
Abstract
Background:
Diabetes prevalence is rising and projected to affect 783 million globally by 2045. Effective diabetes self-management relies on diabetes knowledge, lifestyle modifications, and health care support; yet global health care workforce shortages hinder the provision of adequate care. Socially assistive technologies, such as robots or artificial intelligence, are proposed as potential solutions to meet rising demands.
Aim and Methods:
To map the current literature on Socially Assistive Robots for diabetes care, identifying robotic types, barriers and enablers to use, and impact on health-related outcomes. A scoping review using Arskey and O’Malley’s Framework was conducted, screening studies published between 2013 and 2025 across key databases and extracting data using COVIDENCE.
Results:
Twenty-two studies met the inclusion criteria, mostly focused on children with type 1 diabetes. Studies were largely conducted in Europe, cross-sectional, and with small sample sizes. Socially assistive robots demonstrated high acceptability, especially among younger children, positively affecting knowledge acquisition, self-management, and self-efficacy. Personalized interactions, gamified features, and emotional responsiveness were key enablers of engagement. However, engagement waned over time, particularly when participants’ practical and emotional expectations were unmet. Barriers included usability challenges, privacy concerns, and lack of customization. Economic and sustainability evaluations were absent.
Conclusions:
Despite growing evidence for robotics in diabetes care, research remains methodologically limited and focused primarily on younger populations. Future studies should include adults, employ multi-faceted robotics designs, and be adequately powered to assess acceptability and efficacy across diverse groups, facilitating broader application in diabetes care.
Introduction
In 2021, 10.5% (540 million) of the global adult population were living with diabetes, a figure projected to reach 783 million by 2045. 1 Poorly managed diabetes can cause serious complications, including cardiovascular disease, neuropathy, end-stage renal disease, visual impairment, and cognitive decline, placing a heavy burden on global health care systems. 2 Effective management consists of education, regular health care follow-up, and self-care activities such as blood glucose monitoring, lifestyle adjustments, and medication optimization. 3 These demands often present significant challenges, leading to a high disease burden and distress. 4
Growing global health care workforce shortages have intensified calls for innovation, driving the adoption of technology and artificial intelligence (AI) in care delivery.5-7 Robotic technologies, particularly socially assistive robots (SARs), have the potential to improve health outcomes for people with chronic conditions. 8 In this review, social robots are defined as physical systems with autonomous or semi-autonomous interaction capabilities, often featuring mobility, sensing, and social responsiveness. They are distinct from software-only systems (eg, mobile apps and voice-assistants like Alexa or Google Home) and from diabetes-specific technologies, such as automated insulin pumps and continuous glucose monitors.
Research shows that SARs with facial expressions and social features improve perceived social intelligence, user acceptance, and engagement among older adults, compared with virtual characters on tablets or mobile apps.9-11 SARs offer companionship, enhance safety, and support complex self-management tasks. 12 Their feasibility is increasingly evident in managing conditions like diabetes, chronic obstructive pulmonary disease (COPD), and dementia,13-15 through functions such as health data collection (eg, blood glucose, blood pressure, and medication tracking), reminders, adherence monitoring, and health education.13-16
However, research on robotic applications for diabetes management is nascent, with limited focus across different age groups and diabetes types. Two earlier reviews examined SARs in children with type 1 diabetes, reporting improved diabetes knowledge and adherence to self-management,13,17 but no reviews have investigated their use in the broader diabetes population.
Our review fills this gap by exploring robotic technologies in diabetes care across the lifespan. It examines their impact on diabetes-related health outcomes and identifies facilitators and barriers to implementation. These insights aim to guide future research and inform the development of tailored, effective robotic interventions. The review follows PRISMA-ScR (Preferred Reporting Items for systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines 18 and the protocol was registered on the Open Science Framework (DOI: 10.17605/OSF.IO/5CZ37).
