
Abstract
Keywords
Introduction
Healthcare systems are facing a dual crisis. Firstly, they are facing the increased demands of an ageing population resulting in an escalation of healthcare costs (The Deloitte Future Health Care Centre of Excellence, 2022; Deloitte, 2022); secondly, they face threats from climate change which not only imposes risks on both buildings and service delivery but also changes the health demands of communities and the way in which care is provided (Watts et al., 2021). The synergistic nature of these crises has resulted in an increased awareness of the importance of transitioning to more economically, ecologically, and socially sustainable healthcare practices and facilities. Furthermore, healthcare facilities, particularly hospitals, must align with future legislative, investment, and societal requirements for decarbonization, circularity, and climate resilience to ensure continued performance during a less predictable Anthropocene which it is argued we are entering (Folke et al., 2021; Sachs et al., 2019).
The impact of these trends is already evident in healthcare infrastructure and practices with a rise in the number of “green hospitals” in recent years. These are defined as facilities that aim to improve sustainability by addressing the growing problems of carbon, waste, and water intensity in facilities and aligning to green building design principles (Dhillon & Kaur, 2015). The pressure on healthcare is due to the industry's significant contribution to global climate change, making up 4.4% of global emissions and in some regions as high as 10% of national emissions (Lenzen et al., 2020). Under a business-as-usual scenario, healthcare's global emissions could more than triple by 2050, rising to an annual production of six gigatonnes (Health Care Without Harm & ARUP, 2021), likely placing even greater pressure on the industry to improve ecologically sustainability outcomes of both healthcare practices and infrastructure. These required transitions for healthcare services are also occurring at the same time as rising healthcare costs, compounded by demographic shifts and a restriction of government funding that has resulted in a need to curb the growing cost of healthcare (The Deloitte Future Health Care Centre of Excellence, 2022).
Given this, healthcare providers need to look at ways to improve not only healthcare sustainability but also medical outcomes in a cost-efficient manner (Hamed et al., 2016). This has resulted in looking beyond only the provision of care and into the healthcare environment, placing a stronger emphasis on the importance of a therapeutic environment for health outcomes. Therapeutic environments can positively contribute to the health outcomes for patients by enhancing comfort and privacy, and reducing the number of staff errors, falls, and hospital acquired infections (Huisman et al., 2012; Ulrich et al., 2010). Positive therapeutic environments can also improve the wellbeing of patients and staff, improving outcomes and satisfaction and reducing length of stay. This may in turn contribute to reduced operating costs, better staff retention, and improved service delivery (Huisman et al., 2012). As such, “green hospitals” should focus not only on creating sustainable infrastructure but also address the relationships between the built environment and the therapeutic one. In the increasingly cost-constrained healthcare system, the ability to identify and align both EBD and sustainability design principles may help to maximize overall outcomes of the industry.
The importance of the role of the built environment in patient outcomes has resulted in the emergence of the concept of “evidence-based design” (EBD) which mirrors evidence-based practice and looks to shape building design to enhance patient outcomes by improving the therapeutic environment of hospitals based on evidence (Carr et al., 2011; Hamed et al., 2016; Shepley et al., 2009). Recent examples include studies of how digital technology can enable ICU environments to support patient well-being (Kim et al., 2024), how the built environment can act as a therapeutic intervention in adult mental health inpatient facilities (Rodríguez-Labajos et al., 2024), and how built environment healthcare facilities are experienced by children with disabilities and their families (Yu et al., 2024). Yet, despite the clear role of the built environment for patient experiences and therapeutic outcomes in healthcare settings, and the growing need to make improvements on the ecological sustainability of healthcare infrastructure, recent literature is limited when seeking to identify synergies between the two. While some grey literature has investigated overlapping design principles, for example through guidelines to support complementary WELL building standard design features with other green building certification schemes including BREEAM, LEED, and Green Star (IWBI, 2024) to inform design practitioners, a lack of systematic analysis of peer-reviewed research on the topic represents an opportunity to contribute insights. Indeed, the importance of scholars identifying and communicating the state-of-the-art on topics related to the role of design for therapeutic outcomes is supported by the recent publication of a methods paper proposing a specific process by which to conduct such research (Harris D et al., 2024).
Sustainable hospital designs should produce facilities that care for both patients and the planet, utilizing the transition to sustainable healthcare systems to not only deliver environmentally sustainable buildings but also ones that further promote health and healing. The aim of this paper is to identify which aspects of EBD and sustainable design principles (green hospital design) overlap to align sustainable hospital infrastructure with better service delivery, staff satisfaction, and patient outcomes. This overlap represents therapeutic and sustainable design principles (see Figure 1). A systematic literature review will be conducted to develop a conceptual framework for sustainable EBD which aligns both therapeutic and sustainable outcomes for healthcare facilities.
