
Abstract
Objective:
To identify, examine, and map the characteristics of knowledge of nature-based design in stroke rehabilitation facilities, examine how research in this field has been conducted and identify gaps in knowledge.
Background:
Many stroke survivors have wide ranging impacts, resulting in long hospital stays to undertake rehabilitation. The physical environment can influence brain recovery; however, there is limited evidence to support the design of effective rehabilitation environments. Conversely, the health benefits available from connection with nature are well established. A nature-based design approach may have benefits and implications for the physical environment of inpatient stroke rehabilitation facilities; however, it is unclear what evidence exists in this field.
Method:
This scoping review followed the JBI methodological guidance for the conduct of scoping reviews, with systematic searches of six databases.
Results:
Twenty-eight studies were included in the review. Aims and research methods varied widely. Investigations in 19 studies related to gardens and other designed outdoor nature-based environments. Other studies explored natural analogues, nature inside, inside/outside connections, and the natural environment. Findings from the studies were spread across the fields of design, use, exposure to, and engagement in nature-based environments.
Conclusion:
The characteristics of knowledge underpinning nature-based design in stroke rehabilitation environments are highly diverse, and significant gaps exist in the evidence base. A framework developed during this review for mapping knowledge on the intentions and impacts for spaces and services in this field assisted to identify these gaps and may be applied to other areas of healthcare design research.
Globally, the number of people living with the after effects of stroke has nearly doubled in the last 30 years and is now estimated to be over 101 million, making stroke a leading cause of disability (Feigin et al., 2022). Stroke survivors may experience impacts in their ability to perceive, understand, communicate, move, and interact with the world around them in unique combinations, depending on the area of the brain injured during the stroke event (Stroke Foundation, n.d.). An essential part of stroke recovery is rehabilitation, defined as “a process of active change by which a person who has become disabled acquires the knowledge and skills needed for optimum physical, psychological and social function” (Bernhardt et al., 2017). The stroke rehabilitation process is complex, involving active engagement of the stroke survivor, their family or caregivers, and expert clinical and support staff using stroke-specific treatments and care (Saa et al., 2023). Researchers have shown depression is common poststroke (Chun et al., 2022) and many patients in rehabilitation experience significant periods of inactivity (Sjöholm et al., 2014), boredom, and low stimulation (Kenah et al., 2022; Luker et al., 2015), which may hinder their progress.
To undertake rehabilitation following stroke, patients often face long stays in hospital. For instance, in Australia in 2022, the average length of stay for a stroke survivor in rehabilitation care was 27.9 days, 5 times that of the average hospital stay (Australasian Rehabilitation Outcomes Centre, 2022). Healthcare settings impact the health and well-being of those who use them (Zhang et al., 2019), and longer stays increase exposure to these environments. Researchers have established that the physical environment has a role to play in supporting rehabilitation (Smith & Macdonald, 2015); however, some hospital-based stroke rehabilitation settings underutilize this valuable resource. Contributing factors to this underutilization include a limited evidence base (Bernhardt et al., 2022; Colley & Zeeman, 2020) and a lack of alignment between clinical practice guidelines and hospital design guidelines (Saa et al., 2023).
With considerable evidence currently available of the broad health benefits of contact with nature (Kuo, 2015), gardens, green spaces, and biophilic design in healthcare settings are receiving increasing attention (Abdelaal & Soebarto, 2019; Tekin et al., 2022). Recent studies have documented a range of benefits within healthcare settings, including for people with mental health conditions (Carlson et al., 2020), cancer patients (Blaschke et al., 2017), aged care residents (Sugiyama et al., 2022), families of patients in intensive care units (Ulrich et al., 2020), and nursing staff on breaks (Cordoza et al., 2018). Nature-based environmental design also has potential to improve rehabilitation experiences and outcomes for patients, families, and staff. Outdoor spaces and views of nature have been noted as important means to support emotional well-being and encourage physical, cognitive, and social activities, core functions of rehabilitation to promote brain recovery (Lipson-Smith et al., 2019). However, a recent systematic review of built environments for inpatient stroke rehabilitation found gaps in knowledge, including no targeted research on the impact of outdoor spaces (Lipson-Smith et al., 2021) and it is unclear what evidence exists for other nature-based design in these settings.
Incorporating contact with nature into multifaceted healthcare environments presents challenges but may be informed by the framework of biophilic design. Developed over several decades in response to perceived distance from nature within the built environment, biophilic design aims to enhance and restore beneficial experiences of nature (Kellert, 2018). In seeking to assist the application of biophilic design, Kellert defined three core aspects: direct experience of nature through contact with the elements of the natural environment, such as light, plants, or water; indirect experience of nature via representations of the natural world and its processes, for instance, using nature-based images, patterns, colors, materials, or other simulations of nature; and experience of space and place, for instance, balancing complexity and order, use of sheltered spaces with distant views, transitional spaces, and ecological and cultural connections to place. Each of these may occur in a range of indoor and outdoor spatial contexts; however, it is unclear what knowledge is available to underpin the application of these concepts in the spatial context of inpatient stroke rehabilitation, what research methods have been used to study their impact on stroke patients, their families and staff, and what gaps there are in the knowledge base.
The objectives of this review were to identify, examine, and map the range and characteristics of knowledge about nature-based design in stroke rehabilitation facilities, examine how such research has been conducted, and identify gaps in knowledge. Incorporating the elements defined by Kellert (2018) as noted earlier, this review of nature-based design includes nature and biophilic design indoors, gardens and other nature-based outdoor spaces, and spatial and place-based design aspects, which enable connection with nature, such as transitional spaces, ecological, and cultural qualities. The research questions were: What are the scope and characteristics of knowledge underpinning nature-based environmental design in stroke rehabilitation or related facilities? What research methods have been used to study the impact of nature-based design in these settings on patient, family, and/or staff outcomes? Are there gaps in the research on the design of environments incorporating contact with nature in stroke rehabilitation?
Method
A scoping review is useful for emerging research areas with unclear evidence to identify and map the existing scope, examine how research has been conducted, and identify gaps in knowledge (Munn et al., 2018). A preliminary database search found no systematic or scoping reviews on this subject. This review was conducted following the JBI methodological guidance for scoping reviews (Peters et al., 2021). Steps in this method include preparation of a protocol, identification of review questions, identification of inclusion criteria and search strategy, screening and selection of studies, data extraction, data analysis, and presentation of results. A protocol (Seale et al., 2022) was lodged in an online repository prior to conduct of screening.
