
Abstract
Morinda officinalis, a traditional Chinese medicinal herb, has been used for centuries to enhance bone strength. This scoping review was conducted to comprehensively map and synthesise existing evidence regarding the osteoprotective effects of M. officinalis and the mechanisms through which these effects may occur. A systematic search was conducted using PubMed, Scopus, Web of Science, China National Knowledge Infrastructure, Wanfang, and the Chinese Science and Technology Journal Database, up to November 2025. Seventy-one studies that met the inclusion criteria were analysed. The findings revealed that M. officinalis and its bioactive constituents exert dual osteoprotective actions by promoting bone formation and inhibiting bone resorption. Key bioactive constituents of M. officinalis, including polysaccharides, anthraquinones, iridoid glycosides, and oligosaccharides, were shown to modulate critical signalling pathways such as Wnt/β-catenin, bone morphogenetic protein, Smad, receptor activator of nuclear factor kappa B ligand/osteoprotegerin, p38 mitogen-activated protein kinase, and nuclear factor kappa-B pathways. In cellular models, these constituents were found to enhance osteoblast proliferation, differentiation, and mineralisation, while suppressing the formation of, and inducing apoptosis in, osteoclasts. In animal models, particularly in rodents with ovariectomy-induced osteoporosis, treatment with M. officinalis was consistently associated with improvements in bone mineral density, the restoration of bone microarchitecture, enhanced biomechanical strength, and reductions in inflammation and oxidative stress. Preliminary clinical studies reported that M. officinalis decoction increased bone mineral density and improved bone turnover markers in individuals with osteoporosis. In conclusion, M. officinalis exhibits a multi-constituent and multi-target profile, offering a promising therapeutic approach in osteoporosis through the synergistic actions of its diverse bioactive constituents. Although the preclinical evidence is substantial, high-quality and large-scale clinical trials are required to confirm its efficacy and safety in humans.
Introduction
Osteoporosis is a prevalent metabolic bone disorder characterised by reduced bone mineral density (BMD) and the deterioration of the bone microarchitecture, which increases the risk of fractures, particularly in the hip, spine, and wrist. 1 The prevalence of osteoporosis and osteopenia worldwide was reported to be 19.7% and 40.4%, respectively, according to a meta-analysis in 2022. 2 Compared with age-matched men, postmenopausal women are particularly susceptible to osteoporosis. 3 Fragility fractures associated with osteoporosis lead to significant impairments in mobility and quality of life and elevated mortality rates.4,5 Furthermore, the socioeconomic burden of osteoporosis is substantial, contributing to rising healthcare costs, rehabilitation needs, and requirements for long-term care.6,7
Conventional pharmacological treatments for osteoporosis, including bisphosphonates, selective oestrogen receptor modulators, hormone replacement therapy, and biologic agents such as denosumab and teriparatide, effectively reduce the risk of fractures. However, these treatments are often associated with challenges such as adverse effects and poor long-term adherence. 8 Although they are effective in preventing both vertebral and non-vertebral fractures, these therapies have limitations, including the potential for rare but serious complications.9,10 Consequently, there is increasing interest in complementary approaches such as Traditional Chinese Medicine (TCM), which offers a holistic approach and has been shown to promote bone regeneration with minimal side effects.11,12 Integrating TCM into conventional treatments may represent a more comprehensive approach to osteoporosis management and improve patient outcomes.
Morinda officinalis, known as Bajitian in TCM, is a widely used herbal remedy renowned for its tonic effects, particularly in strengthening bones and nourishing the kidneys. 13 In TCM, kidney deficiency is believed to significantly impact bone health, leading to the historical use of M. officinalis in treating conditions related to bone degeneration.14,15 Recent pharmacological studies have demonstrated that M. officinalis exerts therapeutic effects through various bioactive compounds, including polysaccharides and anthraquinones, which have been shown to stimulate osteoblast activity while inhibiting osteoclast-mediated bone resorption.16,17 For example, specific anthraquinones isolated from M. officinalis exhibit significant antiosteoporotic properties by promoting osteoblast proliferation and enhancing alkaline phosphatase (ALP) activity. 18 These multifaceted actions highlight the potential of M. officinalis as a valuable therapeutic agent in managing osteoporosis and supporting bone health.
This scoping review will summarise the literature on the potential role of M. officinalis in the management of osteoporosis. Specifically, this review will focus on its mechanisms of action, the bioactive compounds involved, and preclinical evidence supporting its use as an adjunct or alternative therapy for osteoporosis.
Materials and Methods
This scoping review was conducted following the established methodological framework developed by Arksey and O'Malley 19 and adheres to the reporting guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews. 20 The protocol of this scoping review had been registered in the Open Science Framework (url: https://osf.io/mkezj/). The primary objective was to systematically map and synthesise the available evidence regarding the effects of M. officinalis on bone health and its potential role in osteoporosis management.
Specifying the Research Question
Our review was guided by a single primary research question, structured using the PCC (Population, Concept, Context) framework. It aimed to investigate the effects of M. officinalis, its extracts, and isolated chemical constituents in bone health and the prevention of osteoporosis. The “Population” encompassed bone cells (osteoblasts, osteoclasts, and osteocytes), animal models of osteoporosis, and human subjects at risk for osteoporosis. The “Concept” focused on the effects of M. officinalis and its derived compounds on bone health, while the “Context” addressed their mechanisms of action and overall effects on bone health in the context of osteoporosis.
Identifying the Relevant Literature
A systematic literature search was performed in November 2025 across three international databases (PubMed, Scopus, and Web of Science) and three Chinese databases (China National Knowledge Infrastructure, Wanfang, and the Chinese Science and Technology Journal Database). The search strategy was designed to encompass all relevant studies without date restrictions. The search string utilised a combination of keywords related to M. officinalis and bone health. The search string used was (“Morinda officinalis” OR “Indian Mulberry Root” OR “Noni Root” OR “Bajitian” OR “Morinda Root”) AND (osteoporosis OR bone OR skelet* OR osteoblast* OR osteoclast* OR osteocyte* OR fracture*). For Chinese databases, the terms “巴戟天” and “骨质疏松” were applied. The search was limited to titles and abstracts to enhance specificity.
Selecting Studies
All identified records were collated and managed using EndNote software (version 21.2, Clarivate, PA, USA), and duplicates were removed. The selection process consisted of two consecutive screening phases, conducted independently by all six authors (YZW, GJC, QW, XJ, XDM, and KYC) working in pairs. Any discrepancies between reviewers during the selection process were resolved through discussion.
The articles were first screened based on title and abstract against predefined inclusion criteria. The full texts of relevant articles were retrieved and thoroughly examined before final inclusion. Studies fulfilling all the following criteria were included: (1) original research articles published in English or Chinese; (2) studies examining the effects of M. officinalis, its extracts, or purified compounds on bone-related cells, animal models of bone disease, or human bone health; (3) studies reporting measurable outcomes related to bone health, such as BMD, bone microstructures, strength, and remodeling, and bone cell activities.
Studies with any of the following criteria were excluded: (1) publications without primary data, such as reviews, commentaries, editorials, or letters to the editor; (2) conference proceedings and abstracts, because the data presented are not complete and potentially overlap with full-length articles; (2) studies that used M. officinalis as a part of complex herbal mixtures, as effects on bone health could not be attributed specifically to the herb; (3) studies that did not report outcomes related to bone health.
