
Abstract
Keywords
Introduction
Modern Lifestyle, Immune Challenges and Public Health Overload
Globally, there has been an increased demand in healthcare systems in response to factors including aging populations, physical inactivity, and unhealthy lifestyles that include the consumption of fast food and alcohol. 1 While the rise in non-communicable diseases and chronic conditions are putting significant strains on public health, the socio-economic burden of upper respiratory tract infections (RTIs) remains high and is not to be overlooked.
The World Health Organization (WHO) estimates that approximately one billion people are infected with influenza each year, resulting in up to 500,000 deaths. 2 In the United States alone, it was estimated that influenza in the 2017–2018 season was associated with more than 48.8 million illnesses, more than 22.7 million medical visits, 959,000 hospitalizations and 79,400 deaths. 3 This burden was higher than any season since the 2009 pandemic. With the surge in hospitalizations and death, public health services such as emergency health services may become overloaded. 4
Metropolitan cities with high population density, air pollution and a subtropical climate are associated with a higher risk of infectious disease outbreak; hence, the socio-economic impacts of upper RTIs in these areas are particularly critical. Hong Kong, a city with high population density, saw a public hospital bed occupancy that exceeded 100% during the peak flu season in 2019, implying that beds were allocated in corridors.5,6 The government has allocated HK$272 million (US$34.9 million) toward influenza vaccination for 2019–20 7 ; however, the estimated effectiveness of the annual vaccine is merely moderate across the different strains, and even lower among children and older adults. 8
In the United Kingdom, a 2016 survey conducted by Self Care Nation revealed more than one-third of the survey respondents had visited a general practitioner (GP) for a minor condition like the common cold, which could have been self-managed with a pharmacist's advice. 9 It was estimated that minor ailments contribute to 20–40% of GP workload, placing an economic burden of £2 billion on the National Health Service (NHS). 10
Clearly there is an urgent need to reduce such burden. One possible solution is the empowerment of self-care, which is defined by the WHO as “the ability of individuals, families and communities to promote health, prevent disease, maintain health, and cope with illness and disability with or without the support of a healthcare provider”. 11
Recognizing pharmacists’ expertise and their high accessibility, NHS England has recently introduced the Community Pharmacist Consultation Service (CPCS), which was being commissioned as an Advanced Service in late 2019. 12 The service aims at reducing demands on the emergency department and other urgent care services by the integration of community pharmacy into the urgent care system, thereby releasing capacity for patients with higher acuity conditions. Under the service, patients with minor illnesses like cold and flu will be referred to a community pharmacy when they make a telephone call to NHS 111. Pharmacists will also provide patients with self-care advice on the management of minor ailments to prevent future unnecessary use of urgent care services.
Meanwhile, the Hong Kong government recently initiated the establishment of district health centres, which promote primary and community healthcare to improve resource utilization, as well as patient involvement and self-care for the management of influenza and other chronic diseases. 13 In this setting, community pharmacists play a significant role in facilitating self-care awareness and public health education; the correct use of micronutrient supplementation is one potential self-care strategy. Among all available micronutrient supplementations, vitamins C, D and zinc have been shown to be associated with improved immune system function in both observational studies and clinical trials, and hence could potentially be used as a self-care intervention to reduce the burden of influenza.
Micronutrients: Suboptimal Intake and Deficiency in South Korea, Taiwan, Hong Kong and Nearby Regions
Micronutrient deficiencies are prevalent and pose public health issues in China, Hong Kong and nearby regions. According to several community-based surveys conducted in Hong Kong, Taiwan and South Korea (Table 1),14–18 vitamin D deficiency or insufficiency is prevalent, particularly in women, including those of child-bearing ages. Notably, in South Korea, the prevalence of vitamin D deficiency increased significantly from 51.8% in males and 68.2% in females in 2008, to 75.2% and 82.5%, respectively, in 2014. 18 Such an increase is multifactorial, which could be due to seasonal fluctuation in serum 25(OH)D levels, 19 use of sunscreen products, and limited sun exposure due to lack of outdoor activities. 20 Our recent study of 5276 participants from the Hong Kong Osteoporosis Study found that a significant portion (90.1%) of Hong Kong Chinese had vitamin D deficiency or insufficiency. 14 With this level of prevalence it is important that healthcare practitioners in these regions are aware of the public health risk and provide corresponding dietary and supplementation advice to the public.