Sustainable hospital designs should produce facilities that care for both patients and the planet, utilizing the transition to sustainable healthcare systems to not only deliver environmentally sustainable buildings but also ones that further promote health and healing
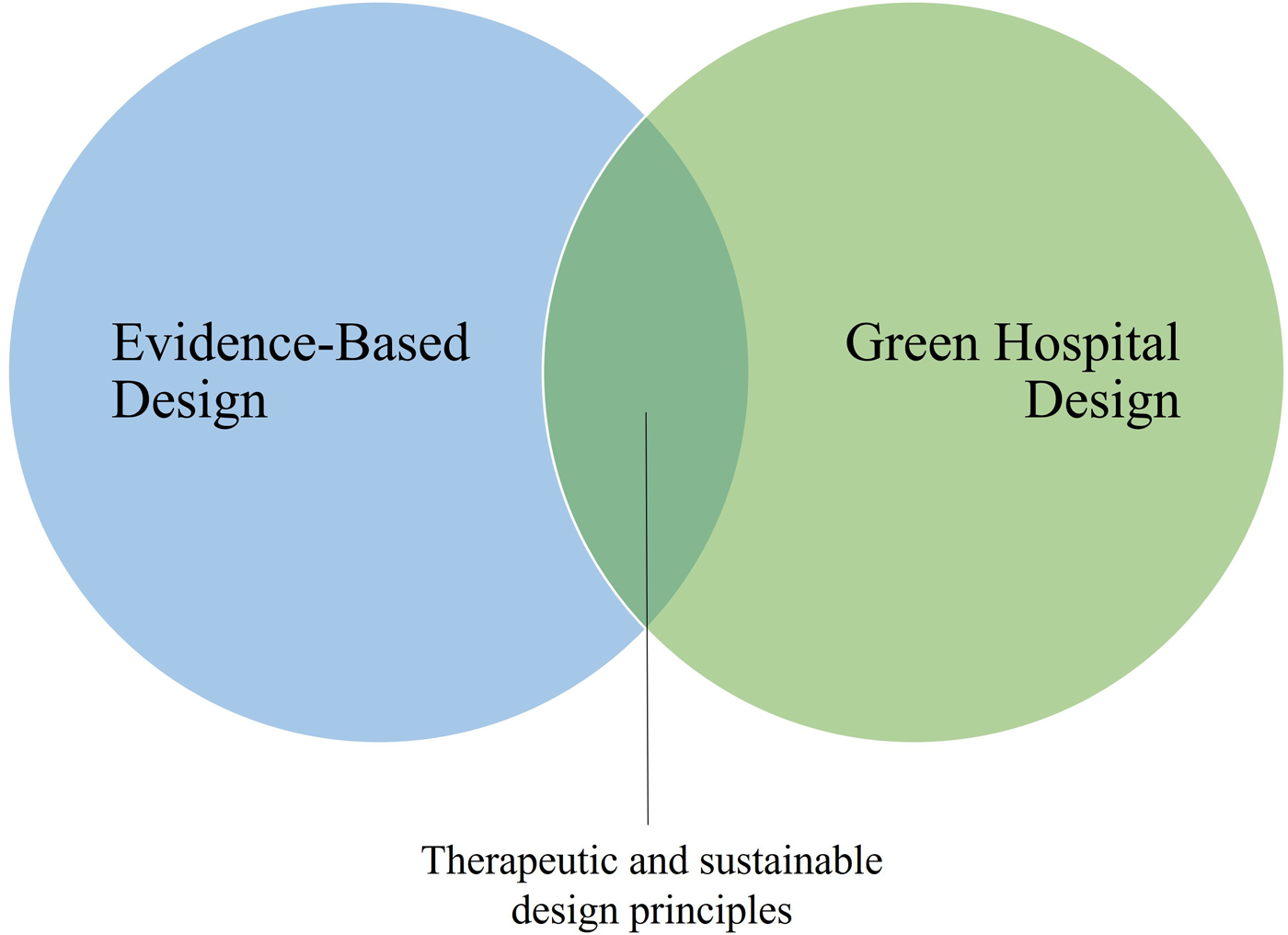
Factors influencing sustainable healthcare infrastructure.
Methods
Search Strategy and Eligibility Criteria
A systematic literature review (SLR) was undertaken. Keyword searches were conducted on two electronic databases: SCOPUS and Web of Science (WoS). Initial keyword selections were tested relating to “evidence-based design” and “green or sustainable healthcare.” The selected keywords relating to sustainability were “green hospital,” sustainable healthcare,” and “climate smart healthcare.” The key search terms for EBD were “evidence-based design,” “therapeutic environment,” and “healing environment.” Following this, a single string with the Boolean operator AND/OR was searched on 21 September 2022 as follows: ((“green hospital*” OR “sustainable healthcare” OR “climate smart healthcare”) AND design*) (“Evidence-based design*”) AND ((“therapeutic” OR “healing”) AND environment) AND (“hospital*” OR “healthcare” OR “healthcare facilit*”)
Initial results were limited to documents published in the English language since 2010 in OECD countries. The initial search yielded 1,215 results; the removal of duplicates resulted in 1,101 documents. Then documents were reviewed based on title relevance to EBD or sustainable healthcare, further limiting the results to 290 documents. Next, an in-depth abstract review was undertaken to assess relevance, and documents were limited to those studies undertaken in acute care (hospital) settings, excluding those relating to specific conditions, in an attempt to produce generalizable results across the whole healthcare setting. After exclusions, this resulted in 94 papers identified for review. Quality was addressed by including only peer reviewed articles published in journals with Q1 or Q2 rankings, and the study approach and methods were assessed for rigor, if appropriate. Full text analyses resulted in a total of 65 articles included in the final review. Figure 2 outlines the SLR screening process. Due to the limited total number of articles meeting the inclusion criteria, the study includes peer-reviewed articles beyond the most recent 10-year period.
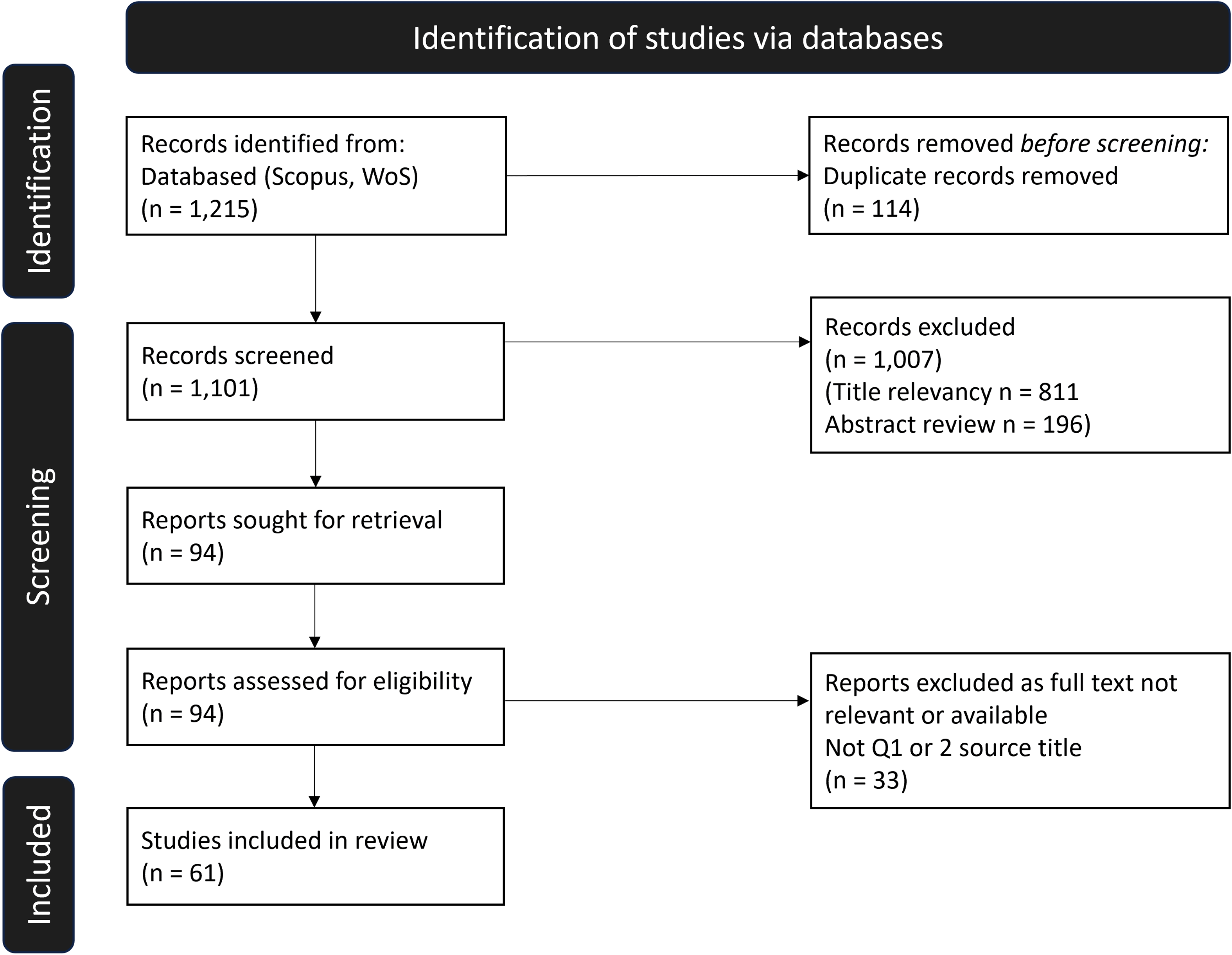
Systematic literature review process.
