
Abstract
This discussion examines the fundamental premise of the Maggie's Centre care philosophy, its success, and why North America has yet to accept this innovative, non-medicalized healthcare paradigm. This UK-based network of 26 centers, the first having opened in 1996, has garnered international attention for innovative architecture, in an orchestrated synthesis of built form with the therapeutic affordances of nature. A Maggie's Center is a distinct community-based healthcare building type for the provision of non-hospital-based counseling and related wellness treatment for women diagnosed with cancer and others coping with cancer. These centers have been built on two continents and typically designed by internationally renowned architects. Numerous peer-reviewed published studies have addressed these centers’ social, behavioral, and physical environment attributes and qualities through a broad-based post-occupancy assessment lens. It is hypothesized that this research collectively has been, to date, insufficiently rigorous, methodologically. This may account, to a certain extent, for why the medical establishment in North America has not yet grasped the healing and spiritual affordances of the Maggie's concept nor the attempt to uniquely incorporate architecture as a therapeutic modality. In response, three interdependent influencing factors (determinants) are presented with respect to three core constituencies of the Maggie's Centre concept with the aim of stimulating further discourse. The evidence-based health design research community, laypersons, cancer patients, survivors, and others suffering from sickness and disease, together with the medical community, can collectively foster further acceptance of this innovative building type for health.
A unique building type for health—the Maggie's Centre—has garnered significant public support over the past 25 years. In 1995, Maggie Keswick Jencks first wrote of her difficult personal experience coping with breast cancer over a prolonged 7-year struggle, enduring multiple cancer diagnoses and treatments, a period of remission, and recurrence. She envisioned an alternative place to the institutionality of the acute care hospital, a new type of place to be wholly dedicated to complementary wellness counseling and physical activities to foster self-empowerment for women and any others who are coping with cancer, as a non-medicalized alternative building type. These would be places without medicalized care, i.e., no on-site nurses and physicians, places that embrace the historically suppressed role of women and others in mainstream hospital architecture who have felt uncared for from the standpoint of emotional and psychological support. This was not the first time this impulse had appeared in the modern era: the freestanding women's maternity hospitals constructed in North America in the late 19th- and early 20th-century urban cores stood as strong symbols of care and concern for women's specialized health needs (Adams, 2008), as did the first modern-era hospice, initiated by the cadre of Nightingale-trained female nurses who opened the first in-residence hospice at St. Joesph's Hospital (1910) in London, UK (Verderber & Refuerzo, 2020).
The global modern hospice movement embraces all who are experiencing the final stages of terminal illness. In the case of hospice, in particular, the architectural result is typically a quasi-domestic type—one that is aesthetically residentialist—broadly expressive of the late 20th-century New Residentialism in healthcare architecture. It has been a direct reaction to the austerity of the generation of modern megahospitals constructed in the post-World War II decades. The megahospital by the 1970s would became a target for its aesthetic minimalism, impersonal scale, and technological obsessiveness (Verderber, 2025; Verderber & Fine, 2000). The New Residentialism arose in the 1980s among architects and forward-thinking clients who sought a sharp break from the megahospital. In keeping with this reactionary movement in healthcare architecture, a Maggie's Centre is an informal drop-in refuge, distinctly liberated and architecturally unencumbered from the burdensome functional and technical complexities of the acute care hospital-based medical center. The first Maggie's Centre, which opened in Edinburgh, Scotland (1996), was designed by the renowned architect Frank Gehry. Charles Jencks, the late imminent architectural historian (and Maggie's husband), would establish the Maggie Keswick Foundation, following Maggie's passing in 1995 at age 53 (Jencks, 2015, 2017). It was he who marshalled the talents of a cadre of distinguished architects to design the first wave of Maggie's Centres in the UK. To date, 28 Maggie's Centres have been built, yet none in North America. Their design attributes have been variously described as exceptional, unconventional, spiritually uplifting, therapeutic, psycho-emotive, and atmospheric (Martin et al., 2019; Van Der Linden et al., 2016). An exhibit, organized by the New York School of Interior Design and curated by the Carnegie Museum of Art in Pittsburgh, was held in 2014. This exhibit, Maggie's Centres: A Blueprint for Cancer Care, showcased the work of Frank Gehry, Piers Gough, Steven Holl, Rem Koolhaas, and Richard Rogers and provided insights into how these influential architects sought to positively alter the look, and more significantly, the atmosphere and feel, of healthcare facilities. Particular emphasis in the exhibit was placed on the incorporation of key therapeutic affordances of nature and landscape and for the buildings in the exhibit having received praise in the architectural and cancer care communities (Kallaway, 2011; Moore, 2021).
