
Abstract
Incorporating sex-specific factors in diabetes research and treatment is essential for advancing precision medicine. There are critical gaps in understanding and applying sex-related differences. Female-specific diabetes pathophysiology manifests in three major areas: life cycle phases (including puberty, pregnancy, and menopause), lifestyle factors (such as responses to nutrition and physical activity), and insulin pharmacology. These elements significantly affect insulin sensitivity and glycemic control in women, yet are frequently underrepresented or ignored in both research and clinical practice. Greater research and clinical focus across these domains is needed to better understand and address sex-based differences in diabetes. Identifying and filling evidence gaps will support more systematic and effective care.
Keywords
Introduction
Managing diabetes in women must account for physiologic factors that are unique to females and not present in males. These sex differences are often overlooked either because of a lack of data or because of a lack of appreciation of existing data. Sex is a biological feature, whereas gender encompasses the social features associated with the sex. This article focuses on sex features. Female physiology must be accounted for in three situations, including during (1) states and hormonal transitions related to the lifecycle, including the reproductive phase, pregnancy, gender-affirming hormone therapy, endocrine disorders, puberty, and menopause, (2) lifestyle management related to responses to nutrition and exercise, and (3) insulin pharmacology. Current treatment approaches for women with diabetes often fail to address critical factors related to reproductive state, life stage, and lifestyle that can all be affected by the person’s sex. 1 Living with type 1 diabetes (T1D) while undergoing gender-affirming hormone therapy presents unique and under-researched challenges, such as changes in insulin needs, insulin resistance, and diabetes self-management.
It is not clear that a “one-size-fits-all” approach is optimal, and such an approach is in strong contrast with the principles of precision medicine. 2 Physiological and pathophysiological factors that can affect women-specific precision medicine are presented in Figure 1. To advance diabetes management in line with the principles of precision medicine, it is essential to integrate physiological, pathological, and therapy-related insights into diabetes technology.2,3 Precision medicine centers on individualized care, tailoring treatment strategies to each person’s unique characteristics. This approach is especially important in diabetes technology, where sex differences significantly influence the usability, lived experience, effectiveness, and outcomes of advanced therapeutic tools such as automated insulin delivery (AID) systems, smartphone applications (apps), and other digital health solutions. By embedding considerations of a person’s characteristics directly into the design and functionality of these technologies, we can create more inclusive and effective tools that meet the diverse needs of a broader range of individuals living with diabetes.