Methods
Study Design and Search Strategy
We conducted a scoping review using Arksey and O’Malley’s five-stage framework to map the literature, identify key concepts, and clarify knowledge gaps. 19 The search strategy was underpinned by the Population Concept and Context (PCC) framework to enable replication, strength and methodological rigor. In collaboration with a subject-matter librarian, CINAHL, Medline (via EBSCO), PubMed Central, Web of Science, Ovid Emcare, Ovid Nursing, Proquest SciTech Collection, IEEE Xplore, ACM Digital Library, Proquest Social Science Premium Collection, and gray literature databases were searched (Table 1). Supplementary searching was undertaken following the CLUSTER method 20 in Google Scholar, checking publications of lead authors, lists of included studies in similar reviews, and backwards and forwards citation searching of papers selected for inclusion via all other search methods. The inclusion and exclusion criteria are presented in Table 2.
Search Strategy.
Inclusion and Exclusion Criteria.
The review aimed to answer the following research questions:
Data Extraction and Synthesis
Potential papers identified through electronic searches were imported into Covidence, and duplicates removed. Two reviewers (AAB and RP) independently screened titles and abstracts, followed by full-text reviews. Discrepancies were resolved through discussion or consultation with a third reviewer (GW). A standardized data extraction form was piloted and revised (Tables 3 and 4). Consistent with scoping review methodology, 19 no formal quality appraisal was conducted, as the aim is to map literature breadth and depth without excluding studies based on quality. However, to ensure rigor and reliability in data extraction, the third reviewer (GW) performed a quality assurance check on all included studies, identifying one inaccuracy that was resolved through reviewer comparison, reference to original papers, and team consensus. Thematic content analysis, guided by Arksey and O’Malley’s framework, 19 was conducted in alignment with the research questions. Identified themes were organized and classified by the authors without predefined categories to minimize bias. Descriptive methods were used for quantitative data analysis. Results are presented using PRISMA (Figure 1), with the completed PRISMA-ScR checklist provided as Supplementary Material.