Why Are There No Maggie's Centres in North America?
In what ways might a community benefit from a Maggie's Centre? It provides a type of care that is generally unavailable in an acute care hospital. The focus is much more holistic. The individual who has cancer or is in remission is not treated as a “patient.” All Maggie's Centres are designed based on the same foundational architectural brief, which is a document provided by the Keswick Foundation to each commissioned architectural firm and its various project consultants (Maggie's Cancer Centres, 2015, 2025a, 2025b). This brief is then reinterpreted at the local level by the administrative staff of the future Maggie's Centre in consultation with local healthcare professionals, the design team, and additional input provided by grassroots cancer care advocates. The intent is for each Maggie's to feature, if not showcase, its architect's personal aesthetic vision and vocabulary, together with that of the commissioned landscape architect. Architects’ and general architectural/engineering (A/E) fees are paid by the Keswick Foundation in conjunction with local philanthropic fundraising.
The 28 Maggie's Centres built to date are located in five countries, with 24 in the UK and one each in Hong Kong, Tokyo, Barcelona, and Groningen (the Netherlands). They are designed by renowned architects, including the aforementioned Frank Gehry, in Scotland, and a second designed by Gehry, in Hong Kong (2013), Zaha Hadid (Kirkcaldy, UK, 2006), Snøhetta (Aberdeen, Scotland, 2013), Steven Holl (London, 2017), and Marlies Rohmer in collaboration with the renowned landscape architect Piet Oudolf (Groningen, 2024). It is no coincidence that no large, specialized “healthcare” architectural firms have been commissioned to date. By contrast, the architects selected are known for their highly intuitive, one-off designs that, often spectacularly, stir the soul, such as Gehry, who garnered world renown for his expressive Guggenheim Museum in Bilbao, Spain. Its subsequent “Bilbao Effect” has come to characterize his built work. As for the late Hadid (1950–2016), many of her adventurously designed buildings have become legendary.
Maggie's Centres are relatively small in physical stature and typically has one level. They are frequently somewhat sequestered, decidedly architecturally distinct from the world of affiliated acute care medical centers. Their imagery, scale, and ambiance seek to thread the transition from the structured reality of cancer treatment to the unstructured template of one's everyday life. Furnishings and artworks are chosen to reinforce a quasi-domestic, inviting informality—expressed in their residentialist scale and atmosphere. A diverse array of design approaches across this network of kindred facilities has been crafted by high-profile architects known for intuitively interpreting the spirit and functionality embodied in the aforementioned provided functional brief. As an aside, anecdotal qualitative evidence, including this author's site visits to six Maggie's Centre case studies in the UK in 2024 (Verderber, 2025), suggests that their contemporary design has been viewed positively by most occupants and staff. However, some staff have expressed the opinion to this author that a small percentage of visitors at first have thought of the centers as architecturally a bit off-putting, “too modern,” and even a bit intimidating due to their expressive unconventionality, with some open plan spaces lacking in personal privacy. The aim of the following discussion is to present three influencing factors that possibly account, either individually or collectively, for why there still are no Maggie's Centres in North America. Each determinant is individually discussed. All three possible influencing factors, together with the transactive space they share, are illustrated in Figure 1.
