
Abstract
Background:
The emergency department (ED) is a complex, volatile, and limited-resource healthcare setting. Many environmental factors, including high patient volumes, overburdened staff, long waits, and a tense atmosphere, converge in the ED. The objective of this study was to perform a systematic review of extant literature to understand how the ED environment drives patient experience and identify methodological or empirical insights for patient-centered ED design.
Methods:
We searched eight academic databases (Web of Science, PubMed, Scopus, Medline [Ovid], CINAHL, PyscInfo, Compendex, and IEEE Explore) to identify studies that employed observational (descriptive) or interventional (evaluative) methodology. We performed a co-citation analysis of potentially eligible articles and a qualitative synthesis of findings from studies included in our final sample.
Results:
Our search yielded 117 records. Of the 35 potentially relevant articles, 18 were published in the last 5 years, and 50% were authored by investigators in the United States. We used 33 articles for a co-citation analysis, revealing three interdisciplinary clusters and promising potential for collaboration across fields. Thirty articles were subjected to a full-text analysis, resulting in the identification of three overarching dimensions linking the ED environment to patient experience.
Conclusion:
The most commonly identified factors influencing patient experience in the ED included overcrowding and wait times, privacy, and communication; however, existing literature is limited. More research is needed to understand how ED environments configure patient experience and can be improved through design. Particularly, there is little research on participatory interventional strategies in the ED, despite strong evidence suggesting a need for stakeholder participation.
Keywords
Introduction
Clinical settings, in general, and emergency departments (EDs), in particular, have long been described as complex, overwhelming, and stressful environments (Aaronson et al., 2018; Boyle et al., 2012; Gordon et al., 2010; Sonis et al., 2019; Ulrich, 1991). EDs are further characterized by high patient volumes, rising service demands, overburdened staff, and an atmosphere of continual exigency (Brysiewicz & Emmamally, 2017; Cypress, 2014; Oyegbile & Brysiewicz, 2020). While diverse structural and process elements constitute this environment, the ED is typically designed to prioritize its main function, that is, to save lives and minimize morbidity (Bailey et al., 2011). This is reflected, for example, in the ED’s open floor layouts, mobile treatment trolleys placed in close proximity to each other and to staff, and curtained cubicles instead of solid partitions (Weiland et al., 2017). In addition, ED operations are also reliant upon many intangible elements that enable smooth service delivery, such as complex communication protocols and triage systems. These and other design attributes facilitate continual patient monitoring, easy access to medical equipment, and rapid response to emergent and urgent situations. However, it is also the same attributes—which facilitate timely and efficient response in a high-tension setting—that may negatively affect patient experiences of seeking and receiving care.
Within healthcare quality literature, it is well-established that EDs continue to be undersized, understaffed, and rife with outdated operational procedures, resulting in bottlenecks and redundant processes that contribute to long wait times and other stress factors (McKay, 1999; Sonis et al., 2019). With competing functional requirements, optimal care provision and patient satisfaction are at risk of being compromised (Weiland et al., 2015). At the same time, for an increasing number of people, the ED forms the initial point of contact with the health system, often constituting a patient’s first hospital experience. The ED has thus aptly been called the “front door of the hospital—as important as the lobby and other high-end areas in creating an overall impression of an institution, its attitude towards its patients, and the quality of care offered” (Glasser, 1998, p. 1).
Therefore, we contend that the role of design and designers in the ED environment concerns many explicit and implicit drivers of functionality, usability, and the overall care experience with and within the built space. Our review is intended to provide an improved understanding of the ED as a designed environment where patient-centered care may be cultivated and enhanced through better design choices. Before proceeding onto our methodology and findings, we provide below a brief background of commonly used terms and their implications in this context, given the interdisciplinarity of the subject matter.
Defining Terminology—Health Facility Design and Evidence-Based Design
Health facility design (HFD) is a generalized phrase used to describe a wide spectrum of activities relating to planning, constructing, and optimizing healthcare settings. As a complex process with multiple focus areas, HFD shapes not only the physical design of the built environment but also affects patient flow, staff efficiency, technical equipment considerations, operational procedures, and information management within a healthcare setting (Hicks et al., 2015). Traditionally, HFD has been based on the past training and industrial experiences of designers with similar projects, client expectations, and adherence to accredited design standards (Ulrich et al., 2008). However, as health systems face demographic shifts, technological change, and increased disease burden, healthcare facilities—many of which were designed decades ago—must evolve correspondingly to meet arising challenges, competing demands, and new ways of working (McKay, 1999).
To keep pace with rapid clinical advancements and transforming healthcare needs, medical practice has shifted toward evidence-based medicine—where there is an emphasis on utilizing the best available current research to inform treatment decisions (Sackett et al., 1996). Drawing upon this core ideal and borrowing from its terminology, HFD has similarly experienced a move toward evidence-based design (EBD), with the goal of improving healthcare quality and patient outcomes through research-informed choices in design practice (Halawa et al., 2020). EBD can hence be broadly described as a framework that encourages the use of rigorous scientific methods to identify and respond appropriately to the links between built environments and human health (Ulrich et al., 2008). Over the past decade, EBD has been incorporated at various levels in building, planning, managing, and improving many healthcare settings (Zimring et al., 2013), with a growing number of disciplines and professions now engaged within and across these domains.
Given its varying applications and the diversity of expertise contributing to the field, the terms EBD and HFD are often used in parallel, and even interchangeably, in the literature base. For the purpose of our study, we are not concerned with dissecting differences in terminology. Rather, the remainder of this paper intends EBD and HFD to mean the one and the same thing in order to capture the breadth of the field, despite variations in vocabulary. As such, we employ these terms in a broad sense, primarily, to position the ED as a designed healthcare environment, and secondarily, to frame design activity widely, including but not limited to physical considerations within. We will now articulate further our conception of design’s scale and scope in health facilities, and next, outline the focus of this review in terms of the emergency setting.
Evidence-Based Health Facility Design—From Micro to Macro Level
While EBD is most commonly seen as the incorporation of scientific methods in live and ongoing HFD or quality improvement projects, concerns have been raised that “the demonstrated value of such methods, however, has not yet resulted in their widespread adoption in healthcare design process in practice” (Halawa et al., 2020, p. 454). We theorize that this problem stems, at least in part, from the relative novelty of design as an academic discipline, where research, theory, and education have frequently lagged behind developments in the field (Rowe et al., 2020). Expanding EBD practice across health facilities requires independent scholarly appraisals of the evidence base—to be performed outside the constraints of singular or stand-alone briefs—in order to foster widespread evidence transferability and promote research uptake. Therefore, with this review, we contribute one such appraisal of the literature—focusing our attention on the ED, which is often regarded as a priority setting within the hospital, and yet, presents persistent challenges for designers, researchers, and healthcare managers.