Study Identification
Search concepts (refer Table 1) and strategies were developed in discussion with research librarians and tested prior to conduct of the final searches. Inclusion criteria are shown in Table 2, and a sample search strategy is included in the Supplemental Material. Electronic databases, including Ebsco Academic Search Complete, Ebsco Cumulative Index to Nursing and Allied Health Literature Complete, Ebsco Medline Complete, Embase, Scopus, and Web of Science, were searched on August 2 and 3, 2022, with search terms adapted to suit each.
Search Concepts.
Inclusion Criteria.
Study Selection
All identified citations were uploaded into Covidence systematic review management software and duplicates checked by one reviewer. Study titles and abstracts were independently screened by two reviewers, full texts of selected studies retrieved, screened independently by two reviewers, and discrepancies discussed until consensus was reached. Articles without nature-based design in the physical environment for inpatient stroke rehabilitation were excluded, for instance, six studies on indoor horticultural therapy for stroke patients with no setting description were excluded. Studies with collective patient groups, such as people with neurological disability (Lakhani et al., 2019) or acquired brain injury (Vibholm et al., 2020), had full text and citation checks completed, and those in which the specific inclusion of stroke could not be confirmed were excluded. Upon review of the preliminary selection, the protocol was revised to include scoping and narrative reviews by agreement of all reviewers. The reference lists of all selected studies were checked for relevant literature and additional studies included, with initial handsearching completed in March 2023. An additional hand search was conducted in January 2024 to update this study during final revisions. As this is a scoping review, critical appraisal was not undertaken (Peters et al., 2021).
Data Extraction and Analysis
Data relevant to answering the research questions were extracted into a customized form (refer Supplemental Material) using Covidence software. Charting was completed by one reviewer and independently checked for completeness by a second reviewer. The extracted results of the included studies were analyzed using basic qualitative content analysis in order to answer the first research question to identify the characteristics of the existing evidence (Pollock et al., 2023) and to accurately describe gaps in knowledge. Open coding was carried out on the extracted results and four main categories were developed. The remaining extracted data were analyzed descriptively.
Results
Database searches identified 7,156 records. Initially, 3,609 duplicates were removed; then, title and abstract screening excluded 3,509 studies. Full texts for 38 studies were retrieved and reviewed for eligibility, with 16 found to be eligible for inclusion. Handsearching of citations from the included studies yielded 11 further articles after screening by two reviewers. The second hand-search to update the study found four potential articles, but upon screening by two reviewers, only one was found to qualify for inclusion bringing the total number of included articles to 28. Refer Figure 1.
Identification and screening flow diagram.
This review aimed to establish the scope of knowledge underpinning nature-based design for stroke rehabilitation environments, the methods used to study this phenomenon and identify gaps in knowledge. The results are shown in Table 3 and this section highlights the key characteristics.
Characteristics of Included Studies.
Study Aims
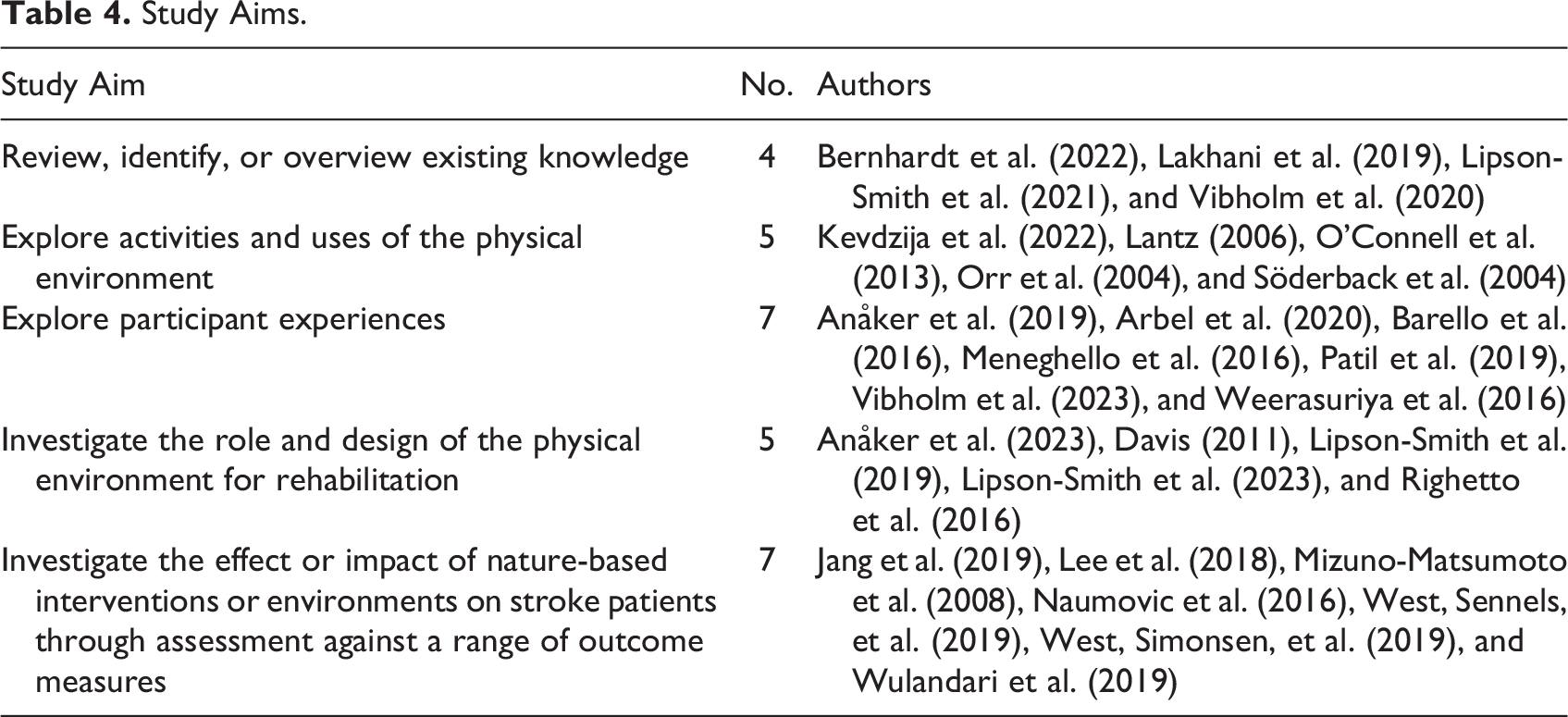
Aims stated in the included studies varied, encompassing review or overview of existing knowledge, exploration of use of the physical environment, exploration of participant experiences, exploration of the role and design of the physical environment for rehabilitation, and investigation of the effect or impact of nature-based interventions on stroke patients through assessment against a range of outcome measures. Refer Table 4.
