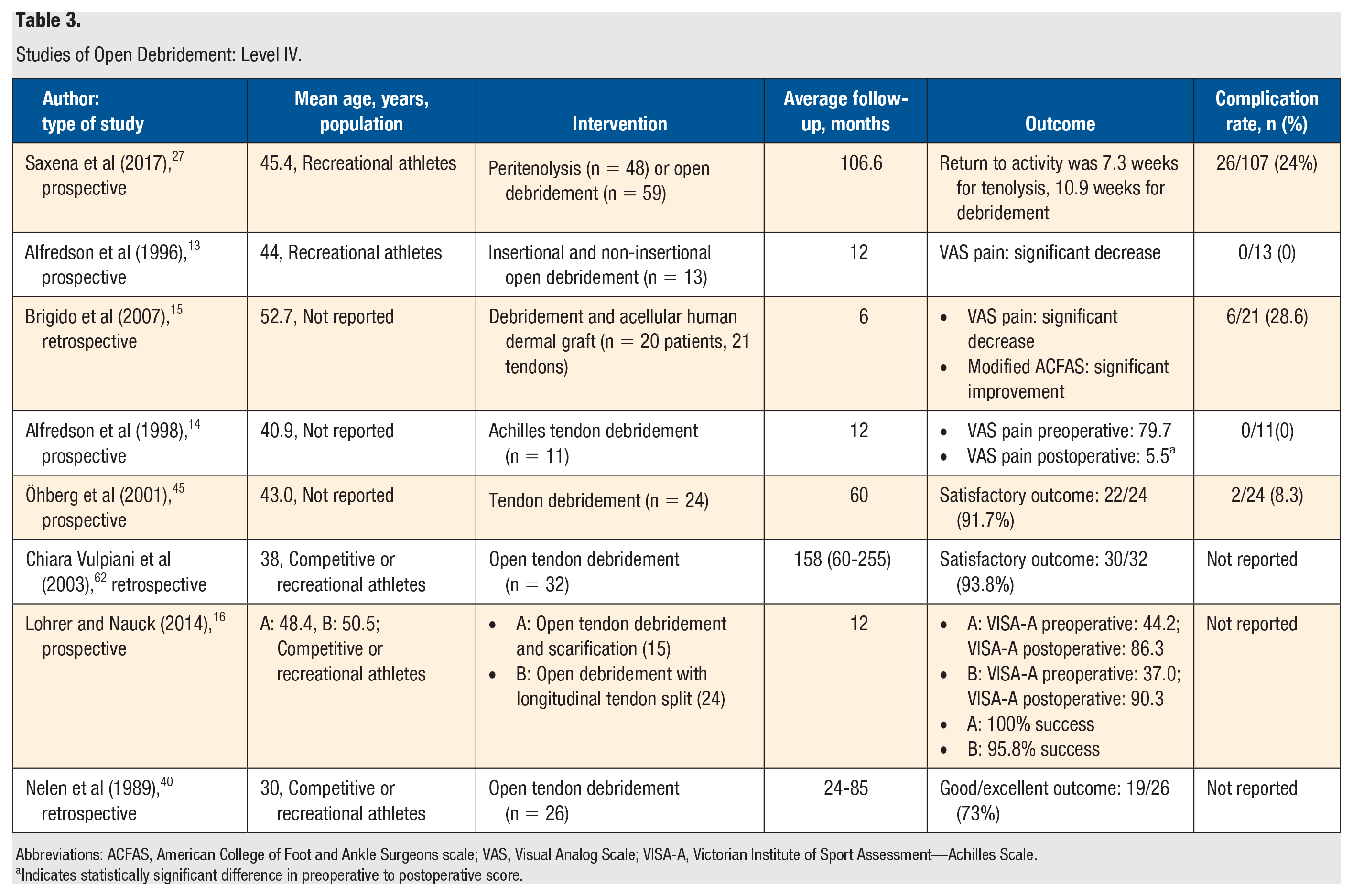
Abbreviations: ACFAS, American College of Foot and Ankle Surgeons scale; VAS, Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment—Achilles Scale.
Indicates statistically significant difference in preoperative to postoperative score.
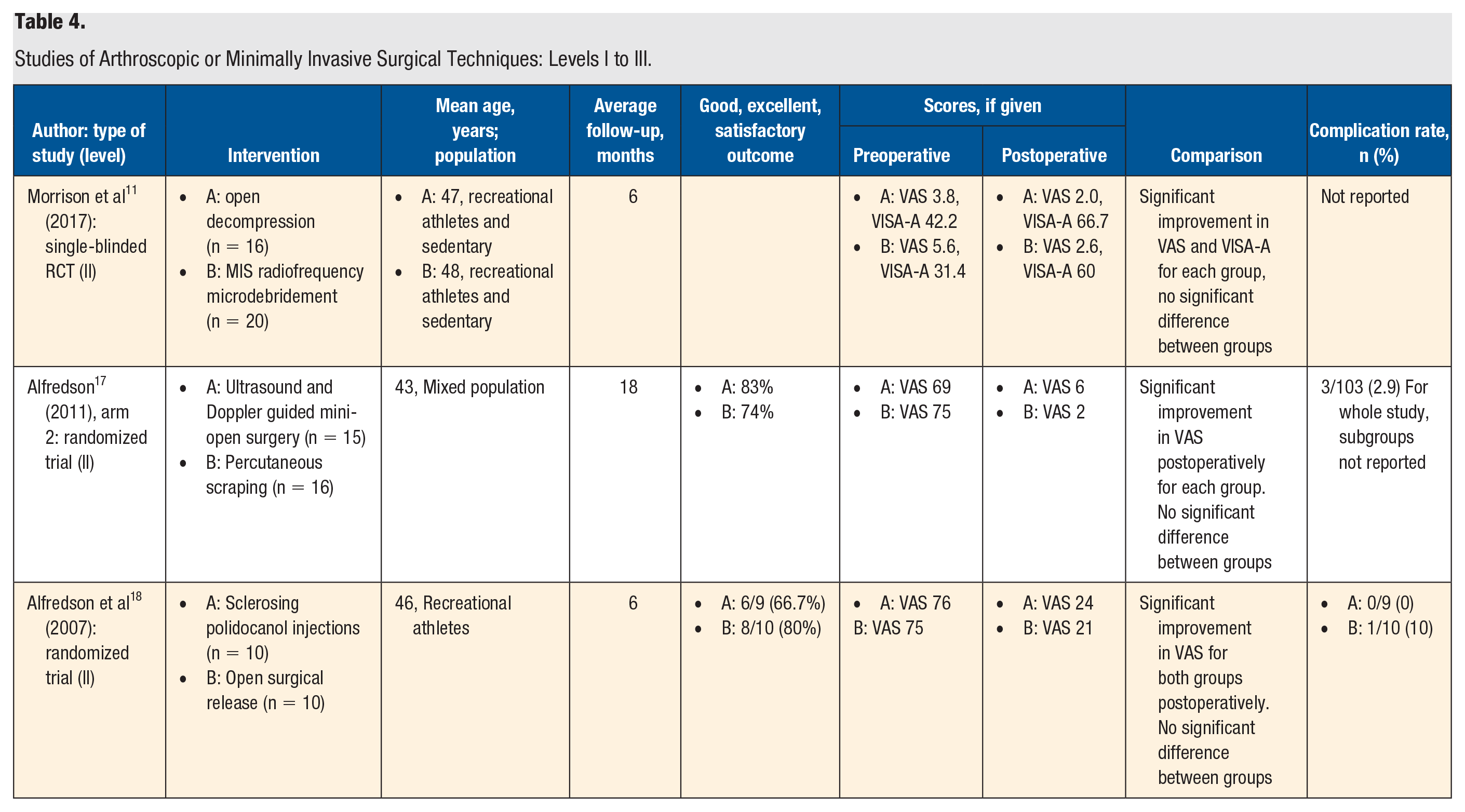
Studies of Arthroscopic or Minimally Invasive Surgical Techniques: Levels I to III.