Building health facilities involves several iterative phases, which can be viewed as design activities undertaken along a spectrum of macro and micro levels. Halawa et al. (2020) provide a useful overview of potential design stages or levels as follows: the planning stage to determine functional and capacity needs; the schematic stage to generate exterior and interior plans including building organization, floor plans, and room layouts; the detailed design stage to consider technical equipment, interior finishes, lighting, seating, signage, and other finer details; and the construction stage, including the development of architectural blueprints and the actual building of the health facility. In a more comprehensive breakdown, the Center for Health Design (CHD) characterizes the nature and scope of EBD activities at health facilities as a continuum: from setting organizational goals, collecting research data, using analyzed data to generate design concepts, and hypothesizing how design choices might affect health outcomes—to collecting performance metrics, monitoring design implementation, and evaluating postoccupancy results (The Center for Health Design, 2022; McCullough, 2010).
While all stages described above may apply to new constructions, the majority of health facilities (including EDs) have already been designed. Within existing structures, design changes are usually made through discrete quality improvement strategies and targeted renovation projects at varying scales. In many scientific investigations or industrial projects to improve health facilities, some of these stages may overlap, contain cyclical iterations, or only involve a few components, rather than all. Moreover, most interventions to improve ED experiences focus on isolated features of the environment at the micro scale, with emerging evidence proving difficult to generalize easily. While we are interested in design activity at any stage or scale, we do not aim to appraise the role of each element of the built environment individually. Instead, in our study, we adopt a high-level, complex systems perspective to source and analyze evidence that links ED design to its impact on patient experience.
Gaps in the Evidence Base—Designing Patient-Centered EDs
Patients seek emergency care for a range of ailments with varying degrees of complexity and urgency, including for non-urgent reasons. Recent literature has suggested a strong correlation between positive assessments of patient experience and important health system goals, including improved health outcomes and care quality, higher staff satisfaction, and reduced medicolegal risk (Sonis et al., 2019). Patient experience is “the sum of all interactions, shaped by an organization’s culture, that influence patient perceptions, across the continuum of care” (The Beryl Institute, 2016), thus indicating a corresponding need for patient-centered health settings and services. However, patient experience in the ED differs from that in other healthcare settings (Aaronson et al., 2018). Patients visiting the ED—often in acute physical or psychological distress—are faced with the converging and compounding effect of multiple stress factors at this setting. Feelings of anxiety, uncertainty, and confusion produced by an unnerving environment may further impede their ability to cope with long waits, clearly describe their conditions, comply with treatment protocols, and understand discharge communication correctly (Iwanowski et al., 2008; Kash & McKahan, 2017; Wilets et al., 2003)—ultimately contributing to poor health outcomes and higher readmission rates (Hastings et al., 2011; Santana et al., 2017). This indicates that the ED environment bears serious implications for patient experience, and by extension, for our healthcare system.
Advancements in evidence-based HFD have consistently demonstrated a positive influence on patient recovery rates, length of stay, and overall satisfaction with quality of care (van Hoof et al., 2015). Yet, the applicability of this work for improving ED settings remains unclear (Abdelsamad et al., 2018; Morris et al., 2012; Welch, 2012). Accordingly, our objective in this systematic review was to better understand the multifactorial role of the ED environment in shaping patient experience. We employed the PICO strategy to clarify our aims and developed the two following research questions to guide our investigation:
Our study distinguishes itself from previous reviews on related topics (Gharaveis et al., 2018; Sonis et al., 2018) by analyzing the implications of ED environment/health facility design on patient experience, identifying the disciplines engaged in the field, and categorizing the resulting evidence under three conceptual dimensions to inform the development of patient-centered EDs.
Methods
Design and Search Strategy
Our reporting strategy follows the PRISMA guidelines (Moher et al., 2009). In December 2021, we performed an electronic literature search of eight scholarly databases (Web of Science, Scopus, PubMed, CINAHL, Medline [Ovid], Compendex, IEEE Xplore, and PsycInfo), supplemented with an independent search on Google Scholar, using predefined terms in title and abstract as available in Figure 1, with minor variations depending on the database. No publication date limits were applied. Wherever available, filters to restrict results to the English language were used. Screening was performed independently by the two authors (A.R. and M.K.) and conflicts were resolved by consensus.
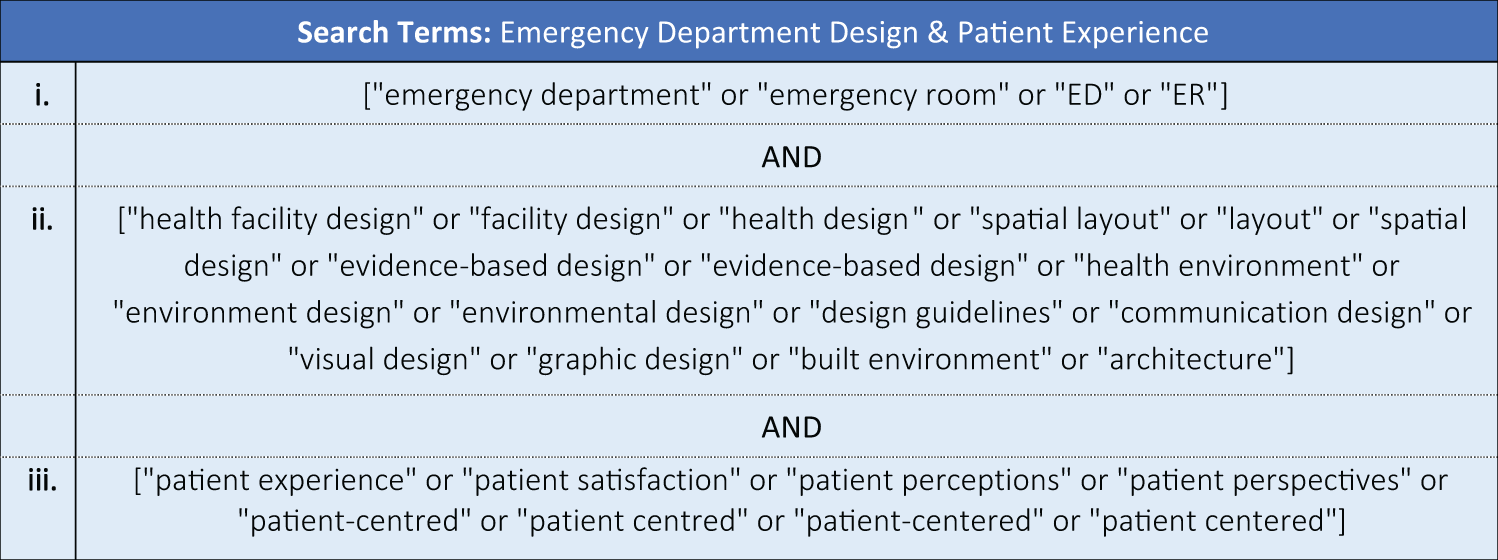
Search string.
Data Extraction
Following our initial assessment, we first extracted the title, abstract, journal name, and publication year from all articles found relevant for eligibility screening. Additional data were then extracted from the full texts, including the study type, research methodology, and geographic location (Online Appendix 1). We performed a qualitative synthesis of findings, instead of conducting a meta-analysis, because there was considerable heterogeneity between the studies in terms of their objectives, methodologies, samples/settings, and outcome measures. To ensure consistency in our analysis, the authors (A.R. and M.K.) verified the suitability of each study’s inclusion in the review and coded it independently, with any differences resolved by discussion.