Study Aims.
Study Design
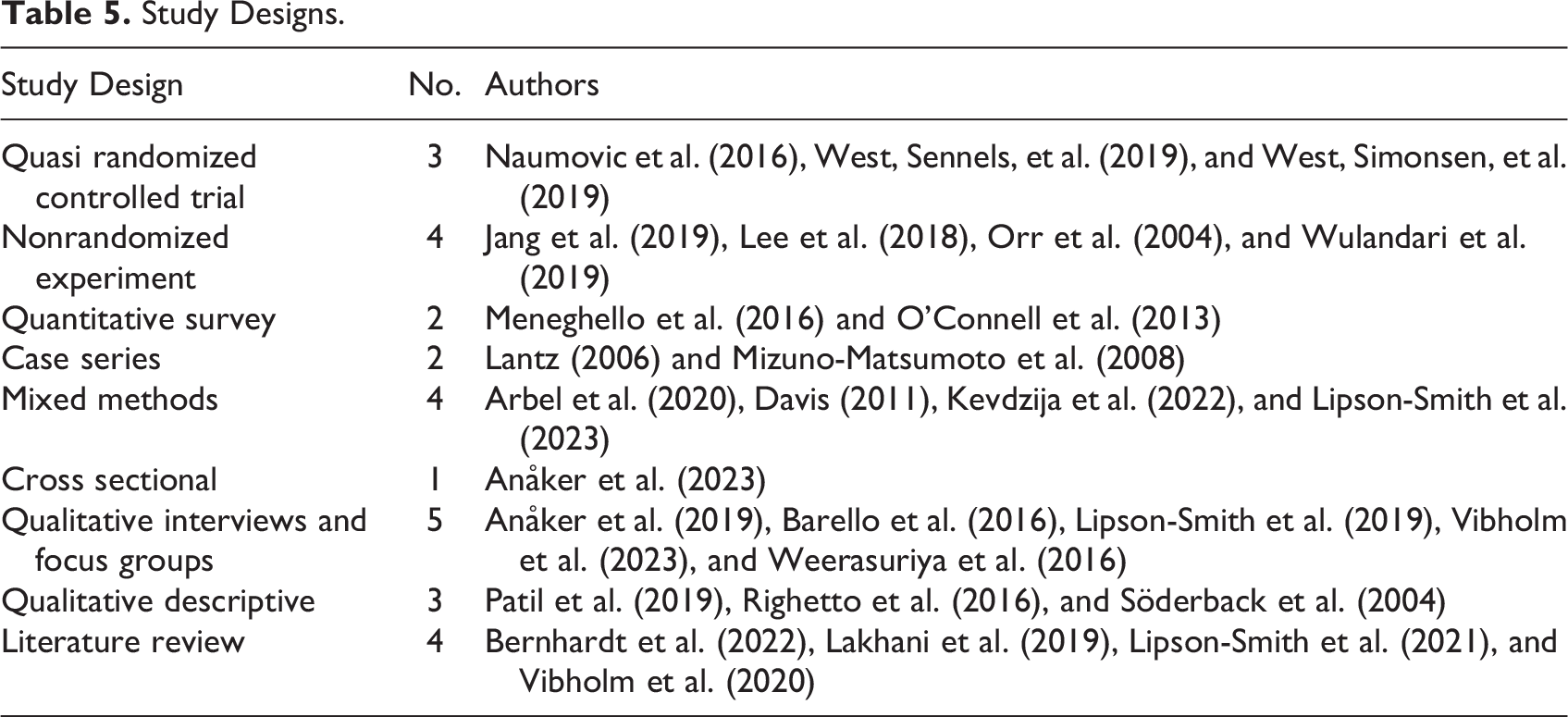
A high diversity of study designs was found across the included studies, refer Table 5. Quantitative studies used data collected through a range of standardized assessment tools, questionnaires, surveys, patient records, medical tests, and reports. Many combined more than one source of data and used statistical analysis methods. Three studies with experimental designs reported use of participant randomization without blinding and no fully blinded studies were found. Qualitative studies collected data via interviews, focus groups, medical records, and therapists’ notes. Mixed methods studies had varied designs, combining quantitative and qualitative data sources noted above and additional methods, including behavioral observation and mapping, patient shadowing, walk-through semi-structured interviews, physical environment checklists, and logbook. Literature review methods included systematic reviews, a scoping review, and a narrative review.
Study Designs.
Participants
Participant numbers in original research studies ranged between 2 and 76. In line with the inclusion criteria, all studies included people undergoing inpatient rehabilitation following stroke, their families, visitors, and/or staff involved in their care and therapy. Additional participants noted in seven original research studies included other inpatients, outpatients, designers, academics, and/or healthcare policy makers (Davis, 2011; Jang et al., 2019; Lipson-Smith et al., 2019; Meneghello et al., 2016; Orr et al., 2004; Söderback et al., 2004; Weerasuriya et al., 2016). Exclusion of patients with specific impairments or conditions was noted in eight original research studies (Anåker et al., 2019; Arbel et al., 2020; Kevdzija et al., 2022; Lipson-Smith et al., 2023; O’Connell et al., 2013; West, Sennels, et al., 2019; West, Simonsen, et al., 2019; Wulandari et al., 2019), for instance, stroke patients with dementia, other severe cognitive impairments, psychiatric disorders, aphasia, dysarthria, or impaired hearing which prevented participation in an interview were excluded in one study (Arbel et al., 2020).
Aspects of Nature-Based Design
This review identified five areas of nature-based design within physical environments for stroke rehabilitation contained in original research studies, refer Figure 2, encompassing: (1) simulations or natural analogues inside hospitals such as lighting which mimics the color and intensity of sunlight (West, Sennels, et al., 2019; West, Simonsen, et al., 2019) and nature-based audio–visual displays (Arbel et al., 2020; Wulandari et al., 2019), (2) nature inside comprised of indoor plants and horticultural material (Anåker et al., 2019, 2023; Jang et al., 2019; Kevdzija et al., 2022), (3) inside/outside connections such as views and access outside (Anåker et al., 2019; Davis, 2011; Kevdzija et al., 2022; Lipson-Smith et al., 2019, 2023), (4) designed nature outside consisting of hospital gardens and green spaces (Barello et al., 2016; Davis, 2011; Lantz, 2006; Lee et al., 2018; Lipson-Smith et al., 2019, 2023; Meneghello et al., 2016; Mizuno-Matsumoto et al., 2008; O’Connell et al., 2013; Orr et al., 2004; Patil et al., 2019; Righetto et al., 2016; Söderback et al., 2004; Vibholm et al., 2023; Weerasuriya et al., 2016), and (5) the natural environment including a park and lake (Naumovic et al., 2016), a fjord with spectacular views (Patil et al., 2019), forests, streams, and an inlet (Vibholm et al., 2023), and a lagoon and the sea (Meneghello et al., 2016; Righetto et al., 2016).