Studies on the Prevalence of Vitamin D Deficiency in Three Regions of Asia.
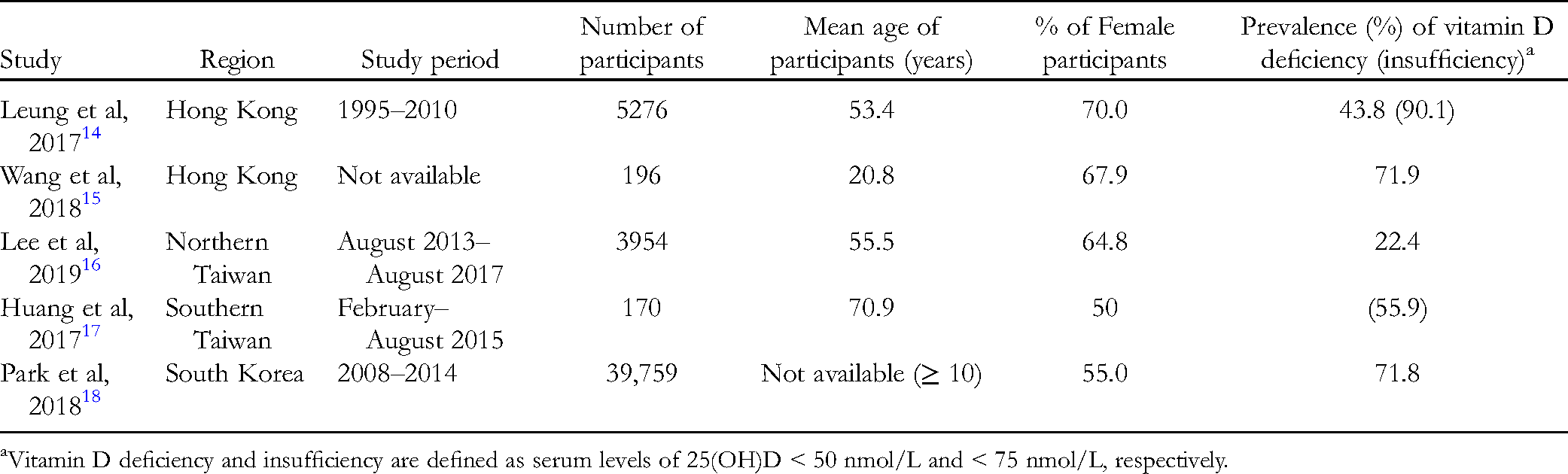
Vitamin D deficiency and insufficiency are defined as serum levels of 25(OH)D < 50 nmol/L and < 75 nmol/L, respectively.
Insufficient intake of zinc is another potential issue worldwide. A study that estimated the global prevalence of zinc deficiency from 2003–2007 showed that approximately 17.3% of the world population were at risk of zinc deficiency, while in East and Southeast Asia and the Pacific, 22.1% of people were estimated to have inadequate zinc intake, with the third lowest estimated zinc intake among all regions studied. 21 One of the causes of such a high prevalence of inadequate zinc could be the reduced zinc levels in soil and agricultural products resulting from modern farming practices. 22 Another possible factor could be eating habits, as research suggests a possible link between fast food consumption and zinc deficiency in children from small families. 22
Of note, micronutrient deficiencies can be very common in vulnerable populations, including patients with psoriasis and prediabetes/diabetes, hospitalized patients and older people.23–28 Children are also a high-risk group for both vitamin D and zinc deficiency. In two recent studies of 25(OH)D in Chinese school-age children, the prevalence of vitamin D deficiency (defined as serum 25[OH]D < 15 ng/mL) ranged from 35.5% to 54.7%29,30; it was also reported that 86.1% of these children had insufficient dietary vitamin D intake. 30 As nutritional guidelines have recently increased the recommended intake of vitamin D among children,20,31 it is expected that more children will be defined as having insufficient dietary intake of vitamin D. Similarly, a high prevalence of low circulating plasma zinc concentration (PZC) has been reported in children in Asian countries. Prevalence rates of low PZC ≥ 10% have been reported in children from 7 out of 9 Asian countries studied, while more than 10% of children from 8 out of 9 Asian countries studied had inadequate zinc intake. 32
Micronutrients for Alleviation of Respiratory Infections: Clinical Evidence
To prevent or treat the common cold and influenza, many people in Chinese communities like Hong Kong use proprietary complementary treatments such as traditional Chinese medicines and herbal-based health products. However, health risks and potential toxicity related to the dehydropyrrolizidine alkaloids and aristolochic acids in such products have been reported. 33 Additionally, the clinical evidence for the effectiveness of these products appears to be less robust than that for micronutrient supplementation, especially vitamins C, D and zinc, which have been studied extensively in clinical research.