Study Characteristics and Data Collection.
Abbreviations: T1D, type 1 diabetes; OAT, off-activity talk; AI, artificial intelligence; T2D, type 2 diabetes; M, median; SD, standard deviation.
Study Findings.
Abbreviations: AI, artificial intelligence; HCPs, health care professionals; T1D, type 1 diabetes; T2D, type 2 diabetes; OAT, off-activity talk; SAR, socially assistive robot.
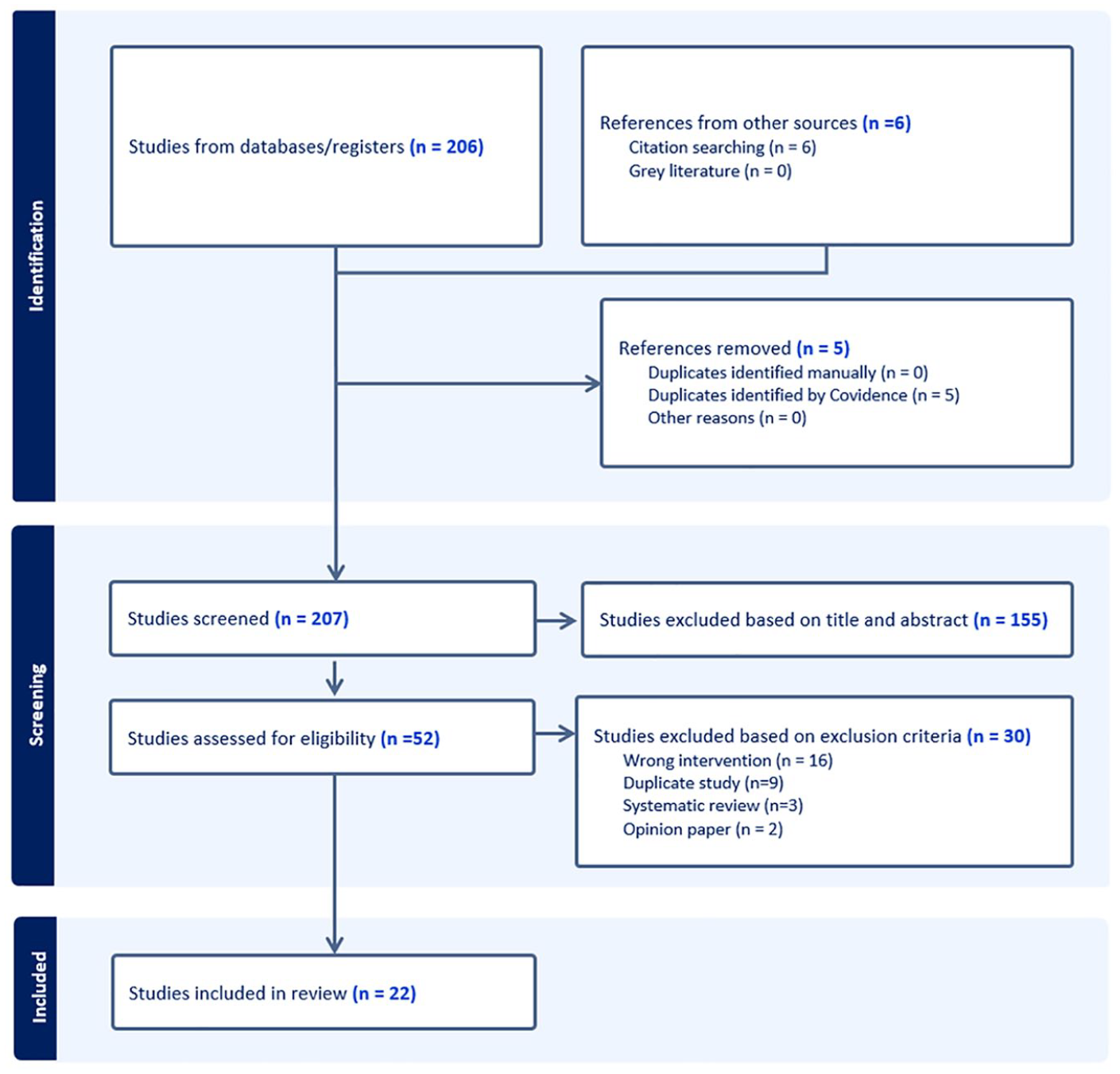
PRISMA diagram of study identifications, screening, and selection.
Results
Study Characteristics
A total of 212 papers were identified from the systematic literature search, and 22 met the inclusion criteria (Figure 1). Tables 3 and 4 provide an overview of the studies’ characteristics and findings.
Sixteen studies were conducted in Europe,21-23,26-29,31-35,37,38,40,41 five in Asia,24,25,30,36,42 and one in Australia. 39 The majority (n=18) of studies focused on children and young people with T1D, of which four included feedback from parents/caregivers26,29,35,38 and three from health care providers.23,29,35 Two studies focused on middle-aged and older adults with diabetes,30,42 and one did not include a specified population. 36 All except one paper 21 reported the setting of the study. Eleven studies22,24,25,27-29,33,35,37,39,42 were conducted in clinical settings, five took place in diabetes camps,26,29,34,37,40 and five focused on the use of robots in home environments.23,34,37,38,41 One study was conducted in community pharmacies, 30 and another in a science museum. 26
Study Designs and Aims
Eight studies22,23,30,31,34,35,38,41 used cross-sectional mixed-methods design and explored multiple aspects of robotic interventions, including emotional responses, engagement, and practical usability. Only one study used a randomized control study design, 25 comparing human-led versus robot-led interventions. Three studies27,28,33 employed quasi-experimental designs, two cross-sectional,24,42 and six21,26,29,37,39,40 qualitative. Two studies32,36 provided descriptive/conceptual frameworks without empirical data, evaluating software architectures for integrating SARs into e-Health platforms, and their potential in long-term diabetes management.