Extracting, Mapping, and Charting the Data
Data from the studies included were extracted into a standardized data-charting form by two independent reviewers (YZW and GJC). The extracted items comprised (1) study identifiers and publication years; (2) the study design and model type (eg, cell line or animal species); (3) specific intervention details, including the extract type, purified compound, and dosage; (4) the duration of the intervention; (5) key findings related to bone health, such as molecular mechanisms, histological alterations, and biomechanical outcomes. The primary data chart also incorporated the following core fields: authors (year), animal/cell model, treatment, dosage/duration, and effects.
Summarising, Synthesising, and Reporting the Results
Given the heterogeneous nature of the studies included in terms of experimental models, interventions, and outcome measures, a narrative synthesis approach was adopted. The findings were organized thematically to address the review's objectives rather than being subjected to a quantitative meta-analysis. Ethical approval was not required, as all data were obtained from previously published studies.
Results
Study Selection
The initial database search yielded 479 records. After the removal of duplicates (n = 205), a total of 274 unique articles were screened based on titles and abstracts. Of these, 201 articles were excluded for the following reasons: (1) not original research (n = 82); (2) not within the scope of the review (n = 51); (3) the use of multi-herb formulations rather than M. officinalis alone (n = 69). In total, 71 articles were retrieved for full-text assessment, all of which met the final inclusion criteria. The study selection process is presented in Figure 1.
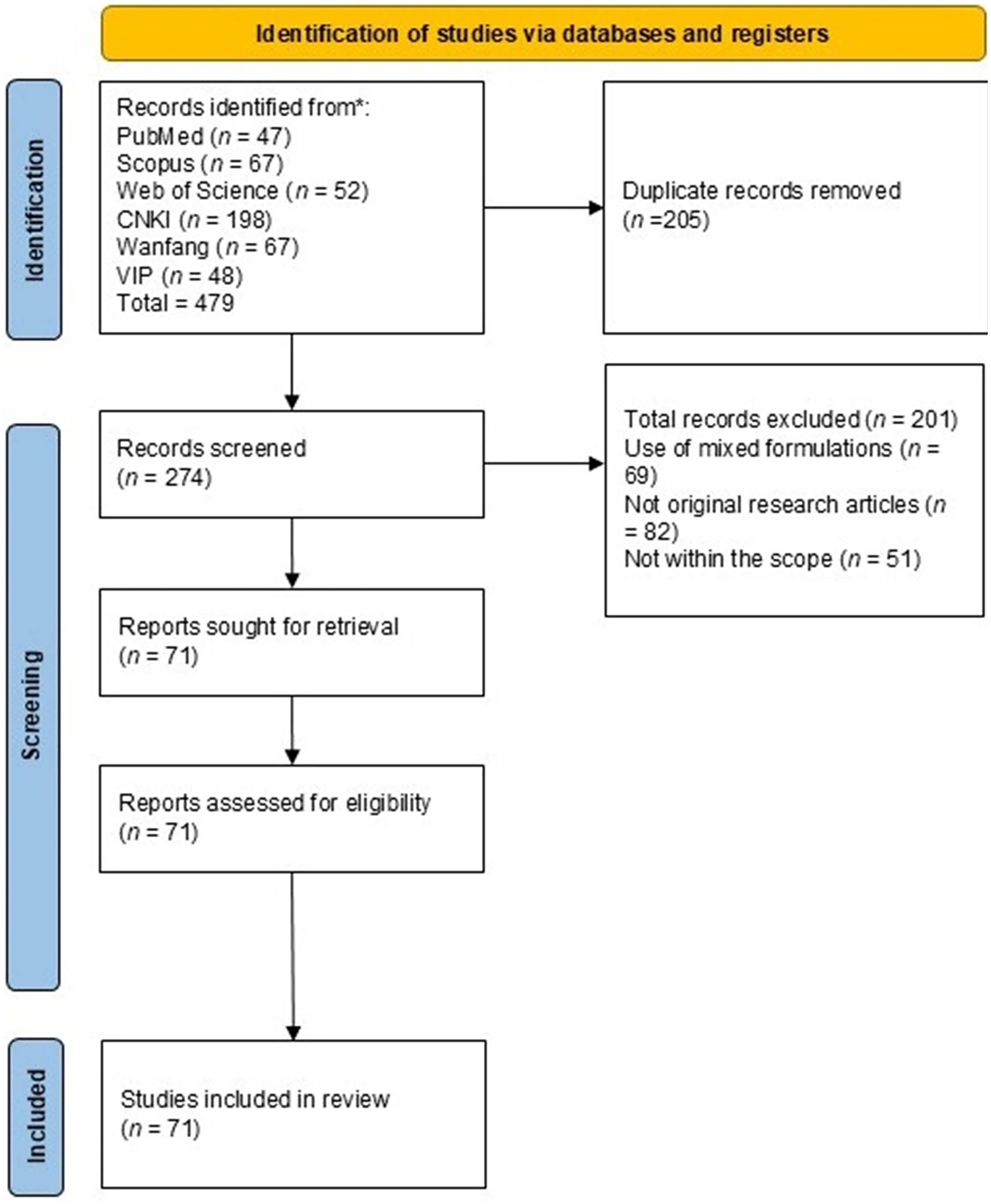
Flowchart showing the selection of articles. Abbreviations: CNKI, China National Knowledge Infrastructure; VIP, Chinese Science and Technology Journal Database.
The 71 studies incorporated diverse research designs, including in vitro and in vivo approaches. Both cellular and animal models were used to assess the osteoprotective effects of these compounds. The in vivo studies (n = 50) primarily utilised ovariectomised (OVX) rats (n = 32)21–52 and glucocorticoid-induced osteoporosis models (n = 2),53,54 along with other models, including zebrafish 55 and AA chickens. 56 All studies included in vitro experiments, with 32 employing cell-based assays and 23 integrating both in vitro and in vivo approaches. Cellular investigations focused on osteoblastogenesis and osteoclastogenesis, utilising diverse cell lines, such as bone marrow-derived mesenchymal stem cells (BMSCs),49,51,54,57–62 human BMSCs (hBMSCs), 57 osteoblastic MC3T3-E1 cells,47,50,52,63–66 bone marrow macrophages (BMMs),54,67 osteoclast precursors,17,31,38,39,58,68–70 primary osteoblasts (OBs),17,68,71–79 and RAW 264.7 macrophages.67,80
Phytochemical Profiles and Formulations Studied
A significant number of studies (n = 25) investigated various crude extracts and formulations of M. officinalis, including aqueous decoctions, ethanol extracts, and medicated sera.29–34,38,39,41–45,53,61,64,68,70,72,73,75,76,79,81,82 One investigation focused on a complex multi-constituent preparation derived from M. officinalis F.C. How, in which at least 26 phytochemicals were identified, predominantly anthraquinone derivatives and iridoid glycosides. 55 Of particular interest was the innovative examination of M. officinalis-derived extracellular vesicle-like particles, which represent a novel approach to investigating the therapeutic potential of plants and demonstrating the remarkable diversity of their bioactive constituents. 65
Other studies focused on bioactive compounds derived from M. officinalis, with the majority (n = 31) examining M. officinalis polysaccharides (MOPs), including structurally characterized fractions such as MOP 70–2, MOP50–2, MOW50–1, and MO90–1, as well as mixed polysaccharide extracts.21–26,28,35–37,46,47,49,52,54,56–58,62,63,66,71,72,77–80,83–86 Anthraquinones (n = 8) represented another key focus, with studies analyzing specific derivatives, including rubiadin,40,74 rubiadin-1-methyl ether, 2-hydroxymethyl-3-hydroxyanthraquinone, and other analogues.17,87–91 Additionally, five studies explored the iridoid glycoside monotropein and other iridoid glycosides,27,50,59,69,92 whereas others investigated oligosaccharides, such as nystose and bajijiasu, along with M. officinalis saponins (Table 1).51,60,67
Classification and Bioactive Compounds/Extracts of M. officinalis.