As shown in a systematic review of 29 placebo-controlled trials, vitamin C supplementation ≥ 200 mg daily reduced the incidence of colds by 52% in physically stressed populations such as athletes and soldiers, and reduced the duration of colds by 8% and 14% in general adults and children, respectively. 34 In addition, a meta-analysis of nine randomized controlled trials found that the administration of extra vitamin C doses at the onset of a cold reduced the disease duration by 0.56 days, shortened the time of indoor confinement by 0.41 days, and reduced symptoms by 0.36–0.45 days. 35
A systematic review and meta-analysis of individual participant data (n = 10,933) demonstrated that vitamin D supplementation was associated with a lower risk of acute RTI (adjusted odds ratio [OR], 0.88; 95% confidence interval [CI], 0.81-0.96; P for heterogeneity < 0.001). 36 Another meta-analysis of five randomized controlled trials suggested a similar benefit of vitamin D in the prevention of RTIs (OR, 0.58; 95% CI, 0.42-0.81; P = 0.001). 37 In several randomized trials conducted in Asian countries, vitamin D supplementation reduced the risk or disease duration of acute lower RTIs, including pneumonia, severe asthma and bronchiolitis, among children with vitamin D deficiency. 38 Other studies have also documented the positive effects of vitamin D supplementation on reducing the incidence of seasonal influenza A among children and improving lung function among people with obesity.39,40
Zinc deficiency is associated with chronic inflammation in children. 41 A study conducted in Taiwan found that zinc supplementation could improve appetite and growth in undernourished children. 42 Evidence shows that zinc lozenges are possibly effective in treating the common cold. 43 In a systematic review and meta-analysis of 17 randomized controlled trials, zinc was shown to reduce the duration of cold symptoms by 1.65 days (95% CI, 0.81-2.50) compared with placebo, while subgroup analyses showed that adult patients (vs. children), higher doses of zinc, and the formulation of zinc acetate were associated with more significant improvements in cold symptoms. 44 A more restricted meta-analysis revealed that a zinc lozenge dose of > 75 mg/day reduced the common cold duration by 2.73 days (95% CI, 1.8-3.3). 45 Some studies conducted in Thailand, Turkey and Iran demonstrated the potential of zinc therapy for improving cold symptoms in children. 46
The use of a vitamin C (1000 mg) and zinc (10 mg) combination was assessed in a pooled analysis of two studies on patients with the common cold. 47 The results showed a significant reduction in the duration of rhinorrhoea over 5 days of treatment compared with placebo.
These findings from randomized controlled trials demonstrated the clinical efficacy of vitamins C, D and zinc in reducing incidence and disease severity of respiratory infections, such as the common cold and influenza.
Discussion
Over-the-counter medicines for cold and flu infections, such as non-steroidal anti-inflammatory drugs and acetaminophen, help relieve discomfort and nasal symptoms; however, these medications appear to have limited effects on other cold symptoms, including sore throat, malaise, sneezing and cough, and are not considered to improve immunity.48,49 Supplementation of vitamins C, D and zinc is a promising complementary remedy, as their efficacy and safety in the prevention and treatment of respiratory infections have been demonstrated across a number of clinical studies. They have consistently been shown to shorten the duration of infections, including colds, seasonal flu and lower respiratory infections, among children in particular.