Co-Citation Analysis
To generate further insights on the disciplines contributing to this evolving area of research, we performed a co-citation analysis of potentially eligible articles to determine the frequency with which two sources are cited together by other documents. Co-citation analysis reveals potential disciplinary silos and can help identify theoretical or methodological areas of scholarly activity, or conversely, gaps in the field. In total, 33 papers were possible to use for this purpose because two articles were not indexed on Scopus, from where we extracted citation data.
Results
Study Inclusion
Our search yielded a total of 117 records, with 34 records from Web of Science, 21 records from Scopus, 9 records from PubMed, 7 records from Medline [Ovid], 6 records from Compendex, 4 records from CINAHL, 2 records from IEEE Xplore, 2 records from PsycInfo, and 32 records from Google Scholar. All records were retrieved and uploaded into Covidence Version 2.0 (Covidence systematic review software, Veritas Health Innovation, Australia) for assessment of eligibility, where they were first screened based on title and abstract, and subsequently, based on full-text readings. The complete search and elimination sequence is available in Figure 2.
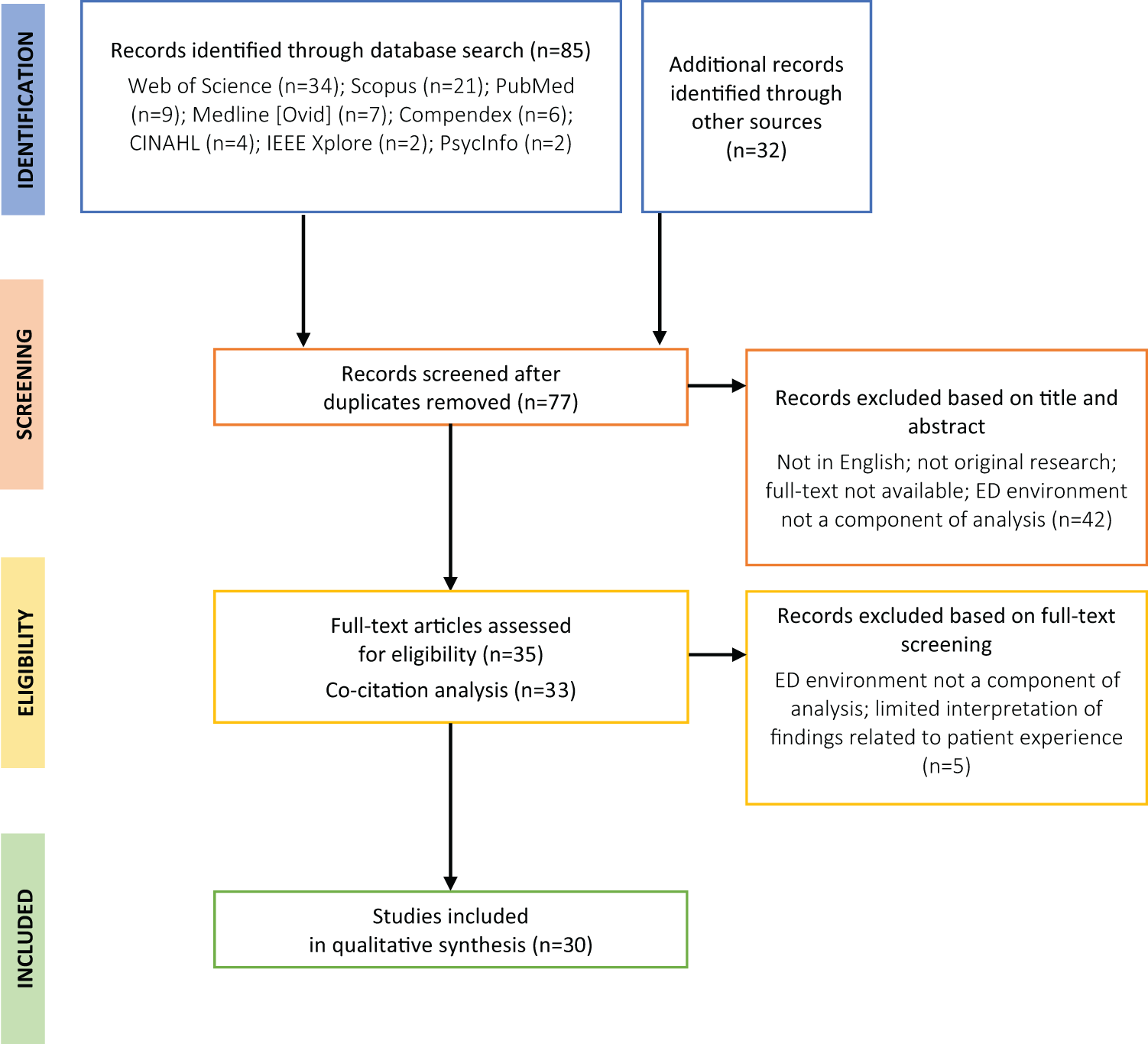
PRISMA flow diagram.
We applied three inclusion criteria. Studies were selected if they (1) had full texts available in the English language; (2) reported the results of empirical research in a peer-reviewed academic journal (i.e., excluding conference proceedings, editorials, theoretical or conceptual commentaries, literature reviews, and research protocols); and (3) presented evidence about the ED environment in relation to patient experience. We also excluded papers that lacked analytic rigor or did not link their findings adequately to patient experience.
Of the total 117 records, 40 were identified as duplicates through automated duplication detection by Covidence Version 2.0 and hand search, yielding a total of 77 records for further screening based on title and abstract. Studies that were not original, not in English, and not related to the ED environment were excluded. At this stage, and the next, we also excluded the very extensive literature on individual design elements in the ED, which would be far beyond the scope of a single review. This left 35 studies for eligibility screening, which were subjected to a full-text reading. Of these, 33 were retained for co-citation mapping to identify contributing disciplines (2 studies were not found on Scopus). We further excluded 5 studies where patient experience was not a significant component of analysis, resulting in a final sample of 30 articles remaining for qualitative synthesis.
Contributing Disciplines and Subject Categories (Co-Citation Analysis)
Next, we examined the methodologies employed within our sample, but it quickly became evident that there was no commonly agreed upon approach to investigate, improve, or evaluate patient-centered ED design. Given the diversity of disciplines driving the field, we performed a co-citation analysis of potentially eligible articles to identify disciplinary clusters using VOSviewer Version 1.6.18. As we note earlier, we were able to do this for 33 articles as two papers were not indexed on Scopus from where we drew citation data.