Results
Sustainability Principles
The first phase of the assessment was to determine the cited sustainability features within the literature. No single defined set of criteria exists for sustainable hospitals, which Castro et al. (2015) note as a key issue that needs to be overcome. This gap has resulted in the interchangeable use of the terms green and sustainable, in which the former focuses on environmental performance and the latter incorporates social outcomes. Consequently, a focus on “green” outcomes does not necessarily mean the design produces a therapeutic environment. Indeed, overvaluing the achievement of higher levels of green certification may actually result in a lesser focus on design features that deliver positive patient wellbeing (Golbazi & Aktas, 2016). Castro et al. (2015) outline that the concept of sustainable hospital building is much broader than green buildings and is “related to the environmental, societal and economic dimensions of sustainable development” (p. 1409).
Key sustainable hospital features mentioned in the literature are summarized in Table 1. These were derived from building, environmental, or sustainability assessment certifications (e.g., the LEED or green star rating systems), and desirable outcomes identified by article authors. Eight key themes were identified as detailed in Table 1.
Sustainable Hospital Features.
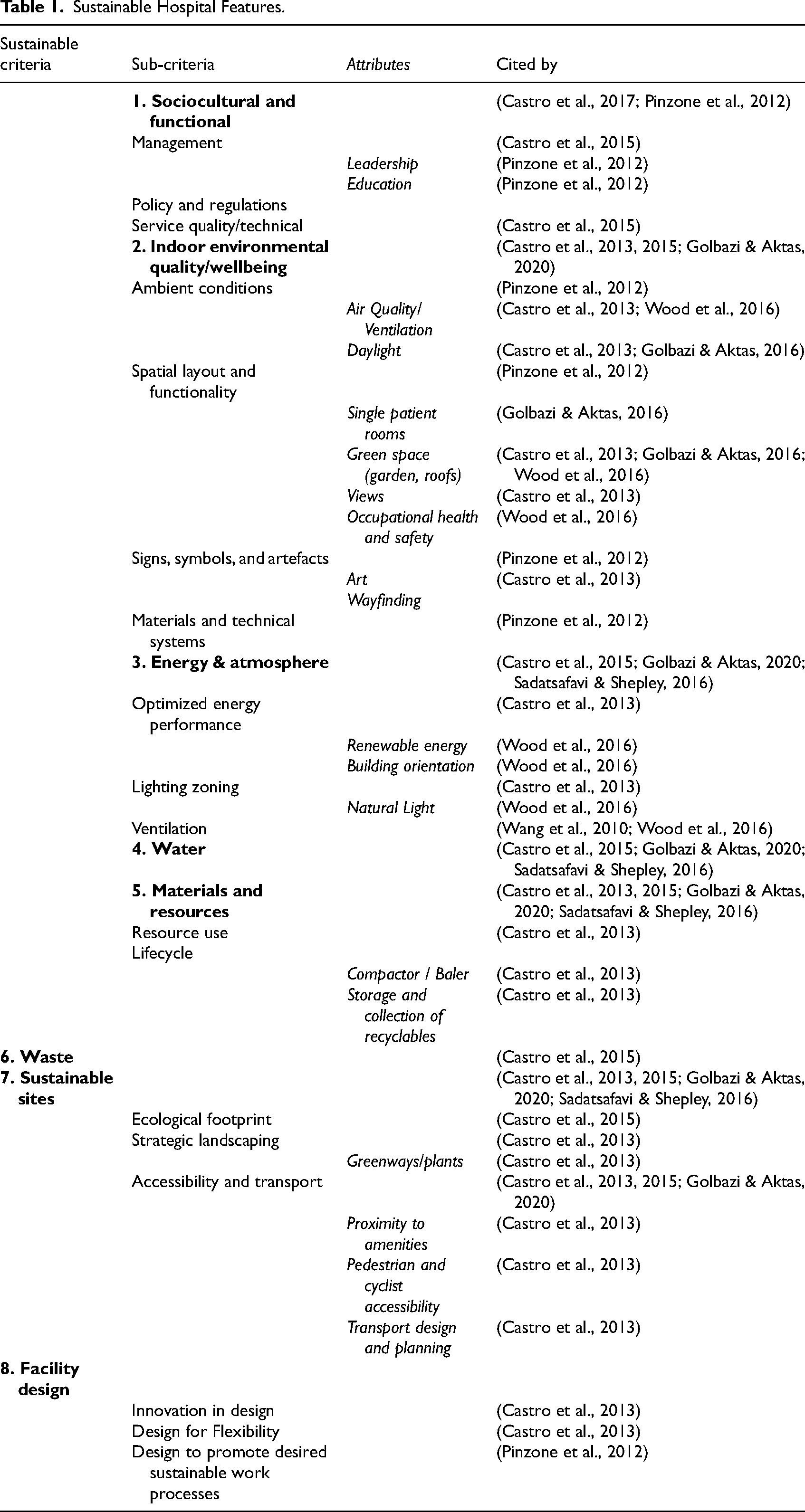
Sociocultural and functional relates to the internal organizational factors that shape and promote sustainable practices within the healthcare setting (Castro et al., 2017; Pinzone et al., 2012). The built environment can be used to shape organizational culture and desired work processes, encouraging participation in sustainability initiatives (Pinzone et al., 2012).
Indoor environmental quality and wellbeing consists of the subcategories of ambient conditions, spatial layout and functionality, signs, symbols and artefacts, and materials and technical systems (Castro et al., 2013; Golbazi & Aktas, 2016; Pinzone et al., 2012; Wood et al., 2016). These refer to the social aspect of the building, creating a comfortable environment for patients, and creating layouts which promote safe work processes (Pinzone et al., 2012).
