
Abstract
Background:
Achilles tendinopathy (AT) patients who are refractory or have a suboptimal response to traditional tendon loading rehabilitation may have an additional component of pain with the plantaris tendon. This systematic review aims to evaluate the efficacy and safety of the combination of Achilles tendon scraping (ATS) and plantaris tendon removal (PTR) for AT.
Methods:
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in PubMed, Embase, and Cochrane Library for studies reporting on concurrent ATS with PTR for AT. Study variables included the number of patients, mean age, mean follow-up time, return to activity (RTA) or sport (RTS), pre- and postintervention patient-reported outcomes (PROs), and complications. A meta-analysis was performed for pre- and postintervention Victorian Institute of Sports Assessment–Achilles (VISA-A) scores.
Results:
Seven studies including 235 patients (291 tendons) with a mean age of 40.8 years (27.2-52) and a mean follow-up time of 23.2 months (6-69.6) were analyzed. Mean preoperative score VISA-A (5 studies), and visual analog scale (VAS) scores (2 studies) were 43.4 (0-74.1) and 6.6 (5.8-7.4), respectively. RTA (1 study) and RTS (4 studies) were 100% and 95.5%. Mean postoperative VISA-A and VAS scores were 92.7 (61-100) and 0.8 (0.8-0.8). Pooled VISA-A mean differences were statistically significant at 43.6 (95% CI: 41.0-46.3, P < .00001). The complication and revision rates were 11 (3.8%) and 5 (1.7%), respectively.
Conclusion:
ATS with PTR demonstrated promising preliminary results, with improved postoperative PROs, high reported rates of RTA/RTS, and low complication and revision rates. These findings should be interpreted cautiously given the limited available evidence and high study heterogeneity.
Keywords
Introduction
Noninsertional Achilles tendinopathy (AT) is a degenerative disease common in patients performing physical exercise, with an estimated prevalence of 6% in this population. 36 It is a clinical diagnosis that can be characterized broadly as pain and functional impairment of the Achilles tendon.19,34 The definition of AT is not widely standardized, and terms such as Achilles tendinosis and tendonitis may present under this clinical umbrella but are often reserved until histologic examination of tissue has confirmed the presence of disorganized healing or inflammation. 13 Although AT is most often associated with overuse of the tendon in athletes, it can also be induced by inflammatory and metabolic conditions unrelated to a patient’s activity level. 36 A variety of extrinsic and intrinsic factors have been proposed to play a role, such as increased age, male sex, obesity, blood supply, tendon temperature, genetic predispositions, systemic diseases, training errors, and overuse. 18
Preliminary treatment of AT is generally conservative and is primarily based on lifestyle modifications such as rest, minimizing aggravating exercises, physical therapy (eg, eccentric exercises), and orthotics.9,33 Medical therapy may include topical and oral nonsteroidal anti-inflammatory drugs (NSAIDs), as their analgesic effects may help alleviate the prime symptom of AT; however, outcomes are mixed and NSAID usage in the treatment of AT does not necessarily have strong scientific backing, especially as inflammation has not been shown to play a major role in chronic AT.6,8 Extracorporeal shock wave therapy or nitroglycerin patches have shown some benefits as well. 33 Corticosteroid injections have yielded significant symptomatic improvements in patients with AT, in both short- and long-term follow-ups. 10 Local adverse effects, such as postinjection flare, subcutaneous hypopigmentation, atrophy, infection, tendon rupture, and accelerated osteoarthritis, must be considered. 10 Up to 24% to 45.5% of patients do not respond to conservative management 16 ; in these patients, surgical intervention classically involves excision of areas of tendinosis in the Achilles tendon, release of peritendinous adhesions, and multiple tenotomies.4,22 According to one systematic review, 4 this Achilles tendon scraping (ATS) procedure can be performed as an open surgery or through a minimally invasive endoscopic approach, with success rates of more than 70%.