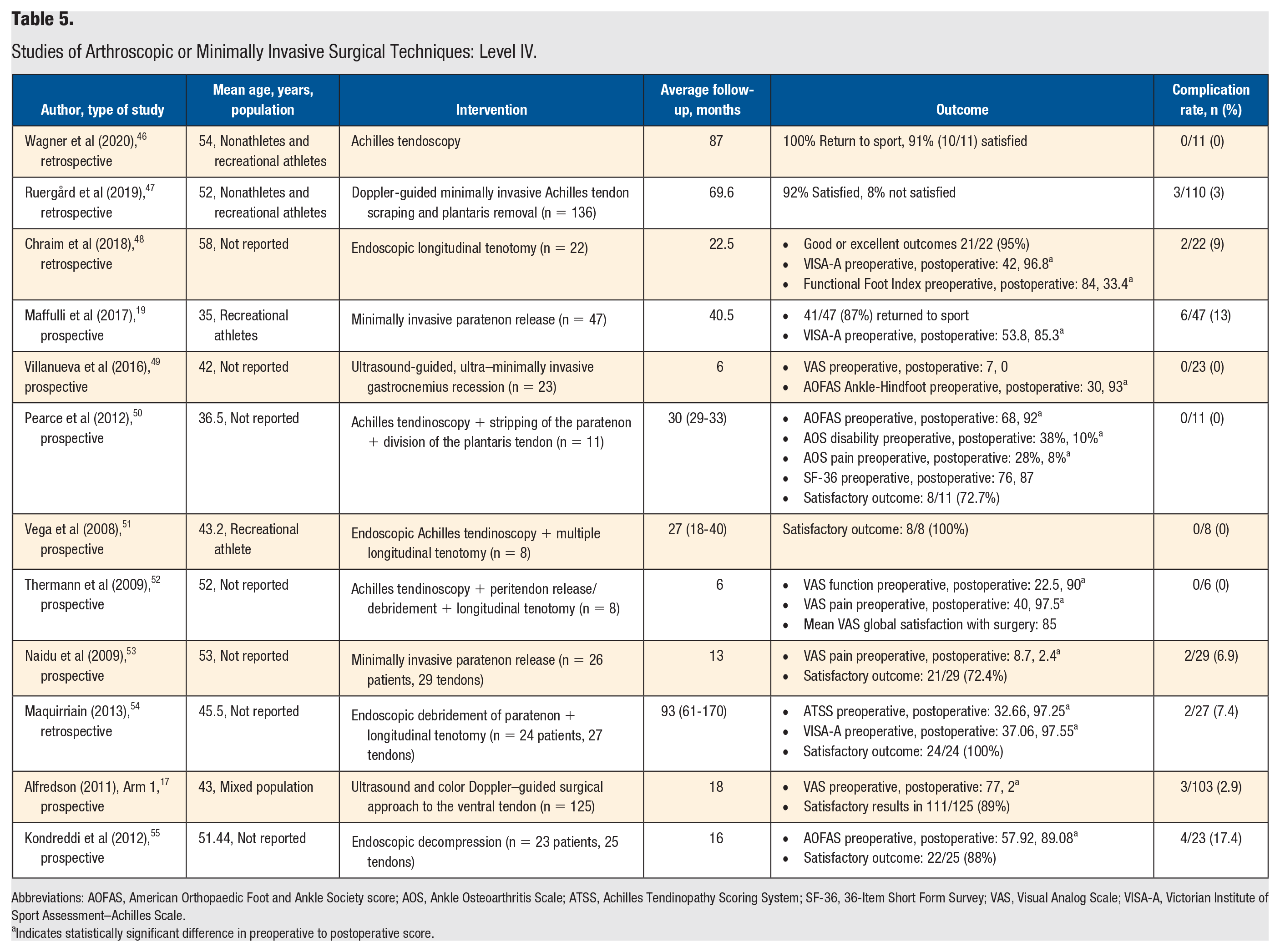
Studies of Arthroscopic or Minimally Invasive Surgical Techniques: Level IV.
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society score; AOS, Ankle Osteoarthritis Scale; ATSS, Achilles Tendinopathy Scoring System; SF-36, 36-Item Short Form Survey; VAS, Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment–Achilles Scale.
Indicates statistically significant difference in preoperative to postoperative score.
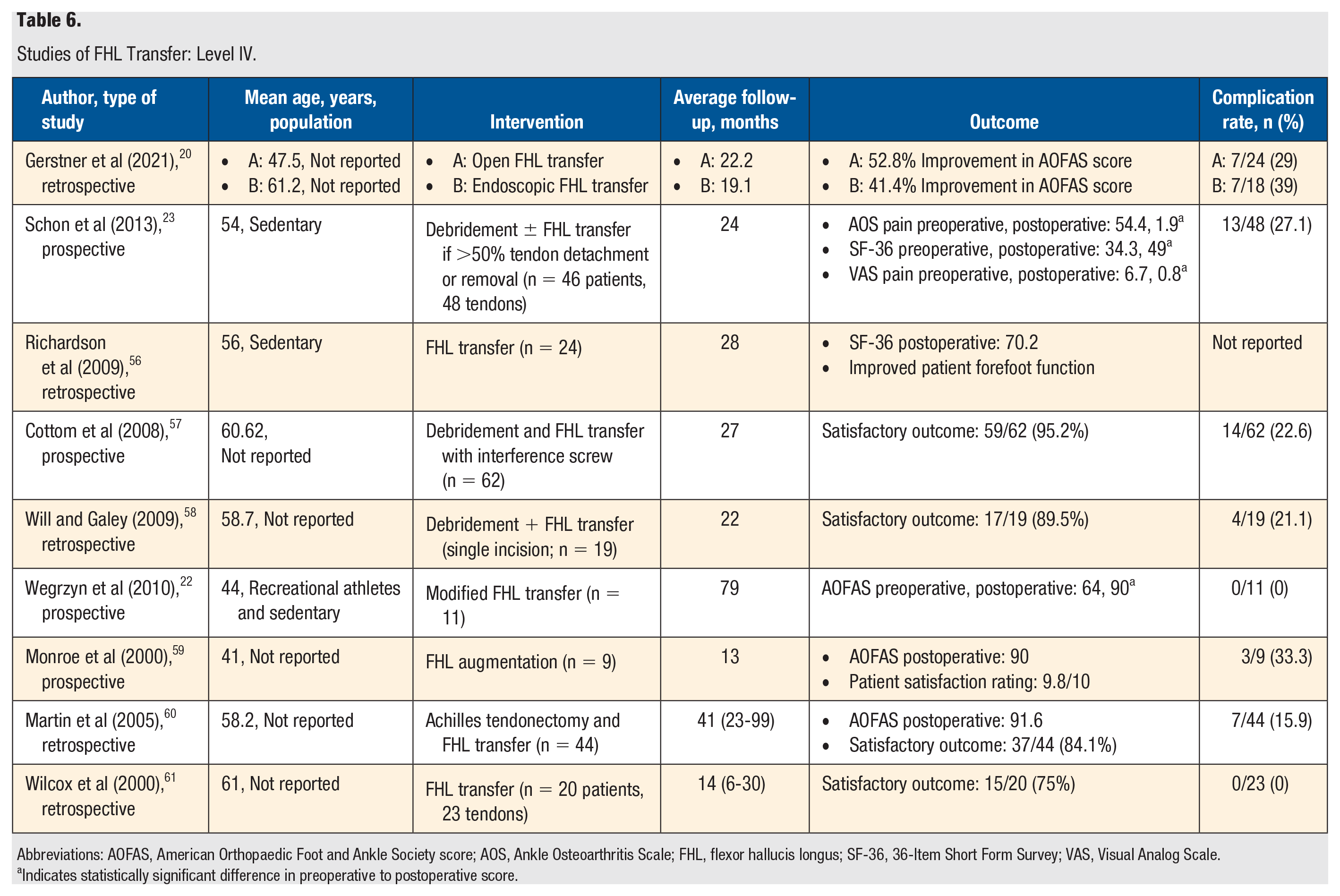
Studies of FHL Transfer: Level IV.
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society score; AOS, Ankle Osteoarthritis Scale; FHL, flexor hallucis longus; SF-36, 36-Item Short Form Survey; VAS, Visual Analog Scale.
Indicates statistically significant difference in preoperative to postoperative score.