Twelve papers stemmed from two EU projects: ALIZ-E26-29,33,35,41 and Personal Assistant for a healthy Lifestyle (PAL).31,32,34,37,40 They describe the design of different facets of the respective systems and evaluate them in various roles, such as educators, motivators and friends. The ALIZ-E project focused on the AI-driven social robots, capable of effective and engaging interaction to support children with T1D, while PAL tested a hybrid e-Health platform combining the robot with an Embodied Conversational Agent (ECA) and mobile health apps for diabetes support in children.
Robotic Devices and Interventions
Fifteen studies used the Aldebaran NAO humanoid robot, 21 -23,26-29,31,32,35,37-41 a popular choice for STEM education and research in robot-child interactive systems due to its compact size, friendly humanoid-like appearance, and interactive capabilities (Figure 2). Three studies used other small humanoid robots: RoBoHoN, a small phone mobile robot by Sharp Corporation, 42 a wheeled semi-humanoid prototype robot called SARA, 24 and a small humanoid robot alongside other robot evaluations. 30 Only one study 25 used a larger robot—Pepper, a wheeled semi-humanoid with a chest-mounted tablet (Figure 2). Study 36 describes a robot-agnostic software framework and tested remote interaction with a NAO robot through videoconferencing. 38
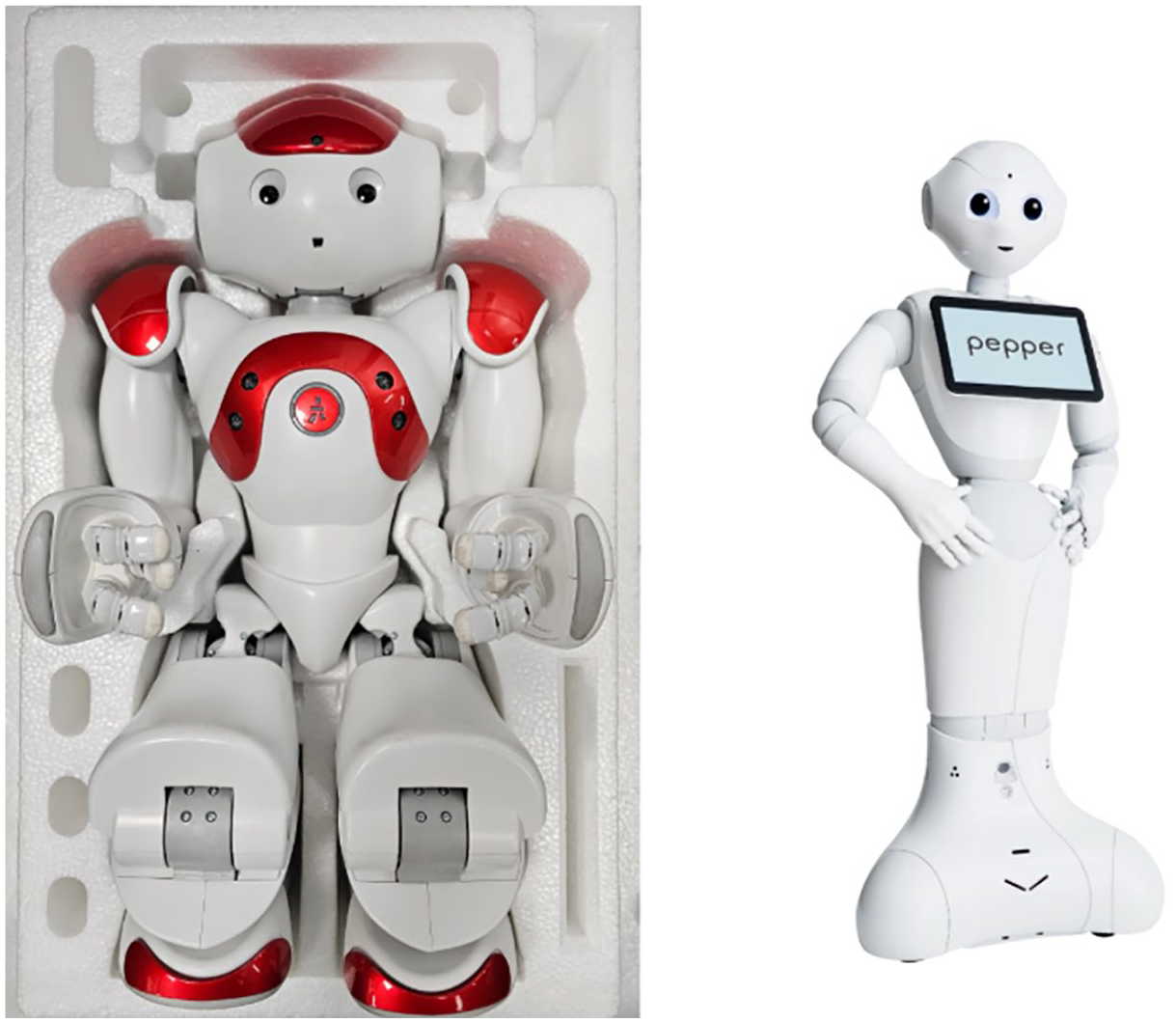
Humanoid robots: NAO (left) and Pepper (right), licensed under the creative commons attribution license 4.0.