Over the past decade, there has been greater interest in the role of the plantaris tendon in the pathophysiology of AT, with evidence suggesting that connections between the plantaris and calcaneal tendon may be a driver of pain in midportion AT. 34 AT patients undergoing reoperation due to persistent symptoms after an ultrasonography and Doppler-guided scraping were found to have thickened segments of the plantaris tendon closely associated with the mid-Achilles tendon. 1 Morphologic analysis and comparison of the plantaris tendon to the Achilles tendon have revealed strikingly similar structural changes and immunoreactivity between the two in AT. 31 Extensive sensory innervation and interconnected blood supply of the peritendinous connective tissue between the Achilles and plantaris tendons may reveal a pathomechanism for the persistence of pain due to plantaris tendon interference in AT. 29
The ATS technique involves targeting the area with high blood flow outside the ventral Achilles tendon. It does not compromise tendon blood flow because only the region with changes is targeted, rather than the entire tendon. It is important to note that there is likely partial denervation of the tendon after this procedure. The advantage of ATS with plantaris tendon removal (PTR) is that the procedure is performed outside of the tendon, thus allowing immediate full weightbearing due to nondisruption of the Achilles tendon structure. This allows earlier rehabilitation and quicker return to Achilles tendon loading activities. Additionally, the minimally invasive nature of this procedure allows local anesthesia, avoiding the risks associated with general or spinal anesthesia. 3 Ultrasonographic and color Doppler imaging help guide the procedure, allowing minimal skin incision and tissue trauma by localizing the exact target. 3
Moreover, augmentation of ATR with PTR has shown great promise as a definitive treatment for AT patients with refractory pain.20,26 This systematic review aims to more clearly elucidate the benefits of combined AS/PTR to optimize surgical decision making and improve patient clinical outcomes. Given its minimally invasive nature, we hypothesize that ATS with PTR will result in improved clinical outcomes and high patient satisfaction rates with low rates of complications.
Methods
The guidelines established by the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) were used to perform a systematic search in 3 databases on September 30, 2024: PubMed, Embase, and Cochrane Library. The following keywords were used to perform the systematic review: ((achilles scraping) OR (tendon scraping)) AND ((((achilles tendinopathy) OR (achilles)) OR (outcomes)) OR (efficacy)).
The PICOT (Patient, Intervention, Comparison, Outcome, Time) method was used to guide our search strategy. Patients of all ages were included. The intervention included the patient population undergoing concurrent ATS with PTR. ATS inclusion was focused on traditional mechanical scraping using a scalpel or blunt dissection. Other techniques, such as tendinoscopy, microtenotomy, radiofrequency, or other minimally invasive tendinopathy techniques, were not included to minimize heterogeneity within techniques. Comparative studies with other treatment modalities were included. Outcomes assessed included patient-reported outcomes (PROs), return to activity (RTA) or return to sport (RTS), complications, and failures. Studies with any follow-up period were included. Inclusion criteria consisted of patients undergoing ATS with PTR. Exclusion criteria included case reports, cadaveric articles, reviews, technique studies, expert opinions, non-English studies, and studies without reported outcomes. Two reviewers independently reviewed all the articles included in this study. If no consensus was reached, a third reviewer was consulted to assess final study inclusion or exclusion eligibility. A reference search was performed for all included studies to assess for additional possible studies to be added to this review. This protocol is registered under PROSPERO, CRD42024587114.
Quality Assessment
Two independent authors used the Methodological Index for Nonrandomized Studies (MINORS) criteria to evaluate the quality of the included studies. 27 MINORS scores ranged from 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with a maximum score of 16 for noncomparative studies and 24 for comparative studies. Any discrepancies were resolved by rigorous reevaluation of the articles until an agreement was reached. Scores of 1 and 2 for 7 or more sections (11 or more for comparative studies) were considered low risk of bias, 5 to 6 sections (9-10 for comparative studies) were at moderate risk of bias, and 4 or fewer sections (8 or less for comparative studies) were high risk of bias.