Energy and atmosphere relate to design factors that reduce the energy demand of buildings and increase air quality. Average energy consumption was found to be correlated with the built surface area (García-Sanz-Calcedo, 2014), and can be influenced by improvements in lighting systems (LED lighting; García-Sanz-Calcedo, 2014), external enclosures (insulation, sealed envelope, solar films; Calama-González et al., 2019; García-Sanz-Calcedo, 2014), and passive design which optimizes natural light (Pinzone et al., 2012) and air circulation (Wang et al., 2010). Improvements targeting energy demand can not only produce energy savings but also financial savings for organizations.
The categories of Water and Waste both relate to encouraging reduction—in the use of water and the production of waste—to limit the environmental impact. Pereno and Eriksson (2020) note the value of taking a lifecycle approach within the design to facilitate processes for optimizing for water and waste to reduce the impacts of the whole system.
The Materials and resources category relates to the utilization of sustainable materials and the sustainable management of resources. This includes during the construction phase, as well as planning for avenues to promote practices for recycling of materials, including the use of compactors and the storage and collection of recyclables in the facility.
Sustainable sites can have a broad impact, contributing to the environmental, social, and economic sustainability of facilities. A sustainable site can allow for ease of accessibility (Haywood et al., 2018), contribute to indoor and outdoor air quality (Gola et al., 2019), maintain ecological value (Castro et al., 2015), enhance the use of landscaping (Castro et al., 2013), and positively impact social and economic regeneration of cities (Castro et al., 2017). Well-positioned facilities can also support the use of low or no carbon transport systems.
Facility design for sustainability relates not only to the spatial layout but also encompasses the need for innovation and flexibility in the design (Castro et al., 2013). Flexibility is needed to accommodate the changes to care delivery during the building's lifespan and cater for the dynamic nature of healthcare (Pinzone et al., 2012). The ability to allow for scalability and adaptability in the design can not only save on resources but also prolong the lifespan of facilities, or promote desired work practices (Pinzone et al., 2012).