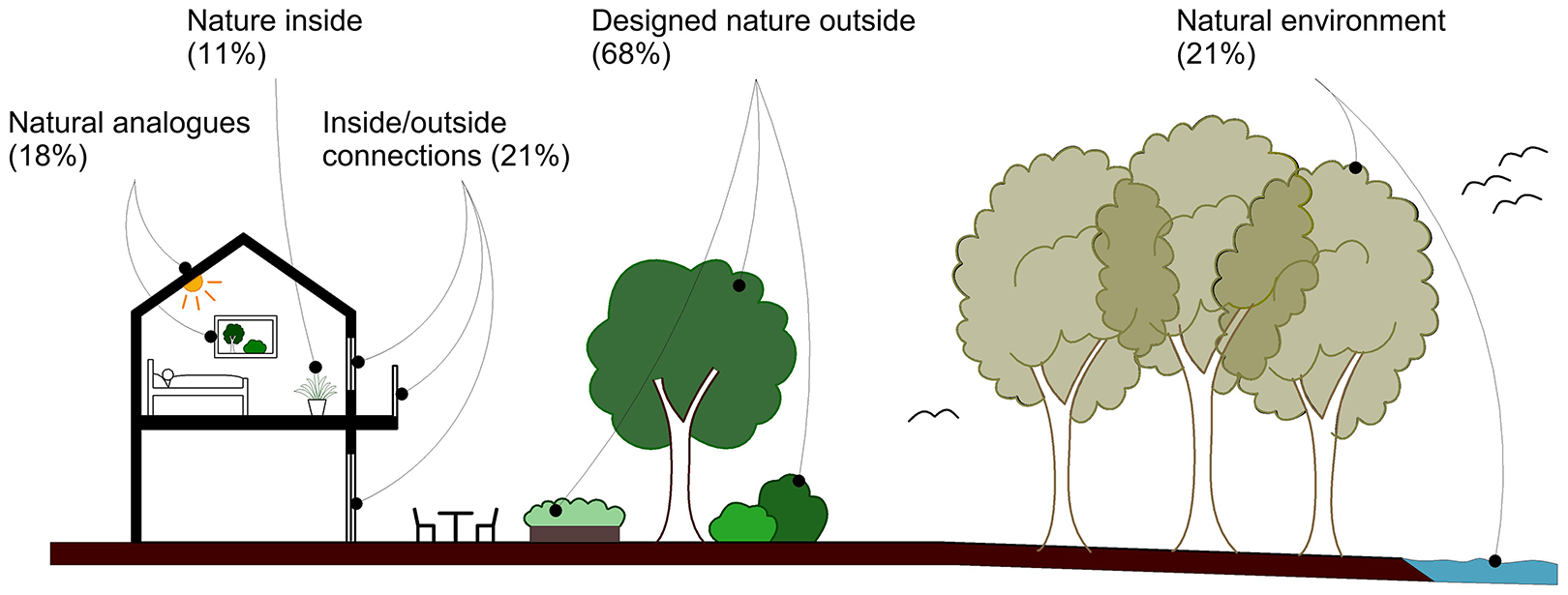
Aspects of nature-based design.
The Scope and Characteristics of Knowledge
The results from the studies were sorted into four broad categories of knowledge about nature-based environments in stroke rehabilitation: (1) intention for use of nature-based environments, encompassing the objectives, meanings, and purposes of healthcare professionals, staff, patients, and families in using these settings, as well as limitations to use; (2) impact from engagement in nature-based activities, encompassing measured outcomes, experiences, and perceived benefits; (3) impact of exposure to nature-based environments, encompassing measured outcomes and experiences of noninteractive exposure; and (4) intentions for the design of nature-based environments, encompassing design principles, design process, and the role and purpose of a range of design elements as identified by architects, designers, healthcare professionals, stroke survivors, families, and other noted study participants. The following sections outline the knowledge in each category, generally from original research studies, with any results from literature reviews explicitly identified. Some studies have results in several categories.
Intentions for the use of nature-based environments
Therapists were reported to use outdoor gardens with stroke patients as an extended therapy space (Vibholm et al., 2023), which can offer opportunities for skills training (Patil et al., 2019; Söderback et al., 2004; Vibholm et al., 2023), sensory stimulation (Söderback et al., 2004; Vibholm et al., 2023), individualized therapy (Lantz, 2006; Patil et al., 2019), purposeful, meaningful (Lantz, 2006; Patil et al., 2019; Vibholm et al., 2023), and stimulating and playful rehabilitation opportunities (Vibholm et al., 2023). Other therapy uses included: patient collaboration and socialization (Lantz, 2006; Patil et al., 2019; Söderback et al., 2004; Vibholm et al., 2023); enhancing motivation, engagement (Lantz, 2006; Vibholm et al., 2023), and a sense of accomplishment (Lantz, 2006); and improving concentration (Vibholm et al., 2023), mood, well-being, and mental health (Söderback et al., 2004; Vibholm et al., 2023).
Orr et al. (2004) found higher uptake of horticultural therapy in neurological rehabilitation patients than orthopedic, concluding it should be prioritized for those with life-changing trauma. Hospital gardens can hold symbolic and spiritual meaning for patients, families, and staff (Weerasuriya et al., 2016), provide opportunities for recreation, relaxation (Lantz, 2006; Lipson-Smith et al., 2019; Söderback et al., 2004), and social activity (Weerasuriya et al., 2016). Views of or time spent in nature or outdoors were found to be a means of escape from feelings of restriction or boredom (Lipson-Smith et al., 2023) and communal spaces with views were found to support patients’ activities (Kevdzija et al., 2022). Davis (2011) found patients valued particular elements in gardens for specific needs, such as a ball court for physical needs; the sun, sky, and plants for emotional/spiritual needs; and seating and a gazebo for social needs. Hospital gardens require staff support, funding, and maintenance (Davis, 2011; Lantz, 2006) to support use. Limitations to use include lack of awareness (Davis, 2011; Weerasuriya et al., 2016), distance (Davis, 2011; Lipson-Smith et al., 2023), inadequate signage, lack of a horticultural therapist (Davis, 2011), weather, uneven terrain, locked wards, and supervision of patients (Weerasuriya et al., 2016). Some patients are unable to access gardens during hospitalization (O’Connell et al., 2013).