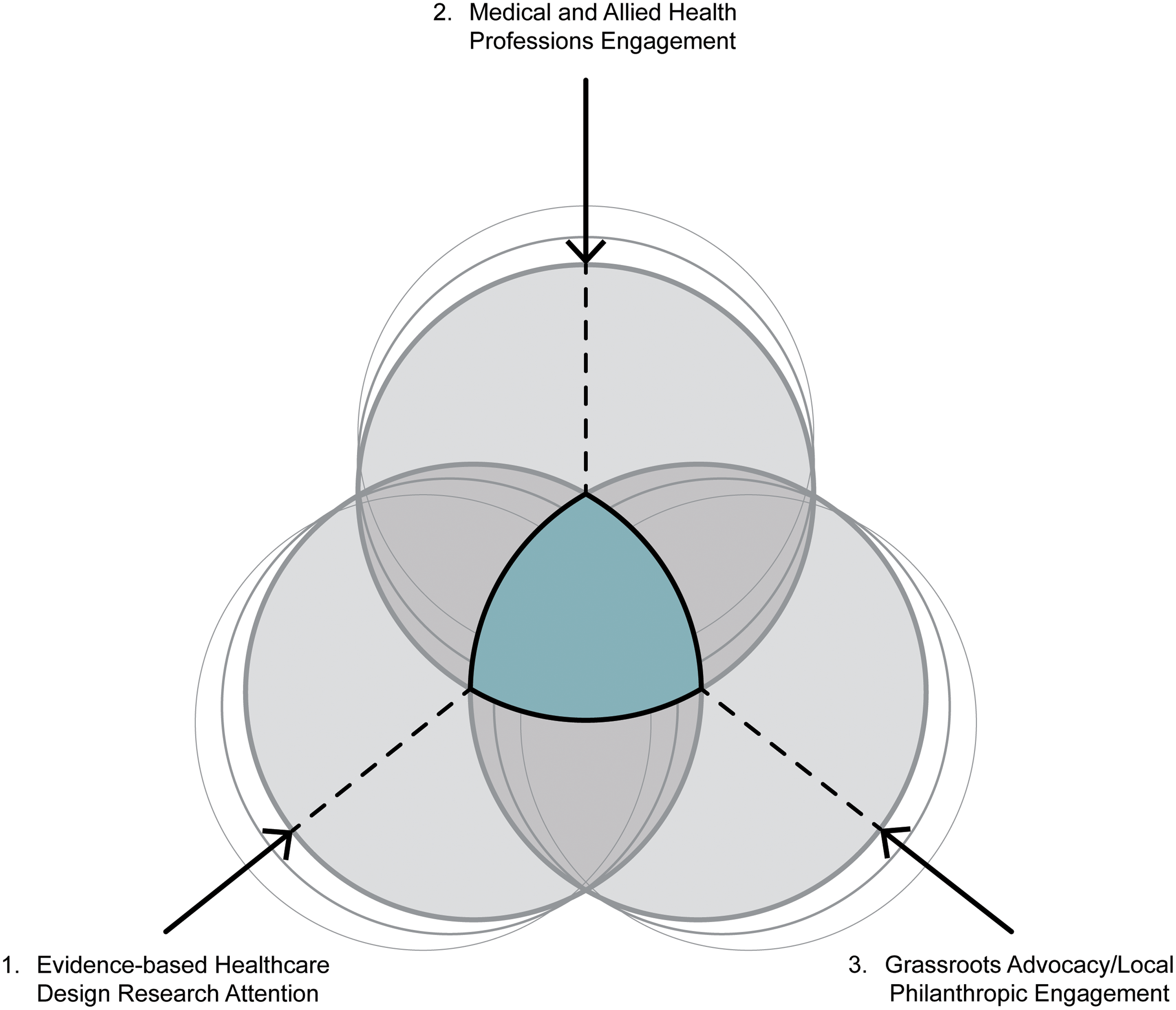
Transactive Space Between Influencing Determinants.
More Rigorous Evidence-Based Research as Catalyst
Key Question: What type of evidence-based design (EBD) research on Maggie's Centres is most needed at this time?
A field research has been conducted in various Maggie's Centres, utilizing the aforementioned mixed-method post-occupancy assessment methodologies. These assessments mainly consist of documentation of the in-use efficacy of the physical setting and its immediate exterior environs by means of surveys, interviews, and focus groups with the bulk of data being principally qualitative. One recent meta-analysis, methodologically filtered through the lens of biophilia theory, identified a number of key Maggie's attributes: their human scale, biomorphic physical properties, semi-open plan interiors, abundant natural light and ventilation, skylights and clerestories, interesting views outward, and emphasis on indigenous vernacular construction materials in construction. Their strong spatial connectivity with nature and landscape has been noted, along with the presence of fireplaces, centrally located kitchens with large family-style dining tables, and varied informal, spacious countertop seating areas. Multisensory opportunities for occupants to engage in prospect-refuge behaviors with nature and landscape have also been cited (Tekin et al., 2023). In a qualitative investigation of the therapeutic properties of the adjacent gardens at 10 Maggie's Centres, key aesthetic and functional layout attributes were found to be integral in fostering a positive psycho-emotive experience (Butterfield & Martin, 2016). These findings are not atypical across the growing body of published peer-reviewed EBD literature on Maggie's Centres (Annemans et al., 2012; Frisone, 2024).