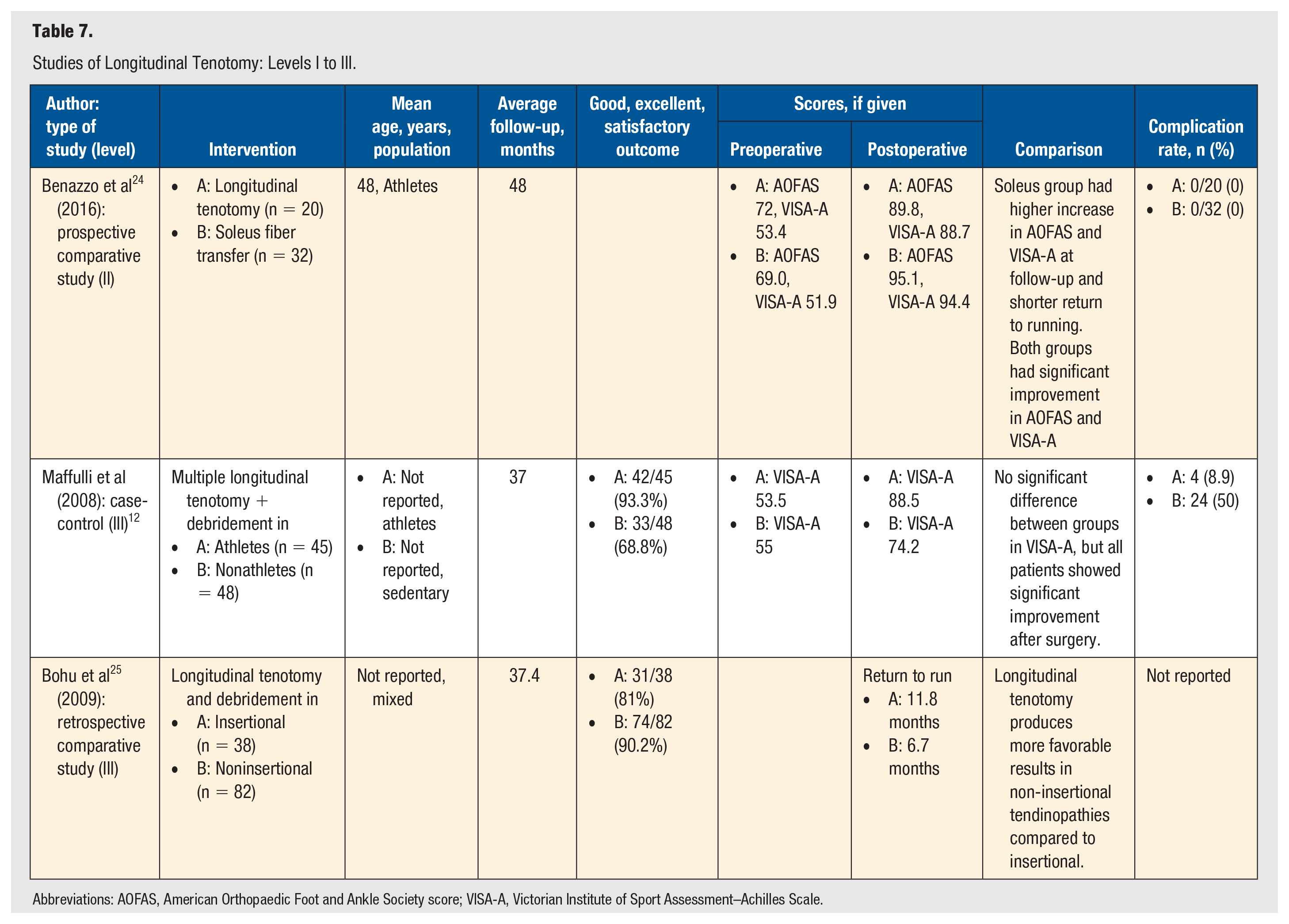
Studies of Longitudinal Tenotomy: Levels I to III.
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society score; VISA-A, Victorian Institute of Sport Assessment–Achilles Scale.
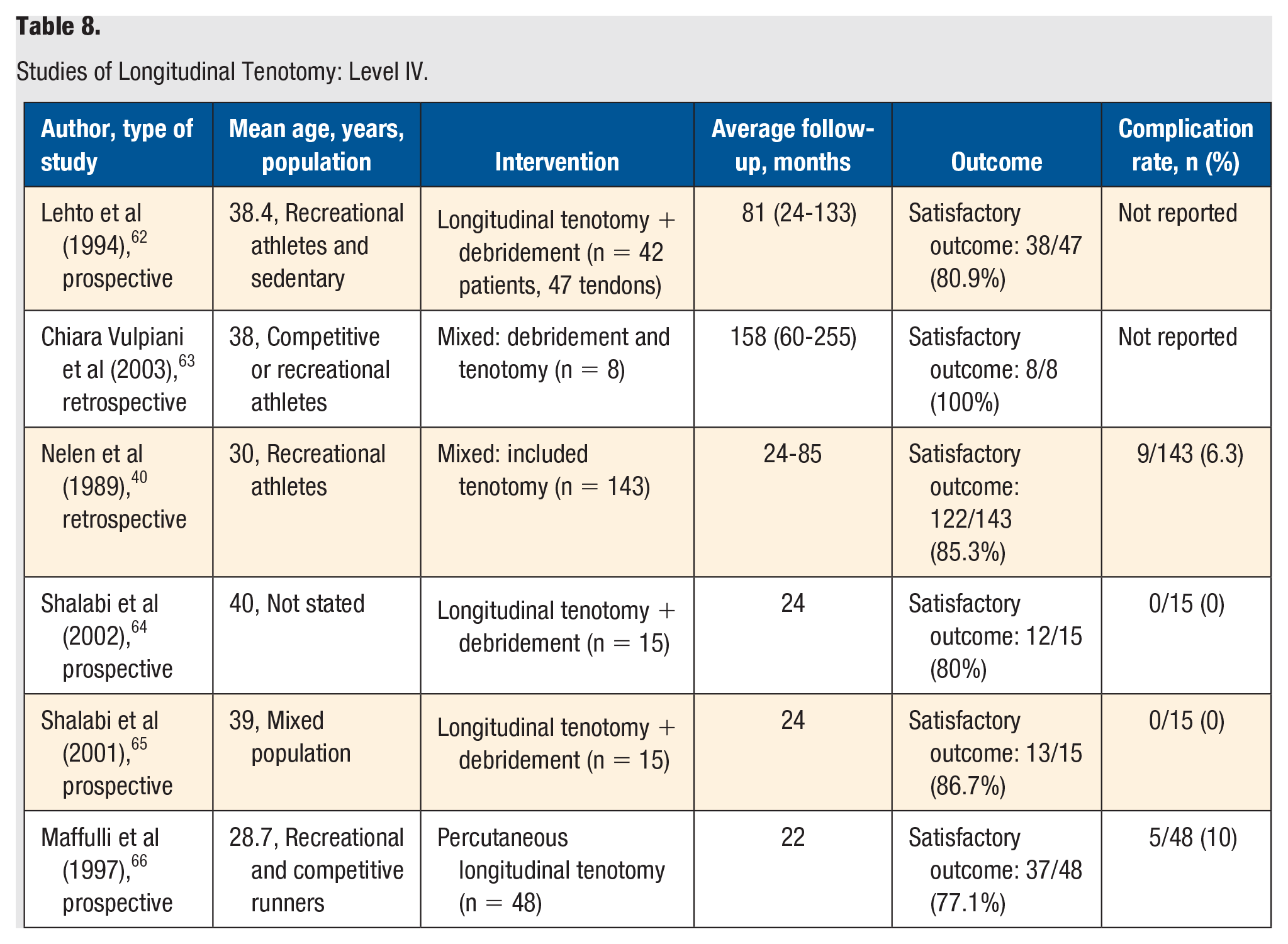
Studies of Longitudinal Tenotomy: Level IV.