Impact of engagement in nature-based activities within nature-based environments
Active engagement of stroke survivors in horticultural and garden therapy programs within nature-based environments were reported to: accelerate improvements in visual and color processing, association, and sensory-motor areas of the brain (Mizuno-Matsumoto et al., 2008); improve vascular health indices (Jang et al., 2019); improve physical skills, such as upper limb function, hand force, balance ability, fall efficacy, activities of daily living (Lee et al., 2018), and visual scanning (Lantz, 2006); and improve mental health by reducing depression (Lee et al., 2018) and stress (Jang et al., 2019; Lee et al., 2018), providing mental rest (Patil et al., 2019), relaxation, a break from the ward (Meneghello et al., 2016), and a link to the outside world (Barello et al., 2016). Motivational benefits found include a sense of achievement (Meneghello et al., 2016; Patil et al., 2019), engagement, shared experiences, connection to past (Patil et al., 2019), increased self-efficacy, choice, agency, aid to communication (Barello et al., 2016), and a link to real-life assisting patients to set goals (Barello et al., 2016; Lantz, 2006). However, a systematic review found only preliminary evidence of positive impacts on the psychosocial health of stroke survivors from engaging in the natural environment (Lakhani et al., 2019).
Impact of exposure to nature-based environments
The impact on stroke survivors of exposure to nature-based design was a third key area of knowledge. The use of naturalistic lighting, which imitates the spectrum and rhythm of sunlight in a rehabilitation ward, was reported to increase stroke patients’ plasma melatonin levels without normalizing the diurnal rhythm and to stabilize cortisol levels, with the researchers noting further studies are required (West, Sennels, et al., 2019). The same lighting was reported to reduce depression within the range of anti-depressant medication without side effects, significantly reduce anxiety, improve well-being, and possibly stabilize circadian rhythm with no significant effect on cognition (West, Simonsen, et al., 2019). Nature-based audio–visual displays in hospital rooms were reported to improve concentration and mood (Wulandari et al., 2019), and in combination with artificial skylights and adaptive daily lighting, improve user experience (Arbel et al., 2020). Plants in patient rooms were found to slightly reduce stress (Jang et al., 2019), while views of nature foster well-being (Anåker et al., 2019). Access to gardens provided patients with links to familiar environments, positive stimulation out of the ward, refuge, and perceived positive impact on recovery (Weerasuriya et al., 2016). Functional improvements in patients’ daily activities were reported after regular outings to a lakeside park (Naumovic et al., 2016).
Design intentions for nature-based environments
The fourth area of knowledge identified was design intentions. An original research study on the design of stroke rehabilitation settings found access to outdoors, green spaces, and views of nature important features with means to foster emotional well-being (Lipson-Smith et al., 2019). The same aspects of nature-based design were linked to improved physical symptoms, stress reduction, opportunities for physical and social activity for patients, and well-being for staff in a narrative review (Bernhardt et al., 2022); however, a systematic review identified gaps in the evidence base for these features (Lipson-Smith et al., 2021). Places that draw patients out of single rooms were identified as important, with access to nature and outdoors fundamental for quality of care (Anåker et al., 2019), while design principles developed for stroke rehabilitation settings include the need for variety and change in the environment and patient-centered design (Lipson-Smith et al., 2023). Patients indicated desire for a variety of common spaces with good views (Kevdzija et al., 2022) and control of stimulation levels in bedrooms (Arbel et al., 2020). Some stroke units in Sweden had real or plastic plants and/or paintings with natural motifs, but only one had a balcony with a view (Anåker et al., 2023). Descriptions of four established therapy gardens were found (Davis, 2011; Lantz, 2006; Righetto et al., 2016; Söderback et al., 2004). Davis (2011) identified important features include good visibility and physical access, signage to support wayfinding, and careful planting selection, with different gardens possibly required to meet specific user needs. The design process for therapy gardens should include therapists and other staff (Davis, 2011; Righetto et al., 2016), patients, and families (Righetto et al., 2016), and ongoing designer input may improve patient outcomes (Davis, 2011).
Discussion
This review has identified and examined the characteristics of knowledge in relation to nature-based design in stroke rehabilitation environments and the methods used in this research. In this section, the authors discuss a framework for mapping this knowledge and identify gaps and limitations.
A Framework for Knowledge of Nature-Based Design in Stroke Rehabilitation Environments
This review found a high diversity in the characteristics of knowledge, encompassing different aims, methods, participants, contexts, and concepts. Elements of nature-based design were characterized as one of the five types, developed in light of Kellert’s (2018) defined aspects of biophilic design, and the position of the element in the physical environment. Natural analogues and indoor–outdoor connections provide indirect experiences of nature; nature indoors, designed nature outdoors, and the natural environment provide direct experiences of nature, while all five types can provide for experiences of space and place. The analysis of results showed these different aspects offer a range of opportunities and impacts in each of the four categories of knowledge about nature-based design.
Reflecting on the relevance of these categories, the authors observed a pattern of links between them. The categories of design intentions and intentions for use relate to the purpose or objective for a nature-based environment, whereas the impact of exposure to and the impact of engagement in nature-based activities categories involve knowledge about their impact, including measured outcome effects, perceived benefits, and experiences of these environments. Furthermore, the categories of design intentions and impact of exposure to nature-based environments constitute knowledge about physical settings or spaces. For example, Lipson-Smith et al. (2019) establish objectives for the design of inpatient stroke rehabilitation facilities, and West, Sennels, et al. (2019) measure and report on the impact of a naturalistic lighting intervention on stroke patients, providing two different types of knowledge about nature-based design within spaces for inpatient stroke rehabilitation. Likewise, the intentions for use category together with the impact of engagement in nature-based activities category constitute a field of knowledge concerning stroke rehabilitation services within nature-based environments. For example, Vibholm et al. (2023) outline a range of purposes for which therapists use garden spaces during rehabilitation with stroke patients, and Lee et al. (2018) measure and report on the effect of a horticultural therapy program on stroke patients, both providing knowledge about therapy services in nature-based settings, but in different categories.