Across all studies, interventions were socially interactive, promoting behavior change. Eleven studies detailed robots delivering behavior change, and support interventions aimed at building confidence and fostering empathetic interactions.23-26,29,30,35,37-39,41 Educational interventions were reported in nine studies, which included educational quizzes and sorting games.23-25,28-30,35,37,38 In six studies, self-management was also a feature and included diabetes diaries, carbohydrate counting, controlling high energy drink intake, and monitoring of glucose levels and food intake.21,23,26,33,34,39
Most of the SAR interventions were tested in scripted/semi-scripted experimental scenarios, requiring various degrees of supervision and control by researchers in short experiments through “Wizard of Oz” interfaces. Noticeable exceptions include the PAL system, whose cognitive architecture enabled autonomous interaction with children over several months, 32 and the system in, 39 which used a simpler rule-based approach to deliver two 60-minute couching sessions and two 15-minutes videos with a NAO robot over eight weeks. Table 4 provides a summary of the study findings.
Barriers, Enablers, and Health Outcomes Associated With SAR Use
The analysis revealed distinct themes related to barriers, enablers, and patient- and family-centered health outcomes associated with SAR use, as illustrated in Figure 3.
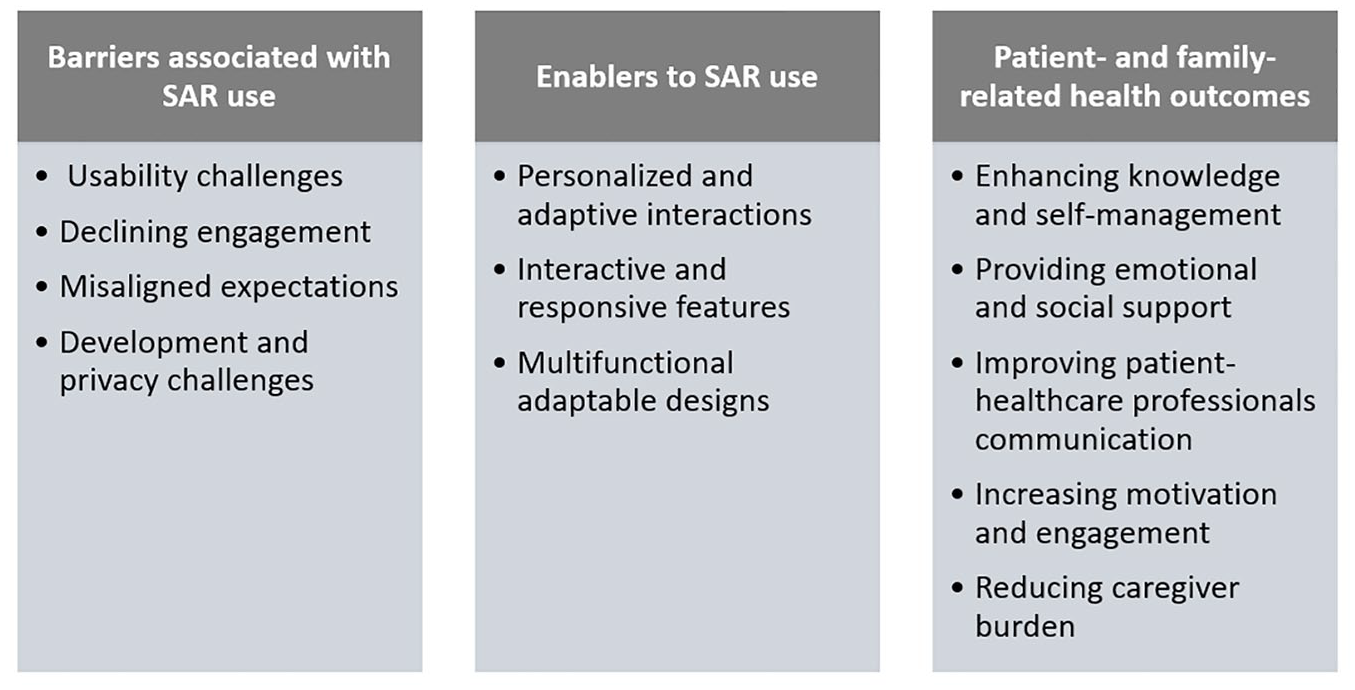
Barriers, enablers, and health outcomes associated with SAR use.
Barriers to SAR use: Practical challenges were cited as discomfort with eye contact, 38 limited customization, and usability concerns. 30 Engagement with the robots declined over time, particularly among older children, reducing motivation to interact with the robots consistently. 27 Misaligned practical and emotional expectations between what children hoped the robot would offer and what it provided, negatively affected their motivation and engagement. 34 Concerns regarding system integration, data privacy, and the technical scalability of robotic systems were reported as significant barriers to development. 32
Enablers to SAR use: Hybrid AI approaches enabled robots to tailor interactions based on user preferences and emotional states, enhancing their relevance and effectiveness.21,32,37,38,40 Interactive features, such as verbal communication, gestures, real-time feedback, and gamified components, enhanced user engagement, particularly for younger users.21,27-29,33,35,38 Emotional responsiveness through eye contact, empathy gestures, and expressions fostered rapport and emotional bonding.26,27,29,35,38,40 Robots also offered multi-functional capabilities, such as diabetes diaries, educational tools, decision support, and