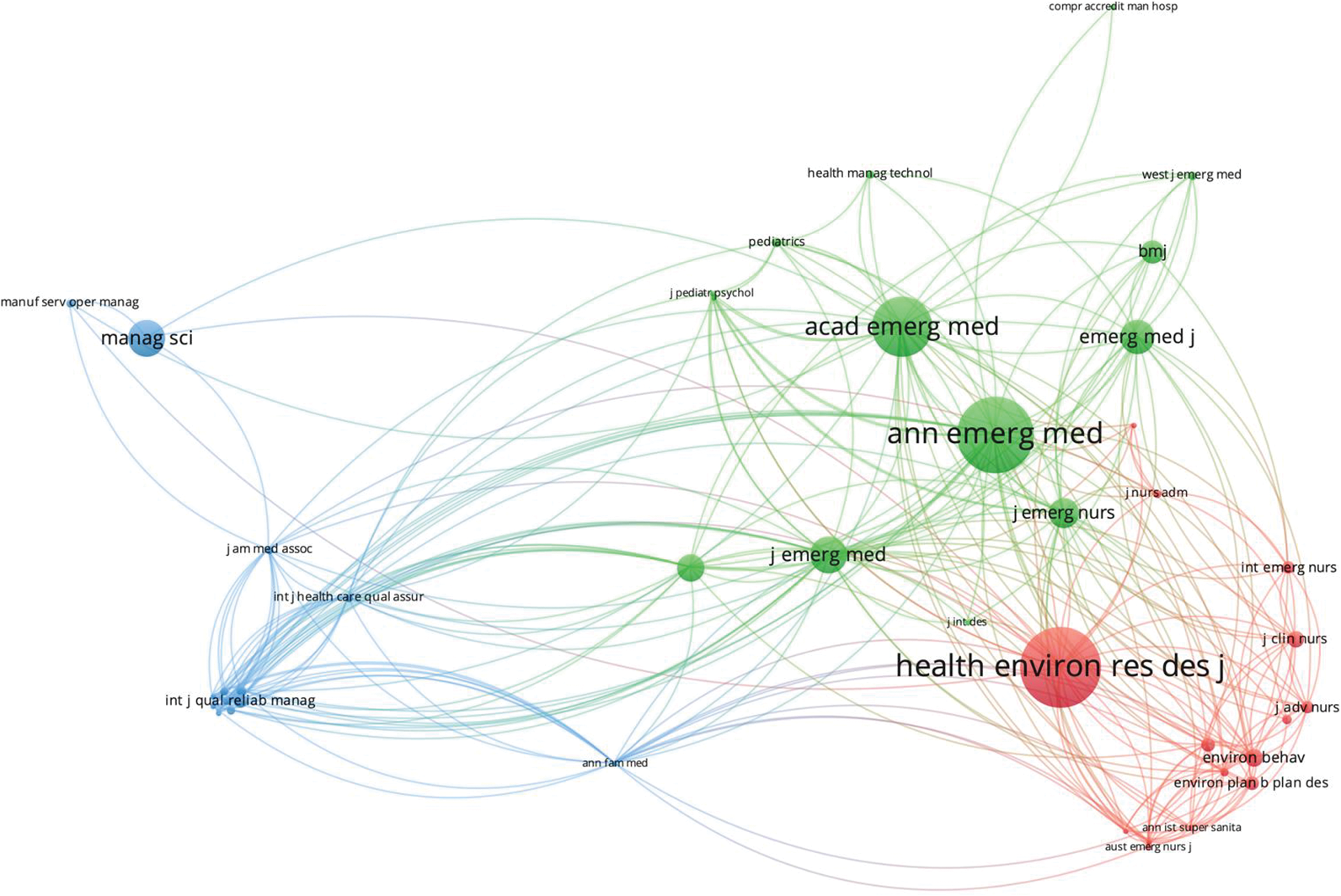
Co-citation analysis identified three interdisciplinary clusters, which we group as follows: Healthcare Engineering and Health Services/Quality Management (blue), General and Emergency Medicine (green), and Nursing Sciences and Health Environment/Facility Design (red).
In co-citation mapping, the cited source forms the unit of analysis, and we include journals that were cited at least twice within the 33 articles. As shown in Figure 3, the distance between any two journals indicates their similarity to each other (van Eck & Waltman, 2010). We employ association strength normalization to reduce the distance between the connected nodes (van Eck & Waltman, 2009). The number of citations is represented by the size of the nodes and the line shows citations present in either direction. This analysis identified three interdisciplinary clusters, which we group as follows (using randomly generated colors, from left to right): Healthcare Engineering and Health Services/Quality Management (blue), General & Emergency Medicine (green), and Nursing Sciences and Health Environment/Facility Design (red). Overall, the literature is concentrated in emergency medicine and healthcare environments research. Intriguingly, we find nursing journals to be closely linked to design journals, indicating scholarly insights shared between the two disciplines. Meanwhile, health quality, management, and operational research appear at the borders, with relatively less cross-citation with facility design literature and slightly more with medical journals. We also note some health technology, architecture, and manufacturing literature at the peripheries of clusters, suggesting the emergence of new scientific areas and the possibility of novel contributions to the field. Based on these findings, there appears to be great potential for further interdisciplinary collaboration.
Sample Characteristics
Figure 4 shows the number of potentially eligible articles by year. Overall, our results indicate an upward trend in ED environment research, and correspondingly, in ED design research pertaining specifically to patient experience. Within this sample, only 5 studies were published prior to 2010 and 30 were published in the last decade (2011–2021), with more than half published within the last 5 years. No studies prior to 1999 were found eligible.