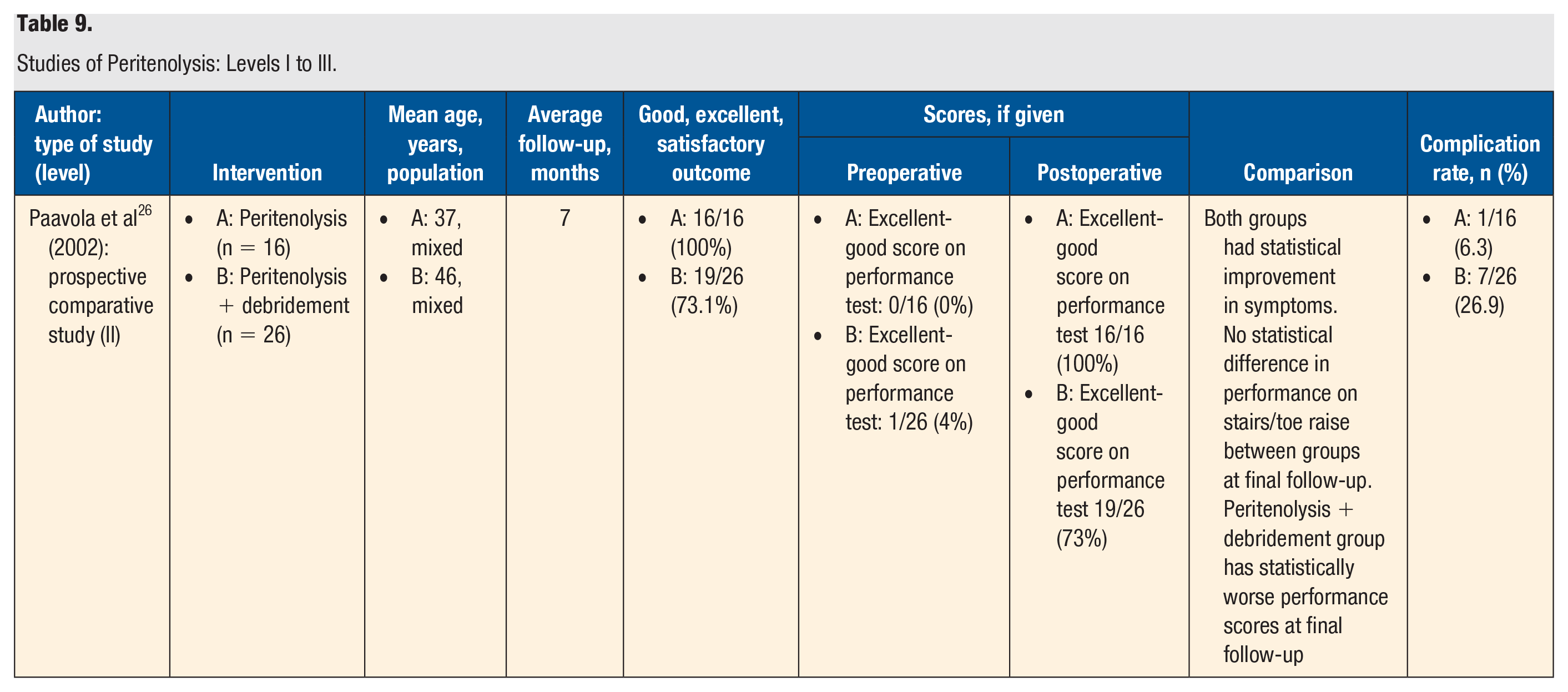
Studies of Peritenolysis: Levels I to III.
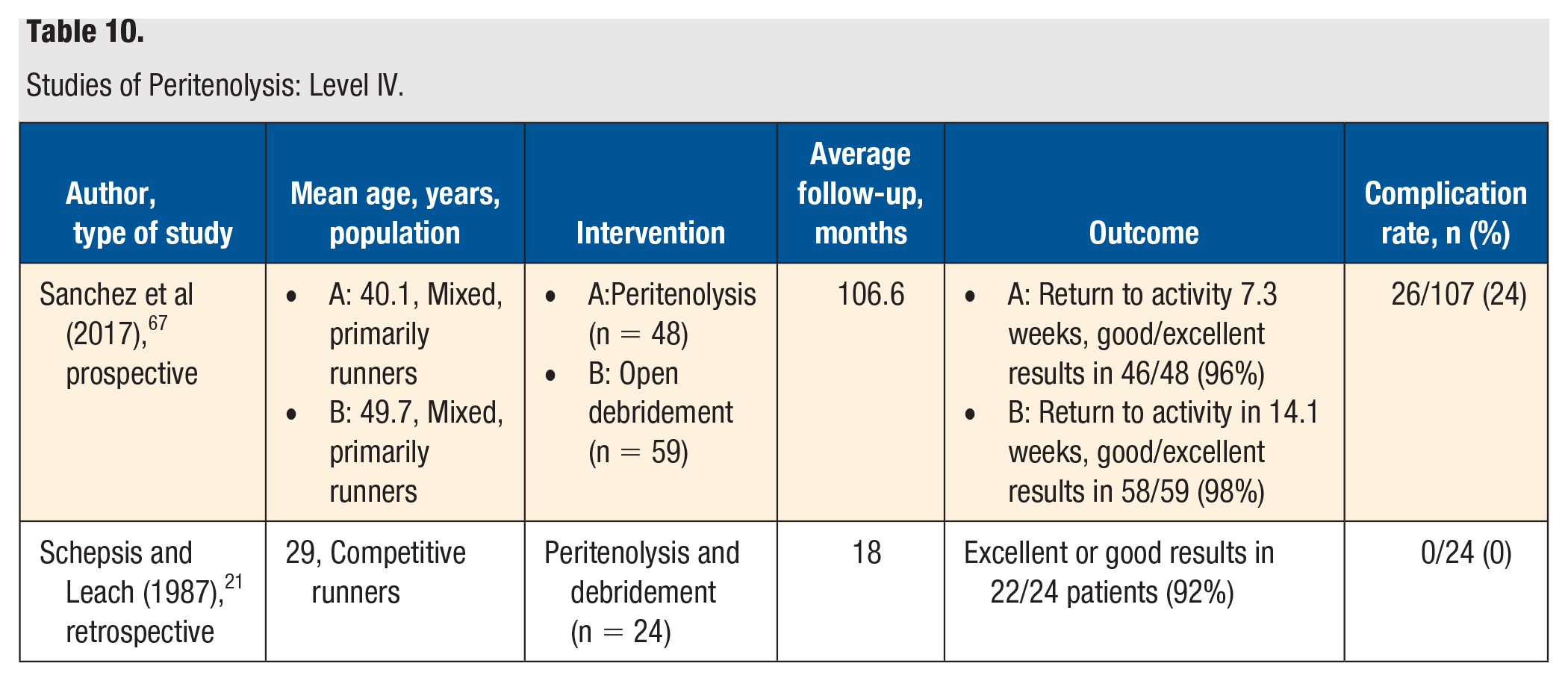
Studies of Peritenolysis: Level IV.