Optimal Nutrient Intake
There is an increasing demand for micronutrients to support the immune response during recovery from illnesses such as the common cold and infections. During infection, the levels of micronutrients including zinc, iron, vitamins A, E and C fall rapidly, which is likely to result from impaired absorption of micronutrients, increased metabolic needs and reduced food intake.50,51
Vitamin C, with its antioxidative and immune-enhancing properties, has been widely investigated as a tool in the fight against the common cold. We now understand that the intensity of the immune response can be amplified when certain micronutrients are combined. Vitamins C, D and zinc work in synergy to boost immunity in terms of epithelial barriers, cellular response and antibody production. 52 As a simple illustration, vitamins C, D and zinc promote the activities of lymphocytes through distinct mechanisms, achieving an overall maximum stimulation of the immune response. 52 As mentioned earlier, the administration of 1000 mg vitamin C plus 10 mg zinc significantly relieved symptoms such as rhinorrhoea in patients with the common cold. 47
In most global and country-specific guidelines, dietary reference intake (DRI) values only represent the daily intake of nutrients that are required to avoid deficiency. The optimal levels of nutrients that are required to achieve a therapeutic effect on the common cold and infections may be much higher than the DRI values (Table 2). 51 A review of multiple studies concluded that regular administration of > 1 g/day vitamin C could help reduce the duration and severity of common colds. 53 As for vitamin D, a meta-analysis of 11 randomized controlled trials indicated that an average dose of 1600 IU/day supplementation significantly lowers the risk of RTI, although there may have been publication bias in some of the included studies. 54 A systematic review revealed that a daily intake of > 75 mg zinc effectively shortens the duration of the common cold, 55 and 10 mg zinc in combination with 1 g vitamin C was shown to help reduce rhinorrhoea and speed up recovery during the common cold. 47 There is a growing body of evidence that micronutrient supplementation can assist individuals in reaching the optimal nutrient levels to support an efficient immune response and facilitate recovery from infections.
Comparison of Dietary Reference Intakes (DRIs) and Therapeutic Effective Doses of Selected Micronutrients.

DRIs for males and females aged > 18 years by the Institute of Medicine. 51 .
the Practice of Self-Care
Self-care can be viewed as any action or activity taken to maintain one's own health. 56 With the global trend of focusing on people-centred care, self-care is increasingly supported as a feasible approach to the management of minor ailments.56,57 The effectiveness of self-care depends on an individual's confidence, health literacy and health awareness. 57 According to the WHO Regional Committee for South-East Asia, self-care should be an essential part of primary healthcare for achieving health outcomes. 58 It is expected to help reduce healthcare costs and improve health equity in the Region. 58 The Member States are dedicated to establishing dialogue between the community and healthcare providers, promoting community participation, and enabling an environment for self-care accessibility. 58 In Hong Kong, the Government has established the Steering Committee on Primary Healthcare Development, which is determined to step up efforts to promote individual and community involvement, enhance coordination between various medical and social sectors, and strengthen district-level primary healthcare services. These measures aim to encourage the public to take precautionary measures against diseases, enhance their capability in self-care and home care, and reduce the demand for hospital services.