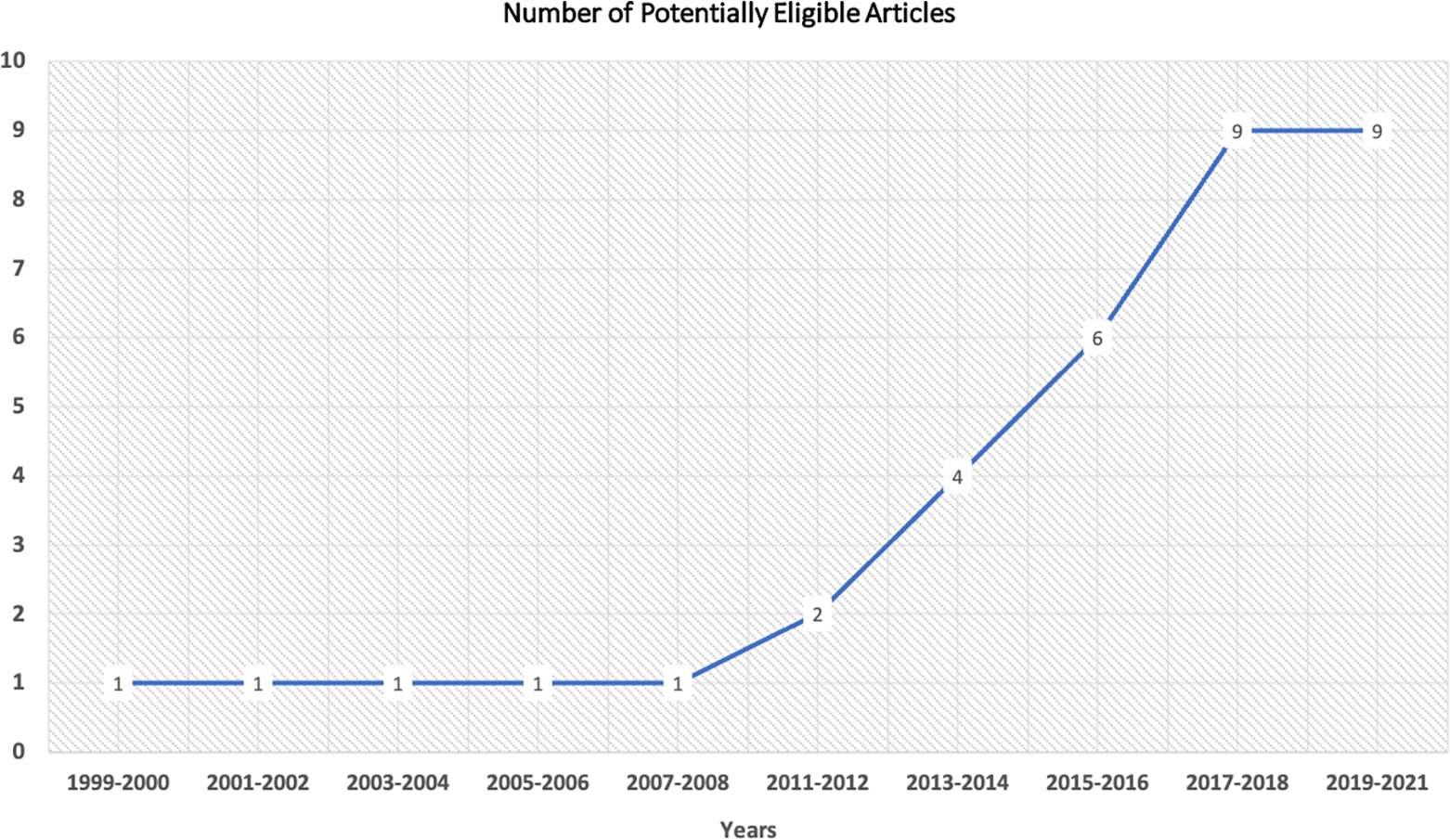
Potentially eligible articles by year.
After screening the full texts of the 35 potentially eligibility articles, 30 were found relevant for inclusion in our qualitative synthesis. Of these, 15 studies were conducted in the United States and 15 were from other countries (Australia = 3, Italy = 2, Canada = 1, United Kingdom = 1, Belgium = 1, Ireland = 1, South Korea = 1, Taiwan = 1, Chile = 1, Sweden = 1, Saudi Arabia = 1, and Saudi Arabia and Egypt [binational study] = 1). In terms of research design, 15 studies used quantitative methods, 12 used qualitative methods, and 3 used mixed methods. The complete list of included articles and their characteristics is available in Online Appendix 1.
Thematic Findings and Discussion
This systematic review aimed to gather and analyze evidence of how ED environment design affects patient experience, and what approaches have been used in the field to identify and address challenges. Our findings relate broadly to three key aspects (split further into subdivisions), as follows: (1) physical and operational dimensions, (2) sociopsychological dimensions, and (3) implementation and evaluation dimensions. While we have attempted to organize our discussion under these domains, we found significant intersections between the themes. For example, patient privacy levels may be linked to physical layouts, and furthermore, these may combine to affect social interactions between ED users and staff. Such overlaps confirm the complexity of the healthcare environment under study and point to the challenge of planning, designing, and managing patient-centered EDs effectively. As such, we may reference the same paper several times in the forthcoming analysis; however, we discuss each study primarily under the dimension most strongly correlated to its main investigative focus and relevance to our research questions. We will now describe each of the three identified dimensions in turn.
Physical and Operational Dimensions
Overcrowding and wait times
In the ED, patient perceptions of service value are tied to the amount of time it takes to receive care (Mazzocato et al., 2012), thus indicating that faster service would improve patient experience. Unsurprisingly, the majority of the literature focused, in whole or in part, on overcrowding and wait times as a major factor influencing patient experience in the ED. Considerable attention has been devoted to address this problem, with most studies in the field being intervention-based and deriving their methodological approaches from diverse disciplines.
In a study of patients presenting to the ED with chest pain, Hall et al. (2008) investigated whether ED layouts affect how long it takes patients to receive physician assessments, reporting that the distance between the clinician area and treatment rooms substantially delayed assessment times, as did the presence of doors rather than curtains. Unexpectedly, however, Sayah et al. (2016) found that the overall length of stay increased in an ED that underwent an expansion, decreasing only after process flow improvements were made and a Rapid Assessment Unit (RAU) was established within. They concluded that reorganizing process flow and providing rapid assessment services was more effective for improving patient experience than facility expansions and renovations. In a similar intervention, Repplinger et al. (2017) implemented a front-end Flexible Care Area (FCA) in an ED to decrease delays in care. In their study, patients receiving care at the FCA reported lower satisfaction levels despite a shorter length of stay, compared to those not seen at the FCA—suggesting that the effect of wait times on patient experience may be moderated by other factors. For example, in Vezyridis and Timmons’s (2014) study, ED wait-time targets were found to alter provider roles and responsibilities, restructure professional hierarchies, and generate resultant pressures on ED staff—with potentially negative implications for patient and staff interactions. Other studies, both from our review sample and those in the broader literature base, have shown that the experience of waiting, in and of itself, is subject to multiple influences. As Sayah et al. (2016) and Annemans et al. (2018) have discussed, better understanding and responding to these influences may involve improving the waiting experience through simple interventions to provide comfort or distractions to the patient. We comment upon these in a subsequent section of this article (see Cerebral and Embodied Experience subsection).
Recognizing the interaction of multiple factors driving ED experience (Zamani, 2019), several authors recommended the use of lean tools to manage high patient volumes and improve overall efficiency. Lean concepts first gained prominence through the work of the Toyota Production Service in the 1950s and have since seen numerous business and service sector applications, with increasing uptake across healthcare management over the decades. In essence, lean thinking and principles focus on the elimination of non-essential structures and activities within a system (Liker, 2004). If applied to healthcare environments, lean concepts offer the advantage of a complex-systems view, helping to identify wasteful or non-value-added services for achieving maximum efficiency (McCarthy, 2006; Ng et al., 2010). In our review sample, the authors used a variety of methods from lean thinking, such as quality function deployment (Abdelsamad et al., 2018), process flow mapping (Alowad et al., 2020; Barros et al., 2020; Twanmoh & Cunningham, 2006), value stream mapping (Alowad et al., 2020), and root cause analysis (Alowad et al., 2020).
From a user perspective, wait times in between the steps needed to obtain ED services result from a breakdown of the healthcare process (Mazzocato et al., 2012)—a problem that lean tools have the potential to rectify. For example, Twanmoh and Cunningham (2006) implemented a series of changes across the input, throughput, and output levels in the ED. To improve input, they reorganized the triage and admission processes. To improve throughput, they modified the physical layout for easier staff movement and communication, changed staffing patterns based on anticipated patient volume, and revised policies for interactions with radiology staff. To improve the output of patients leaving the ED, they used lean thinking to identify the causes for discharge and admission delays, established a system for flagging the charts of discharge-ready patients, and implemented admission orders to decrease overall wait times.