The four knowledge categories have been drawn together into a framework to illustrate the interrelationship of intention and impact with spaces and services (IISS), refer Figure 3. Many aspects of nature-based design are also closely linked to local climate, topography, ecology, and culture. The IISS framework acknowledges and is grounded in this relationship with location and context.
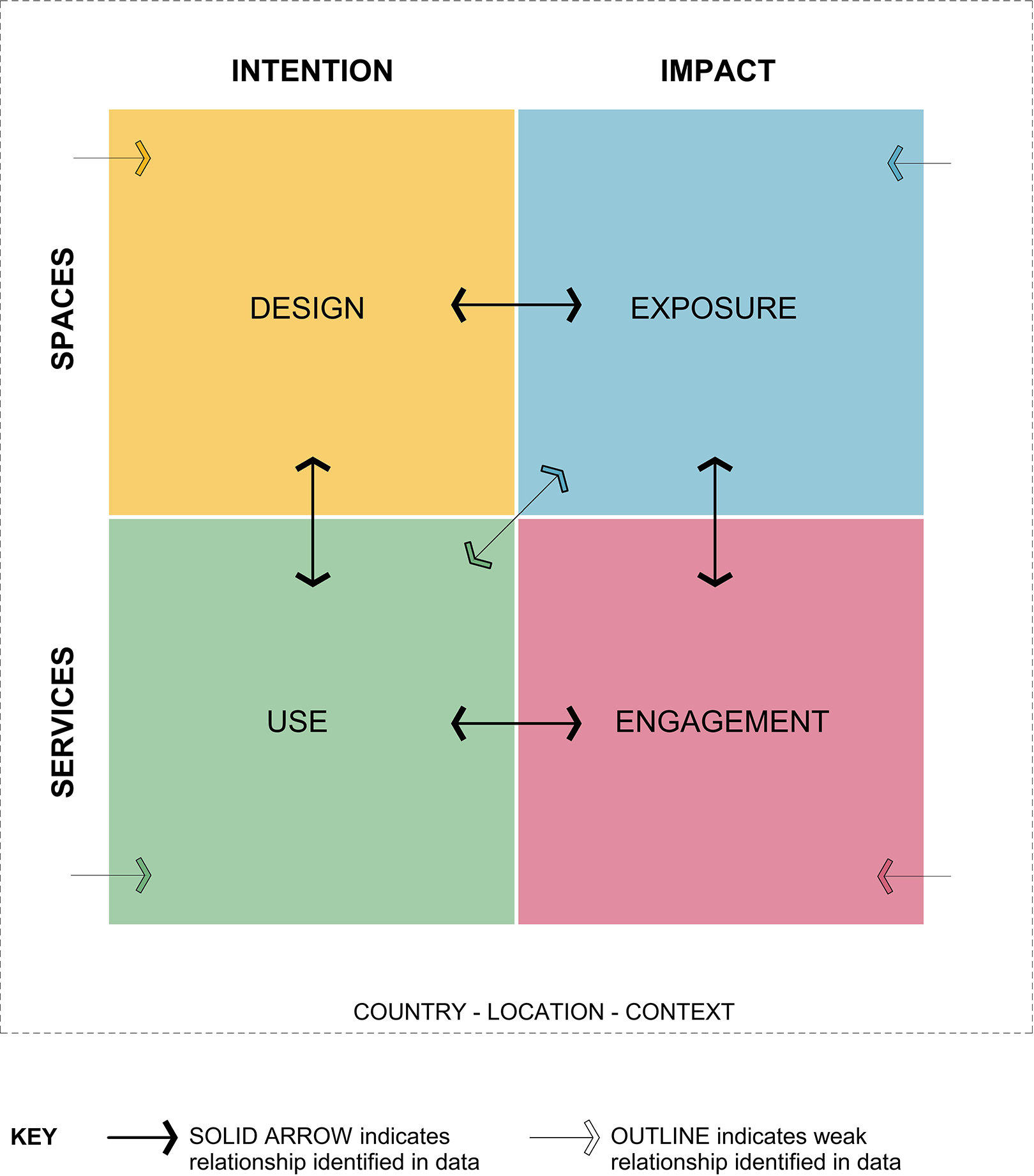
Intention and impact with spaces and services framework.
To illustrate the complexity of knowledge identified, the IISS framework has been used to map the range of study aims and research methods, refer Figure 4. This illustrates, for instance, that quasi randomized controlled trials have only been found in investigations on the impact of exposure to nature-based design, a category in which more than half the studies were quantitative or mixed methods. Conversely, the category of intentions for use of nature-based environments contains more qualitative studies than other categories. The area of impact of engagement in nature-based activity has a balance of qualitative and quantitative approaches and is the only category in which all studies had the investigation of this phenomena as a core aim. While the category of design intentions contains a high number of studies, more than half did not include the investigation of nature-based design in their original aim, but rather found this in their results, illustrating this is the least developed of the identified knowledge categories.