real-time monitoring, supporting cohesive diabetes self-management. Hybrid approaches combining avatars with real robots31,32,34,37,40 and using tele-conference software to access a real robot 41 were designed to increase access to expensive robot platforms, usually confined to research labs. Robots with modular designs, cloud connectivity, and integration with e-Health platforms, supported real-time updates, remote monitoring, and adaptability across diverse settings, including homes, clinics, and camps.23,26,30,32,36,37
Patient- and family-related health outcomes: Robots enhanced participants’ understanding of diabetes and improved their self-management skills by delivering tailored education on insulin use, diet, and physical activity.23,25,27-29,35,37 One study 30 showed that middle-aged and older adults benefited from self-directed learning using robots, while another 42 reported that robot-led interviews raised awareness of diabetes management, in adults with diabetes, positively affecting glycemic control. Robots also provided emotional support and companionship, reducing stress during hospital visits,26,29 and fostering engagement and motivation through emotional bonding.27,28,35,38,40,41 They enhanced communication among patients, families, and health care professionals through real-time feedback and streamlined data sharing,21,23,24,29,42 thus helping clinicians better address patient needs.21,23,32 Robots also reduced the burden on caregivers by encouraging patient autonomy, particularly among children, and by offering educational tools and real-time updates.26,29,35,37,41 Features like quizzes increased children’s interest and participation in self-management.27,28 Off-activity talk (OAT) sustained motivation for robot interactions, 33 while trivia games, verbal feedback, and physical interactions further boosted enjoyment and engagement.24,25,38,40
Discussion
To our knowledge, this is the first review to explore the effect of SARs on diabetes care across the lifespan, offering valuable insights into their application. The review emphasizes how participants interact with SARs and demonstrates their contribution to diabetes self-management. Findings indicate that SARs positively impact health by promoting confidence, knowledge acquisition, and effective lifestyle monitoring. Our findings suggest that future SAR designs should prioritize multi-modal capabilities to support behavior change, enhance self-management, and foster confidence and knowledge acquisition. Integrating cloud-based technology and AI allows real-time interactions and access to current information, though care must be taken to address potential risks associated with misinformation and disinformation during the design and decision-making process.