Although used extensively in healthcare quality improvement, concerns have been raised that lean thinking techniques are often applied singularly, rather than being combined together for better outcomes (Robinson et al., 2012). In order to maximize its potential benefits, it has been suggested that a combination of lean tools be used to address ED congestion (Camgoz Akdag et al., 2018). Most studies included in our review used multiple lean techniques together or in combination with other (non-lean) methods. Morgareidge et al. (2014) used discrete event simulation (DES), a lean tool, alongside space syntax analysis (SSA) to improve process flow and redesign the ED space. Simulation tools provide the advantage of making current bottlenecks—and the impact of corresponding interventions on service levels—visible instantaneously within the simulation program (Camgoz Akdag et al., 2018; Wang et al., 2015). In another study, Abdelsamad et al. (2018) assessed two EDs based on stakeholder surveys in tandem with international design standards, finding several discrepancies and gaps in their current designs. In response, they proposed a new ED design that combined both stakeholder-identified requirements as well as international design standards using quality function deployment, another lean tool. Barros et al. (2020) developed and tested new production workflow designs based on lean and non-lean concepts derived from several interdisciplinary areas (modularity, economics and management, optimization, and machine learning), with their results showing a subsequent reduction in ED length of stay and substantial cost savings for the ED. Alowad et al. (2020) used a combination of process flow mapping, value-stream mapping, and root cause analysis to determine that ED flow is affected by limited bed capacity, unavailability of necessary staff, ED layout, and lack of understanding among patients about the nature of emergency services. To address these challenges, they developed a value stream map to streamline ED activities and minimize wait times.
Taken as a whole, the literature focusing on overcrowding and wait times indicated that existing designs do not adequately meet the needs and demands of the dynamic ED environment. Although facility expansions and renovations may be possible and beneficial in some instances, this is not always the case, whereas service planning and process efficiency have often shown better outcomes in comparison. Moreover, while ED wait times are the dominant factor shaping patient experience, short waits could negatively affect other service experience factors, and conversely, longer waits could be made more tolerable by improving related experiential dimensions. Finally, given that each ED is unique, the authors recommended selecting improvement tools most appropriate for local needs and cultural considerations, and actively involving stakeholders to determine what these particular challenges and priorities may be.
Privacy and security
Understandably, privacy and security issues are a key concern for patients in any healthcare context. However, the ED’s structure and environment appears to create unique challenges to these, and as such, many authors highlighted the importance of ensuring privacy and security in emergency care. In a survey-based study, Lin and Lin (2011) reported a strong relation between perceived privacy levels and patient satisfaction, identifying six predictors, as follows: personal information overheard by others, overhearing others’ personal information, unintentionally heard inappropriate conversations from healthcare providers, being seen by irrelevant persons, space provided for privacy when being physically examined, and providers’ respect for patients’ privacy.
Three studies in our review sample specifically evaluated the challenges surrounding the use of curtains in EDs (Barlas et al., 2001; Hall et al., 2008; Hartigan et al., 2018). While solid walls certainly provide a greater sense of privacy than curtains, many EDs continue to utilize curtains due to the ease of moving people and equipment around, cost-effectiveness, and the need to easily monitor patient status. Barlas et al. (2001) reported that curtain walls met HFD standards; however, patients perceived inadequate visual and auditory privacy, with concerns raised about being overheard or seen by others during their medical examinations. This was thought likely to affect their ability to describe their conditions fully and accurately, with implications for appropriate treatment decisions. Similarly, Hartigan et al. (2018) found that patients in an obstetric ED perceived significantly improved privacy levels after refurbishments were made to replace curtained partitions with walled cubicles. Investigating if ED layouts affected the time it took for patients to see a physician, Hall et al. (2008) found that doors—which afford more privacy—delayed assessment times compared to curtains. The authors noted, however, that further research is required to understand how the need for designing private patient areas might be reconciled against the importance of transparent spaces to monitor and respond to rapidly changing patient acuity (Barlas et al., 2001; Hall et al., 2008). Relatedly, examining how ED design affects staff in five American EDs, Gharaveis et al. (2019) highlighted the legal obligation for HIPAA (Health Insurance Portability and Accountability Act) compliance, suggesting the use of glass doors in combination with curtains to allow for both patient monitoring and private staff–patient discussions.
In a study represented here by two papers (Pati et al., 2014; Pati et al., 2016), the authors examined how the ED’s physical attributes affect security and efficiency for patients and staff, and accordingly, what design decisions may facilitate efficient and safe ED operations. Importantly, they found security and efficiency to be mutually reinforcing concepts, whereby improving efficiency would potentially enhance security (and vice versa). Using multidisciplinary gaming alongside semi-structured and touring interviews, they identified 16 domains of design decision-making and improvement for ED designers and planners to consider, as follows: entrance and waiting areas, traffic management, internal waiting areas, the triage process, examination/treatment area configuration, examination/treatment area centralization versus decentralization, examination/treatment room standardization, adequate space, nurse work space, physician work space, adjacencies and access, equipment room, psychiatric evaluation room, staff de-stressing room, hallway width, and results waiting area.
Overall, the literature suggested that issues regarding privacy and security had direct correlations to patient satisfaction. In many instances, the authors identified complex trade-offs between physical materials utilized (e.g., doors vs. curtains) and resulting effects. As concerns around privacy and security will most likely continue to grow in future, the authors recommended approaches that take into account the full range of the stakeholder spectrum and their experiences in devising design responses. In light of these findings, we suggest that health facility designers and quality improvement researchers attend closely to the sociodemographic characteristics of the population served by a particular ED (see Patient Characteristics subsection) and consider utilizing participatory approaches (see Implementation and Evaluation Dimensions subsection) to extract stakeholder knowledge about privacy and security nuances at each site.
Sociopsychological Dimensions
Cerebral and embodied experience
As discussed previously, much of the literature focuses on reducing ED wait times to improve patient experience. However, wait times cannot be eliminated completely, given the need to prioritize patients based on changing acuity (Weiland et al., 2017). Accordingly, some authors noted that the experiential dimensions of the ED environment may be better designed to support long waits, and more generally, patient experience as a whole (Annemans et al., 2018; Buffoli et al., 2016; Viotti et al., 2020). Notably, Viotti et al. (2020) found that environmental comfort did not appear to significantly moderate the relationship between wait times and patient satisfaction. The authors suggested that ED users, as opposed to other healthcare users, may be too distressed by their health concerns to attach much significance to physical comforts, considering the urgency of the situation. On the other hand, Annemans et al. (2018) discovered that unoccupied time sensitized some patients to notice—and altered how they responded to—spatial details. They also found that patients appreciated small interventions, such as coffee machines, magazines, and televisions in waiting areas, which are not always present in EDs. Sayah et al. (2016) suggest the possibility of “disneyfication” (p. 345) in the ED, that is, incorporating waiting management techniques, such as distractions, updates about wait time status, and environmental modifications, alongside reducing wait times by applying lean thinking to eliminate unnecessary steps and use split-flow design techniques (organizing separate treatment areas based on patient acuity).