Data Extraction and Statistical Analysis
Study variables evaluated in this systematic review include title, publication date, study year, number of patients and ankles, mean age ranges, mean follow-up time ranges, pre- and postoperative PROs, and rates of complications. Extracted data were collected and analyzed using Google Sheets (Google Drive; Google, Mountain View, CA). If applicable and available, descriptive statistics such as mean, percentage, SDs, and ranges were reported. Meta-analysis was performed to compare pre- and postoperative PROs if at least 3 studies reported a similar PRO. Heterogeneity was assessed using the I2 statistic. P values of less than .05 were considered statistically significant. Forest plots were generated with Cochrane’s Reviewer Manager application (RevMan, version 5.4; The Cochrane Collaboration, London, United Kingdom).
Results
The initial systematic search yielded 52 articles from PubMed, Embase, and Cochrane Library. Of these articles, 14 were removed as duplicates, leaving 38 articles to screen. The title and abstract for these articles was screened for inclusion, and 26 articles were excluded, leaving 12. A full-text review was conducted when 5 studies were excluded for wrong intervention (n = 3) or wrong outcomes (n = 2), yielding 7 studies to be included in this systematic review.3,5,7,11,20,21,25 The screening process is further detailed in Figure 1.

PRISMA diagram of the article selection process.
Patient Characteristics of Included Studies
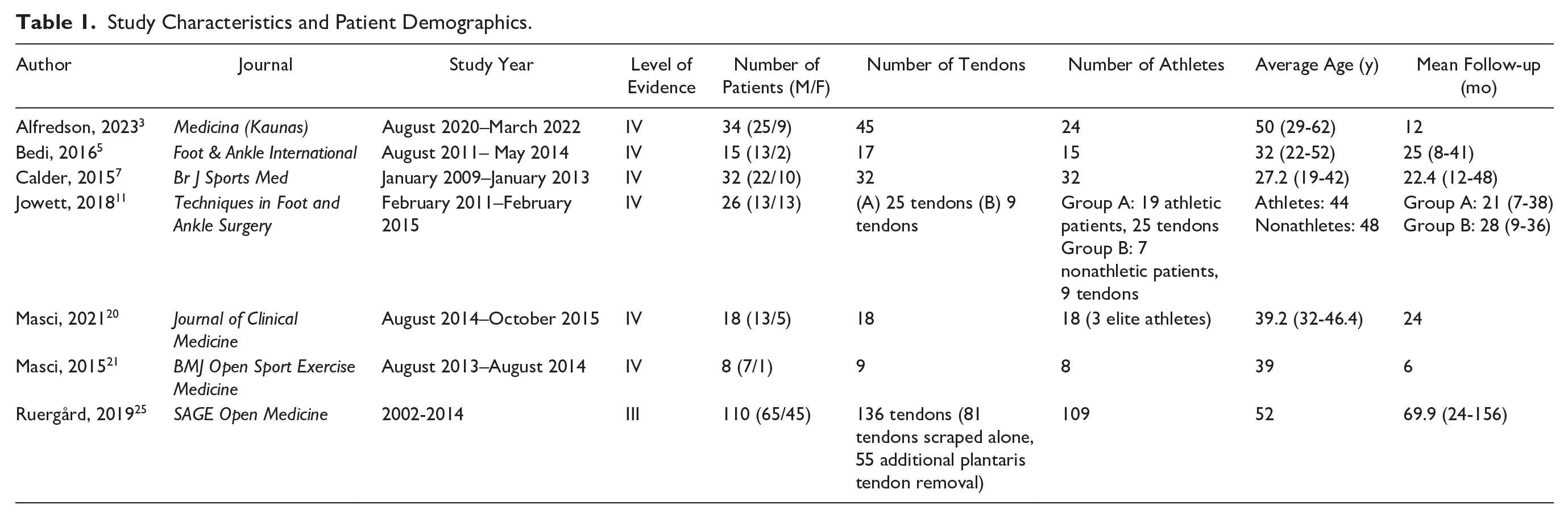
There were a total of 235 patients and 291 tendons (61% male, 39% female), with a mean age of 40.8 years (27.2-52) and a mean follow-up time of 23.2 months (6-69.6). A majority of the studies included athletes (91.4%). Table 1 summarizes the study characteristics and patient demographics included in this study.
Study Characteristics and Patient Demographics.