Classification and Bioactive Compounds/Extracts of M. officinalis.
Abbreviations: MOP, M. officinalis polysaccharides; MOH, M. officinalis F.C. How; MOEVLPs, M. officinalis-derived extracellular vesicle-like particles.
Across in vitro and in vivo models, preparations derived from M. officinalis were consistently shown to exert osteoprotective effects. Serum derived from animals administered with M. officinalis granules or extracts was found to suppress osteoclast differentiation, reduce the expression of key osteoclastogenic markers such as receptor activator of nuclear factor κB
(RANK), carbonic anhydrase II, and nuclear factor of activated T-cells 2, and diminish resorptive activity.31,70,76 Simultaneously, osteoblast function was promoted through the enhanced proliferation of bone marrow mesenchymal stem cells and the upregulation of osteogenic transcription factors, including core-binding factor alpha 1 (Cbfa1) [also known as runt-related transcription factor 2 (RUNX2)].61,76
In OVX and glucocorticoid-induced osteoporotic rodents, water and ethanol extracts were reported to increase BMD, improve the trabecular architecture, elevate the maximum tibial load, and modulate bone turnover markers, partly through the suppression of RANK ligand (RANKL) signaling and the regulation of metabolic pathways such as arachidonic acid, lipid, and nucleic acid metabolism.30,38,39,41,44,53 Certain preparations also appeared to influence endocrine pathways, as increases in circulating oestrogen and osteoprotegerin (OPG), along with reductions in ALP and RANKL, were observed following chronic administration.33,41
Other studies reported improvements in antioxidant capacity and musculoskeletal endurance, although direct bone outcomes were not always measured. 81 Taken together, the findings for monomeric constituents, aqueous and ethanolic extracts, and clinical-type granules suggest that M. officinalis exerts complementary anabolic and anti-resorptive actions, thereby supporting bone mass preservation and trabecular integrity across diverse experimental paradigms. A consolidated overview of these observations is presented in Table 2, which summarises evidence on the effects of various preparations across bone-related in vitro and in vivo models.
Summary of Effects of Different M. officinalis Extracts and Formula Granules on Bone Health Outcomes.

Summary of Effects of Different M. officinalis Extracts and Formula Granules on Bone Health Outcomes.
Abbreviations: ↑, upregulation/increase; ↓, downregulation/decrease; AA, arachidonic acid; ALP, alkaline phosphatase; BMD, bone mineral density; BMSCs, bone marrow mesenchymal stem cells; CA II, carbonic anhydrase II; Cbfa1, core-binding factor alpha 1; CTX-I, C-terminal telopeptide of type I collagen; DEX-rats, dexamethasone-treated rats; E2, oestradiol; GSH-Px, glutathione peroxidase; mRNA, messenger ribonucleic acid; NFAT2, nuclear factor of activated T-cells 2; OB, osteoblasts; OC, osteoclasts; OPG, osteoprotegerin; OVX, ovariectomized; RANK, receptor activator of nuclear factor kappa-B; RANKL, receptor activator of nuclear factor kappa-B ligand; SD rat, Sprague Dawley rat; SOD, superoxide dismutase; Tb.Sp, trabecular separation; Tb.Th, trabecular thickness; TRAP, tartrate-resistant acid phosphatase.
However, these studies suffered from a critical limitation in that the phytochemical profile of the crude extracts was not characterised or standardised, limiting reproducibility.
Growing evidence suggests that MOP is a promising natural therapeutic candidate in both the prevention and management of osteoporosis. Evidence from both in vitro and in vivo studies has demonstrated that MOP can promote osteogenesis, inhibit bone resorption, regulate bone metabolism, and modulate key signalling pathways associated with bone health.
Effects of MOP on Bone Cells
In vitro evidence suggests that MOP exhibits both osteogenic and anti-resorptive activities by promoting stem cell differentiation and osteoblast activation, while concurrently suppressing osteoclastogenesis.
In hBMSCs, MOP (80 µg/mL) significantly promoted osteogenic differentiation while inhibiting adipogenesis through modulation of the miR-210–3p/SCARA3 axis. This was reflected by increased expression of ALP, bone morphogenetic protein (BMP) 4, and RUNX2, reduced expression of proliferator-activated receptor gamma (PPAR-γ) and CCAAT/enhancer-binding protein (CEBP)-α, enhanced cell viability, and reduced apoptosis. 57 Similar osteogenic activity was observed in rat BMSCs, where MOP (10-40 µg/mL) activated the Wnt/β-catenin pathway, upregulated RUNX2, osteocalcin (OCN), collagen type I alpha 1 chain (COL1A1), and Osterix, and increased mineralisation. 62 Additional mechanistic work showed that osteoblast differentiation was driven through the miR-21/phosphatase and tensin homolog (PTEN)/phosphoinositide 3-kinase (PI3 K)/protein kinase B (AKT) pathway, accompanied by the suppression of adipogenic signalling. 49
In MC3T3-E1 pre-osteoblasts, different MOP fractions exhibited distinct activities. MOP70–2 (16.1-80.4 µM) markedly enhanced proliferation, differentiation, and mineral deposition in a time- and concentration-dependent manner over 3–21 days. 66 The fructan-rich fraction MOW50–1 (5-40 µg/mL) increased ALP activity, whereas MOP50–2 showed no significant effect, indicating that specific fructan components were key contributors to osteogenic activity. 47 Prolonged exposure to MOW90–1 (50-250 µg/mL) further upregulated RUNX2, Osterix, OCN, and osteopontin (OPN) and promoted robust mineralisation over 18 days. 52 The osteogenic potential of MOP in this model was further supported by findings showing that enzymatically extracted polysaccharides significantly enhanced cell proliferation, ALP activity, and the secretion of collagen type I and OCN in a concentration-dependent manner. Acidic polysaccharides with a defined structural profile were also reported to markedly promote osteoblast proliferation and differentiation, thereby reinforcing the role of MOP as an effective osteogenic stimulant. 63
MOP also exerted marked anti-resorptive effects. MOP-derived exosomes inhibited osteoclast differentiation in bone marrow macrophages by suppressing genes associated with bone resorption and reducing their proliferative capacity. These effects were mediated through the downregulation of prostaglandin-endoperoxide synthase 2 (PTGS2) and were shown to counteract glucocorticoid-induced osteoclast activation. 54 In RAW264.7 macrophages, serum containing MOP (derived from 1-2 g/kg in vivo dosing) induced osteoclast apoptosis and inhibited differentiation in a dose-dependent manner by downregulating miR-214–3p, thereby increasing neural precursor cell-expressed developmentally downregulated 4-like (NEDD4L) expression. The silencing of NEDD4L prevented these protective effects, confirming the role of the miR-214–3p/NEDD4L axis. 80
Earlier investigations further supported the osteogenic potential of MOP. Aqueous extracts of M. officinalis significantly enhanced primary osteoblast proliferation in a dose-dependent manner, with maximal activity at 100 µg/mL. 77 Increased ALP activity elevated intracellular OCN, and the upregulation of transforming growth factor (TGF)-β1 mRNA indicated stimulated differentiation and collagen synthesis. 77 Purified MOP displayed superior efficacy to crude extracts, leading to pronounced increases in proliferation, ALP activity, OCN secretion, and TGF-β1 expression at 100–200 g/L. 71
Additional mechanistic insights were provided by studies in rat BMSCs, where MOP enhanced ALP activity, mineralised nodule formation, and RUNX2 and OPN expression via p38 mitogen-activated protein kinase (MAPK) activation; the inhibition of p38 markedly reduced these effects. 58 MOP-containing serum further suppressed Dickkopf-related protein 1 (DKK-1), facilitated activation of the Wnt/β-catenin pathway, and reduced osteoblast apoptosis by modulating B-cell lymphoma 2 (Bcl-2) and Bcl-2–associated×protein (Bax) expression.78,79
Anti-resorptive effects were confirmed in multi-cell systems. In co-cultures, MOP-containing serum increased OPG mRNA expression and reduced the RANKL mRNA expression. 68 Aqueous extracts produced a dose-dependent increase in both OPG/RANKL mRNA and protein ratios in mesenchymal stem cells.72,73 Iridoid glycosides from M. officinalis further suppressed tartrate-resistant acid phosphatase (TRAP) activity and reduced bone resorption capacity without affecting cell viability. 69 Additional solvent fractions, including the n-butanol fraction and residual ethanol extracts, also promoted osteoblast proliferation, ALP secretion, OCN production, and TGF-β1 expression.64,75
Overall, these findings demonstrate that MOP regulates bone remodelling through the coordinated activation of the p38 MAPK and Wnt/β-catenin pathways, the modulation of pro-osteogenic and anti-resorptive gene networks, and interactions with active fructan-rich fractions, such as MOW50–1 and MOW90–1. This multi-target profile highlights its potential as a promising therapeutic candidate in osteoporosis (Table 3).