It is noteworthy that, to date, there is no published evidence that any Maggie's Centre have explicitly incorporated evidence-based design EBD research findings. It is equally worth noting that this contrasts with the oft-stated mission of EBD research, which, first and foremost, is to incorporate, in the earliest stages of the design process, results available from high-quality evidence-based data (Center for Health Design, 2009; Sackett et al., 1996). Moreover, it continues to be erroneously assumed in some quarters that Maggie's Centres are in fact designed based on empirically based EBD research (Allen & Macomber, 2020; Putievsky-Pilosof & Grobman, 2021). This seems to not be the case. Interestingly, as for the EBD research published to date on Maggie's Centres, it has not focused on quantifiably ascertainable, precise, direct health outcome metrics, metrics having either an adverse or positive causative effect on occupant well-being or health status outcomes. However, at least 14 Maggie's Centres have been subjected, as of this writing, to some degree of systematic on-site post-occupancy environmental assessment. In actuality, the published studies to date have almost singularly addressed qualitative occupant satisfaction data. This disregard for analyzing direct health outcome metrics is exemplified in one recent study. It focused on occupant comfort metrics measured in two Maggie's Centres in the UK. The study found that large windows and shallow roof eaves allow excessive thermal gain (Namakula et al., 2023). This stand-alone finding was then extended to broadly imply that these two buildings are deemed uncomfortable in this regard by their occupants, without the researchers having directly observed, interviewed, or surveyed a single person in either of these Maggie’ Centres and without soliciting any type of outcome data, i.e., frequency of visits, recovery rates, staff turnover or absenteeism, or psychological well-being.
Will only more rigorous, causal, “harder data” that address direct health outcomes and staff performance metrics attract the serious attention of the medical and philanthropic communities in North America? Nonetheless, viable EBD research strategies exist at present which provide a useful roadmap to address the (possible) dilemma of perceived non-rigorousness. These represent a continuum from subjectivity, at one end, to rigorous objectivity on the other. Methodologies associated with various stages along this continuum include building type precedent analysis, systematic on-site post occupancy assessment, analysis of case studies, focused interviews, ethnographic investigations, quantitative surveys, controlled observational studies, quasi-experimental studies, and randomized controlled trials (Haj, 2013; Harris et al., 2008; Viets, 2009). This work can be designed to be one of two methodological types. First, comprehensive, longitudinal assessments can be conducted across the entire current Maggie's network. Second, in-depth case study methods can focus on occupants’ outcomes across a facility subset. In other words, more quantitatively based post-occupancy assessments are needed, assessments linked with specific health and staff performance outcome metrics whether conducted in only a few or across the entirety of the Maggie's Centre network (Figure 1).
Support of the Health Professions as Catalyst
Key Question: What is required to spark interest in this building type within the health science professions in North America?
Rigorous, systematic EBD research on the existing Maggie's network may result in the medical and allied health communities becoming interested in building one or more Maggie's Centres in North America. More specifically, the types of studies that can accrue a higher degree of “research agency” might include the following types of longitudinal studies: (1) assessment metrics across a period of months, to determine whether a client's number of visits and the length of duration per visit results in a higher personal heightened self-sense of empowerment (agency) in coping with one's personal health status; (2) assessment metrics whereby the analysis of client visits does (or does not) result in a more rapid rate of health status improvement while actively undergoing medical treatment, i.e., 62% of clients who visited their local Maggie's once per week for 2 hours or more per session over a period of 4 months experienced a significantly higher rate of cancer remission compared to patients who did not visit; (3) assessment metrics conducted systematically on staff attitude and outlook, work performance, and job productivity from the standpoint of these factors’ possible impact of their interactions with the physical setting and its immediate site environs, i.e., 44% of the staff surveyed across 12 program sites in the UK reported that the quality of the physical setting has a “very pronounced” impact on one's day-to-day well-being and performance; 36% of staff interviewed indicated a high level of job satisfaction with their Centre's greenhouse and its adjacent outdoor gardens. Or, for example, Maggie's Centres located in large cities experience a 35% higher rate of staff turnover after a period of 1 year compared to their counterparts in small-town and rural settings. Examples such as these of more in-depth EBD design research rigor and occupant outcomes are recommended if the philanthropic, medical, and allied health professions in North America are to perhaps become intellectually engaged and professionally vested in Maggie Keswick's initial vision and in seeing it brought to their own community (Figure 1).