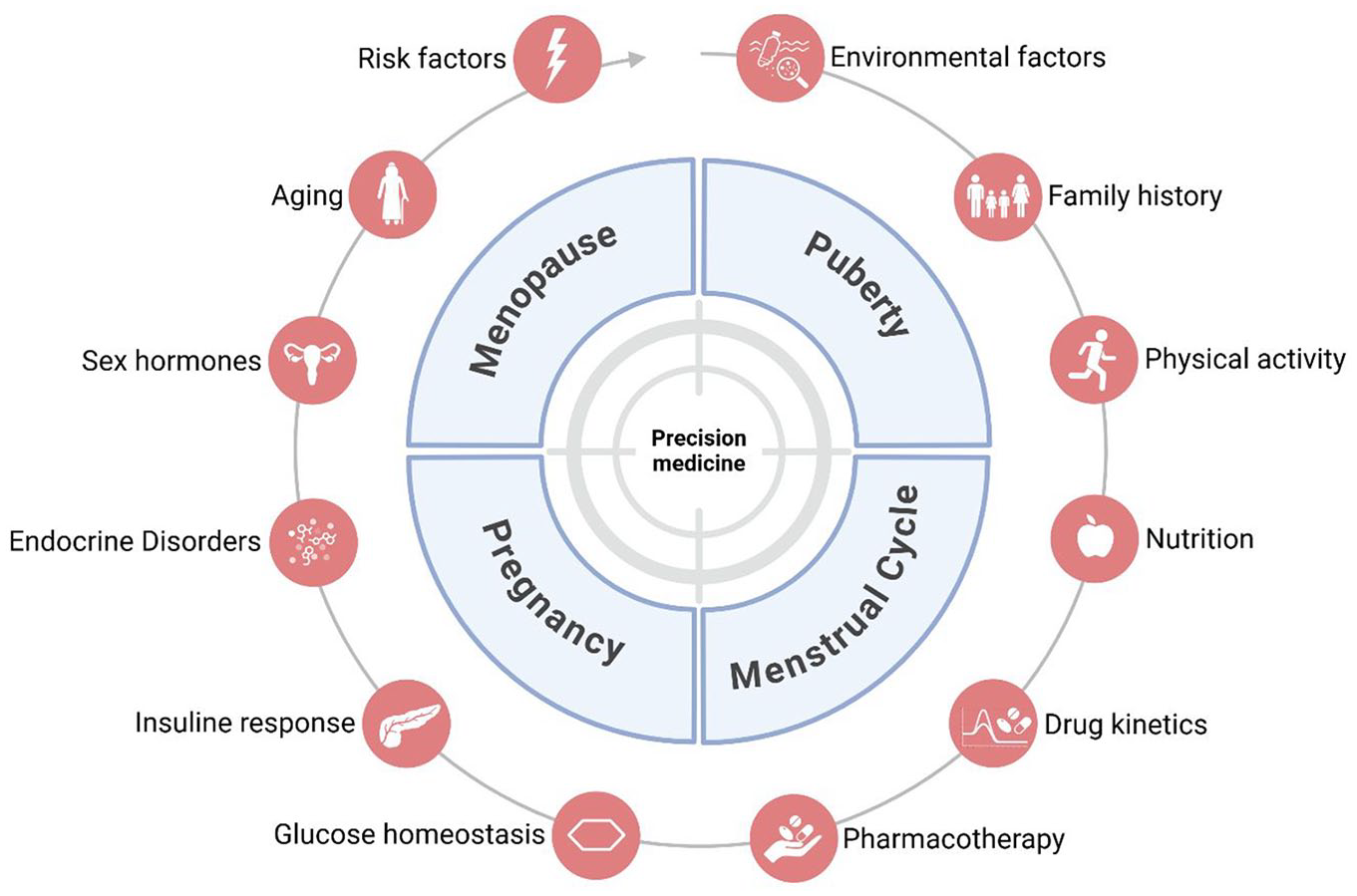
Sex-specific factors related to life cycle, lifestyle, and pharmacology that can affect diabetes management.
Based on data of how physiology affects women with diabetes related to life cycle, lifestyle, and insulin pharmacology, it will be possible to develop a fortified precision medicine approach. For example, sex hormones influence numerous aspects of glucose metabolism, including insulin sensitivity, gastric emptying, eating behaviors, body composition, and energy homeostasis. Yet, in the management of diabetes, these effects are typically not accounted for.
Better input into precision medicine management of diabetes will lead to improved outcomes. Many unique aspects of female pathophysiology are currently understood, but more research is needed to fully understand how sex difference in physiology affects diabetes. This knowledge will lead to opportunities for clinicians, researchers, and manufacturers to collaborate in integrating considerations of sexually dependent physiology into clinical research, the development of medical products for diabetes therapy, and diabetes care.
This editorial aims to underscore the significance of a sex-specific approach to diabetes management, which, in our opinion, can greatly improve the care of many patients with diabetes. Additional background about topics potentially relevant to the main themes of this commentary can be viewed in the Supplement to this article.
Life Cycle
Reproductive Phase
In adolescence, the menstrual cycle introduces additional complexity for women managing diabetes. Insulin sensitivity fluctuates throughout the cycle, with as many as 70% of women with T1D and a menstrual cycle experiencing a marked decrease of insulin sensitivity during the luteal phase,4-7 resulting in increased glycemia and significant variability in time spent within the target glucose range.4-6 Current treatment protocols fail to account for variations in insulin requirements throughout the menstrual cycle, emphasizing the need for research and technological innovations, such as AID systems and apps, that are capable of more precise adaptation during different cycle phases. These variations are currently neglected in the international consensus guidelines, which recommend a minimum of 14 days of continuous glucose monitoring (CGM) data to report time in range (TIR). This duration is insufficient to capture glycemic variations throughout the menstrual cycle, which typically spans 28 to 30 days and includes distinct phases associated with changing levels in glycemia.