In vitro Evidence of the Effects of MOP on Osteogenesis and Osteoclastogenesis in Cellular Models.

In vitro Evidence of the Effects of MOP on Osteogenesis and Osteoclastogenesis in Cellular Models.
Abbreviations: ↑, upregulation/increase; ↓, downregulation/decrease; ALP, alkaline phosphatase; Bax, BCL2-associated X protein; Bcl-2, B-cell lymphoma 2; BMP2/4, bone morphogenetic protein 2/4; BMSCs, bone marrow mesenchymal stem cells; BSP, bone sialoprotein; CC3, cleaved caspase-3; CEBP-α, CCAAT/enhancer-binding protein alpha; COL I, type I collagen; CTSK, cathepsin K; CTX, C-terminal telopeptide of type I collagen; DKK-1, Dickkopf-1; DPD, deoxypyridinoline; GSK3β, glycogen synthase kinase-3 beta; hBMSCs, human bone marrow mesenchymal stem cells; HEK293, human embryonic kidney 293 cells; Hyp, hydroxyproline; MC3T3-E1, mouse calvarial pre-osteoblasts; miR-101-3p, MicroRNA-101-3p; miR-210-3p, MicroRNA-210-3p; miR-214-3p, MicroRNA-214-3p; MMP9, matrix metalloproteinase 9; MO, M. officinalis; MOP, M. officinalis polysaccharides; MOP-Exo, exosomes derived from MOP-treated cells; MOP70-1/MOP70-2, inulin-type fructan fractions of MOP; MOW50-1/MOW90-1, active polysaccharide subfractions of M. officinalis; mRNA, messenger ribonucleic acid; NEDD4L, neural precursor cell-expressed developmentally downregulated protein 4-like; OB, osteoblast; OC, osteoclast; OCN, osteocalcin; OPG, osteoprotegerin; OPN, osteopontin; Osx, Osterix; p-GSK3β, phosphorylated glycogen synthase kinase-3 beta; PI3 K/AKT, phosphatidylinositol 3-kinase/protein kinase B signalling pathway; PPAR-γ, peroxisome proliferator-activated receptor gamma; PTGS2, prostaglandin-endoperoxide synthase 2; RANKL, receptor activator of nuclear factor kappa-B ligand; rBMSCs, rat bone marrow mesenchymal stem cells; RUNX2, runt-related transcription factor 2; SCARA3, scavenger receptor class A member 3; SD, Sprague Dawley; TGF-β1, transforming growth factor-beta 1; TRAP, tartrate-resistant acid phosphatase; Wnt/β-catenin, wingless/β-catenin signalling pathway.
The anti-osteoporotic efficacy of MOP was consistently verified across multiple animal models, most notably in OVX rodents. In OVX rats, MOP administration was repeatedly shown to attenuate bone loss, as reflected by significant increases in BMD, bone mineral content (BMC), and serum OCN and 1,25-dihydroxyvitamin D₃ levels. 37 Further support for these effects was provided in studies in which 400 mg/kg MOP was administered for one month, resulting in a significant increase in BMD while TRAP-5b and N-telopeptide of type I collagen (NTx) decreased, indicating reduced bone resorption. 57 The restoration of bone remodelling balance was indicated by the upregulation of OPG mRNA, the suppression of RANKL mRNA, and a reduced RANKL/OPG ratio in the lumbar vertebra. 22 Dose-dependent improvements in BMD were also reported, accompanied by elevations in serum 5-hydroxytryptamine (5-HT) and vascular endothelial growth factor. 21 Similarly, 400 mg/kg MOP administered for four weeks improved BMD and restored bone turnover through increases in bone-specific ALP (BALP) and bone Gla protein, further indicating beneficial effects on postmenopausal bone metabolism. 49
Mechanistic investigations further demonstrated that MOP enhanced bone mass by upregulating osteogenic genes, such as BMP-2 and Cbfa1. 23 The OPG/RANK/RANKL pathway was identified as a principal regulatory target, with MOP dose-dependently improving femoral neck BMD and restoring disrupted signalling by increasing OPG while suppressing RANK and RANKL expression. 24 Consistently, M. officinalis oligosaccharides (MOOs) were also shown to exert osteoprotective effects in OVX rats by modulating this pivotal pathway. Treatment with MOO significantly increased bone formation markers [BALP, procollagen type I N-terminal propeptide (P1NP)], BMD, trabecular number, and OPG expression, while reducing bone resorption markers [TRACP-5b, C-terminal telopeptide of type I collagen (CTX-1)], trabecular spacing, osteoclast number, and RANKL expression. High doses of MOOs (75 mg/kg/day) showed effects on bone mass, microstructure, and biomechanical strength comparable to those of alendronate sodium, primarily through the regulation of the OPG/RANKL signalling axis. 45 This effect on OPG was partially attributed to reductions in the pro-inflammatory cytokines interleukin-1 (IL-1) and tumour necrosis factor-α (TNF-α). 35 Consistently, MOP dose-dependently reduced serum TNF-α and IL-6, improved the trabecular architecture, and enhanced biomechanical properties. 26
Additional mechanisms were also elucidated. The mitigation of oxidative stress contributed to improved bone microarchitecture, with monotropein, a key iridoid glycoside, shown to alleviate osteoporosis through antioxidant activity. 27 Furthermore, it was concluded that the anti-osteoporotic effect of MOP likely involves the inhibition of the Notch1/hairy and enhancer of split-1/peroxiredoxin-1 pathway. 28 Benefits beyond direct bone regulation were noted, including the modulation of serum trace elements and inflammatory cytokines, 36 as well as the improvement of both lipid metabolism and bone metabolism in OVX rats fed a high-fat diet. 43 MOP was also reported to improve bone mass, bone strength, and bone microstructure while reducing circulating oxidised low-density lipoprotein levels and downregulating β2-adrenergic receptor protein expression. 25