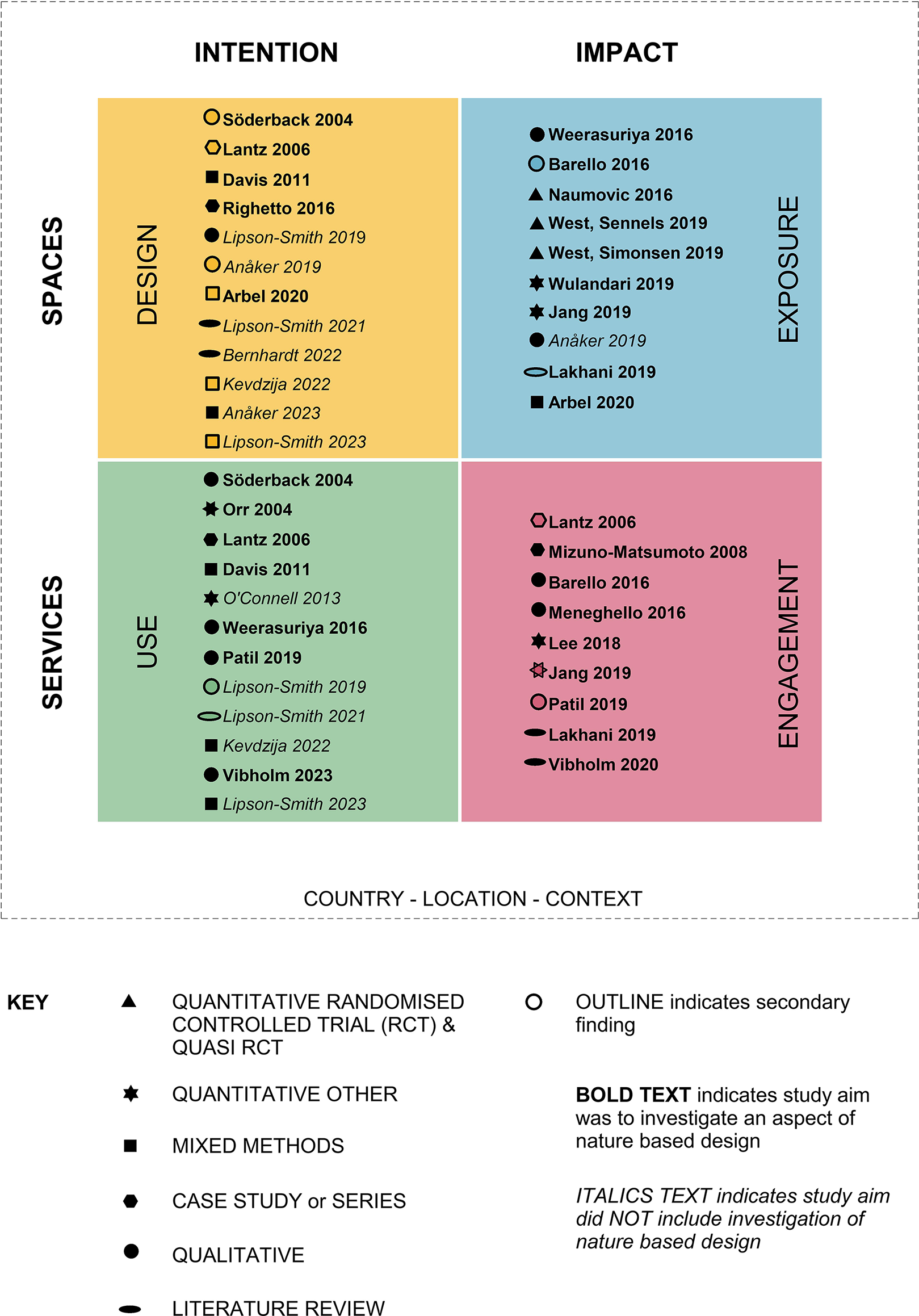
Research methods.
To illustrate the aspects of nature-based design investigated in each category, concentric fields were overlayed on the framework, with internal natural analogues in the center and the natural environment at the outer edge. Studies were located in the relevant fields, with multiple entries for studies incorporating several design aspects, refer Figure 5. This provides a detailed map of the evidence, clearly illustrating knowledge gaps.
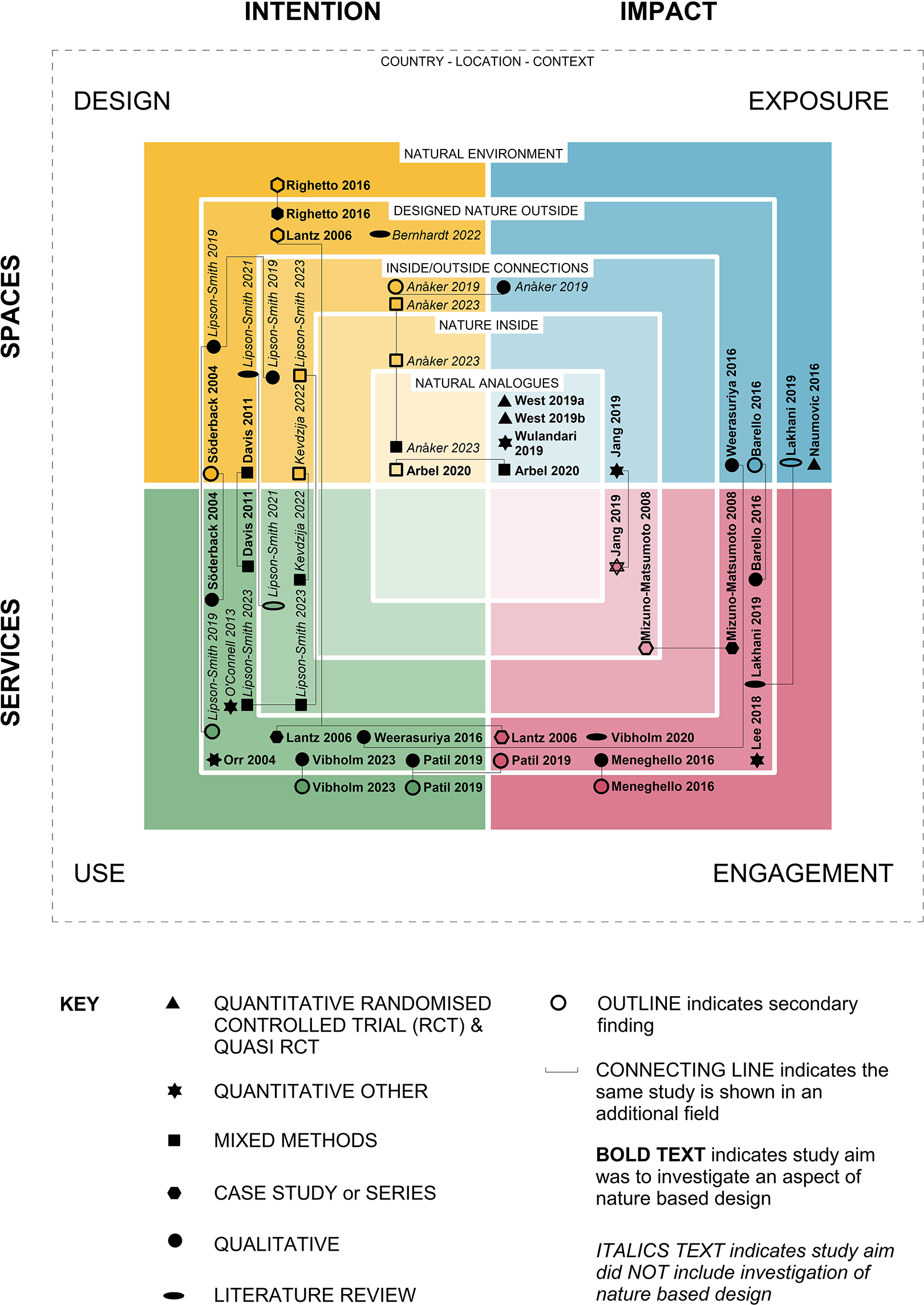
Characteristics of knowledge.