Pregnancy
The reproductive years bring unique challenges for women with T1D, especially during pregnancy when maintaining stricter glycemic targets (63-140 mg/dL) is essential for both maternal and fetal health. 8 While AID systems are transforming T1D management, only one system is currently cleared for use during pregnancy. 9 Most AID systems lack algorithms tailored for both pregnancy- and breastfeeding-specific physiology, leaving people living with T1D and their health care providers to navigate fluctuating insulin requirements, increased hypoglycemia risks, and delays in insulin action without adequate technological support. While open-source systems like DIY Loop and OpenAPS offer more customizable features grounded in lived experience, they are not explicitly designed to support hormonally driven life stages such as pregnancy, breastfeeding, or menopause. As a result, individuals must often rely on manual adjustments or community-sourced workarounds, placing a significant cognitive and emotional burden on users during already vulnerable periods. In addition, the global increase in cases of type 2 diabetes (T2D), obesity, and cardiovascular diseases highlights the critical role of maternal and paternal peri-gestational factors on fetal programming of metabolic and cardiovascular conditions in offspring.10-12 This emphasizes the need for precise, intergenerational diabetes technologies.
Gender-Affirming Hormonal Therapy
Living with T1D while undergoing gender-affirming hormone therapy presents unique and under-researched challenges, such as changes in insulin needs, insulin resistance, and diabetes self-management, all compounded by the psychological stress of navigating often non-affirming health care systems. Inclusive, respectful care, and research that center the lived experiences of trans and non-binary individuals are essential to improving health outcomes and fostering trust in diabetes care.
Endocrine Disorders
Conditions such as polycystic ovary syndrome (PCOS), which is the most common endocrine disorder in women, are associated with insulin resistance and a higher risk for T2D.13-16 These disorders are also accompanied by fertility challenges and represent a sex-specific cardiovascular risk.17-19 Knowledge of the interplay between endocrine disorders and diabetes may improve diabetes control on an individual level and furthermore support individuals to improve reproductive and cardiovascular health.
Puberty
Adolescence presents unique challenges for people living with T1D, as hormonal changes during puberty lead to physiological insulin resistance and increased glycemic variability. 20 Elevated HbA1c levels and difficulties with weight management during this stage are compounded by psychological, hormonal, and physical changes, while being exposed to both a greater likelihood of engaging in more risk-prone behaviors and the pressures of managing a chronic condition during a formative life stage.21-23 Despite advancements in CGM and AID systems, which have proven safe for use during puberty, these technologies are not fully optimized to address the specific needs of teens, leaving a gap in holistic and tailored support during this critical stage.
Menopause
As women transition into menopause, declining estrogen levels decrease insulin sensitivity and lead to increased glycemic variability. Symptoms like night sweats, mood swings, and sleep disturbances complicate diabetes management, yet current AID systems lack targeted adaptations for this stage of life. 24 Further research is critical to ensure diabetes technologies can support women effectively during menopause and adequately address the impact of these hormonal shifts.
Lifestyle
Nutrition
Nutrition plays a vital role in diabetes management, and sex-specific needs must be considered to optimize health outcomes for people living with T1D. Hormonal balances and fluctuations, body composition, and metabolic rates differ between sexes, all of which affect dietary requirements.25,26 For instance, women often require higher levels of iron and folic acid due to menstrual cycles, pregnancy, and lactation. At the same time, men generally need more calories and protein to support greater muscle mass. However, most dietary guidelines are standardized across sexes, highlighting an urgent need for research and guidelines that reflect these fundamental differences in nutritional needs.