Sustainability Enablers, Barriers, and Motivators
Motivators for improving the sustainability of facilities included seeking improvements to patient and staff satisfaction and enhancing public image, as well as boosting environmental performance (Thiel et al., 2014). Golbazi and Aktas (2020) found when comparing LEED certified facilities to the national average that patients rated green facilities slightly better in overall facility ratings, an increase of 3.5% compared to the national average, and also recorded an increase of 5.6% when asked if they would recommend the facility to others. Additionally, green retrofitting of facilities has been shown to have environmental, economic, social, and functional benefits, with findings showing it can result in energy use reduction and improved energy performance/efficiency, lowered costs, reduction in greenhouse gas and CO2 emissions, and improvements in indoor environmental quality (IEQ; Ergin & Tekce, 2020). A comparative longitudinal study by Thiel et al. (2014) comparing patient outcomes after an upgrade to a facility with green certification, found that there was a reduction of 70% in bloodstream infections at the new facility, and a reduction in the number of corrections to the Medication Administration Record per 1,000 doses by 49%. The same study also showed a 25% reduction in staff turnover and a 30% reduction in position vacancies, with a 5% increase in staff satisfaction (Thiel et al., 2014). However, previous research has also shown high variability in reported findings for operational and maintenance cost benefits for green hospital facilities which could act as a barrier (Sadatsafavai et al., 2014; Sadatsafavi & Shepley, 2016). A key enabler defined by Pinzone et al. (2012, p. 7) is the need to create “synergic changes in both the physical structures and the organizational approaches.” They outline a need to align organizational and architectural levers through four key propositions.
Evidence-Based Design
