
Abstract
Background and Aim
Shipixiaoji granules (SPXJ) is traditional Chinese medicine that treats hepatocellular carcinoma (HCC). However, its efficacy in HCC is still unknown. This prospective study assessed the outcomes of using SPXJ combined with tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs) in the management of patients with unresectable HCC.
Methods
This study was conducted as a single-arm phase II clinical trial. We recruited patients diagnosed with CNLC stage Ⅱ to Ⅲ HCC. The treatment regimen included oral lenvatinib (12 mg for patients weighing ≥60 kg; 8 mg for those weighing <60 kg) once daily, intravenous tislelizumab (200 mg) every 3 weeks, and SPXJ twice daily. The primary endpoint was defined as progression-free survival (PFS) in accordance with RECIST 1.1 criteria.
Results
Fifty-four patients were enrolled in this study. The primary endpoint was achieved, with a median PFS of 12.7 months. The objective response rate (ORR) was recorded at 55.6%. The disease control rate (DCR) was observed at 98.1%. Additionally, we compared PFS based on the participants’ sleep behavior. The results indicated that patients with a morning chronotype had a median PFS of 14.1 months, while those with a night chronotype had a median PFS of 9.85 months (95% CI: 1.366-6.853, P < .05). Treatment-related adverse events were reported in 96.3% (n = 52) of patients.
Conclusions
The combination of SPXJ, lenvatinib, and tislelizumab demonstrated substantial safety and anti-tumor efficacy as first-line treatment for unresectable HCC. Moreover, patients’ sleep behavior significantly influences treatment efficacy.
Introduction
Global cancer statistics indicate that hepatocellular carcinoma (HCC) ranks sixth in incidence and fourth in mortality among malignant tumors, posing a significant public health concern in China.1,2 Alarmingly, approximately half of these patients are diagnosed with unresectable HCC. The National Comprehensive Cancer Network (NCCN) has recommended atezolizumab plus bevacizumab as the preferred initial therapy for unresectable HCC.3-6 Other clinical trials, including the BGB-A317-211 study, have demonstrated encouraging antitumor effects with systemic treatments combining tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs) 7 Despite these survival benefits, the 5-year survival rate for patients with unresectable HCC remains below 20%.8,9
Years of research on the integration of Chinese medicine (CM) and Western medicine have led to the development of numerous Chinese patent drugs, plant extracts, and empirical formulations for clinical applications.10,11 So far, CM has played a crucial role in the treatment of HCC, particularly for unresectable cases. The effectiveness of these treatments has also gained increasing recognition.1,12,13 Liu et al showed that Fuzheng Jiedu Xiaoji, a Chinese formulation combined with transcatheter arterial chemoembolization significantly extended overall survival (OS) and progression-free survival (PFS) and reduced the mortality rate among patients with HCC. 14 Additionally, numerous studies indicate that Chinese medicine has the potential to modulate the immune microenvironment 15 and suppress angiogenesis in HCC.5,16,17
Shipixiaoji granules (SPXJ), a Chinese patent drug, have been shown to have definitive curative effects after more than a decade of clinical validation and are widely used in the prevention and treatment of HCC. Previous studies have shown that SPXJ enhances energy metabolism by modulating mitochondrial fission and fusion to treat HBV-related HCC. However, there is currently a lack of epidemiological evidence to substantiate this claim. Therefore, we conducted a prospective, single-arm, phase II trial to investigate the efficacy and safety of SPXJ combined with lenvatinib and tislelizumab.
Material and Methods
Study Design
This prospective, single-arm, phase Ⅱ trial was conducted at the Affiliated Hospital of Hunan Academy of Chinese Medicine. The trial protocol is detailed in Figure 1. The Research Ethics Board of the Affiliated Hospital of Hunan Academy of Chinese Medicine approved the trial (Clinical Trial Number: 2022HNCM023), and the study was conducted in accordance with the principles of the Declaration of Helsinki. Participants were enrolled from July 1, 2022, to July 1, 2023. All participants provided written informed consent prior to enrollment.

Trial protocol.
Inclusion Criteria
Participants who met the following inclusion criteria were eligible for this study: (1) a diagnosis of HCC confirmed by pathology or typical HCC characteristics identified using ultrasound combined with computed tomography (CT) or magnetic resonance imaging (MRI), 18 in accordance with the guidelines proposed by the Chinese Liver Cancer Association; 19 (2) aged between 18 and 70 years, with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 1, Child-Pugh class A or B, and CNLC stage Ⅱ to Ⅲ; (3) deemed inoperable after multidisciplinary team (MDT) discussion or refusal to undergo surgical or interventional treatment; (4) no prior systemic treatment; (5) an expected survival time of more than 3 months; (6) no severe primary diseases of the nervous system, heart, lungs, hematopoietic system, endocrine system, or mental illness.