Exercise
Exercise impacts glucose levels differently in women and men, with women showing a smaller decrease in glucose levels during physical activity compared to men. This is partly due to sex hormone-dependent differences in fuel utilization: women may rely more on lipid metabolism, which alters glucose variability during exercise.27,28 Despite this evidence, current exercise protocols for managing T1D are predominantly based on male-centric data, highlighting the need for sex-specific studies to develop more accurate insulin adjustment guidelines for non-males. 29
Insulin Pharmacology
Research on insulin formulations for diabetes management of insulin-treated patients often neglects potential sex differences in pharmacokinetic and pharmacodynamic aspects, because women may be underrepresented in some phase 1 trials that primarily use male participants to reduce variability. Despite known variations in insulin sensitivity across menstrual cycle phases and differences in body surface or total body water, for example, regulatory agencies do not mandate sex-specific pharmacokinetics and pharmacodynamic studies, leaving a significant gap in understanding the sex-specific differences of insulin action. 30 Systematic evaluations and analyses of existing data focusing on differences between sexes could enhance personalized diabetes care.
Conclusions and the Future of Personalized Diabetes Care: Toward Precision Sex-Aware Diabetes Care
Over the past decades, we have witnessed a revolution in diabetes management across all life stages, driven also by new technologies that facilitate targeted, personalized care.
Leveraging data from CGM and AID systems enables the development of tailored strategies to address specific needs at different life stages, from puberty, through reproductive age and pregnancy, menopause, to old age. Comprehensive CGM data analysis and evaluation of glucose patterns across hormonal phases, such as menstrual cycles, menopause, and transitions experienced by transgender and gender-diverse individuals, can enhance individualized care, and digital tools tailored to these hormonal variations could improve outcomes for all.
Necessary steps to properly achieve precise, personalized, and effective reproductive health needs in women, compared to men, with diabetes require addressing sex differences in (1) life cycle events, (2) lifestyle responses to nutrition and exercise, and (3) insulin pharmacology for insulin-treated patients. Achieving this potential requires a commitment to sex-sensitive research to address specific needs. Designing medical products with sex factors in mind is essential to make the care of people living with T1D more accurate irrespective of their sex. Ultimately, regulatory requirements and economic advantages may help drive the development, prescription, and use of devices and treatment plans that recognize differences in sex-specific physiology.
We are in an era of using precise individualized data to treat patients with diabetes and other diseases. The saying that “one size does not fit all” pertains to the need for more research into sex-specific pathophysiology in treating and applying technology to treat diabetes.
Definitions
Sex refers to the biological and physiological characteristics that define individuals as male or female, such as chromosomes, hormones, and reproductive anatomy.
Gender is a social construct that includes the social, cultural, psychological, and behavioral aspects of being a gender by encompassing the roles, behaviors, identities, and societal expectations associated with being a man or a woman, which can vary across cultures and over time.
Supplemental Material
sj-docx-1-dst-10.1177_19322968251340673 – Supplemental material for One Size Does Not Fit All: The Need for Sex-Specific Precision Medicine in Diabetes Technology
Supplemental material, sj-docx-1-dst-10.1177_19322968251340673 for One Size Does Not Fit All: The Need for Sex-Specific Precision Medicine in Diabetes Technology by Stefanie Hossmann, Susanne Tan, Julia K. Mader, David C. Klonoff, Dawn Adams, Hanne Ballhausen, Lia Bally, Maria L. Balmer, Vincent Braunack-Mayer, Anne Bonhoure, David Burren, Charlotte K. Boughton, Deniz Cengiz, Claudia Eberle, Chiara Fabris, Maya Friedman, Elke Fröhlich-Reiterer, Tim Gunn, Olga Gusyatiner, Theresa Hastings, Valentina V. Huwiler, Saira Khan-Gallo, Carol J. Levy, Othmar Moser, Aisling Ann O’Kane, Cameron Keighron, Nick Oliver, Temiloluwa Prioleau, Tanja Thybo, Jane Yardley, Thomas Zueger, Gabriele Faber-Heinemann, Lutz Heinemann and Martina Rothenbühler in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors acknowledge Diabetes Center Berne for this study.
Abbreviations
AID, automated insulin delivery; apps, applications; CGM, continuous glucose monitoring; HCP, health care provider; PCOS, polycystic ovary syndrome; TIR, time in range; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.