The second phase was to identify common themes related to EBD from the literature. EBD acknowledges the link between the built environment and occupant health, and promotes the use of design principles that are based on research and practice (Shannon et al., 2020). These principles can be used to promote desired health outcomes and positively contribute to improving patient and staff satisfaction, experience, and performance (Bilec et al., 2010; Sidenius et al., 2017). Carmel-Gilfilen and Portillo (2016) state that a “holistic culture of care” can be fostered by employing both empathetic and user-centered design approaches. By integrating the needs of users into design, healthcare buildings can deliver a holistic experience of both the intangible and tangible (Martens et al., 2019; Rashid, 2010; van Oel et al., 2021). As users “measure the quality of the service experience based on what they can see, feel, and understand” (Steinke, 2015, p. 33), moving towards healthcare buildings that are psychosocially supportive as well as promoting better health outcomes will result in many benefits (Rehn & Schuster, 2017).
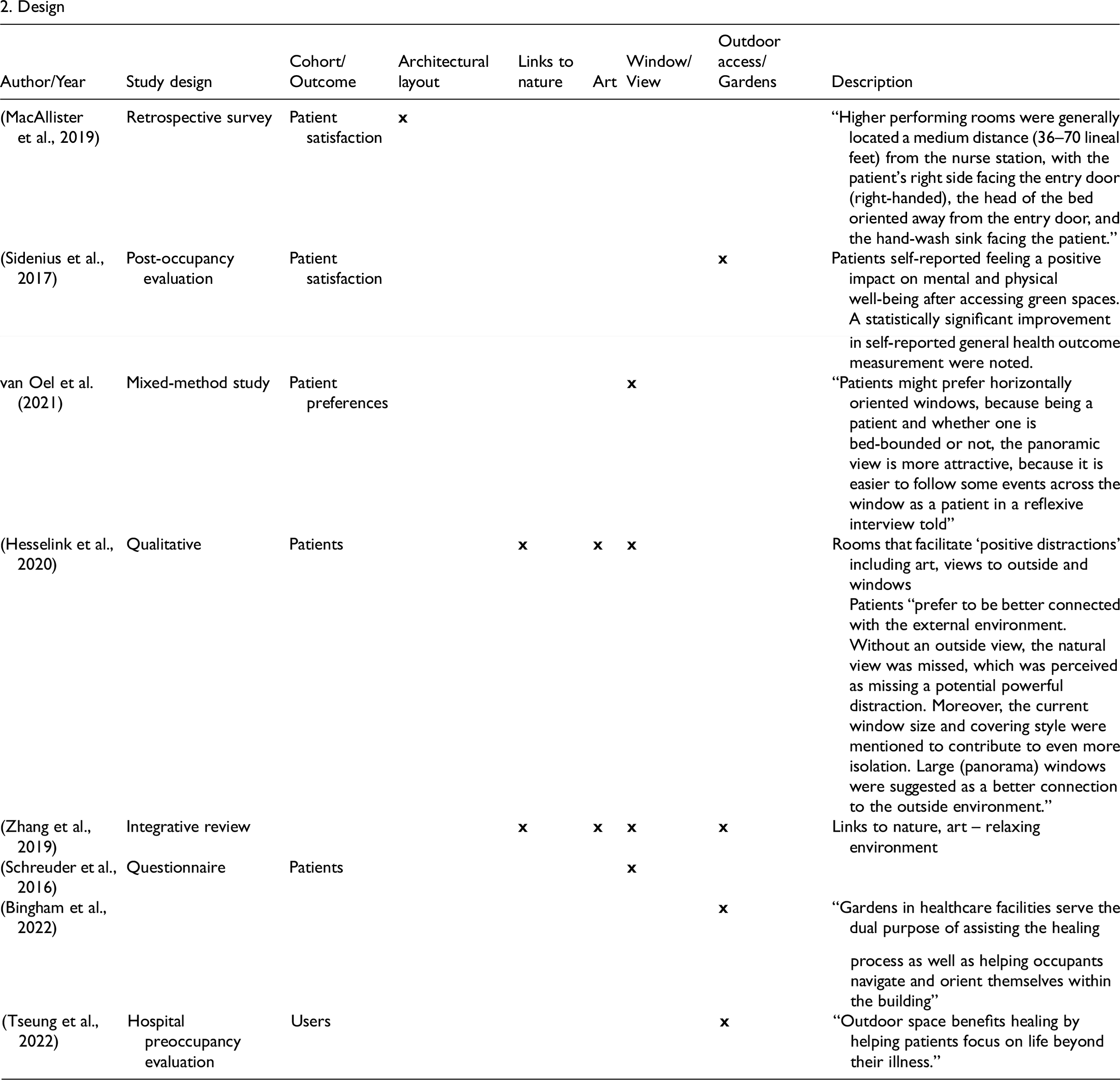
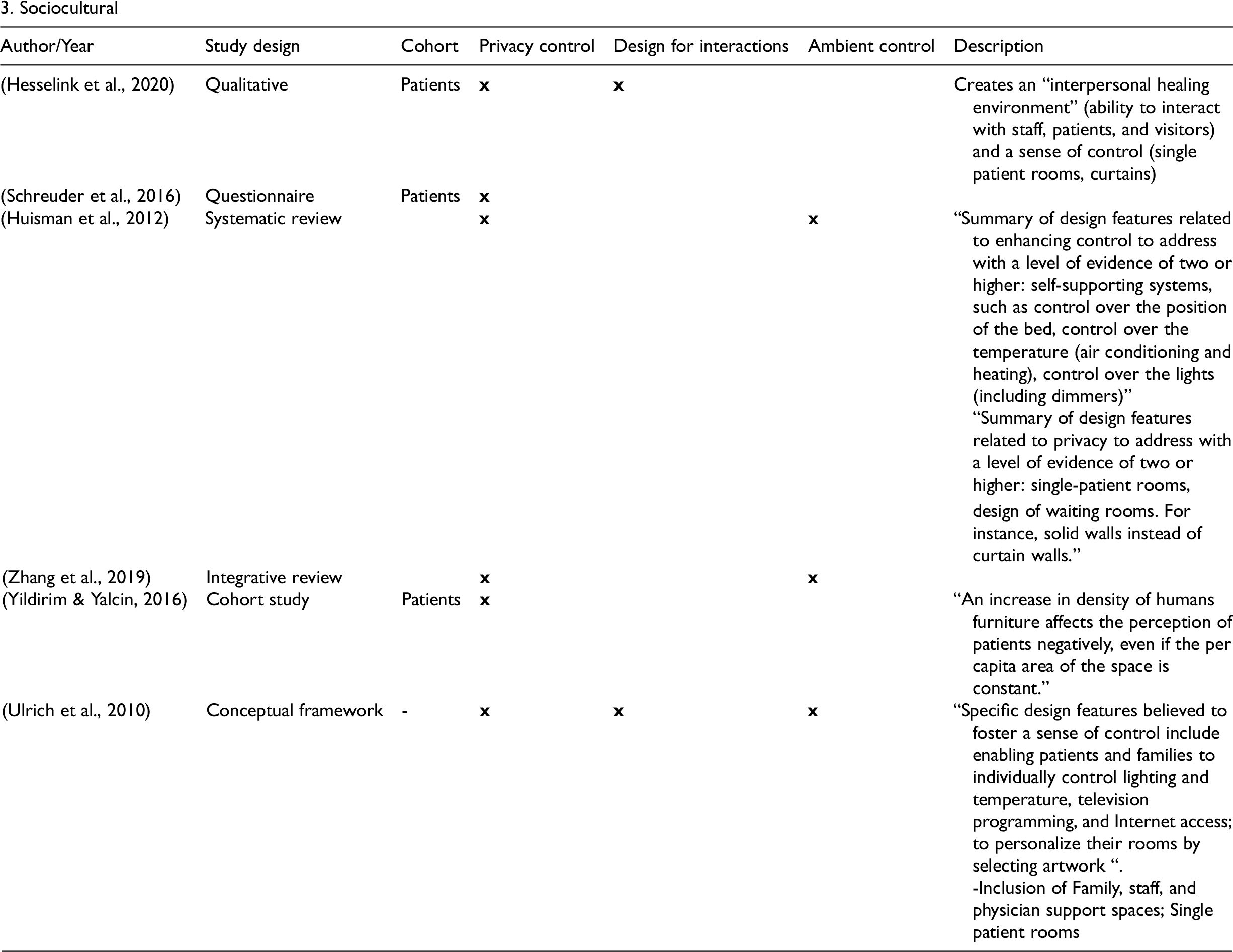
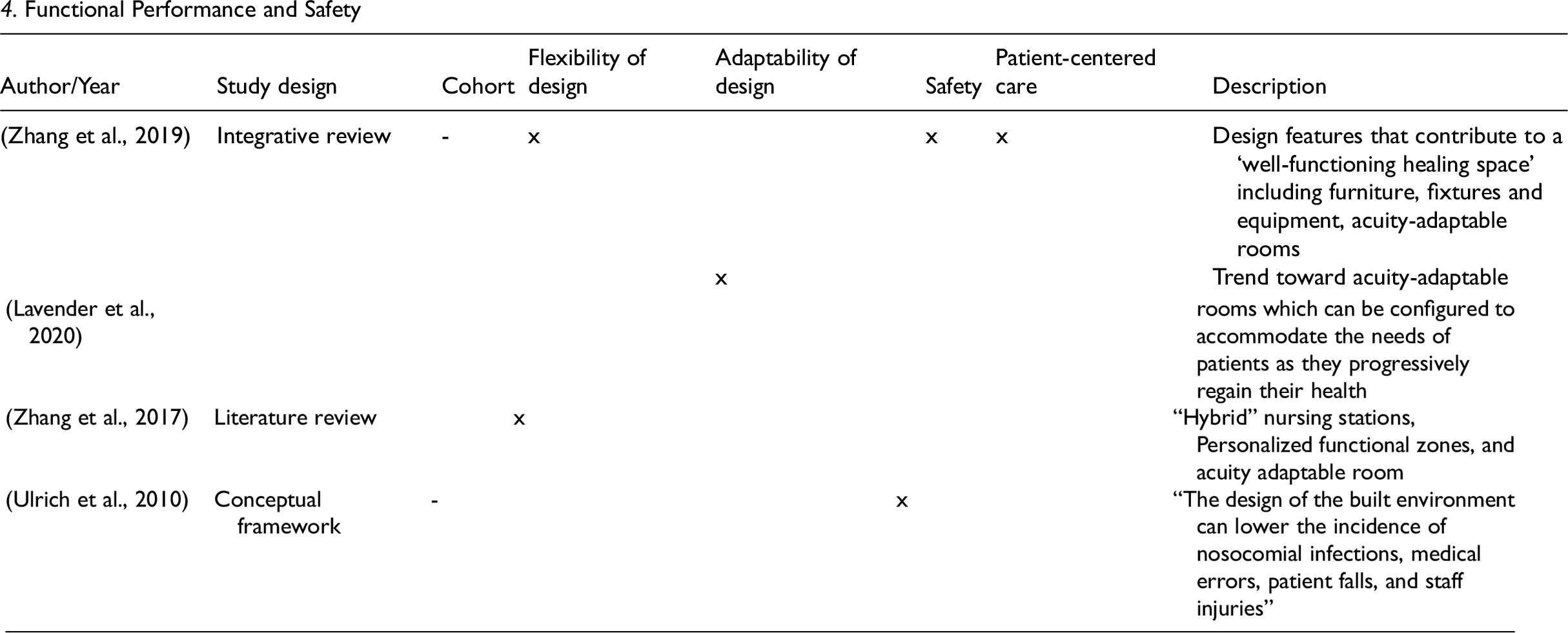
The common EBD themes identified are shown in Table 2, along with a description of the study and key findings. Findings were categorized into the following groups: Indoor environmental quality, which outlines indoor ambient conditions and aesthetic features; Design, which focuses on the architectural layout and building design; Sociocultural, which focuses on designing for interactions and control; and lastly Functional performance and safety, which relates to features that promote safe practice and patient-centered care.
EBD Features.
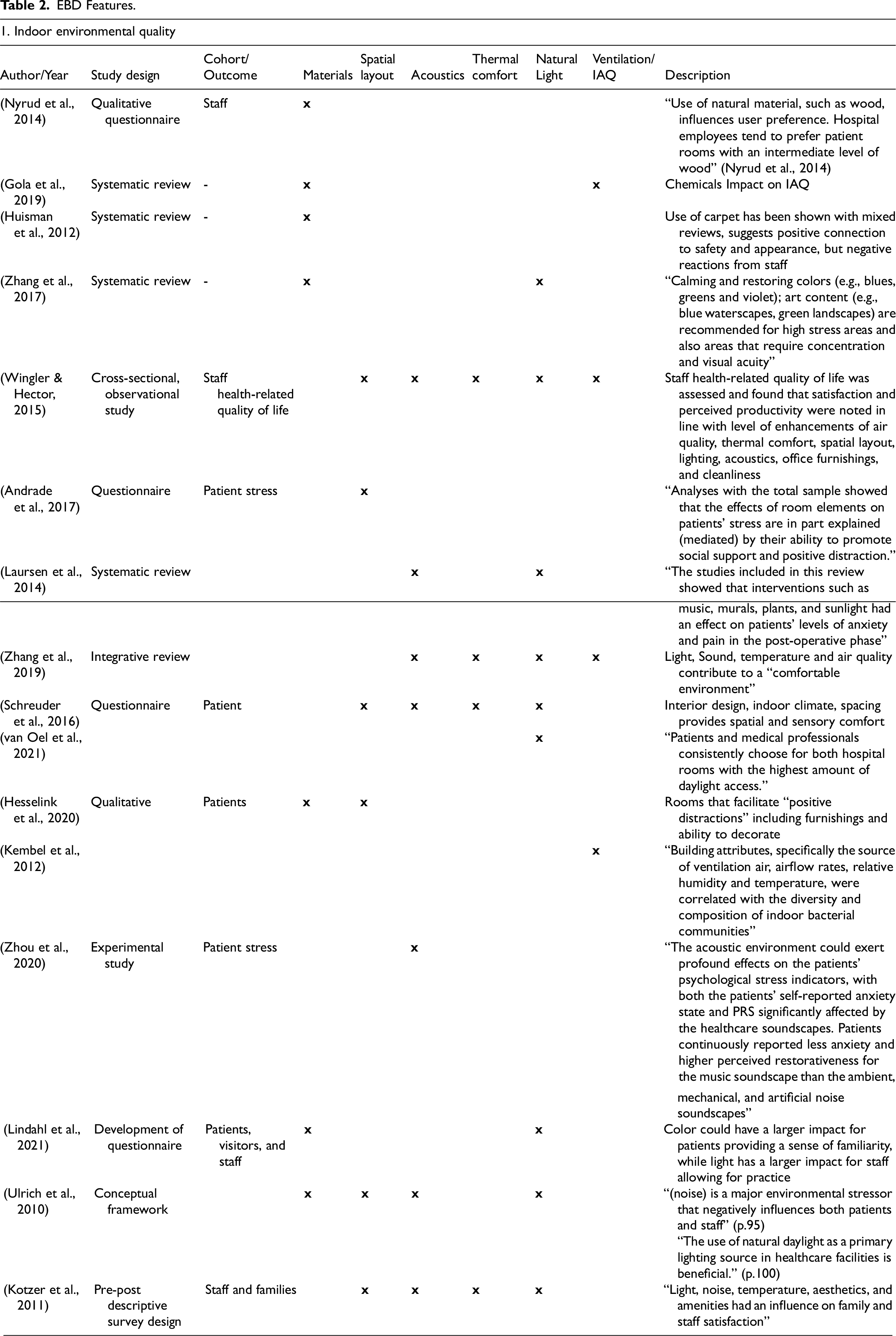
IEQ was discussed in 16 studies and was the most common focus of the studies reviewed. IEQ can be further divided into materials, spatial organization (layout), acoustics, thermal comfort, natural light, and ventilation/indoor air quality (IAQ). Enhanced IEQ can both directly and indirectly contribute to patient health outcomes, including through increased comfort, satisfaction, and safety (Wingler & Hector, 2015). Design features can be used as “positive distractions” for patients while also enabling better performance and safety of staff by supporting productivity and a reduction in errors (Quan et al., 2017; Wingler & Hector, 2015). Additionally, sound and light can contribute to feelings of alertness among staff and facilitate patient communication (Sundberg et al., 2017).