Exclusion Criteria
The exclusion criteria were as follows: (1) history or presence of other malignant tumors; (2) severe infectious diseases; (3) human immunodeficiency virus (HIV) infection; (4) gastrointestinal hemorrhage within the past 30 days; (5) pregnancy; (6) language communication barriers.
Procedures
The participants received intravenous tislelizumab (200 mg) on day 1 of a 21-day treatment cycle, in combination with oral lenvatinib (12 mg for patients weighing ≥60 kg or 8 mg for those who weigh <60 kg) once daily. SPXJ is a traditional Chinese medicine (developed by Hunan Guohua Pharmaceutical Co. Ltd) consisting of 11 herbs, namely: Astragalus, Ginseng, Peach Kernel, ground beetle Insect, Gecko, Banzhi, Pinellia, Poria, Epimedium, Shi Jianchuan, Solanum nigrum. Additionally, the patients were administered oral SPXJ twice daily until disease progression. Afterwards, the patients were administered 6 g of SPXJ orally twice daily. The patients then continued treatment until disease progression, death, the emergence of intolerable toxicity, or the withdrawal of consent.
Outcomes and Clinical Assessments
Each 21-day period constituted a treatment cycle. All patients underwent re-evaluation every 6-8 weeks. Evaluations included imaging with CT or MRI and laboratory tests, including routine blood tests, liver function tests, and alpha-fetoprotein (AFP) levels. Tumor response was assessed using the RECIST version 1.1 criteria. The primary endpoint was PFS, defined as the time from enrollment to disease progression, including the PFS rate at 6, 12, and 18 months. The secondary endpoints included OS, defined as the time from enrollment to death, objective response rate (ORR), defined as the proportion of patients whose tumor volume reduction reaches the predefined value and can be maintained for the minimum required duration, and disease control rate (DCR), defined as the proportion of patients whose tumor volume reduction reaches the predefined value and is maintained for the minimum required duration, representing the sum of the complete response and partial response rates.
Safety Evaluation
Safety was evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.03 (NCI CTCAE v4.03). Tumor assessments were performed by two independent radiologists, and the best responses were documented. All responses were confirmed by a subsequent assessment after 4 weeks. All observations pertinent to the safety of the study medication were recorded in the case report form and included in the final report.
Assessment of Sleep Behaviors
All enrolled patients self-reported their data, and a questionnaire was used to collect information regarding sleep behaviors. The participants’ chronotype preference was assessed using the Morningness-Eveningness Questionnaire Self-Assessment version (MEQ-SA), developed by Horne & Ostberg. 20 According to the categorizing score, sleep behaviors were classified as morning type (scores 59-86), intermediate type (scores 42-58), and evening type (scores 16-41). 21