The therapeutic potential of MOP was extended to other osteoporosis models. In a rodent model of glucocorticoid-induced osteoporosis, MOP administration was shown to improve trabecular bone microarchitecture and reduce osteoclast activity. 54 In aged rats, MOP supplementation was found to increase femoral and vertebral BMD, improve bone strength, and reduce serum ALP and IL-6 levels. 84 Furthermore, in a broiler model of tibial dyschondroplasia, MOP was demonstrated to restore tibial growth plate morphology and calcium, as well as phosphorus metabolism, which was linked to the upregulation of BMP-2, Mothers against decapentaplegic homolog 4 (Smad4), and RUNX2. 56
Active subfractions of MOP, such as MOW50–1 and MOW90–1, were specifically investigated. MOW50–1 was shown to preserve bone architecture and stimulate osteoblast activity, 47 while MOW90–1 was found to enhance femoral BMD and trabecular structure by upregulating osteogenic markers, including RUNX2, Osterix, OPN, and OCN. 52 In male Wistar rats, MOP treatment was reported to upregulate osteogenic genes and modulate the RANKL/OPG ratio, further supporting its role in the transcriptional regulation of bone metabolism. 83
Multiple studies in OVX rats demonstrated dose-dependent improvements in BMD and mineral balance following oral MOP administration (100-300 mg/kg, 30 days), alongside reductions in pro-inflammatory cytokines, indicating anti-inflammatory and mineral-regulatory effects. 85 Subcutaneous MOP injection (50-75 mg/kg, three weeks) enhanced osteoblast activity and rebalances bone remodelling via the modulation of the OPG/ RANKL/RANK pathway. 86 At higher doses (300 mg/kg, eight weeks), MOP improved the trabecular structure and antioxidant status by suppressing the PGC-1α/peroxisome PPAR-γ pathway, a mechanism that was reversed upon pathway activation, confirming its mechanistic role. 46 In OVX mice, MOP (500 mg/kg, four weeks) elevated BMD and induced osteoclast apoptosis through the miR-214–3p/ NEDD4L axis, which involves the upregulation of proapoptotic markers (Bax and cleaved caspase-3) and the downregulation of Bcl-2. 80
MOP demonstrates osteoprotective effects by promoting bone formation through key osteogenic pathways (Wnt/β-catenin, BMP/Smad, and OPG/RANKL/RANK), inhibiting osteoclast differentiation via the miR-101–3p/PTGS2 and miR-214–3p/NEDD4L pathways, and restoring mineral balance alongside antioxidant and anti-inflammatory functions. These results support the traditional use of M. officinalis and offer a mechanistic basis for its potential clinical application in osteoporosis treatment. These findings validate the traditional use of M. officinalis and provide a mechanistic foundation for its clinical translation in osteoporosis management (Table 4).
Evidence of the Antiosteoporotic Effects of MOP in Animal Models.

Evidence of the Antiosteoporotic Effects of MOP in Animal Models.
Abbreviations: ↑: upregulation/increase; ↓: downregulation/decrease; 1,25(OH)₂D₃, 1,25-dihydroxyvitamin D3; 5-HT, 5-hydroxytryptamine (Serotonin); ADRB2, β2-adrenergic receptor; ALP, alkaline phosphatase; BALP, bone-specific alkaline phosphatase; Bax, Bcl-2-associated X protein; Bcl-2, B-cell lymphoma 2; BGP, Bone Gla Protein (Osteocalcin); BMC, bone mineral content; BMD, bone mineral density; BMP, bone morphogenetic protein; BMP-2, bone morphogenetic protein 2; BV/TV, bone volume/tissue volume; Cbfa1, core-binding factor alpha 1 (Runx2); Conn.D, connectivity density; CTX-1, C-terminal telopeptide of type I collagen; Dmp1, dentin matrix acidic phosphoprotein 1; DPD, deoxypyridinoline; GIOP, glucocorticoid-induced osteoporosis; GSH-PX, glutathione peroxidase; HDL-C, high-density lipoprotein cholesterol; Hes1, Hairy and enhancer of split-1; HOP, hydroxyproline; IL, interleukin; IL-1, interleukin-1; IL-6, interleukin-6; LDL-C, low-density lipoprotein cholesterol; MDA, Malondialdehyde; miR-101-3p, MicroRNA-101-3p; miR-214-3p, MicroRNA-214-3p; MMP-9, Matrix Metalloproteinase-9; MO, M. officinalis; MO90, 90% ethanol extract of M. officinalis; MOO, M. officinalis oligosaccharide; MOP, M. officinalis polysaccharide; NEDD4L, neural precursor cell expressed developmentally downregulated 4-like; Notch1, neurogenic locus notch homolog protein 1; NTx, N-telopeptide of type I collagen; OCN, osteocalcin; OPG, osteoprotegerin; OVX, ovariectomised; OX-LDL, Oxidized Low-Density Lipoprotein; P, phosphorus; PGC-1α, peroxisome proliferator-activated receptor-gamma coactivator 1-alpha; PPAR-γ, peroxisome proliferator-activated receptor gamma; Prdx1, peroxiredoxin 1; RANK, receptor activator of nuclear factor kappa B; RANKL, receptor activator of nuclear factor kappa B ligand; RUNX2, runt-related transcription factor 2; rALP, rat alkaline phosphatase; rOPG, rat osteoprotegerin; rPPAR-γ2, rat peroxisome proliferator-activated receptor gamma 2; rRANKL, rat receptor activator of nuclear factor kappa B ligand; SD, Sprague Dawley; SMI, Structure Model Index; Smad4, mothers against decapentaplegic homolog 4; SOD, superoxide dismutase; Tb.N, trabecular number; Tb.Sp, trabecular separation; Tb.Th, trabecular thickness; TC, total cholesterol; TG, triglyceride; TNF-α, tumour necrosis factor-alpha; TRACP/TRAP, tartrate-resistant acid phosphatase; TRACP-5b, tartrate-resistant acid phosphatase 5b; VEGF, vascular endothelial growth factor.