The Role of Community Pharmacists in Facilitating Self-Care
Community pharmacists are involved in primary healthcare development as the experts in self-care and drug management. Given their accessibility to the general public, they are well positioned to assist with expanding awareness of the concept of self-care. 57 A web-based survey involving adults from the UK, the USA, Australia and Japan found that information obtained from pharmacies was considered reliable and widely used for self-care. 59
In the UK, the NHS has established pharmacy-based minor ailments schemes, which enable eligible patients to seek healthcare advice on minor ailments and access medicines at a community pharmacy in listed locations. The schemes aim at facilitating self-care, thereby reducing the burden on GP and emergency departments. A study on the minor ailments schemes in Scotland reported that minor ailments being treated at pharmacies were cost effective, saving a total of £106 million. The health outcomes of patients participating in the scheme were similar to those who received treatment from a GP or emergency department. 60
Community pharmacists can facilitate self-care of diseases such as RTIs by giving practical advice, particularly on the appropriate use of antibiotics. The Global Action Plan on antimicrobial resistance published by the WHO in 2015 identified the misuse and overuse of antimicrobials as a major contributing factor to the global antimicrobial resistance crisis. 61 The Hong Kong Strategy and Action Plan on Antimicrobial Resistance, which was launched in 2017, aimed to facilitate the engagement of healthcare professionals and patients in adopting infection control measures and proper use of antibiotics. 62 About 90% of upper RTIs such as the common cold and influenza are of viral origin, for which antibiotic treatment is useless. However, for some patients who have the misconception that antibiotics are the basic treatment for all RTIs, it would be a paradigm shift to accept a different practice. Public Health England's ‘Keep Antibiotics Working’ national campaign advocates embracing antimicrobial stewardship and reducing unnecessary prescriptions in collaboration with community pharmacy. 63 A questionnaire showed that non-medical prescribers including pharmacists and nurses could satisfy patient expectations of RTI consultations with non-antibiotic management strategies. 64 Multiple studies have demonstrated that pharmacists, as a first medical contact, provide safe, effective and timely management of influenza-like illnesses, with high patient satisfaction.65–67
A community pharmacist acting as the key partner to empower consumer self-care is focused on five areas: 1) acting as the first contact point for the public, making an initial diagnosis and referring patients to medical care only if deemed necessary; 2) recommending non-prescription medications or micronutrient supplementation for conditions manageable by patient self-care; 3) serving as a partner in disease prevention and long-term health management by giving health advice including hygiene practices, dietary nutrient intake, and smoking cessation,; 4) providing health screening services for cardiovascular health, micronutrient insufficiencies, osteoporosis, diabetes, etc; and 5) reviewing and optimizing medication use and safety. Taken together, this level of pharmacist support could enable the public to make informed healthcare decisions for themselves.56,57
In view of the greater awareness of vitamin supplementation among the general public, healthcare professionals can now feel at ease recommending rational micronutrient supplementation as a part of self-care, without worrying that patients would then stop observing healthy eating habits. 68 The Global Respiratory Infection Partnership is one example of a program that encourages pharmacists to promote and increase self-care awareness in the management of upper RTIs without the use of antibiotics. 69 In Hong Kong, for example, there are more than 600 community pharmacies, which offer the general public a readily accessible primary contact point for consultation on drug and supplement use.
Given the study evidence, the relationship between micronutrients (particularly vitamins C, D and zinc) and respiratory infections appears intertwined, involving multiple immunomodulatory and immunostimulatory mechanisms, as well as varying lifestyle and biological factors. Micronutrient supplementation can be considered a feasible self-care strategy for the prevention and management of the common cold and acute respiratory infections alike, especially among children and other vulnerable groups. This approach could relieve the strain on medical care resources, and reduce work and school absences.
Conclusions
In densely populated cities, respiratory infections are posing a formidable challenge to the immune systems of individuals and the public healthcare system at large. In recent years, more evidence on the roles of certain micronutrients in the management and prevention of respiratory infections has emerged. In particular, the synergistic roles of vitamins C, D and zinc in enhancing the immune system have become more apparent, emerging as the “golden nutrients” in terms of immune support, and serving as a useful addition to the primary care portfolio of pharmacists and self-medication. While more research in this field is encouraged, these micronutrients have been shown to reduce the risk, duration and severity of RTIs. The optimal dosage of nutrients is important when a therapeutic immune-enhancing effect is desired. As shown in clinical studies, the dosages are often higher than recommended daily intake levels (Table 2). The evidence-based utilization of micronutrients has the potential to be further expanded to form an efficient primary care strategy. The government and healthcare institutions are encouraged to examine this potential in their future planning.
Footnotes
Acknowledgments
The authors would like to thank Best Solution Company Limited (Mr CT Tsoi) for drafting the first version of the manuscript, which is funded by Bayer HealthCare Limited.
Authors’ Contributions
PKLC and CLC contributed to the conception of the review and acquisition, analysis and interpretation of the literature. EFWY contributed to the acquisition of the literature. All authors revised the manuscript critically and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bayer HealthCare; The editorial assistance is funded by Bayer HealthCare Limited.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.