Statistical Analysis
Simon's two-stage design was employed with a one-sided α error of 5% and a power of 80%. Kaplan-Meier curves were used to calculate PFS rates with associated 95% confidence intervals (CIs). All statistical analyses were conducted using SPSS software version 25.0 (IMB Corp., Armonk, NY, USA). The PFS rates at 6, 12, and 18 months were calculated, and the ORR and DCR were determined using the Clopper-Pearson method.
Results
Patients’ Characteristics
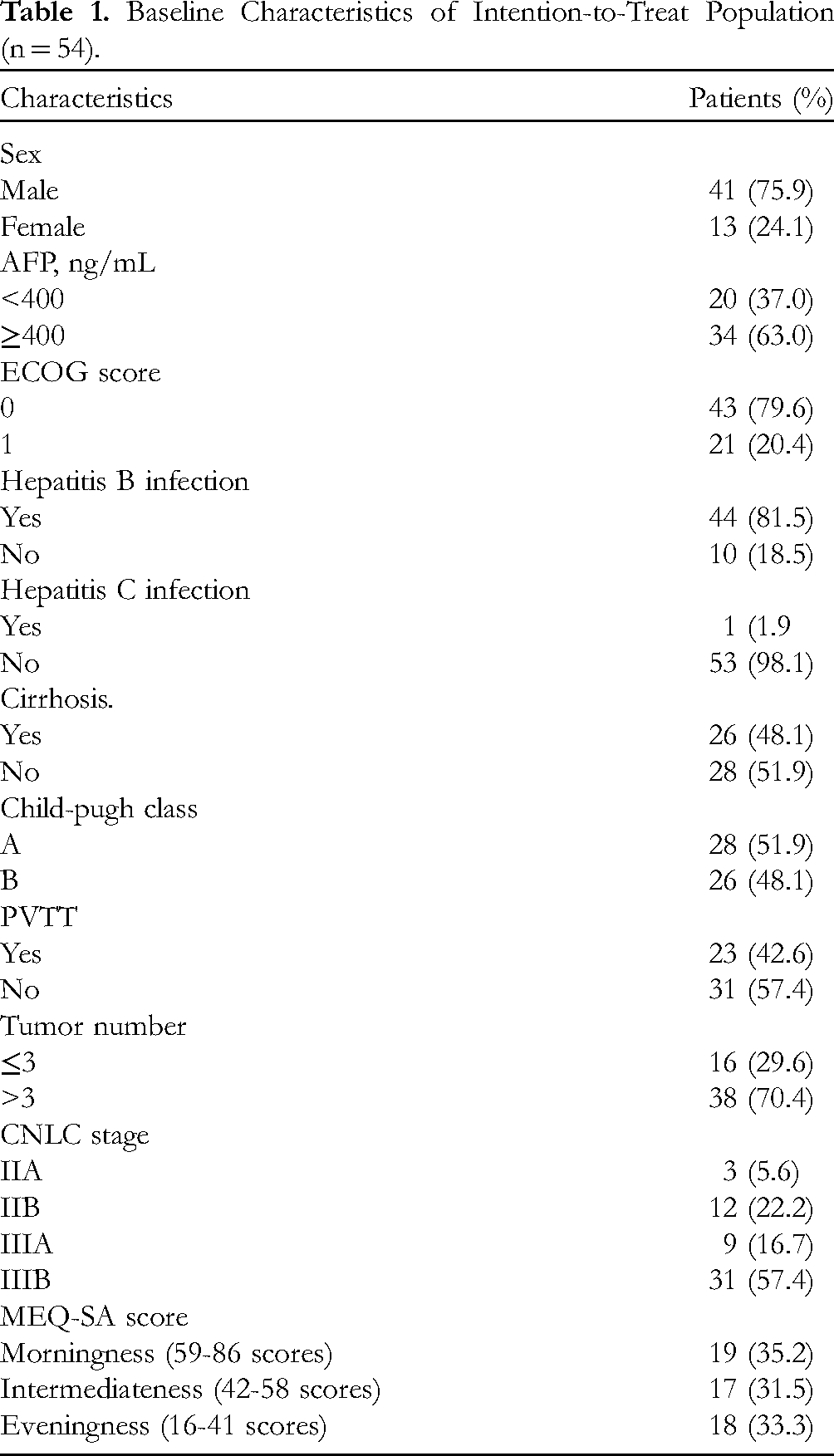
A total of 68 patients with HCC were included in this study. Of these, five cases were excluded for not meeting the inclusion criteria, four cases were excluded for meeting the exclusion criteria, and five participants dropped out due to loss of follow-up. Ultimately, 54 cases were included in the final analysis. The patients’ sleep behaviors were assessed using the MEQ-SA, categorizing them into morningness, intermediateness, and eveningness. Of the 54 patients included in the study, 19 were classified as morning type (35.2%), 17 as intermediate type (31.5%), and 18 as evening type (33.3%). The patients’ baseline characteristics are presented in Table 1.
Baseline Characteristics of Intention-to-Treat Population (n = 54).
Efficacy
In this study, the median follow-up time was 18.4 months. All patients reached the primary endpoint of the study. According to RECIST 1.1 evaluation criteria, 30 patients achieved partial response (PR), 23 patients had stable disease (SD), and one patient had progressive disease (PD), resulting in an ORR of 55.6% and a DCR of 98.1%. The media PFS was 12.7 months. The PFS rates at 6, 12, and 18 months for the patients were 94.4%, 55.6%, and 5.6%, respectively (Figure 2).

Kaplan-Meier curves of progression-free survival (n = 54).
Additionally, we conducted a stratified analysis based on sleep chronotype, specifically morningness and eveningness. The median PFS for patients with morning and evening chronotypes were 14.1 months and 9.85 months, respectively, (95% CI: 1.366-6.853, P < .05, refer to Figure 3).

Kaplan-Meier curves of progression-free survival between morningness and eveningness.
Safety
Overall, 96.3% (n = 52) of patients in this study experienced treatment-related adverse reactions. The most common adverse reactions included hand-foot syndrome (n = 37, 68.5%), nausea (n = 26, 48.1%), diarrhea (n = 16, 29.6%), fatigue (n = 15, 27.8%), granulocyte reduction (n = 29, 53.7%), hypertension (n = 6, 11.1%), thrombocytopenia (n = 11, 20.4%), abdominal pain (n = 13, 24.1%), epistaxis (n = 2, 3.7%), decreased hemoglobin levels (n = 10, 18.5%), and pruritus (n = 15, 27.8%).