The MINORS score for the included studies can be found in Table S1. The risk of bias was determined to be low in 3 studies7,21,25 and moderate in 4 studies.3,5,11,20
Surgical and Patient-Reported Outcomes
Five studies used the Victorian Institute of Sports Assessment–Achilles (VISA-A) scores to assess pre- and postoperative reporting outcomes for patients.3,5,7,20,21 Visual analog scale (VAS) scores were used to assess patient outcomes for 2 of the studies,7,25 and the Foot and Ankle Outcome Score (FAOS) was used in 1 study. 7 Mean preoperative VISA-A scores throughout the studies were 43.4 (0-74.1) whereas mean postoperative VISA-A scores were 92.7 (61-100).
The pooled postoperative VISA-A score was statistically significant compared with preoperation with a mean difference of 43.6 (95% CI 41.0-46.3, P < .00001, I2 = 91%) (Figure 2).

Forest plot depicting the standardized mean difference change from preoperative to postoperative Victorian Institute of Sports Assessment–Achilles score.
Mean preoperative VAS scores were 6.6 (5.8-7.4), which decreased to a mean postoperative VAS score of 0.8 (0.8-0.8). However, Ruegard et al did not differentiate the VAS scores between the 2 groups that underwent only ATS or ATS with PTR. 25 Results for all PROs can be found in Table 2.
Surgical Outcomes and PROs.
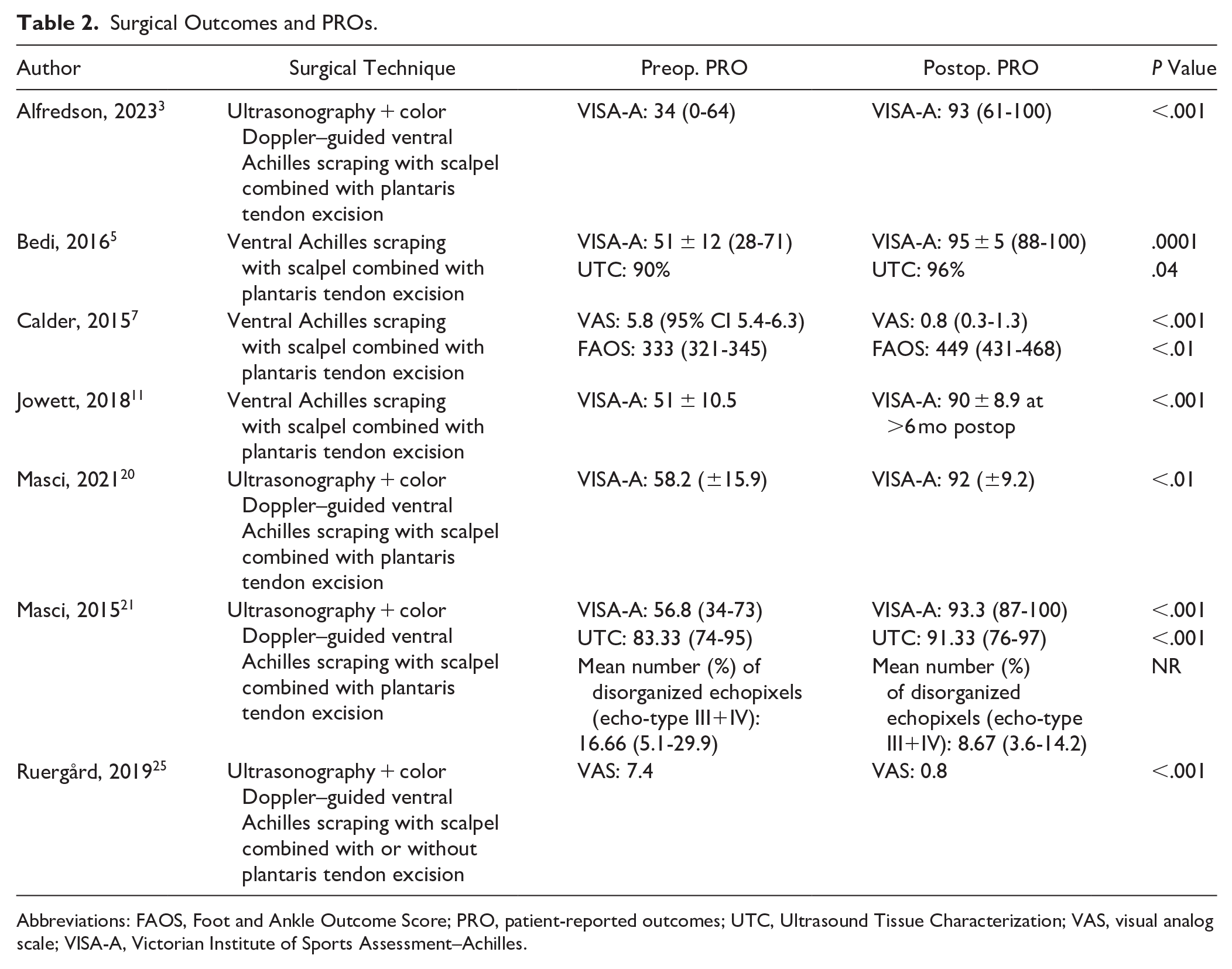
Abbreviations: FAOS, Foot and Ankle Outcome Score; PRO, patient-reported outcomes; UTC, Ultrasound Tissue Characterization; VAS, visual analog scale; VISA-A, Victorian Institute of Sports Assessment–Achilles.
Bedi et al noted improvements in VISA-A scores from 51 ± 12 to 95 ± 5 (P < .0001) 6 months postintervention, indicating statistically significant patient outcomes. The Ultrasound Tissue Characterization (UTC) scans pre- and postoperatively also showed increases in echo types 1 and 2 from 90% ± 8% to 96% ± 5% and decreases from 10% ± 8% to 4% ± 5%, indicative of improved tendon structure. 