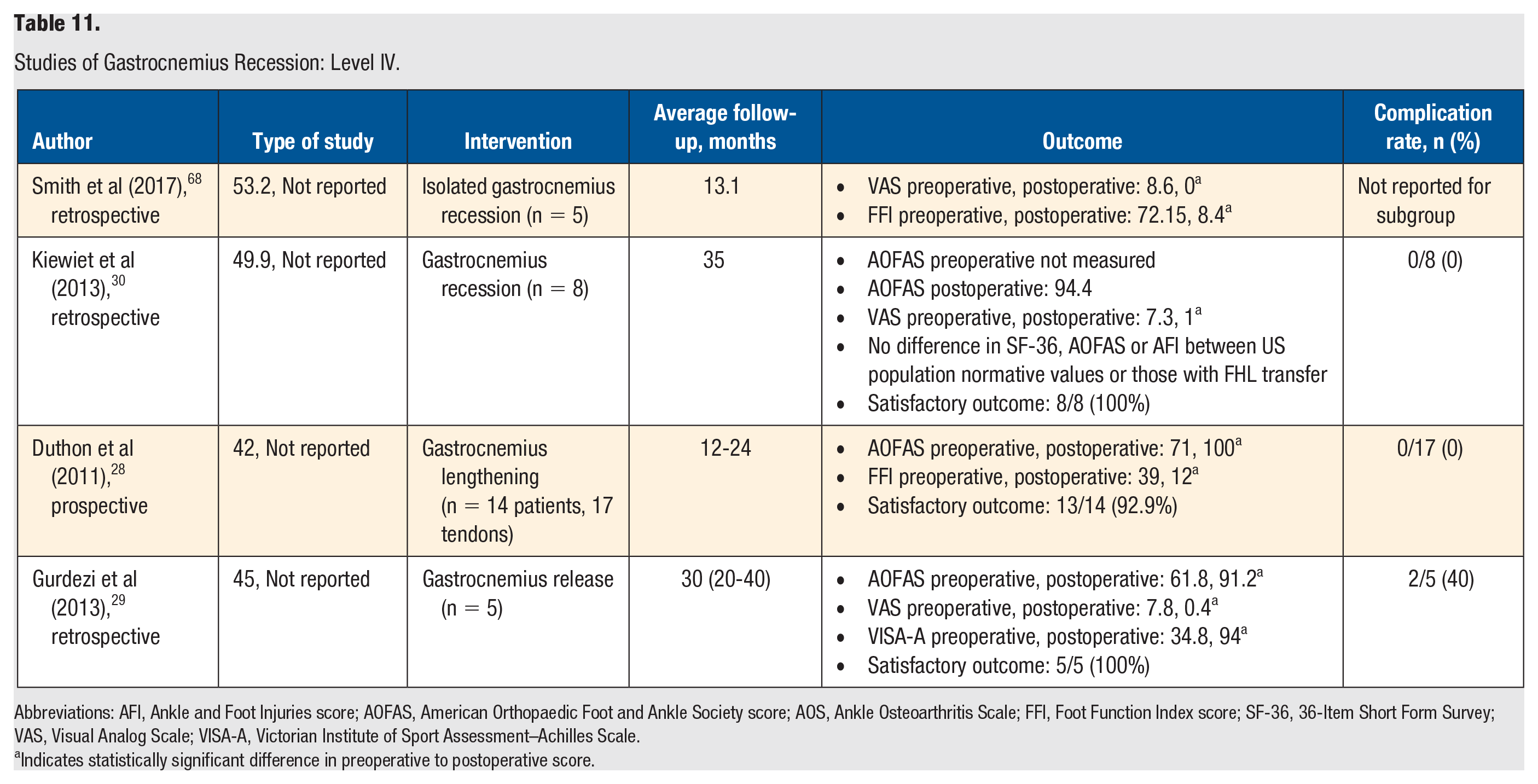
Studies of Gastrocnemius Recession: Level IV.
Abbreviations: AFI, Ankle and Foot Injuries score; AOFAS, American Orthopaedic Foot and Ankle Society score; AOS, Ankle Osteoarthritis Scale; FFI, Foot Function Index score; SF-36, 36-Item Short Form Survey; VAS, Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment–Achilles Scale.
Indicates statistically significant difference in preoperative to postoperative score.
Studies of Plantaris Excision: Level IV.
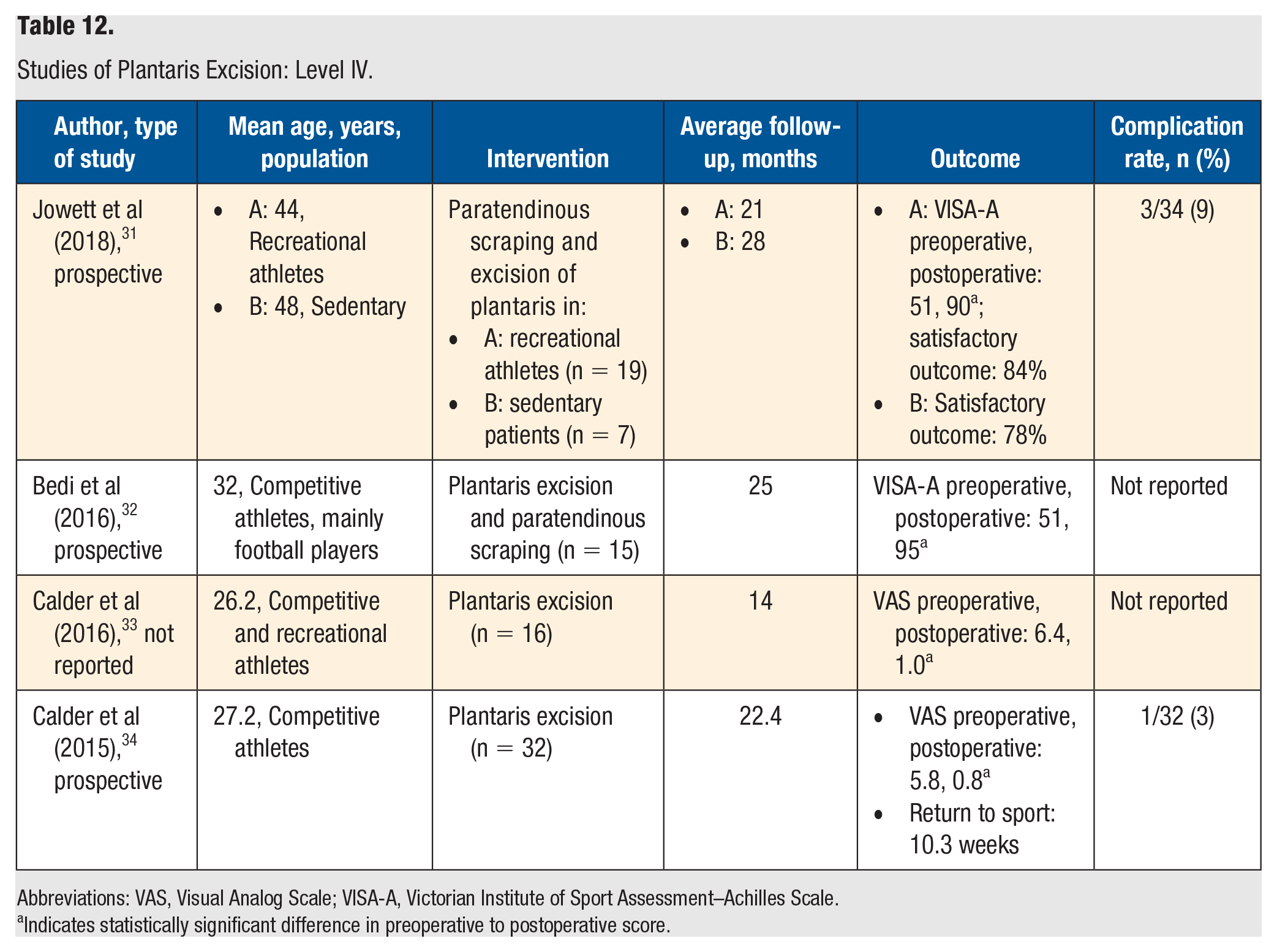
Abbreviations: VAS, Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment–Achilles Scale.
Indicates statistically significant difference in preoperative to postoperative score.
Studies of Other Surgical Treatment Methods: Level IV.