Discussion
Unresectable HCC is primarily characterized by its invasiveness, high rates of recurrence and metastasis, and limited efficacy of anti-tumor medications. 22 The disease often has a poor clinical prognosis, marked by recurrence and resistance to treatment. TKIs combined with ICIs currently represent the standard first-line medical intervention for HCC. SPXJ is an in-hospital preparation used for the treatment of HCC in our hospital. Our previous research showed that SPXJ combined with sorafenib can improve patients’ OS and quality of life. 23 In this study, we conducted a single-arm, prospective phase II clinical trial to further explore the clinical efficacy of SPXJ combined with TKIs and ICIs.
In recent years, several clinical studies have investigated the use of TKIs in combination with ICIs for the management of HCC. The IMbrave150 study demonstrated that the combination of atezolizumab and bevacizumab significantly improved OS and PFS outcomes compared to sorafenib. The ORR increased by 30%, while the DCR improved by 74%. Additionally, the median duration of response (DoR) was reported to be 18.1 months. 24 The study successfully met the primary endpoint established by the research team. Based on imaging evaluations, the ORR was 55.6% and the DCR was 98.1%. In the BGB-A317-211 study, the ORR and DCR for lenvatinib plus tislelizumab in patients with unresectable HCC were 38.7% and 46.8%, respectively 7 In our study, the median PFS was significantly longer compared to that of the BGB-A317-211 study. The OS endpoint was not reached due to an insufficient median follow-up time. Only 10 patients had reached the secondary endpoint of mortality, with a data maturity of 18.5%. Therefore, additional follow-up is necessary to draw more conclusive results. These findings suggest that SPXJ, in combination with lenvatinib and tislelizumab, may enhance PFS in patients.
Preclinical studies provide complementary evidence on the effect of sleep behavior on cancer progression and treatment efficacy.25,26 The impact of sleep behavior on the progression of HCC is primarily related to the regulatory effects of the circadian clock on immune escape.27,28 Wu J et al reported that the circadian clock gene BMAL1 was associated with bevacizumab resistance and that inhibiting the expression of BMAL1 may prevent resistance to anti-angiogenic therapy in patients with colorectal cancer 29 Additionally, another study showed that the circadian clock component RORA suppressed programed cell death 1 ligand 1 (PD-L1) expression and was significantly positively correlated with T-cell infiltration and recruitment in patients with melanoma. 30 Furthermore, the circadian rhythm affects the infiltration of immune cells into tumor tissue through blood vessels by influencing the level of adhesion molecule ICAM-1 expressed on the surface of endothelial cells. 31 Preclinical studies indicate that a RORA agonist combined with an anti-CTLA4 antibody synergistically increased T-cell antitumor immunity. 30 This suggests that the sleep chronotype may influence the immune status of patients, thereby affecting patients’ outcomes in this study.
Regarding safety, our study's findings are similar to those of other studies that combined TKIs and ICIs, and no specific treatment-related toxicities were observed. Additionally, the incidence of toxicities were lower than those reported by IMbrave150 and other studies.24,32 No patient in our study experienced fatal toxic side effects during the study period.
As an early-stage clinical trial with a single-center, single-arm design, the relatively small sample size is a limitation of our study. Additionally, only 7.4% of patients in our study were females infected with hepatitis B virus, whereas the proportion of female patients with HCC in the Chinese population is 24.5%. Therefore, subsequent studies with larger sample sizes are needed to validate these findings. Furthermore, the long-term survival data obtained in our study require additional follow-up.
Conclusion
In summary, the combination of SPXJ, lenvatinib, and tislelizumab demonstrated good safety and anti-tumor activity as a first-line treatment for unresectable HCC. Additionally, our findings indicate that patients’ sleep behaviors affect treatment efficacy.
Footnotes
Credit Authorship Contribution Statement
Zhen Zhang: Writing – Original Draft, Investigation, Methodology, Formal Analysis, Data Curation. Zicheng Liang: Formal Analysis, Methodology, Formal Analysis, Data Curation. Xiaoning Tan: Resources, Methodology, Software. Huiying Jian: Conceptualization, Supervision, Resources. Wenhui Gao: Resources, Writing – Review & Editing, Methodology. Puhua Zeng: Visualization, Funding Acquisition, Writing – Review & Editing, Validation, Project Administration.
Data Availability
The datasets generated and analyzed during the current study are not publicly available to protect subject privacy, but they are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethic Statements
This study was approved by the Institutional Review Board of the Hunan Academy of Chinese Medicine (Clinical Trial Number 2022HNCM023).
Funding
The authors express their gratitude to the patients who participated in the trial and to the medical staff of the participating centers. This study was funded by the National Natural Science Foundation of China (Grant Nos. 81603603, 82074425), the Hunan Science and Technology Planning Project (Grant No. 2023SK2057), the Hunan Provincial Administration of Traditional Chinese Medicine Research Project (Grant No. B2023089), the Hunan Provincial Natural Science Foundation (Grant No. 2023JJ40403), and the Graduate Student Innovation Project of Hunan University of Chinese Medicine (Grant ID: 2023CX113).