While our review does not specifically focus on individual physical attributes (e.g., seating), we include such studies if they report implications for ED patient experience at the macro-level. For instance, Robinson and Green (2015) showed that ambient lighting in the ED improved perceptions of passive waiting time, and by extension, increased patient satisfaction. In a pre–post study at a recently renovated ED, Lindahl et al. (2021) designed a self-reporting questionnaire to assess if light and color affected awareness/orientation; safety/security; functional abilities; privacy; personal control; and stimulation among patients, families, and staff. Their results showed light and color to be distinctive elements shaping the perceived supportiveness of the physical environment. Similarly, Buffoli et al. (2016) developed an evaluation tool to assess the humanizing qualities of the physical ED space and the social aspects of service processes in the ED. This tool was validated with two user groups—adult and pediatric patients—and helped identify potential fields of intervention at the test site. Overall, the authors noted the general scarcity of validated tools for testing how the physical attributes of ED environments relate to social and psychological perceptions of care, indicating an important area for future investigations.
Given that ED nurses are often involved in and expected to represent patient perspectives in ED design projects, Annemans et al. (2018) examined if patient understandings of the ED space differ from those of nursing staff. They found that patient perceptions could be grouped into material, social, and temporal aspects. Patients were largely affected by their embodied experiences (e.g., being wheeled through corridors; altered visual perspectives when lying down), emotional state, associations with prior hospital visits, collective experiences shared with accompanying family members, social interactions with staff and other patients, and the time spent waiting to receive care. In particular, they highlighted the nuances that distinguish patient experiences from those of ED nursing staff, calling for meaningful collaboration between nurses and patients for designing patient-centered EDs.
Interpersonal interactions, information needs, and shared decision-making
Previous literature has suggested that staff-patient communication is among the most important factors influencing patient experience in the ED (Sonis et al., 2018). Communication involves multiple interactions between ED staff and users at several contact points—through registration, triage, waiting spaces, treatment, and discharge—suggesting multiple opportunities (and challenges) with regard to meeting patient expectations and improving service quality. Some authors further noted that ED patients spend much of their time waiting to receive information about what happens next, observing environmental cues (sounds, other patients, physician–nurse interactions, etc.) to anticipate upcoming interventions, and navigating through service stages or different areas of the ED using signage and wayfinding aids (Annemans et al., 2018; Harvey et al., 2021). Moreover, Viotti et al. (2020) showed that the relationship between wait times and patient satisfaction was significant wherever patients perceived a low degree of humanistic care (human-centered or person-centered care; see Conclusion and Future Research Potential section), and became insignificant with a high degree of humanistic care. Accordingly, they recommended redesigning work processes for ED staff, developing training resources to cultivate empathetic communication skills, and actively engaging patients in care decisions.
Several authors noted that patient involvement in medical decision-making shaped patient perceptions of humanistic care and improved patient experience (Melnick et al., 2015; Viotti et al., 2020; Watson et al., 1999; Yoo et al., 2018). Here, digital aids used at the bedside may maximize the time physicians spend with their patients, allay the anxieties of ED users, fulfil their need for information about their health status, and increase their participation in care. Yoo et al. (2018) tested a new health information technology device to facilitate communication between ED staff and patients. Their findings indicated that the device satisfied information-seeking behaviors among ED patients, alleviated anxiety, and, ultimately, increased patient satisfaction. Similarly, Melnick et al. (2015) evaluated the use of a patient-centered bedside clinical decision support (CDS) for patients presenting to the ED with brain concussions. The CDS was successful in decreasing the time physicians spent at desktop-based electronic health record interfaces, which are typically located away from patients.
Patient characteristics
Overcrowding, noise, long wait times, security, and privacy issues may pose additional barriers for particular patient profiles, such as those with advanced illnesses, comorbidities, mental health concerns, addictions, age-related cognition and dexterity challenges, etc. For example, Weiland et al.’s (2017) survey-based investigation revealed that ED staff consider it important to allocate separate private spaces for cancer patients in the ED. Similarly, Philip et al. (2018) reported that ED cancer patients expressed concerns over communication, general environmental characteristics, and delays in symptom management—indicating the need to redesign the ED to better serve its multifaceted functions and diverse patient demographics. In another study, Gharaveis et al. (2019) note that psychiatric patients form another key demographic to consider while designing EDs, particularly in designating separate spaces for medical observation and aiding visibility throughout the entrance, waiting, and treatment areas for ease of supervision by both staff and security personnel.
Given the aging of populations worldwide, older adults present another important patient profile that merits the attention of ED planners, designers, and healthcare managers. Watson et al. (1999) reported that elderly patients’ perceptions of ED care were influenced by information needs, wait times, professional competency and caring service, process and facility design, and personal tolerance/acceptance when their needs were not met. While reducing wait times is important, implementing rapid triage and diagnostic processes may not be ideal in the case of older adults with comorbidities. The broader literature base outside this review has also indicated that functional or cognitive impairments may make the experiences of elderly patients substantially different from those of other users (Hwang & Morrison, 2007). Accordingly, there is a need for further research on and the development of geriatric interventions, structural modifications, and process improvements specifically aimed at caring for older adults in emergency settings.
Implementation and Evaluation Dimensions—General Considerations
Though most field literature links ED experience to waiting, many authors contend that built spaces can support smooth service delivery at a macro level, beyond waiting-related experiences alone. Yet, the majority of physical improvements in the ED are made at the micro level, with resulting evidence being of an incremental and less generalizable nature (Cama, 2009). This concern is reflected in our review sample by Pati et al. (2014) and Pati et al. (2016), who noted that physical elements must be considered thoroughly during the initial design stage as these are impractical to modify once the ED is already built. For example, Saba and Bardwell (2004) show that the principles of universal design (accessibly designed buildings) have helped several EDs in the United States with adaptive change management goals, accounting for local needs in quality improvement, and ultimately, resulting in more inclusive and patient-centered EDs. Working across four EDs (one rural and three urban), Harvey et al. (2021) examined the challenges faced by ED patients in order to identify targeted design improvements at test sites as well as to develop an overarching provincial strategy for wider application at other EDs. Using a multimethod approach (patient interviews, patient surveys, staff surveys, staff interviews combined with department walkthroughs, journey mapping, and ethnographic observation), they identified four domains relevant for ED patient experience, grouped as: communication and expectations; layout, space, and wayfinding; privacy; and processes and staffing.