Many of the studies reviewed focused on children with T1D, reflecting a strong interest in this population. This focus likely stems from two key factors. Children are generally more receptive to playful, interactive technologies and benefit from emotionally engaging educational tools. In addition, early childhood is a critical period for developing lifelong self-management habits, making it a strategic time for intervention. 43 The studies demonstrate how SARs can enhance education, motivation and self‑management through gamification, storytelling and emotionally responsive interactions. These findings align with research involving children undergoing cancer treatment, where SARs were found to reduce anxiety and improve treatment‑related behaviors. 44 Similarly, SARs enhanced social communication and emotional engagement in children with autism 45 and promoted behavior changes like increased physical activity and improved inhaler technique in children with obesity and asthma.46,47 However, as with diabetes‑focused interventions, these studies report declining engagement over time due to the novelty effect and limitations in robot capabilities. This common challenge reflects a mismatch between user expectations and SAR functionality across conditions, highlighting the need for age‑appropriate, co‑designed interventions. 48
Whilst SARs appear effective in pediatric diabetes care, there remains limited evidence supporting their efficacy among adults. This discrepancy may stem from adult reluctance toward robotic assistance in favor of traditional human interaction, 49 caregiver resistance, 50 or a growing focus on AI in diabetes self-management.51,52 Despite the limited research on SARs in adults with diabetes, their successful application in other health contexts suggests strong potential for integration. For instance, SARs have improved adherence to physical therapy in cardiac rehabilitation, 53 COPD, 14 and poststroke care, 54 approaches that could be adapted to promote regular exercise—a key factor in glycemic control. Similarly, in elderly care, SARs have enhanced social interactions, reduced loneliness, and improved mood and cognitive engagement in older adults, including those with dementia.55,56 They have facilitated therapeutic activities and interactive conversations, contributing to better emotional well-being and overall quality of life. 57 Given the link between diabetes, cognitive decline, and emotional distress, 58 these combined benefits could enhance self-management in older adults with diabetes. However, unlike children who value SARs’ playfulness, older adults tend to prioritize practicality, reliability, cost-effectiveness, and maintaining genuine human connections. 59
While this review incorporates studies included in previous reviews on SARs in pediatric diabetes care,13,17 it extends existing findings by exploring barriers and enablers influencing their use. Identified barriers include usability challenges, such as limited customization, misaligned user expectations, declining engagement over time, and concerns about system integration, privacy, and scalability. In contrast to the two prior reviews on SAR use in older adults, which highlighted technological challenges as a barrier,60,61 our review did not observe this issue. Interestingly, prolonged use improved SARs use in older adults with dementia, 60 contrasting with the “declining engagement” theme observed here. These differences reflect the distinct needs of different demographic groups, emphasizing the importance of personalized interventions. Enablers, such as personalized interactions and multi-functional designs were consistently identified in our review and others,60,61 while emotionally responsive features showed mixed effects, facilitating or hindering use depending on context. 61 Addressing barriers, while leveraging enablers, is crucial to optimizing SARs to meet diverse user needs across demographics and settings.
A key strength of this review is its comprehensive literature search combined with a thorough data synthesis approach. However, the evidence included in this review is subject to some methodological limitations. Many of the studies included are cross-sectional, offering a snapshot of robotics potential benefits in diabetes care but lacking the ability to capture trends, variation, or longitudinal effects. Cross-sectional designs are also susceptible to selection and recall bias reducing the generalizability of findings. 62 Furthermore, comparative studies included were not sufficiently powered to draw definitive conclusions. Consequently, current evidence remains insufficient to support widespread implementation of robotic technology in health care. Another key limitation is the geographical concentration of studies in high-income countries (eg, Netherlands and the United Kingdom), with 16 out of 22 studies conducted in European settings. This limits the generalizability of findings to other cultural and health care contexts.