5 Masci et al 21 showed an increase in VISA-A score from 56.8 (range 34-73) preoperatively to 93.3 (range 87-100) (P < .001) 6 months postoperatively. The UTC showed a statistically significant (P < .001) increase in the mean percentage of echo-type 1 and 2 from 83.3 (range 74-95) to 91.3 (range 76-97) whereas the mean echo-type III+IV) decreased from 16.7 (range 5.1-29.9) to 8.7 (range 3.6-14.2). These findings were consistent in all patients. Seven of 8 patients (8/9 tendons) were satisfied with the result of the treatment. In 2021, Masci et al noted the mean VISA-A scores increased from 58.2 ± 15.9 to 92.0 ± 9.2 at 24 months postoperatively (P < .01). The UTC showed a statistically significant (P = .01) increase in the mean percentage of echo-type 1 and 2 from 79.9% (±11.5) to 86.4% (±10.0). 20
RTA/RTS
Of the 7 studies (235 patients), RTA and RTS were reported by 1 and 4 studies, respectively.3,5,7,11,20 Alfredson et al reported 100% RTA at preinjury levels at 1-year follow-up for 34 patients (45 tendons). 3 Eighty-five of 89 patients (95.5%) had RTS at preinjury levels, with 2 studies reporting a mean RTS at 11.2 months (10.3-12). The full RTA and RTS details can be found in Table 3.
Return to Activity or Sport and Complications or Revisions.

Complications
Across the included studies, 11 complications (3.8%), consisting of wound ruptures, wound infections, neuropathic pain, and ongoing pain, were reported. Five revision surgeries (1.7%), including repeat ventral scraping, gastrocnemius lengthening and tibial nerve neurolysis, and flexor hallucis longus transfer, were reported. These complications were resolved following appropriate medications and revision surgeries. The full details can be found in Table 3.
Discussion
This systematic review found that ATS with PTR demonstrated high postoperative PROs (all with significant improvements), including a statistically significant mean difference of 43.6 for VISA-A (P < .00001) but with an I2 of 91%. However, the strength of this conclusion is limited by substantial heterogeneity among studies (I² = 91%) and the overall low level of evidence. Additionally, there were high rates of RTA at 94.1% and RTS at 95.6%. Furthermore, there were low rates of complications at 4.5% and revisions at 2.03%.