The anti-osteoporotic potential of anthraquinones, the principal bioactive constituents of M. officinalis, was also investigated. These compounds were found to exhibit dual regulatory effects in bone remodelling, promoting osteogenesis while suppressing osteoclastogenesis, with their mechanisms of action being influenced by specific structural features.17,18,90
On the osteogenic front, certain anthraquinones were demonstrated to activate the Wnt/β-catenin pathway, a key signalling axis in bone formation. The derivative M13 significantly stimulated osteogenic differentiation in mesenchymal stem cells and embryonic limb explants, an effect achieved via glycogen synthase kinase-3β phosphorylation, β-catenin nuclear translocation, and the upregulation of osteogenic markers, including RUNX2, COL1A1, and OPN. 18 The pathway specificity was confirmed, as these effects were negated by a Wnt inhibitor. Furthermore, specific anthraquinones, namely, 2-hydroxy-1-methoxyanthraquinone and 13,8-trihydroxy-2-methoxyanthraquinone, were shown to enhance osteoblast proliferation and alkaline phosphatase activity at nanomolar concentrations. 17
Concurrently, potent antiresorptive effects were observed. In vitro, rubiadin was demonstrated to inhibit osteoclast formation, TRAP activity, and bone resorption pit formation in a concentration-dependent manner. A reduction in cathepsin K activity was also reported, indicating the suppression of osteoclast functional capacity. 74 Another compound, rubiadin-1-methyl ether (RBM), was found to attenuate RANKL-induced nuclear factor-kappa B (NF-κB) activation by reducing p65 phosphorylation and nuclear translocation, leading to a lower expression of key osteoclastogenic genes and impaired F-actin ring formation. 90 Furthermore, RBM was shown to disrupt Beclin1-dependent autophagy, which contributed to the inhibition of osteoclast differentiation. 91 More broadly, anthraquinones were reported to increase the OPG/RANKL ratio and induce early apoptosis in osteoclast precursors. 87
These in vitro findings were substantiated in preclinical in vivo studies. In an OVX rat model, the administration of M. officinalis total anthraquinone effectively reduced urinary calcium and phosphate excretion, suppressed bone resorption markers, and partially preserved bone formation, thereby preventing bone loss without exhibiting uterotrophic effects. 40 Similarly, treatment with ethanol extracts of the roots was shown to improve trabecular BMD and reduce resorption markers in OVX rats. The administration of rubiadin was also reported to increase serum P1NP and oestradiol levels, while reducing CTX-1 in OVX rats. Transcriptomic analyses revealed supportive changes in gene expression. 89
In summary, anthraquinones from M. officinalis have been demonstrated to exert osteoprotective effects through multi-target mechanisms, primarily involving the activation of osteogenic Wnt/β-catenin signalling and the suppression of osteoclastogenesis via NF-κB and autophagy pathways. While preclinical evidence is promising, clinical validation is currently lacking, and the potential synergistic effects between anthraquinones and polysaccharides from this herb warrant further exploration. 88
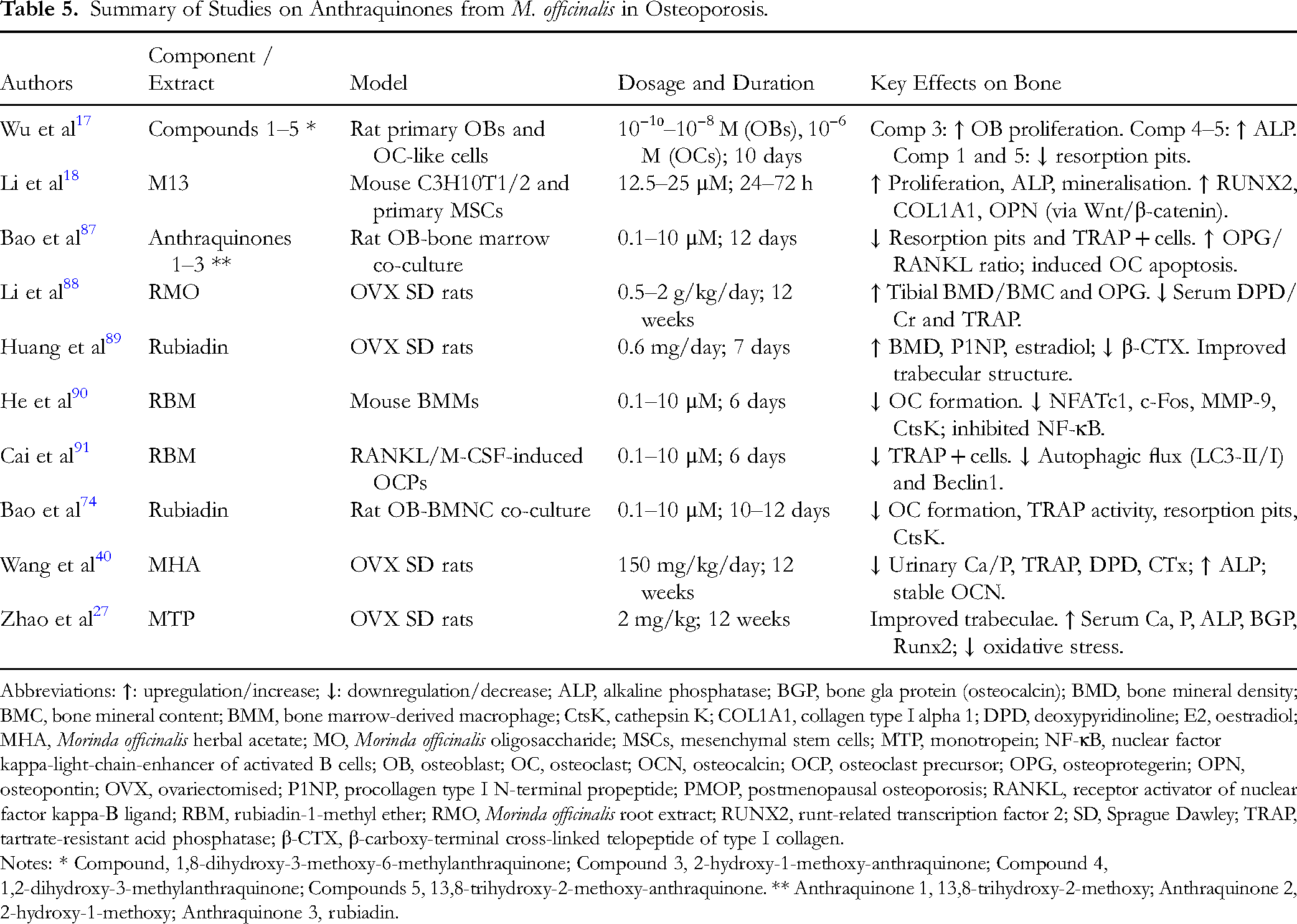
A summary of the evidence concerning the therapeutic potential of anthraquinones from M. officinalis is presented in Table 5.
Summary of Studies on Anthraquinones from M. officinalis in Osteoporosis.
Summary of Studies on Anthraquinones from M. officinalis in Osteoporosis.
Abbreviations: ↑: upregulation/increase; ↓: downregulation/decrease; ALP, alkaline phosphatase; BGP, bone gla protein (osteocalcin); BMD, bone mineral density; BMC, bone mineral content; BMM, bone marrow-derived macrophage; CtsK, cathepsin K; COL1A1, collagen type I alpha 1; DPD, deoxypyridinoline; E2, oestradiol; MHA, Morinda officinalis herbal acetate; MO, Morinda officinalis oligosaccharide; MSCs, mesenchymal stem cells; MTP, monotropein; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; OB, osteoblast; OC, osteoclast; OCN, osteocalcin; OCP, osteoclast precursor; OPG, osteoprotegerin; OPN, osteopontin; OVX, ovariectomised; P1NP, procollagen type I N-terminal propeptide; PMOP, postmenopausal osteoporosis; RANKL, receptor activator of nuclear factor kappa-Β ligand; RBM, rubiadin-1-methyl ether; RMO, Morinda officinalis root extract; RUNX2, runt-related transcription factor 2; SD, Sprague Dawley; TRAP, tartrate-resistant acid phosphatase; β-CTX, β-carboxy-terminal cross-linked telopeptide of type I collagen.
Notes: * Compound, 1,8-dihydroxy-3-methoxy-6-methylanthraquinone; Compound 3, 2-hydroxy-1-methoxy-anthraquinone; Compound 4, 1,2-dihydroxy-3-methylanthraquinone; Compounds 5, 13,8-trihydroxy-2-methoxy-anthraquinone. ** Anthraquinone 1, 13,8-trihydroxy-2-methoxy; Anthraquinone 2, 2-hydroxy-1-methoxy; Anthraquinone 3, rubiadin.