Support from Community-Based Cancer Treatment Advocates as Catalyst
Key Question: How to foster enthusiasm and collective agency on the part of a local community-based advocacy group to procure its own Maggie's Centre?
As to the question of facility procurement, as mentioned above, this has nearly always required partnering with an affiliate medical institution located in close geographic proximity to one or more available sites where a Maggie's Centre could feasibly be constructed. In the UK, most Maggie's Centres have been built on public land parcels owned and provided by the nearby partnering local health trust. In the case of Canada, where virtually all hospital-based medical centers are publicly owned, it would currently not be possible to build a private-sector health-related facility on available public land. In the US, however, the land acquisition scenario is often different: a private-owned hospital-based medical center would have comparably few, if any, such land ownership or legal restrictions. In any case, a suitable site is purchased or donated, one ideally in walkable proximity to the affiliated medical center. It is important to foster a mutually productive relationship, a partnership to the extent possible in order to garner the fullest degree of agency, i.e., support, from the affiliated actor-institution.
Strategic planning is a process through which an organization agrees on and builds key stakeholder commitment to priorities deemed responsibly essential to its mission and to its organizational environment. Strategic planning guides the acquisition and allocation of resources to achieve these priorities. It is highly important to not eschew difficult or sensitive questions, to focus on the most important priorities, to produce a formal document, and to ensure this document is linked to annual workplans with clearly definable outcomes (Allison & Kaye, 2015). In the present scenario, the organizational mission statement is provided a priori with further particular goals and objectives to be defined subsequently at the local level. This process can be initiated by conducting due diligence with key decision-makers at all levels of government and with local community leaders. This can occur after having first assembled a “vision team” to champion the cause and identifying a volunteer-based board of directors to guide the building procurement process through the many stages that lie ahead. It will be important to carefully monitor daily operations once construction is completed following initial occupancy together with ongoing operational budgets by means of accepted facility management performance metrics.
A formal fundraising organization or trust is essential as the main vehicle for courting and onboarding local philanthropic support. The affiliate medical campus's political agency and fiduciary resources can be of great assistance from the earliest stages of building procurement. An obvious item of importance early on is carefully selecting the architectural firm, because descriptive architectural and landscape renderings and models can be critical to a successful fundraising drive. It is important to be aware of the fact that no two Maggie's Centres are precisely the same. That said, the operative assumption is that Determinant 1 will activate Determinant 2, with both functioning in concert to activate proactive leadership engagement at the local community level (Determinant 3). In 2023, the Keswick Foundation's total income was £32,301,000 (US$43,470,685). This total included all fundraising activities, legacies and trust donations, corporate sponsorships, and Facebook challenges. Of this total, £23,917,000 (US$32,187,498) was spent on building new centers and in refurbishing existing ones, in providing daily operational expenses, and in-person and online support programs across the Maggie's network (Maggie's Care Centres, 2025b).
It is important to be aware of the fact no two Maggie's Centres are precisely the same. The operative assumption is Determinant 1 will activate Determinant 2, with both functioning in concert to activate proactive leadership engagement at the local community level (Determinant 3).
Successful Keswick Foundation fundraising activities conducted during the recent COVID-19 lockdown in the UK included a “Maggie's Culture Crawl” whereby donors across the UK became sponsors of individual cancer patients (Maggie Keswick Jencks Cancer Caring Centres Trust, 2022). Often, it is the family of a loved one having been lost to cancer that spurs a large donation or through a corporate foundation bequest in the name of the founder of a local business lost to the disease. Well-known figures in the world of sports have donated significant sums to the Keswick Foundation in the UK for facility construction costs. In 2024 alone, 327,405 visits occurred across the total Maggie's network, including 226,000 visits from persons with cancer and over 101,000 visits from their friends and loved ones (Maggie's Cancer Centres, 2025a). These and other efforts have proven effective in garnering local fiscal support and symbolize a far broader movement to promote population health in a rapidly changing world (Boston Women's Health Book Collective, 1998). The overlapping interdependency between this third determinant and the other two determinants is illustrated in Figure 1.