Furthermore, excluding non-English studies may have introduced language bias by omitting research from countries with advanced robotics, thereby limiting global relevance. However, this decision was necessary due to limited translation resources and the need to ensure consistent data extraction. Many studies were laboratory-based, possibly overestimating the acceptability and feasibility of robotic technologies compared with real-world environments. In addition, most studies were led by robotics experts with limited evidence of collaboration with health professionals, highlighting the need for interdisciplinary partnerships. Moreover, none of the reviewed studies assessed the environmental impact of their intervention. Advancements in health technology must prioritize environmental and social sustainability. Digital pollution is likely to escalate as increased efficiency and cost reductions drive higher consumption and demand. 63 Therefore, the immediate effects of such technologies may appear positive, long-term implications may prove detrimental.
Finally, it remains unclear how the cost of robotic technology compares to that of traditional health care provider visits aimed at coaching to optimize self-management. In the field of surgical robots, cost-benefit aspects have been explored, noting reductions in open surgery rates. 64 However, such interventions remain prohibitively expensive due to high material and depreciation costs. 65 In the context of AI, these applications may be more economically viable for treatment rather than diagnostic purposes. 66 Some reviewed papers explored ways to facilitate access to expensive robotic hardware by exploiting virtual avatars and/or video calls, as seen in the PAL project. While these approaches and nonembodied conversational agents like chatbots show promise, further research is needed to validate their cost-effectiveness and impact. 67
Recommendations for Future Research
To address the identified gaps, the following recommendations for future research are proposed:
Conduct robust, adequately powered randomized controlled trials involving both children and adults with diabetes, featuring at least 6 months of follow-up, to evaluate the effects of SARs on key clinical outcomes such as HbA1c, quality of life, and self-management behaviors in real-world clinical and home environments.
Incorporate cost-effectiveness analyses using tools, such as cost diaries and health service logs, comparing SARs with standard professional coaching from national health care payers’ perspectives.
Foster interdisciplinary collaboration among robotics engineers, health care professionals, behavioral scientists, and end users through participatory design to co-create and refine SAR prototypes.
Expand SAR research to low- and middle-income countries through partnerships with local institutions, adapting content to local languages and cultural norms using equity-focused frameworks.
Collaborate with environmental scientists to assess SAR interventions environmental impact, measuring lifecycle carbon footprint, energy use, and e-waste generation.
Conclusions
This review has provided a comprehensive and novel insight into the use of robotics in diabetes care across the lifespan. However, methodological limitations constrain the ability to draw definitive conclusions around widespread implementation in health care. Future robotic design for adults with diabetes should prioritize self-management support, confidence building, and knowledge acquisition. Future studies should adopt an interdisciplinary approach, ensure methodological rigor, and place greater emphasis on cost-benefit analysis, sustainability and patient-centered outcomes.
Supplemental Material
sj-docx-1-dst-10.1177_19322968251356298 – Supplemental material for Robotics Use in the Care and Management of People Living With Diabetes Mellitus: A Scoping Review
Supplemental material, sj-docx-1-dst-10.1177_19322968251356298 for Robotics Use in the Care and Management of People Living With Diabetes Mellitus: A Scoping Review by Amani Al Bayrakdar, Mauro Dragone, Gosha Wojcik, Alistair McConnell, Maria King and Ruth Paterson in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
AI, artificial intelligence; ECA, embodied conversational agent; IDF, International Diabetes Federation; OAT, off-activity talk; PAL, personal assistant for a healthy lifestyle; PCC, population concept and context; SARs, socially assistive robots; T1D, type 1 diabetes; T2D, type 2 diabetes; WHO, World Health Organization.
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.