Given the growing interest in minimally invasive techniques, looking at the efficacy and complication rates compared with open procedures is important. Traditional surgical methods for AT repair are effective in restoring strength and function but are tendon-invasive and typically require long rehabilitation. 3 A systematic review covering 62 studies from 1964 to 2014, with an average follow-up time of 40 months, found a mean reported success rate of 83.5% (36%-100%). 12 A 2016 systematic review found that open procedures had varying results for patient satisfaction and complication rates. 4 However, Lohrer et al 15 found that success rates were similar for open compared with minimally invasive approaches at 78.9% and 83.6%, respectively (P = .987). The complication rates for open were higher at 10.5% compared with minimally invasive procedures at 5.3% (P = .053). 15 Similarly, Baltes et al 4 found greater complication rates for open procedures compared with minimally invasive procedures. These findings support the favorable outcomes and low complication rates of minimally invasive approaches like ATS with PTR.
The peritendinous approach also appears to promote a faster RTS compared with more invasive and wider areas of excision surgeries. 26 This technique was supported by immunohistochemical analysis, which demonstrated that there were few nerves inside the Achilles tendon but several running close to the blood vessels on the ventral side of the Achilles tendon. 5 UTC also demonstrates the expected alignment of collagen structure in the medial Achilles tendons after the procedure and is a reliable method of analyzing changes in tendon structure. 14
For patients who do not improve or have suboptimal responses with gradual tendon loading regimens, the plantaris tendon may be mechanistically involved in a subset of these patients. Alfredson et al 3 suspect that if the plantaris tendon is involved, there is a paradoxical worsening of pain localized on the medial side of the Achilles tendon during eccentric training. In several studies, the plantaris tendon was thickened and located close to and interfered with the medial side of the Achilles tendon.1,29,31,35 A sonographic investigation of cadavers found that there exists some degree of normal multidirectional Achilles-plantaris tendon motion. Smith et al 28 suggested that because of the existence of normal Achilles-plantaris tendon motion, alterations in motion or repetitive stress can produce pain. Thus, the plantaris tendon should be evaluated in every patient who presents with Achilles or calf pain. Histologic evaluation of excised thickened plantaris tendons demonstrated similar tendinosis changes as seen in AT. In midportion AT, the plantaris tendon showed similar morphologic changes to the Achilles tendon and can be considered a cofactor in some cases. 30 However, Calder et al 7 found that among 16 patients, 13 of 16 (81%) had a histologically normal plantaris tendon, which suggests that plantaris involvement may not be purely tendinopathic and could be compressive or frictional. Intrinsic and extrinsic foot muscle morphology exhibit differences between healthy individuals and patients with midportion AT. Thus, changes in foot and ankle biomechanics can potentially disrupt the AT.23,24 Additionally, a cadaveric study found that the maximal compressive force for the Achilles and plantaris tendons was at terminal range plantarflexion, supporting the compressive theory pathophysiology. 32 Thus, the excision of the PT may help alleviate these compressive forces on the medial Achilles tendon. However, in some cases, patients may present with medial Achilles pain but have findings of plantaris tendinopathy and a structurally normal Achilles tendon. 2 The plantaris tendon also demonstrates high sensory innervation, further supporting its potential role as a pain mediator. 31 Even in the absence of plantaris tendinopathy, removal of the plantaris tendon can improve pain symptoms in midportion AT, supporting the compressive or frictional phenomenon noted earlier. 7 This highlights the biomechanical relationship between the Achilles and plantaris tendons and the potential pain signaling derived from the high sensory innervation and inflammatory changes in the peritendinous tissue.
Across the studies in this systematic review, there was a trend of improved clinical outcomes being more common for athletic populations compared with nonathletic groups. Maffulli et al 17 matched 45 athletic and 48 nonathletic patients and found that open surgical treatment for Achilles tendinosis had an 8.9% unsatisfactory rate in athletes and 18.8% in nonathletes. In this cohort, nonathletes had a greater body mass index, calf circumference, and subcutaneous body fat. These subjects experienced longer recovery times, complications, and increased rates of further surgery. Another consideration is that athletes may have greater motivation to RTA, better access to resources, and compliance with the rehabilitation recommendations.