A range of monomeric constituents derived from M. officinalis were reported to exert significant regulatory effects on both osteoblasts and osteoclasts. Anthraquinone-rich fractions promoted osteoblast proliferation and alkaline phosphatase activity while simultaneously reducing osteoclastic resorption, indicating dual, structure-dependent actions on bone cells. 17 Iridoid glycosides, such as monotropein, were demonstrated to prevent bone loss in OVX models, enhance bone mineral parameters, stimulate osteoblast activity, and inhibit inflammatory mediators and RANKL-associated resorption pathways.50,59 Other constituents, including bajijiasu and nystose, suppressed osteoclastogenesis by inhibiting NF-κB, nuclear factor of activated T-cells, and RANKL signalling while favouring the osteogenic commitment of mesenchymal stem cells via the BMP and Wnt pathways.51,67
Polysaccharide-enriched fractions further promoted osteogenic differentiation by activating BMP/Smad signalling and increasing matrix mineralisation. 60 Multi-component extracts enhanced skeletal mineral deposition in zebrafish models by coordinating the suppression of osteoclast-related genes. 55 In addition, extracellular vesicle-like particles derived from M. officinalis stimulated osteoblast proliferation and matrix formation by activating MAPK/cAMP response element-binding protein/ribosomal S6 kinase 1 signalling, contributing to improved trabecular parameters in vivo. 65
Together, these findings suggest that the monomeric constituents of M. officinalis exert complementary anabolic and anti-resorptive effects, supporting bone formation and inhibiting osteoclast activity across various experimental systems. A consolidated overview of these compounds and their reported effects is presented in Table 6, which summarises the osteogenic and anti-resorptive actions observed across relevant in vitro and in vivo models.
Summary of the Osteogenic and Antiresorptive Effects of Monomeric Compounds Derived from M. officinalis.

Summary of the Osteogenic and Antiresorptive Effects of Monomeric Compounds Derived from M. officinalis.
Abbreviations: ↑, upregulation/increase; ↓, downregulation/decrease; ALP, alkaline phosphatase; Bajijiasu, a monomeric compound isolated from Morinda officinalis; BMC, bone mineral content; BMD, bone mineral density; BMMs, bone marrow-derived macrophages; BMSCs, bone marrow mesenchymal stem cells; BMP, bone morphogenetic protein; BV/TV, bone-volume-to-total-volume ratio; CAII, carbonic anhydrase II; c-Fos, proto-oncogene protein Fos; Col2a1, collagen type II alpha 1 chain; CREB, cAMP response element-binding protein; DEX, dexamethasone; GSH-Px, glutathione peroxidase; HUC-MSCs, human umbilical cord mesenchymal stem cells; IL-1, interleukin-1; IL-6, interleukin-6; MAPK, mitogen-activated protein kinase; MC3T3-E1, murine pre-osteoblastic cell line; MOEVLPs, Morinda officinalis-derived extracellular vesicle-like particles; MOH, Morinda officinalis How extract; MOS, Morinda officinalis saccharide; NFAT, nuclear factor of activated T cells; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; OB, osteoblast; OCN, osteocalcin; OC, osteoclast; OPN, osteopontin; OVX, ovariectomised; p-CREB, phosphorylated CREB; p-RSK1, phosphorylated ribosomal S6 kinase 1; RANK, receptor activator of nuclear factor-κB; RANKL, receptor activator of nuclear factor-κB ligand; RAW264.7, murine monocyte/macrophage cell line; RSK1, ribosomal S6 kinase 1; RUNX2, runt-related transcription factor 2; sRANKL, soluble receptor activator of nuclear factor-κB ligand; Smad, mothers against decapentaplegic proteins; SOD, superoxide dismutase; TB.Th, trabecular thickness; TRAP, tartrate-resistant acid phosphatase; Wnt, wingless-related integration site signalling pathway.
The clinical translation of preclinical findings has been explored in a limited number of studies (Table 7). In patients with primary osteoporosis, an M. officinalis decoction combined with calcium supplementation was reported to yield a markedly higher overall effective rate, along with greater improvements in lumbar symptoms, BMD, and biochemical markers, such as serum OCN and urinary pyridinoline, compared with calcium alone. 82 In postmenopausal women with kidney Yang-deficiency osteoporosis, six months of oral M. officinalis decoction resulted in significantly greater increases in lumbar and hip BMD, accompanied by higher serum oestradiol and reduced ALP levels, relative to treatment with alendronate. 32
Summary of Clinical Studies on M. officinalis for Osteoporosis.

Summary of Clinical Studies on M. officinalis for Osteoporosis.
The critical limitations of the two clinical trials included a lack of methodological rigour. Methods of randomisation, allocation concealment, and double blinding were not reported. The dose of decoction used was not disclosed, and the duration of treatment was not reported in one trial. Hence, the results obtained are merely suggestive, requiring validation via better-designed trials.
M. officinalis, a fundamental herb in TCM renowned for reinforcing the kidney and strengthening bone, has been the subject of extensive pre-clinical and preliminary clinical investigation for its potential in osteoporosis management. This scoping review summarises evidence from cellular, animal, and clinical studies, demonstrating that its osteoprotective effects are primarily mediated through a multi-targeted, dual-action mechanism: promoting bone formation and inhibiting bone resorption. This multi-component, multi-target strategy is conceptually supported by network pharmacology analyses, which have identified 26 bioactive compounds within M. officinalis, including anthraquinones, iridoid glycosides, and saccharides, that are predicted to collectively target 257 genes implicated in key processes such as osteoclast differentiation and MAPK signalling. 55
The pro-osteogenic properties of M. officinalis were established through in vitro studies. An aqueous extract was found to stimulate osteoblast proliferation in a dose-dependent manner, enhance ALP activity, increase intracellular OCN levels, and upregulate TGF-β1 mRNA expression, indicating a comprehensive promotion of osteoblastic differentiation and function. 77 These initial findings were subsequently confirmed and refined, with the MOP fraction identified as a key active component, demonstrating superior efficacy over the crude aqueous extract in enhancing osteoblast proliferation, ALP activity, OCN secretion, and TGF-β1 expression. 71 The mechanistic basis for this was further elucidated, revealing that MOP promoted the osteogenic differentiation of BMSCs via the activation of the p38 MAPK signalling pathway, as evidenced by enhanced ALP activity, mineralised nodule formation, and upregulated RUNX2 and OPN expression, effects that were abolished by a p38 inhibitor. 58 An additional mechanism was suggested by the observation that MOP-containing serum suppressed the protein expression of DKK-1, a key inhibitor of the Wnt signalling pathway, while simultaneously increasing osteoblast proliferation and ALP activity. 79 Beyond stimulating bone formation, M. officinalis and its components were demonstrated to exert potent anti-resorptive effects. The inhibition of osteoclast formation and function was a consistent finding, with bioactive compounds such as rubiadin shown to suppress osteoclast formation, TRAP activity, bone resorption pit formation, and cathepsin K activity in a concentration-dependent manner. 74 This anti-osteoclastogenic activity was further linked to the modulation of the critical OPG/RANKL/RANK axis. Serum containing M. officinalis was found to upregulate OPG mRNA and downregulate RANKL mRNA in an osteoblast-osteoclast co-culture system, 68 and the aqueous extract was shown to increase the OPG/RANKL ratio in mesenchymal stem cells, 73 thereby shifting the bone remodelling balance towards bone formation. This was corroborated by in vivo findings where MOP administration upregulated OPG and downregulated RANKL expression in the bones of OVX rats.22,24
The efficacy of these mechanisms was robustly validated in preclinical animal models, particularly in OVX rats. The administration of MOP was consistently reported to prevent bone loss, significantly increasing BMD and BMC, while improving the trabecular microarchitecture and biomechanical strength.23,37 These effects were mechanistically linked to the regulation of the OPG/RANKL pathway22,24 and a reduction in pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α.26,35,36 The therapeutic portfolio of M. officinalis was further expanded to include other bioactive compounds. The iridoid glycoside monotropein was shown to ameliorate osteoporosis in OVX mice by enhancing BMD, improving bone microstructure, and suppressing serum levels of IL-1, IL-6, and sRANKL while also promoting the proliferation and differentiation of osteoblastic cells in vitro.27,50 Anthraquinones demonstrated dual osteogenic and anti-resorptive effects in vitro, with their activity being structure-dependent.17,74 Furthermore, other components such as nystose, 51 bajijiasu, 67 and iridoid glycosides 69 were also reported to inhibit osteoclastogenesis and promote osteogenesis through various signalling pathways, including NF-κB, BMP/Wnt, and RANKL.