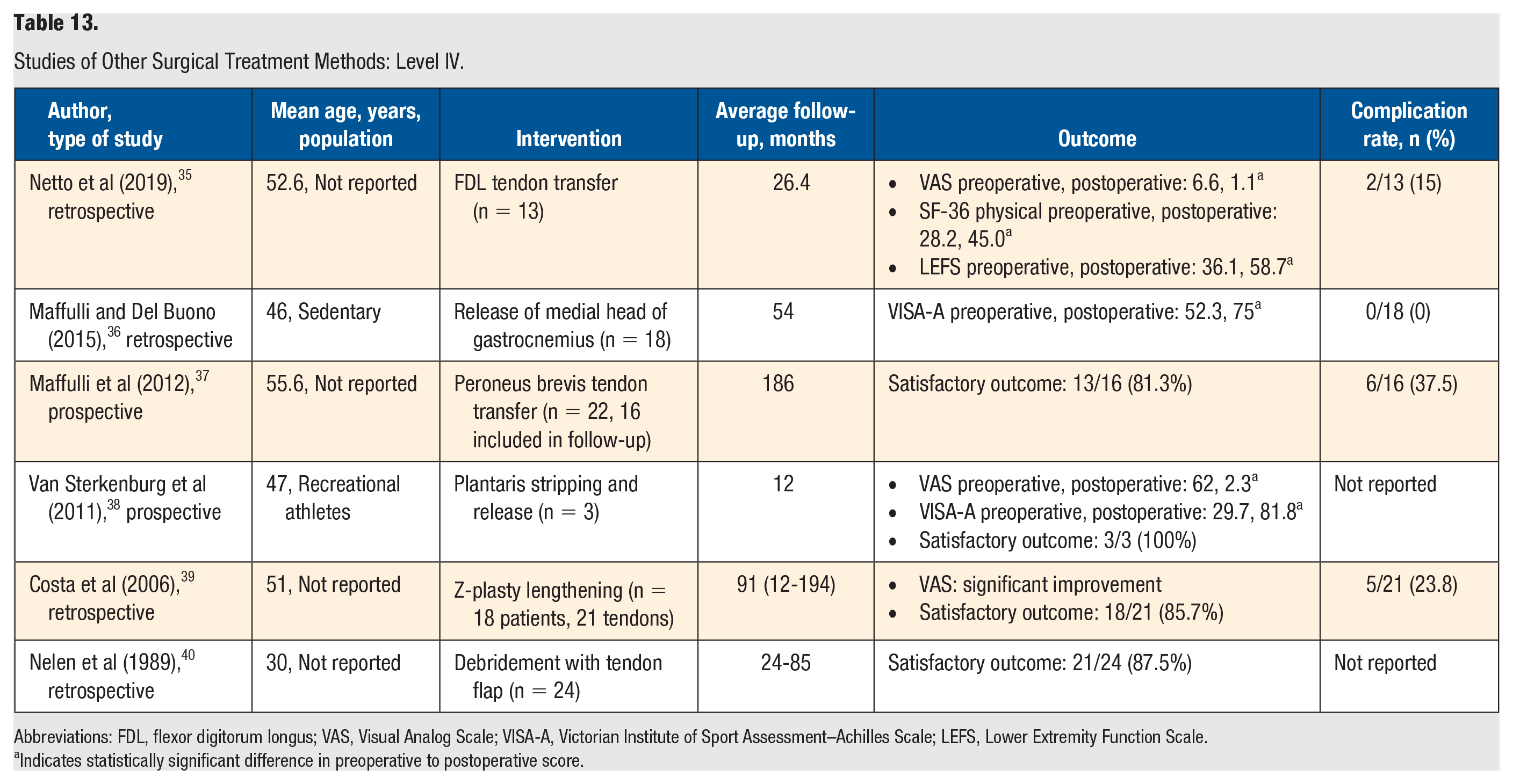
Abbreviations: FDL, flexor digitorum longus; VAS, Visual Analog Scale; VISA-A, Victorian Institute of Sport Assessment–Achilles Scale; LEFS, Lower Extremity Function Scale.
Indicates statistically significant difference in preoperative to postoperative score.
Open Debridement
Levels I to III
The highest-quality study examining the outcome of open debridement was 1 level II single-blinded RCT (Table 2). Morrison et al 11 produced an RCT where patients received either radiofrequency microdebridement or traditional surgical decompression. The mean age in the surgical decompression group was 47 years, whereas the mean age in the radiofrequency group was 48 years. No high-level athletes were enrolled in the study. Both the microdebridement (n = 20) and open (n = 16) groups had a statistically significant improvement in VAS and VISA-A scores; however, no difference was found between treatment modalities at 6 months.
In a case-control, level III study, Maffulli et al 12 investigated excision and debridement in age-matched men (n = 45) and women (n = 41). Both recreational athletes and sedentary individuals were included. The male cohort had significantly fewer complications, higher proportion of satisfied patients, and more marked improvement in VISA-A scores than the female cohort. Both cohorts had improved VISA-A scores postoperatively.
Levels IV and V
There were 8 level IV studies identified that reviewed open debridement (Table 3). The majority of the studies had a population of recreational or competitive athletes with a mean age in the 40s. The rates of a satisfactory treatment outcome ranged from 73.1% (19/26) to 100% (37/37). Furthermore, 4 of the studies reported a statistically significant improvement in their measuring scales for pain, function, and activity level.13-16 Visual Analog Scale (VAS) pain scores decreased significantly following treatment in these 3 studies. Moreover, in one of these studies, the modified American College of Foot and Ankle Surgeons scores showed significant improvement following treatment, though the complication rate in this study was high (28.6%) because of inclusion of minor complications in the total rate. 15 Complications included deep-venous thrombosis (1%), superficial infection (4%), suture reactions (13%), and hypertrophic scarring (8%).
Grade of Recommendation
Based on the previously mentioned literature, the operative procedure of open debridement is assigned a grade B recommendation (fair evidence, level II or III studies with consistent findings), supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. Open debridement procedures were shown to provide promising results overall in terms of patient satisfaction, pain level, and/or tendon functionality.
Arthroscopic or Minimally Invasive Surgical Techniques
Levels I to III
There were 3 level II studies investigating arthroscopic or minimally invasive surgical techniques as treatment for chronic noninsertional Achilles tendinopathy (Table 4). Alfredson 17 conducted a randomized trial comparing ultrasound and Doppler-guided mini-open surgery (n = 15) with percutaneous scraping (n = 16). The average follow-up was 18 months. Both groups had a statistically significant improvement in VAS postoperatively, and there were no differences between groups at final follow up.
Morrison et al 11 produced an RCT where patients received either radiofrequency microdebridement or traditional surgical decompression in a mixed active, athletic and sedentary population. Both the microdebridement (n = 20) and open (n = 16) groups had a statistically significant improvement in VAS and VISA-A scores; however, no difference was found between treatment modalities at 6 months. The authors reported no significant differences in the results between open treatment and percutaneous treatment.
Alfredson et al 18 conducted a randomized trial comparing active patients treated with sclerosing polidocanol injections (n = 9) with open surgical revision of the area with vasculo/neural ingrowth on the ventral side of the Achilles tendon (n = 10). At the 6-month follow-up, 6 of 9 patients (66.7%) in the injection group and 8 of 10 patients in the release group (80%) were satisfied with the treatment and had a significantly reduced level of tendon pain. The injection group improved significantly from a preoperative VAS score of 76 to a postoperative score of 24 (P < .05); the release group also improved significantly from a preoperative VAS score of 75 to a postoperative score of 21 (P < .05). There were no statistically significant differences between the 2 groups.
Levels IV and V
There were 12 level IV studies identified that reviewed arthroscopic or minimally invasive surgical techniques (Table 5). Most studies (10 of 12) included a mixed or not reported population. The mean age of the participants was less than 40 years in 2 studies, in the 40s in 4 studies, and in the 50s in 6 studies. The rates of a good or excellent outcome ranged from a low of 72.4% (21/29) to 100% (24/24). A fairly low complication rate was noted as well, ranging from 0% (0/11) to 17.4% (4/23). Complications included superficial wound infections, deep venous thrombosis, hypertrophic scarring, delayed wound healing, and sural nerve injury. There were 5 instances of sural nerve palsies related to Minimally Invasive Surgery (MIS) Achilles tendon stripping out of 47 patients. 19 Most studies (10 of 12) also demonstrated statistically significant improvement in pain and/or function.
Grade of Recommendation
Based on the previously mentioned literature, arthroscopic or minimally invasive surgical techniques are assigned a grade B recommendation (fair evidence, level II or III studies with consistent findings), supporting them as an effective treatment for chronic noninsertional Achilles tendinopathy. Minimally invasive techniques were shown to provide promising results overall in terms of patient satisfaction, pain level, and/or tendon functionality, with minimal complications.
Flexor Hallucis Longus Transfer
Levels IV and V
There were 9 level IV studies identified that reviewed FHL transfer (Table 6). Only 3 studies reported the population studied; 2 of these included only sedentary patients, whereas the third included both recreational athletes and sedentary patients. The mean age of patients tended to be older in the studies of this treatment, with 3 in the 40s, 3 in the 50s, and 3 in the 60s. The rates of a satisfactory treatment outcome ranged from 75% (15/20) to 95.2% (59/62). However, a relatively high complication rate was reported in these studies, ranging from 0% (0/23) to 39% (7/18). Complications included delayed wound healing, hypertrophic or sensitive scars, deep vein thrombosis, superficial infection, and deep peroneal nerve palsy. All 9 studies showed either improvement in pain or tendon functionality or a good-to-excellent subjective patient outcome following treatment. Furthermore, 3 of the studies reported a statistically significant improvement in pain, function, and activity level.20-22 In the Schon et al 23 study, the VAS pain scores and the Ankle Osteoarthritis Scale pain scores decreased a statistically significant amount, and the 36-Item Short Form Survey scores increased a statistically significant amount following FHL transfer. However, a fairly high number of complications (27.1%) were reported. In this study, 2 patients had deep vein thrombosis, 6 had superficial infection or delayed wound healing, and 4 had scar pain. In Wegrzyn et al, 22 the American Orthopaedic Foot and Ankle Scores (AOFAS) increased a statistically significant amount following FHL transfer. The sample size of this study was small, but no major complications with regard to wound healing were noted.