Despite the low number of patients and relatively short follow-up time included in this review, this systematic review is of clinical significance by providing a comprehensive overview of the current literature on ATS with PTR. To our knowledge, this is the first systematic review to evaluate this procedure and clinical outcomes and rates of complications. Future studies should focus on conducting larger population, prospective, randomized controlled trials, and longer-term follow-up studies to provide more conclusive evidence on the efficacy of this procedure for AT. Comparative studies should also be conducted on other surgical procedures, nonsurgical treatment, and placebo. Additionally, future studies should use validated methods and instruments for evaluating functional outcomes and pain scores to better interpret the results across studies.
The results of this systematic review must be taken into context with its limitations. First, most of the included studies do not have a control or comparator group, thus preventing the interpretation of these results in the context of another treatment group. This also prevents the determination of whether the ATS or PTR, a combination of the procedures, or other confounding factors (natural healing, rehabilitation protocol) were responsible for the clinical improvement and improved tendon structure seen. Second, the term “scraping” can encompass various approaches, including the traditional mechanical scraping, tendinoscopy, microtenotomy, or radiofrequency. More studies are required to pool outcomes before recommending a specific approach. Third, the meta-analysis had a substantial heterogeneity of 91%, given that most studies had a higher level of evidence. This indicates substantial heterogeneity within the study design and patient populations, limiting the strength of the pooled effect; thus, these findings must be interpreted with caution. Although most studies were prospective, only 1 was retrospective in design. However, these studies were not randomized or anonymized. There are also variations within baseline patient populations and study characteristics. Thus, the generalizability of these findings may be limited and susceptible to selection bias, observer bias, and confounding variables. Fourth, the number of studies and patients across the included studies was relatively small. Fifth, there were no measures of clinical benefit, such as minimal clinically important differences, to determine whether improvements in PROs were clinically meaningful. Additionally, some PROs, such as VAS, may have interpretive variability and may not capture the full complexity of patient outcomes, limiting the interpretation of those findings.
Conclusion
ATS with PTR, in initial studies with lower evidence, has shown encouraging preliminary results with improved postoperative PROs, excellent rates of RTA/RTS, and low complication rates. This study was limited by a relatively small patient population and a lack of comparator groups. Further investigation is needed into PTR as a potential adjunct in surgical planning for selected patients with midportion Achilles tendinopathy.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251346791 – Supplemental material for Achilles Tendon Scraping With Plantaris Tendon Removal for Achilles Tendinopathy: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251346791 for Achilles Tendon Scraping With Plantaris Tendon Removal for Achilles Tendinopathy: A Systematic Review and Meta-analysis by Jimmy Wen, Meraj Alam, Romteen Sedighi, Burhaan Syed, Ramy Khalil, Mouhamad Shehabat, Bethany Joy, Daniel Razick, Adam Razick and Eldo Frezza in Foot & Ankle Orthopaedics
Footnotes
Appendix
Methodological Quality and Risk of Bias.

| Author | Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Data Collection | Endpoints Appropriate to Study Aim | Unbiased Assessment of Study Endpoint | Follow-up Period Appropriate to Study Aim | Loss to Follow-Up Less than 5% | Prospective Calculation of Study Size | Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alfredson, 2023 3 | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | - | - | - | - | 11/16 |
| Bedi, 2016 5 | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | - | - | - | - | 11/16 |
| Calder, 2015 7 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | - | - | - | - | 14/16 |
| Jowett, 2018 11 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | - | - | - | - | 12/16 |
| Masci, 2021 20 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | - | - | - | - | 14/16 |
| Masci, 2015 21 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | - | - | - | - | 12/16 |
| Ruergård, 2019 25 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | - | - | - | - | 13/16 |
Ethical Approval
Ethical approval was not required.
Data Availability Statement
The data sets used and/or analyzed in the current study are available on reasonable request. Please contact J.W. to request data from the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
PROSPERO registration
CRD42024587114
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.