Knowledge Gaps
This review has identified a high level of interest in the use of and engagement in gardens and designed nature outside during rehabilitation, using therapeutic gardening and horticultural therapy as directed interventions to address a range of stroke impacts. However, the current review identified considerably less knowledge on the intentions for use of and the impact of engagement in other aspects of nature-based environments, with minor findings for the natural environment, inside/outside connections, and nature indoors and no findings on natural analogues. For instance, while Anåker et al (2023) found the presence of plastic plants in some Swedish stroke units, no studies were identified which explored the intended use of these and other simulations of nature within stroke rehabilitation settings, or the impact on stroke survivors, families, and staff from active engagement with such features.
The knowledge category of design intentions also has the majority of findings relating to designed nature outside. There were a number of descriptions of gardens; however, only one study completed an extensive multimethod post-occupancy evaluation (Davis, 2011), which correlates with findings by Paraskevopoulou and Kamperi (2018) that such studies on hospital gardens are sparse. Other key findings in this category concern the importance and value of nature-based outdoor spaces and views in stroke rehabilitation. These findings are significant; however, as these were not targeted studies, there is little detail on specific design features or elements. Furthermore, this category had few findings on natural analogues, nature inside, and the natural environment, providing little guidance to optimal nature-based design in stroke rehabilitation environments.
The category of impact of exposure to nature-based environments includes evidence on the impact of only two natural analogues, indicating there are many other such simulations still to be explored. The remainder of this category has low coverage, with just one study identified containing findings on nature indoors, one on experiences of inside/outside connections, and two studies in each of the remaining fields. This category had the lowest findings on designed nature outside, but also the only targeted study on the impact of the natural environment in stroke rehabilitation. The significance of place, context, and/or location was noted in several studies but not explored in depth. As a crucial quality of nature-based design (Kellert, 2018) and an important aspect for stroke survivors’ connection with the outside world, this is another notable knowledge gap.
Researchers have previously shown a range of limitations in the evidence base for the optimal design of environments for stroke rehabilitation (Colley & Zeeman, 2020; Lipson-Smith et al., 2021; Nordin et al., 2021) and gardens in healthcare settings (Paraskevopoulou & Kamperi, 2018; Ulrich et al., 2020). The findings of this review add a new dimension to this knowledge mapping, showing significant gaps for nature-based design in stroke rehabilitation environments. Further research in this field is required to support the positive application of nature-based design and provide associated benefits for patients, families, and staff in these settings.
Healthcare Design Knowledge
The IISS framework developed during this review to map knowledge of nature-based design in stroke rehabilitation environments has relevance for design research beyond the current study. The development of high-performing health environments, aided by evidence-based design (Halawa et al., 2020), relies on high quality research. Mapping research has assisted in the current study to identify the scope of and numerous gaps in knowledge. The framework provides a structure for classifying multidisciplinary knowledge, which is crucial for the design of complex environments, enabling connections to be drawn between intentions for and impacts of physical spaces and the services which use them. A recent study by Saa et al. (2023) demonstrated the importance of linking healthcare design and clinical practice guidelines, highlighting the value of mapping interconnections between these different domains of knowledge. The IISS framework has potential for use to map knowledge in many areas of healthcare design research.
Limitations
The database searches for this review located just over half the included studies, with the rest identified by citation searching. Database searches were limited by a smaller range of terminology for stroke used in the search terms than in the located studies and search terms did not include impairment type, therapy type, or collective terms for participant groups, which were referenced in some studies. The authors limited this review to studies published in English, and as it was a scoping review, they did not undertake any quality appraisal of the included studies (Peters et al., 2021). Therefore, conclusions about the trustworthiness of the identified knowledge cannot be made.
A lack of context descriptions in some studies resulted in their exclusion from this review, while other studies lacked clarity on patient diagnosis. These findings may indicate evolving key words in this field; however, it is also likely that the multidisciplinary approach required for investigations involving healthcare, design, built, and natural environments had an impact. Participation in some studies was noted to have been only available to people without a range of cognitive or communication impairments, which can be caused by stroke. Stroke rehabilitation settings must cater for people with all stroke-related impairments; thus, it is essential to include such participants in design research.
Conclusion
This review has identified the scope and characteristics of the existing knowledge underpinning nature-based design in stroke rehabilitation environments, encompassing design, use, exposure to, and engagement in nature-based design types including natural analogues, nature inside, inside/outside connections, designed nature outside, and the natural environment. The authors have identified the range of research methods used and, through mapping the findings, shown significant gaps in knowledge. Nature-based design has clear potential to make substantial contributions to positive inpatient stroke rehabilitation experiences and outcomes; however, evidence-based design in this field requires significant further research. Furthermore, the IISS framework developed during this review provides a useful structure for examining and mapping knowledge in the broader health design research sphere.
Implications for practice
Use of garden settings and horticultural and garden therapy activities may offer a wide range of benefits for stroke patients, their families, caregivers, and staff and should be considered by healthcare designers and practitioners for stroke rehabilitation settings.
There is a need for further research on the design, use, and impact of natural analogues, nature inside, inside–outside connections, and the natural environment to support and optimize the wider use and benefits of nature-based design within stroke rehabilitation environments.
Healthcare design researchers should consider the use of the IISS framework, which provides a tool to assist characterizing and mapping healthcare design evidence, highlighting the different types of knowledge required to support the design of high-performing environments.
Research into nature-based design in healthcare environments would be assisted by the provision of clear and thorough descriptions of physical settings in healthcare research reporting, which may provide important insights and crucial data for these settings.
Supplemental Material
Supplemental Material, sj-docx-1-her-10.1177_19375867241251832 - Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review
Supplemental Material, sj-docx-1-her-10.1177_19375867241251832 for Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review by Belinda Seale, Aaron Davis, Justin Lawson, Louisa Smith, Joanne Watson and Claire Henderson-Wilson in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867241251832 - Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review
Supplemental Material, sj-pdf-1-her-10.1177_19375867241251832 for Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review by Belinda Seale, Aaron Davis, Justin Lawson, Louisa Smith, Joanne Watson and Claire Henderson-Wilson in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-2-her-10.1177_19375867241251832 - Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review
Supplemental Material, sj-pdf-2-her-10.1177_19375867241251832 for Nature-Based Design in Stroke Rehabilitation Environments: A Scoping Review by Belinda Seale, Aaron Davis, Justin Lawson, Louisa Smith, Joanne Watson and Claire Henderson-Wilson in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Belinda Seale is supported by an Australian Government Research Training Program Scholarship. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Funding sources disclosed in the included evidence sources are noted in Table 7. of the supplemental material.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.