Grade of Recommendation
Based on the previously mentioned literature, the operative procedure of FHL transfer is assigned a grade C recommendation (poor evidence, level IV or V studies with consistent findings) supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. It should be noted, however, that the FHL transfer procedure was shown to provide promising results overall in terms of patient satisfaction, pain level, and/or tendon functionality and may warrant a level II to III study in the future that would better define the outcome and evidence for such a surgical intervention.
Longitudinal Tenotomy
Levels I to III
One level II study and 2 level III studies investigated longitudinal tenotomy as treatment for chronic noninsertional Achilles tendinopathy (Table 7). Benazzo et al 24 prospectively compared athletes who were treated with longitudinal tenotomies (n = 20) and those who underwent soleus fiber transfer (n = 32). Both groups had significantly improved AOFAS and VISA-A scores postoperatively, although the soleus fiber transfer had a statistically significantly greater increase compared to the longitudinal tenotomy group. The soleus fiber transfer group also had a shorter return to run without pain (98.9 compared with 122.2 days). This was a medium follow-up study with final outcomes measured at 4 years.
Maffulli et al 12 conducted a case-control study of multiple longitudinal tenotomy and debridement treatments in athletes (n = 45) compared to nonathletes (n = 48). The follow-up for this study was 37 months. The authors stated that there was no significant difference between the 2 study groups in their VISA-A scores preoperatively or postoperatively, but all patients showed significant improvement after surgery. The VISA-A scores of the athlete group improved from 53.5 preoperatively to 88.5 postoperatively, and the VISA-A scores of the nonathlete group improved from 55 preoperatively to 74.2 postoperatively. The nonathlete group had a lower satisfaction level (33/48 patients indicated a satisfactory outcome, or 68.8%) compared with the athlete group (42/45 patients indicated a satisfactory outcome, or 93.3%), likely as a result of the higher rate of complications in the nonathlete group (50%) compared with the athlete group (8.9%).
Bohu et al 25 retrospectively compared longitudinal tenotomy and debridement in a group with insertional Achilles tendinopathy (n = 38) with a group with noninsertional Achilles tendinopathy (n = 82). The average follow-up for this study was 38 months, though the range of follow-up was quite large, spanning 7 to 98 months. The noninsertional group indicated a high satisfaction with the treatment outcome, with 74 of 82 patients (90.2%) indicating a good or excellent postoperative outcome.
Level IV
There were 6 level IV studies identified that reviewed longitudinal tenotomy (Table 8). Three studies included athletic populations, 2 studies had mixed populations, and 1 study did not report the activity level of the population. The mean age of patients was in the 20s in 1 study, 30s in 4 studies, and 40s in 1 study. The rates of a satisfactory treatment outcome ranged from 77.1% (37/48) to 100% (8/8). Few major complications were noted other than in the study by Maffulli et al, 12 which had a complication rate of 10%. Complications included superficial infections that responded to oral antibiotics, scar hypersensitivity, and hypertrophic scarring, and all responded to treatment.
Grade of Recommendation
Based on the previously mentioned literature, the operative procedure of longitudinal tenotomy is assigned a grade C recommendation (poor evidence, level IV or V studies with consistent findings), supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. The single level II study showed soleus fiber transfer to confer a greater increase in AOFAS and VISA-A scores compared with longitudinal tenotomy, although both groups had improved scores postoperatively. The 2 level III studies did not demonstrate longitudinal tenotomy to be superior to other operative interventions, though they did show good results for patients treated with longitudinal tenotomy. Longitudinal tenotomy procedure was shown in all studies to provide promising results overall in terms of patient satisfaction with the outcome.
Peritenolysis
Levels I to III
The highest-quality study examining the outcome of peritenolysis was 1 level II study (Table 9). Paavola et al 26 carried out a prospective study (level II) comparing peritenolysis (n = 16) with peritenolysis with debridement (n = 26), with a follow-up at 7 months. This was comparing the surgery for patients with intratendinous lesions (peritenolysis with debridement) with those with only peritendinous involvement (peritenolysis). They found that there was no significant difference in symptoms outcome between groups; however, the peritenolysis had significantly higher performance scores at final follow-up compared to the peritenolysis and debridement group. At the 7-month follow-up, all 16 patients in the peritenolysis group stated that they were satisfied with their treatment outcome, compared with 19 of 26 patients in the peritenolysis with debridement group. Peritenolysis alone had fewer complications as well.
Levels IV and V
There were 2 level IV studies identified that reviewed peritenolysis (Table 10). Saxena et al 27 prospectively examined primarily runners with a mean age in their 40s who underwent either debridement for tendinosis (n = 59) or peritenolysis for paratendinosis or tendinosis (n = 48). The mean return to activity was shorter for the peritenolysis group. Both groups had very favorable results, with 96% good or excellent results in the peritenolysis group and 98% in the debridement group.
Schepsis and Leach 21 retrospectively reviewed competitive runners with a mean age of 29 years with Achilles tendinopathy treated surgically. In the noninsertional subgroup, patients were treated with peritenolysis ± debridement. In all, 15/24 patients returned to their previous level of activity, and 22/24 patients had good or excellent outcomes.
Grade of Recommendation
Based on the previously mentioned literature, the operative procedure of longitudinal tenotomy is assigned a grade C recommendation (poor evidence, level IV or V studies with consistent findings), supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. All 3 studies identified that reviewed peritenolysis demonstrated good results for patients treated with peritenolysis. Although there were level II and III studies in support of peritenolysis, the number of studies addressing peritenolysis was minimal overall, thereby preventing a higher recommendation.
Gastrocnemius Recession
Levels IV and V
There were 4 level IV studies identified that reviewed gastrocnemius recession (Table 11). No studies reported the activity level of their population. Three studies had a mean age in the 40s, and 1 study had a mean age in the 50s. The rates of a satisfactory outcome ranged from 92.9% (16/17) to 100% (8/8). All 4 studies demonstrated statistically significant improvement in ankle pain and functionality, as measured by AOFAS, Foot Function Index, VAS, and/or VISA-A. A range of complications was reported, from 0% in 2 studies to 40% in 1 study.28-30 It should be noted that this study only had 5 patients. 29
Grade of Recommendation
Based on the previously mentioned literature, the operative procedure of gastrocnemius recession is assigned a grade C recommendation (poor evidence, level IV or V studies with consistent findings), supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. Although the number of available studies on gastrocnemius recession was minimal, it should be noted that gastrocnemius recession was shown to provide promising results overall in terms of patient satisfaction, pain level, and/or tendon functionality, with minimal complications. A larger higher-level study is warranted.
Plantaris Excision
Level IV
There were 4 level IV studies that examined excision of the plantaris tendon ± paratendinous scraping (Table 12). Jowett et al 31 looked at paratendinous scraping and excision of plantaris in recreational athletes (n = 19) and sedentary patients (n = 7) in their 40s. There was a statistically significant improvement in VISA-A scores and an 84% satisfaction rate in the recreational athlete group. There was a slightly lower satisfaction rate of 78% in the sedentary group; this was not compared with the recreational athlete group, so its statistical significance is unknown. VISA-A scores were not reported in the sedentary group.
Bedi et al 32 prospectively examined plantaris excision and peritendinous scraping in 15 professional or semiprofessional athletes with a mean age of 32 years. There was a significant improvement in the VISA-A score, and 14/15 (93%) had satisfactory results. Additionally, there was a statistically significant improvement in the aligned fibrillar structure of the Achilles tendon confirmed with UTC scanning postoperatively.
Calder et al 33 studied 16 competitive and recreational athletes with a mean age of 26 years who underwent plantaris excision. There was statistically significant improvement in mean VAS scores and all domains of the Foot and Ankle Outcome Scale (FAOS) postoperatively. The excised tendon was found to be histologically normal in 13/16 cases (81%), but inflammatory changes in the peritendinous connective tissue was evident in all cases.