Design was the focus of eight reviewed studies. Subcategories of design were related to architectural spatial design, links to nature, art, windows/views, and outdoor access/use of gardens. MacAllister et al. (2019) found a connection between patient satisfaction with a facility and the spatial layout. Certain features, such as room orientation, distance to the nursing station, and door and bed orientation, were significant contributors. Despite single patient rooms not being the focus of any study reviewed, this feature was frequently identified as a positive contributor to patient satisfaction (Ulrich et al., 2010), with Yildirim and Yalcin (2016) finding that satisfaction decreased with an increase in human density even when the space per person remained consistent. The use of identical patient rooms was also found to decrease staff errors by allowing easier delivery of routine care (Zhang et al., 2019). The inclusion of links to nature in the design, use of art, windows, and views to nature all act as positive distractors, creating a relaxing environment which improves patient comfort and satisfaction (Zhang et al., 2019). The use of panoramic style windows was found to be preferable for patients and creates a larger connection to the outside environment. The presence of a garden was also shown to contribute to improved self-reported mental and physical wellbeing among patients (Sidenius et al., 2017), and Bingham et al. (2022) noted that a garden could also act to support wayfinding.
Sociocultural themes were discussed in six studies. These specifically related to an enhanced sense of control to support privacy and address ambient conditions, and facility design that facilitates interactions. Fostering a sense of control can result in improvements in stress, comfort, and satisfaction (Ulrich et al., 2010) and reduce negative distractors from undesirable ambient conditions (Zhang et al., 2017). Creating an interpersonal healing environment through facilitating social interactions among staff, patients, and visitors was also noted as a key factor for healing (Hesselink et al., 2020). Flexibility for visitors and the allocation of “family support spaces” (Ulrich et al., 2010) to facilitate connection has also been identified as important for support and healing.
The Functional performance and safety EBD theme was discussed in four studies. Zhang et al. (2017) outline the need for design to contribute to a well-functioning healing space contributing to patient-centered care. Safety enhancements can be achieved through design features that reduce the occurrence of hospital acquired infections, patient falls, medication errors, or workplace injuries. This can be based on the principles already discussed, including materials, lighting, ventilation, or layout, and can also be enhanced through other elements, such as the positioning of hand sinks/soap, equipment availability, and emergency systems (Zhang et al., 2019). Additionally, flexibility and adaptability are common principles that appear to facilitate ongoing functional performance and efficiencies (Zhang et al., 2019). The use of hybrid or decentralized nursing stations (Zhang et al., 2017), acuity adaptable rooms (Lavender et al., 2020; Zhang et al., 2017, 2019), and the ability to support visitor and staff spaces are beneficial.
EBD Enablers, Barriers, and Motivators
Designing facilities based on EBD principles has diverse benefits that can positively impact patients, families, staff, and organizational outcomes (Ulrich et al., 2010). An analysis of EBD case studies by Zadeh et al. (2015) noted that “a considerable ROI (return on investment) resulted from improved clinical outcomes” when implementing EBD principles (p.70). The use of technology in the design phase was seen to be an enabler for designing facilities that result in therapeutic outcomes. Co-designing for value generation with key stakeholders enables greater collaboration with end users and ensures that designs meet the needs of end users. Enablers such as 3D visualizations (van Oel et al., 2021), use of narratives (Carmel-Gilfilen & Portillo, 2016), stakeholder engagement in the predesign phase (Elf et al., 2016), and the use of systems such as Building Information Modelling (Wang et al., 2010) can also assist in ensuring EBD is incorporated into building design. Zadeh et al. (2015) also recommend the use of evidence on lifecycle costs and benefits to support decision makers through improved transparency about long-term benefits.
Discussion
Conceptual Framework for Sustainable EBD
The studies included in this review suggest that synergies lie between sustainable hospital infrastructure design and EBD, providing the potential to enable increased outcomes across ecological, social, and economic performance of facilities. In the increasingly cost-restricted healthcare landscape, integrating the benefits of EBD and sustainable hospital infrastructure design could help to support the rationale to invest in ecologically sustainable initiatives by highlighting the co-benefits for patients and staff, further to the environmental and economic benefits. Table 3 shows a theoretical framework for evidence-based sustainable design for healthcare, highlighting the possible benefit areas for end users. While the literature features studies of individual cases or a small number of cases (see literature table) it is yet to provide a framework to map alignment of both the design principles that achieve both these critical aspects for the future of health care (sustainable healthcare infrastructure design and therapeutic outcomes). In addition, important work by industry such as how to align the WELL Building Standard with other globally recognized green building certification schemes (LEED, BREEAM, Green Star) (IWBI, 2024) is tailored to design practitioners seeking to use such schemes, rather than analyzing the peer-reviewed evidence base. Our study complements current practitioner information and individual concept or case study peer-reviewed articles by providing a systematic review and analysis of the evidence-base of the peer-reviewed literature relevant to the topic. In doing so, the study contributes a preliminary framework to the literature to be drawn upon by scholars and practitioners including decision makers (regulators, investors, and other stakeholders) as well as designers, and to be built upon through further research. For example, research should compare the framework with other frameworks in the literature based on single concepts only, and to further refine the framework as further case studies and research is undertaken. Analysis of the current peer-reviewed academic literature identifies two areas with the largest potential for synergies: Indoor environmental quality and wellbeing and Energy and atmosphere.
Conceptual Framework for Sustainable Evidence-Based Design for Healthcare.