The Future
This discussion has sought to highlight challenges as well as opportunities inherent in procuring one or more Maggie's Centres for construction in North America. Will Maggie Keswick Jenck's initial vision yet inspire the construction of the first Maggie's Centre in North America? While not intending to inadvertently conflate very dissimilar building types—acute care hospitals with Maggie's Centres—the unencumbered quasi-domestic residentialist architecture of the Maggie's concept holds enormous potential to positively impact North American healthcare architecture. Nevertheless, one might ask: “Aren’t there already numerous non-medicalized, non-fee drop-in day counseling programs in many places that already provide services comparable to what a Maggie's Centre provides?” In fact, yes, many communities have such programs, such as the Gilda's Club drop-in centers in the greater Toronto metropolitan area, which were inspired by Gilda Radner's courageous battle against cancer. The main difference, however, is expressly architectural. Although Gilda's and other drop-in day facilities for cancer patients undoubtedly provide excellent counseling, they do not self-consciously express a comparable synthesis of built environment aesthetics with unencumbered informality in architecture for health.
While not intending to inadvertently conflate very dissimilar building types—acute care hospitals with Maggie's Centres—the unencumbered quasi-domestic residentialist architecture of the Maggie's concept holds enormous potential to positively impact North American healthcare architecture.
In theory, the moment of synergy and subsequent action becomes possible when all three influencing determinants presented in Figure 1 are in relative interdependency and synchronicity. The three discussed here are not weight-ordered in terms of priority, because no two scenarios will be alike. It is assumed any one of these determinants could be the primary driver in a given community. The collective energy embodied in all three when functioning in synchronistical alignment is translatable, providing energy to fuel participating actor-agents in the procurement process. Much is possible when all key actor-agents are focused on the same end goal. This is the space illustrated in the shaded center at the heart of Figure 1. This is not to imply, however, that a host of other influencing factors does not also shape the facility procurement process. Additional influencing determinants include challenges inherent in attaining carbon neutrality in architecture, cost containment, offsite prefabrication, critical regionalist concerns embracing an architecture of locality, cultural appropriateness, the gathering together of local political support, ethical concerns associated with environmental conservation and site remediation challenges and, importantly, an anticipation of any future medical science breakthroughs—specifically in the realm of cancer care and treatment.
These influences will likely surround a core nexus of concern in establishing productive, sustainable partnerships, meaningfully engaging and instilling actor-agency within the local medical and allied health communities, engaging local elected officials, instilling agency among influential local and community health advocate-leaders, and fostering philanthropic actor-agency leadership at the local level. Procuring a newly built building for healthcare is a daunting prospect, and synchronistic alignment of internal with exogenous determinants typically takes far longer than initially anticipated. But without focused strategic thinking combined with sheer perseverance, little is achievable.
Regarding the function of EBD in healthcare architecture, in recent years, it has experienced broader adoption in many everyday professional practice contexts, a positive development (Levin, 2023). But in some quarters, EBD for healthcare design has acquired a concurrent critique for being too rigid and prescriptive (Lundin, 2015). Yet this is a problem also persisting in the health science professions (Feres et al., 2020; Oliveira et al., 2021). Perhaps the same inertia persists whereby it will take more effort to convince the medical establishment in North America of the value-added proposition of a local Maggie's Centre. As for architectural practitioners, many believe that EBD for health remains inherently retrospective, whereas designers by contrast are trained to function in practice as forward-thinkers oriented to the future as a requisite condition for their aesthetic imagination and professional success (Peavey & Vander Wyst, 2017). This presents an open question: does the incorporation of EBD knowledge for healthcare necessarily enhance or inhibit creativity (Brandt et al., 2010)? A balance is recommended representing a thoughtful, compassionate blend of personal experience and intuitive design with rigorous research-based knowledge although the construction of one or more Maggie's Centres in North America will likely rest primarily on philanthropic leadership.
Implications for Practice
An overview of the network of 26 Maggie's Centres, the first having opened in the UK in 1996, is briefly presented, as an emerging, informal, non-medicalized building type for health in the 21st century.
This building type expresses imaginative architectural and landscape design work of noted design professionals, and the buildings have garnered public acclaim. However, no Maggie's Centres have been built in North America, and possible reasons for this are discussed.
A call for more extensive evidence-based design research is made, as one key strategy to further substantiate the physical setting attributes and behavioral affordances associated with this emerging building type for health.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.