Developing and implementing patient-centered interventions in the ED is a broad-ranging enterprise that takes place at many levels and scales. The literature further emphasizes the necessity—and problematic lack—of participatory work in this domain, which suggests that diverse experiences (of both staff and patients) about particular pain points and local challenges are frequently overlooked (Abdelsamad et al., 2018; Annemans et al., 2018). Some authors described participatory means for ongoing and cyclical process/facility improvement, which we believe may prove particularly valuable for macro level, systemic change management in terms of patient-centered ED design. For instance, in a postoccupancy evaluation, Fay et al. (2017) identified workflow, communication, privacy, confidentiality, safety, and security as the key factors affecting ED experience. They presented a collaboratively conceived design charrette to translate their findings into practice and actively engage stakeholders in ongoing quality improvement processes. In another evaluation study, Piper et al. (2012) examined the effectiveness of experience-based co-design (EBCD) programs in three Australian EDs. The key informants in their study reported that EBCD was a useful and sustainable method for improving patient experience and health service quality at test sites. Similarly, Woitas et al. (2014) found that ED design proposals did not adequately meet ED needs, and consequently, implemented a participatory process resulting in the redesign of an ED with quiet, separate ED clinical work areas, universal patient rooms, and other patient-centered design features.
Limitations
Before concluding, we will note several limitations of this systematic review. First, since we only included English language articles, we may have missed relevant papers published in other languages. Second, while we have attempted to define the subject matter and scope of this investigation, our search strategy may not capture the terminologies utilized by others. This is partly, but not wholly, a result of differential keyword use (e.g., “person-centered,” “human-centered,” “patient-centered”). Given the diversity of disciplines contributing to the improvement of ED structures and processes, there are many extended technical areas (e.g., issues specific to process flow) that may describe some elements of what we are studying. Third, even when examining the same elements, authors may adopt variable conceptual meanings of terms like “design” and “healthcare environment.” Therefore, it is possible that scholarly characterizations of the phenomena pertinent to our research questions may differ from our own. Fourth, our search strategy omitted vocabulary for individual design attributes (e.g., acoustics, seating, light fixtures, signage boards) as these are beyond the scope of a single review, and therefore, we may have missed some papers of relevance that were not picked up by our search terms. Finally, while we focused on deriving insights with relevance for patient-centered ED design, further evidence could potentially be inferred from excluded papers where patient experience is not the main focus of analysis. Accordingly, we outline below some potential areas for future research, based on the evidence gaps identified through our review, as well as some important articles that did not meet our inclusion criteria.
Conclusion and Future Research Potential
This systematic review investigated the role of evidence-based health facility design on patients’ experiences of care in the ED. Our findings confirm previous literature where wait times, privacy, and communication are identified as the dominant factors influencing ED patient experience. This review adds that long wait times can be made more tolerable by creating a more supportive waiting environment, often facilitated through simple interventions. While physical design elements (e.g., layout, security features) are best considered during the initial construction phase, process flow mapping techniques are highly effective for increasing ED efficiency and reducing length of stay at existing EDs. Meanwhile, designing private areas without impeding patient monitoring needs has remained an unresolved challenge for ED designers, planners, and managers. Additionally, patient satisfaction is found to increase when patients’ needs for information about their health status are met and their involvement in medical decision-making is considered—a goal often achieved through the use of digital aids and empathetic staff communication. Individual and local factors—including patients’ embodied spatial experiences and sociodemographic differences—form important but often overlooked aspects in ED design. Finally, change implementation—whether through large-scale reconstruction or small-scale quality improvement activities—is more successful when stakeholders (both patients and staff) are consciously engaged throughout the research/design process. However, given that patients utilize EDs for one-time medical emergencies, it is challenging to plan and conduct participatory research involving patients in ED improvement. Further research is needed to understand how healthcare user perspectives can be incorporated meaningfully in the design of patient-centered EDs. Future researchers should also consider recent extensions of patient-centered care to emerging empathy-driven concepts like person-centered, human-centered, people-centered, and whole-person care—where patients are regarded as complex individuals with physical, behavioral, emotional, and social care needs, and importantly, as equal partners in care.
Among ineligible studies, staff experiences with the ED space (layout, structure, workflow, etc.) formed the main area of investigative focus (of these studies, we excluded those without adequate insights for patient experience). Acknowledging that staff satisfaction may implicitly influence patient satisfaction and experiences with care services, we highlight three subdomains from these studies that merit further investigation. The usability of the ED environment for staff affects their ability to provide appropriate, compassionate, efficient, and timely care to patients (Fay et al., 2018; Gharaveis et al., 2018; Meng et al., 2021; Zamani, 2019), suggesting a critical need to develop and validate models for staff engagement in ED design and improvement. Next, ED staff are particularly prone to burnout as a result of long hours spent working in a tense and volatile environment, and accordingly, staff respite areas to ameliorate stress constitute an important, but uncommon, domain for design intervention in the ED (Salmela et al., 2020). Finally, pertaining to both security concerns as well as staff emotional health, future research should explore how design can help safeguard against rising violence towards ED staff (Lenaghan et al., 2018).
In general, we found that research concerning ED design is often limited in scope to a single location, or targets individual design attributes within EDs, despite the widely recognized need for synergistic improvement methods more suited to the ED’s co-attendant structures and processes. In addition, local variations across EDs mean that quality improvement priorities—and strategies for addressing them—may differ greatly. In this regard, the literature offers promising evidence on the use of interdisciplinary techniques and stakeholder participation for attaining patient-centered outcomes in ED improvement. The need for diverse stakeholder perspectives (from both patients and staff) is especially pertinent for informing ED design; yet, the literature indicates limited representation in participatory knowledge generation from these groups. For this reason, we urge researchers to employ (and to report on their successes and failures with employing) participatory design approaches that harness these largely untapped knowledge sources when devising and conducting future ED quality improvement research. Additional investigation is warranted to further characterize the dynamic interaction of factors and diverse user group needs within the ED environments, and ultimately, to identify interventional strategies that improve patient experience effectively and holistically.
Implications for Practice
ED environment design is an emerging topic in health quality management and patient experience literature, showing significant development over the last decade.
Although widely correlated with patient satisfaction in other settings, EBD practices have seen limited application in ED settings.
We offer a structured and updated literature review to better understand how the ED environment drives patient experience and identify methodological and empirical insights for patient-centered ED design
In addition to classifying key findings under three dimensions relevant for ED environment design, we found that research and interventions within this domain are often limited in scope to a single location or target individual design attributes within EDs—despite the need for synergistic improvement methods that may better address the ED
There is strong evidence that stakeholder engagement and collaboration across fields can improve care quality and patient experience; however, future research should investigate how participatory quality improvement can best be achieved, given the diversity of factors and user groups in the ED.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867221137097 - The Impact of the Healthcare Environment on Patient Experience in the Emergency Department: A Systematic Review to Understand the Implications for Patient-Centered Design
Supplemental Material, sj-pdf-1-her-10.1177_19375867221137097 for The Impact of the Healthcare Environment on Patient Experience in the Emergency Department: A Systematic Review to Understand the Implications for Patient-Centered Design by Aidan Rowe and Michelle Knox in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Faculty of Arts, University of Alberta, Canada. Michelle Knox is funded by the Canadian Institutes of Health Research under funding reference number 170680.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.