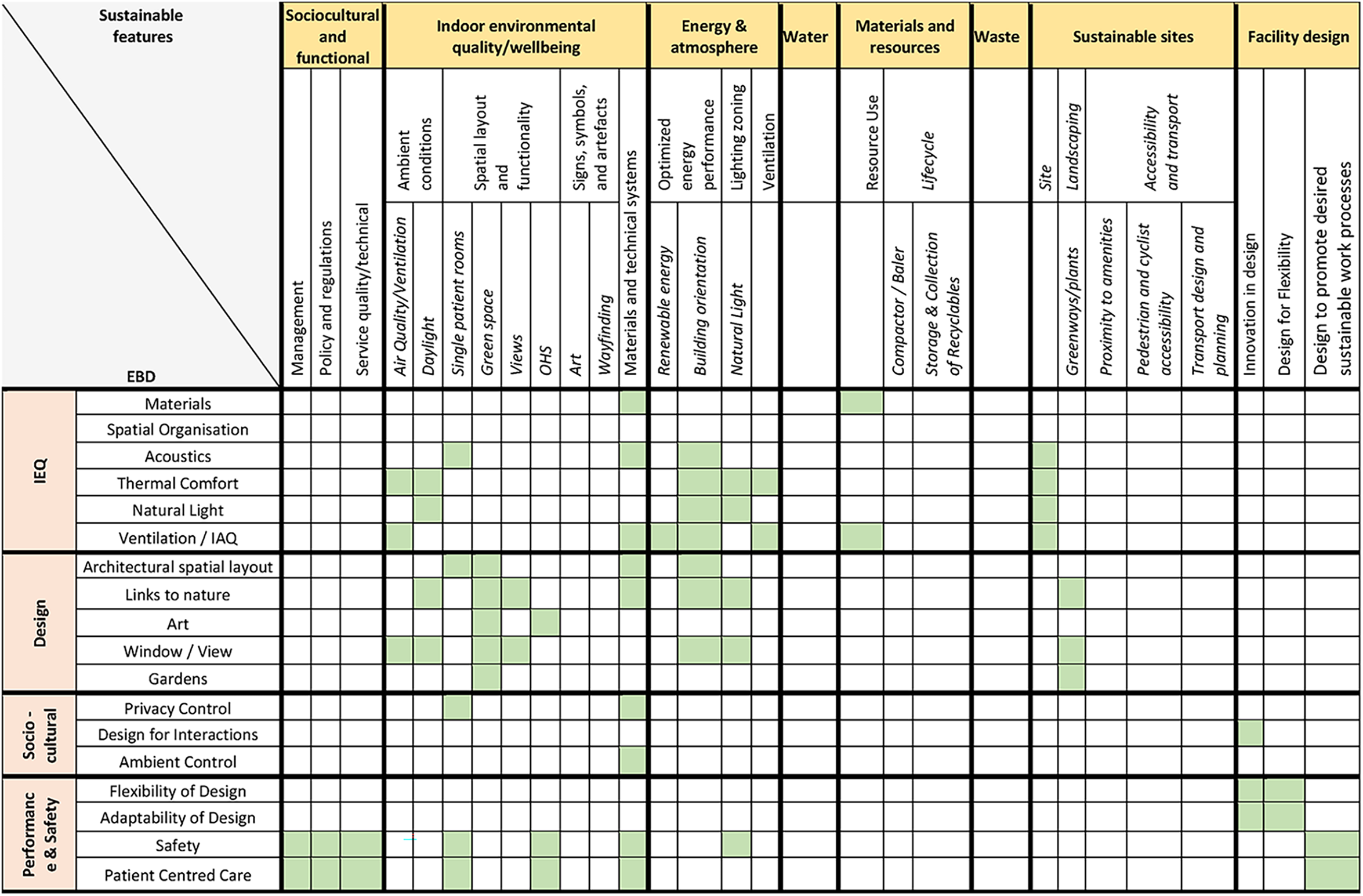
Indoor environmental quality and wellbeing predictably aligns well to the concept of EBD, as the goal of both is to create a positive indoor environment for users. Interestingly, the choice of sustainable materials not only limits the ecological impacts from the buildings, but can limit both noise and impact to IAQ and can be used to provide links to nature (e.g., use of wood). Material choice can also increase safety by reducing falls and workplace injuries. The availability of technical systems can be used to provide control of privacy and ambient conditions to patients, as well as contributing to safety and patient-centered care.
Energy and atmosphere most notably aligns with increased natural light and air quality. Strategic facility orientation and architectural approaches that create passive designs optimizing natural light can reduce energy demands and improve user satisfaction (García-Sanz-Calcedo, 2014; Lavy et al., 2015; Wood et al., 2016). Ulrich et al. (2010) outline the use of self-shading orientations and improved building envelopes to limit demands for heating, ventilation, and air conditioning as well as aiding improvements in air quality (Wang et al., 2010). The inclusion of user controls for ambient conditions such as blinds and protective glazing films can reduce energy demand while also enhancing a sense of control for patients (Lavy et al., 2015; Pinzone et al., 2012). Building orientation can further be used to enhance the use of views and windows, with links to nature acting as a positive distraction for healing.
Aspects of the Sustainable sites category show moderate synergies with IEQ and design aspects of EBD. The choice of site can facilitate the optimization of natural light and ventilation and provide opportunities for building orientation to support energy optimization (Gola et al., 2019). Site accessibility can facilitate social support as it can impact informal caregivers’ ease of access to the hospital (Haywood et al., 2018; Zhang et al., 2017).
Sociocultural and functional elements can align with existing systems and practices for management, and with policies that help shape service quality. The importance of leadership and organizational culture for delivering patient-centered care extends to shaping sustainability behaviors. The sociocultural context the physical environment sits within can alter how care is delivered, instilling values of sustainability, and shaping work processes can help to successfully implement sustainability initiatives within a healthcare setting.
Facility Design has potential synergies with EBD principles for performance and safety. Adaptability and flexibility of design can help to accommodate changing patient needs and future healthcare demands, and could be extended to the changes brought by the health impacts of climate change. Designing for the future can ensure that facilities are better equipped to adapt to and cope with a changing climate, and can also limit the need for redesign, thus reducing capital investments and resource use.
Materials and resources showed limited synergies with EBD principles while Water and Waste were not shown to have any synergies with the EBD principles based on the evidence included in this review.
Material choice can enhance EBD benefits and can be used to reduce impacts on IAQ from the use of materials with high chemical loads. While limited or no synergies were revealed in this review, the benefits of water and waste management systems as well as sustainable materials and resource use can have important ecological impacts extending beyond the built environment of a facility, also offering potential for reduced operating costs.
Conclusion
The results of this paper indicate that there are areas of synergy between EBD principles and sustainable healthcare infrastructure design principles that can inform decision-making to optimize co-benefits for patients and the planet. With increasing demands for the healthcare system to reduce their environmental impact and at the same time reduce costs, the framework developed and detailed analysis of the current peer-reviewed studies can help decision makers to prioritize and justify investment in design principles that achieve both sustainability and therapeutic outcomes based on the latest evidence from the peer-reviewed literature. While the potential of the framework is currently limited to the studies in the literature to date, this can be updated and refined as further research is undertaken. Furthermore, it may identify topics for future studies to provide evidence or clarification of outcomes of design principles for sustainability and therapeutic outcomes.
The results of this paper indicate that there are areas of synergy between EBD principles and sustainable healthcare infrastructure design principles that can inform decision-making to optimize co-benefits for patients and the planet
Implications for Practice
Facilitate the use of design features that can result in better environmental sustainability while also delivering therapeutic environments.
Support the healthcare industry to meet the challenges of reducing their impact on the environment while reducing costs (selecting design features that improve patient outcomes, thereby reducing hospital stay lengths and the associated costs).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The University of Queensland, Sustainable Infrastructure Research Hub.