Calder et al 34 prospectively examined plantaris tendon excision in 32 elite athletes with a mean age of 27 years. There was a significant improvement in VAS and all domains of the FAOS; 90% of athletes reported a satisfactory outcome and 94% returned to sport.
Grade of Recommendation
Based on the previously mentioned literature, plantaris tendon excision is assigned a grade C recommendation (poor evidence, level IV or V studies with consistent findings) supporting it as an effective treatment for chronic noninsertional Achilles tendinopathy. Plantaris tendon excision was shown to provide promising results overall in terms of patient satisfaction, pain level, and/or tendon functionality, with minimal complications.
Other Surgical Treatment Methods
Level IV
There were 5 level IV studies identified that reviewed other surgical treatment methods for chronic noninsertional Achilles tendinopathy (Table 13). These methods were FDL tendon transfer, 35 medial head of gastrocnemius release, 36 peroneus brevis tendon transfer, 37 plantaris stripping and release, 38 Z-plasty tendon lengthening, 39 and debridement with tendon flap. 40 The 5 techniques demonstrated a postoperative satisfaction rate ranging from 81.3% (13/16) to 100% (3/3). Furthermore, 4 of the studies reported a statistically significant improvement in pain, function, and activity level.35,36,38,39 In van Sterkenburg et al, 38 the VAS pain scores decreased significantly following plantaris stripping and release, and VISA-A scores increased significantly postoperatively. In Costa et al, 39 results following tendon lengthening showed a long-term (7.5 years) reduction in VAS scores for sporting activity in 20 of the 21 procedures performed (P < .0005), which suggests excellent long-term reduction of Achilles pain after tendon lengthening. However, a high complication rate (23.8%) was reported with this treatment. There was 1 instance of deep vein thrombosis and pulmonary embolus, 1 instance of superficial infection, 1 keloid scar, 1 minor skin adhesion, and 1 postoperative sural nerve palsy.
Grade of Recommendation
There is insufficient evidence to assign a grade of recommendation for FDL tendon transfer, release of medial head of gastrocnemius, peroneus brevis tendon transfer, plantaris stripping and release, Z-plasty lengthening, or debridement with tendon flap for noninsertional Achilles tendinopathy.
Discussion
This review provides some insight into which operative options for chronic noninsertional Achilles tendinopathy are supported by the current literature. In general terms, all interventions reviewed here for the treatment of chronic noninsertional Achilles tendinopathy have literature to support their efficacy. There is no operative procedure that may be assigned a grade A recommendation (good evidence, level I studies with consistent findings for or against recommending intervention).
Open debridement has been assigned a grade B recommendation, with fair evidence to support it. Open procedures have traditionally been the backbone of surgical management of noninsertional Achilles tendinopathy and have stood the test of time.21,35
Arthroscopic and minimally invasive techniques have been assigned a grade B recommendation with fair evidence to support them. This is not surprising because recent literature over the past 10 years has pointed to the benefits of using MIS and arthroscopic techniques in treating foot and ankle pathology, perhaps because of diminished rates of wound compromise and neurological injury as a result of lesser soft-tissue stripping and dissection.41,42 Such minimally invasive and arthroscopic techniques may prove valuable in the treatment of a concerning area, the noninsertional zone of the Achilles tendon, which is known for wound healing issues that can result in deleterious outcomes. 43 Minimally invasive repair of acute Achilles tendon ruptures has been shown to have significantly fewer complications than open repair in a recent level I trial, with no difference in rerupture rates. 29 This trend toward minimally invasive treatment could potentially also be seen in chronic Achilles tendinopathy treatment. It is evident that larger more robust studies are warranted to better study the outcome of such minimally invasive and arthroscopic techniques about the Achilles tendon and to improve on the level of existing evidence.
Although only obtaining grade C recommendation, peritenolysis and gastrocnemius recession (previously cited as grade C recommendation by Cychosz et al 44 ) have promising evidence, with level II to III studies in their favor. These techniques will require further level I to III studies to better assess outcomes and add to the supporting evidence.
For the remainder of the included surgical interventions, the majority of evidence in the literature is based on level IV studies, with only a few level II or III studies and no level I studies. There are inconsistent findings in comparative studies that are properly powered with validated and appropriate measures to allow any definitive conclusions on which treatment is best. Although current literature for these surgical techniques provides weak evidence for treatment guidelines, in the authors’ clinical experience, many patients gain benefit from their use. Before stronger recommendations can be made for the treatment of chronic noninsertional Achilles tendinopathy, original high-quality articles providing a higher level of evidence are needed.
Limitations
Many of the trials with higher level of evidence compared 2 surgical techniques. Few high-level studies compared operative and nonoperative techniques. Many studies did not separate athletes and nonathletes, who may have different functional demands postoperatively and, thus, different results. Studies often did not delineate the severity of disease, and many studies used mixed techniques, which limits the ability to draw conclusions.
Conclusion
Based on the results of this review, there is fair evidence (grade B) for minimally invasive and arthroscopic techniques for treatment of noninsertional Achilles tendinopathy and for open debridement. There is poor evidence (grade C) in support of FHL transfer, longitudinal tenotomy, peritenolysis, gastrocnemius recession, and plantaris tendon excision. There is insufficient evidence (grade I) to support or refute the use of FDL tendon transfer, release of the medial head of gastrocnemius, peroneus brevis tendon transfer, plantaris stripping and release, Z-plasty lengthening, or debridement with tendon flap for treatment of chronic noninsertional Achilles tendinopathy.
Footnotes
Appendix
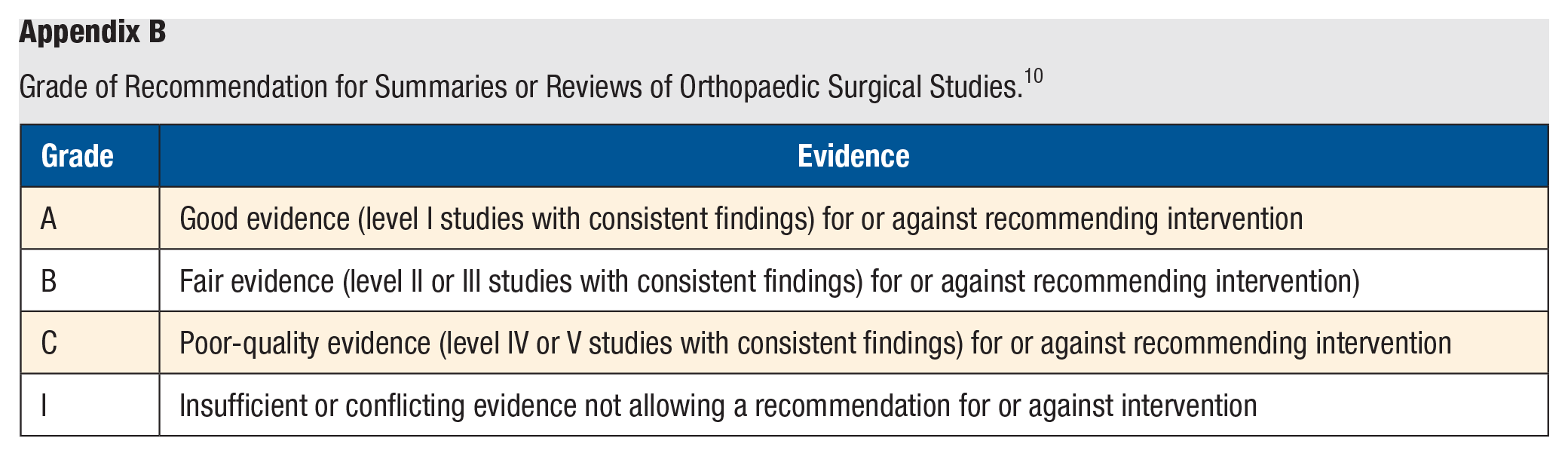
Grade of Recommendation for Summaries or Reviews of Orthopaedic Surgical Studies. 10
| Grade | Evidence |
|---|---|
| A | Good evidence (level I studies with consistent findings) for or against recommending intervention |
| B | Fair evidence (level II or III studies with consistent findings) for or against recommending intervention) |
| C | Poor-quality evidence (level IV or V studies with consistent findings) for or against recommending intervention |
| I | Insufficient or conflicting evidence not allowing a recommendation for or against intervention |
Authors’ Note
There are no disclosures relevant to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.