Figure 2 summarises the signalling pathways believed to be involved in the actions of extracts and bioactive constituents of M. officinalis.

Proposed mechanisms by which M. officinalis and its bioactive constituents regulate bone remodelling. In osteoblasts, polysaccharides, oligosaccharides, extracellular vesicle-like particles, and crude extracts activate BMP/Smad, Wnt/β-catenin, MAPK, and PI3 K/AKT signalling, enhancing osteogenic gene transcription and bone formation. In osteoclasts, these constituents increase osteoprotegerin and suppress RANKL-mediated NF-κB/NFATc1 signalling, inflammatory responses, and autophagy, thereby reducing osteoclast survival and activity. Abbreviations: AKT, protein kinase B; AQ, anthraquinone; BJJ, bajijiasu; BMP, bone morphogenetic protein; BMP-R, bone morphogenetic protein receptor; CREB, cAMP response element-binding protein; ERK, extracellular signal-regulated kinase; EVLPs, extracellular vesicle-like particles derived from Morinda officinalis; GSK-3β, glycogen synthase kinase-3 beta; JNK, c-Jun N-terminal kinase; LC3, microtubule-associated protein 1 light chain 3; MAPK, mitogen-activated protein kinase; miR, microRNA; MOO, Morinda officinalis oligosaccharide; MOP, Morinda officinalis polysaccharide; MTN, monotropein; NEDD4L, neural precursor cell expressed developmentally downregulated protein 4-like; NF-κB, nuclear factor kappa-B; NFATc1, nuclear factor of activated T-cells, cytoplasmic 1; Nys, nystose; OPG, osteoprotegerin; PI3 K, phosphoinositide 3-kinase; PTEN, phosphatase and tensin homolog; PTGS-2 (COX-2), prostaglandin-endoperoxide synthase 2 (cyclooxygenase-2); RANK, receptor activator of nuclear factor κB; RANKL, receptor activator of nuclear factor κB ligand; RSK, ribosomal S6 kinase; Smad, mothers against decapentaplegic homolog; TRAF, tumour necrosis factor receptor-associated factor.
While pre-clinical and preliminary clinical findings are encouraging, several important limitations within the current evidence base must be acknowledged and utilised to guide future investigation. Firstly, the clinical evidence remains limited and of moderate quality. Existing trials are typically small-scale and short in duration and often lack rigorous double-blinding and appropriate placebo controls.32,82 Large, well-designed randomised controlled trials with long-term follow-up are required to establish clinical efficacy and safety with greater certainty. Secondly, although numerous mechanisms of action have been proposed, many studies remain fragmented. Mechanistic work often focuses on single pathways or target genes without integrating results into a coherent regulatory network or validating observations across complementary in vitro and in vivo models. Future studies would benefit from using systems biology approaches, including multi-omics, to achieve a more comprehensive understanding of how this herb's diverse constituents interact within the bone remodelling system. Thirdly, the lack of standardisation remains a major challenge. Different studies employ highly variable preparations of M. officinalis, including crude decoctions, aqueous or ethanol extracts, isolated fractions, compound formulations, and medicated serum, with differing extraction methods, dosages, and treatment durations. This heterogeneity limits comparability and makes it difficult to determine the most effective and reproducible forms. The standardisation of extraction protocols and chemical profiling is therefore essential. Fourthly, results for complex or secondary osteoporosis models remain scarce. Most studies rely on the standard ovariectomised model, whereas investigations in glucocorticoid-induced, age-related, and diabetic osteoporosis models are still limited.34,53 Expanding research into these models would help clarify the herb's broader therapeutic potential. Finally, research has focused predominantly on bone-specific outcomes, with relatively few comprehensive toxicological or pharmacokinetic studies. A deeper understanding of the absorption, distribution, metabolism, and excretion of key bioactive compounds, along with long-term toxicity assessments, is crucial to the successful clinical translation of these compounds.
In summary, the results of two decades of research provide substantial support for the osteoprotective potential of M. officinalis. Its multi-component, multi-target properties, mediated largely through polysaccharides,22–24,26,37,71,77 anthraquinones,17,40,74 and iridoid glycosides,27,50,69 act synergistically to regulate bone remodelling by promoting osteoblast activity58,63,64,71–73,75,77,79 and inhibiting osteoclast function.31,38,39,68–70,74,76 Despite strong pre-clinical evidence, progress remains limited due to the scarcity of high-quality clinical trials, the absence of standardised preparations, and the need for more integrated mechanistic and safety investigations. Future research should therefore prioritise the development of standardised extracts, robust clinical studies, and deeper mechanistic and toxicological evaluations to fully establish its efficacy, safety, and therapeutic value in osteoporosis management.
This review is not without limitations. It includes only English and Chinese literature from six databases. Grey literature was not included. This may lead to selection bias, with studies published in other languages and those with negative results not being included. A critical appraisal of all the studies was not performed due to the nature of the scoping review. Potential low-quality studies may have been included, which could affect the overall conclusions of the review.
This scoping review summarises the available preclinical and preliminary clinical evidence on M. officinalis for osteoporosis management and provides an integrative interpretation beyond summarising individual studies. The collective data suggest that its osteoprotective actions arise from a multi-component, multi-target network that influences key regulators of bone remodelling. MOP and anthraquinones are supported by the most consistent mechanistic evidence, demonstrating osteogenic activity through the Wnt/β-catenin, BMP/Smad, and MAPK pathways and anti-resorptive effects via the modulation of RANKL/NF-κB signalling. While these mechanistic patterns are reproducible across diverse models, variations in cell systems, extract standardisation, and animal study designs introduce uncertainty and limit external validity.
Across multiple preclinical models, including ovariectomised, glucocorticoid-induced, and ageing-related osteoporosis, M. officinalis consistently improves bone density, microarchitecture, and biomechanical strength, lending biological plausibility to its therapeutic potential. However, the evidence base remains dominated by laboratory studies, with limited and methodologically variable clinical data. Future work must therefore prioritise rigorous human trials, the clarification of interactions among the herb's constituents, and systems-level approaches to better characterising its network pharmacology. Overall, M. officinalis remains a promising multi-target candidate for osteoporosis, but its clinical integration requires stronger, standardised, and translationally relevant evidence.
Footnotes
Acknowledgements
The authors used ChatGPT version 3.5 (OpenAI, San Francisco, California) to polish the language of the manuscript, but they are responsible for the content.
Authors’ Contributions
Conceptualisation: Yuanzhong Wang and Kok-Yong Chin. Drafting: Yuanzhong Wang, Guiju Chen, Qin Wang, Xiaodong Ma, Xia Ji. Writing - Review & editing: Kok-Yong Chin.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universiti Kebangsaan Malaysia, Chongqing Chemical Industry Vocational College, Chongqing Chemical Industry Vocational College, Chongqing Municipal Education Commission, (grant number FF-2024-172, HZY202314315044, HZY202314315045, HZY202314315047, KJQN202404512).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.