
Abstract
Background:
The development of diabetes technology is rapid and requires education and resources to be successfully implemented in diabetes care management.
Method:
In an observational study, we evaluated the use of advanced diabetes technology, resource utilization, and glycemic control. The study population was 725 individuals with type 1 diabetes (T1D) living in Region Halland, Sweden. The study cohort was followed for 7 years between 2013 and 2019.
Results:
Children aged 0 to 17 years were associated with significantly better glucose control than young adults aged 18 to 25 years. The mean HbA1c in children and young adults was 53 mmol/mol (7.0%) compared to 61 mmol/mol (7.7%) (P < .0001), respectively. Comorbidities such as attention deficit hyperactivity disorder (ADHD), autism, and coelic disease were associated with higher HbA1c. All groups, regardless of age and comorbidity, showed a positive effect on glucose control after visiting a dietitian or psychologist. Differences were found between the age groups in terms of more use of advanced diabetes technology and more frequent visits to a physician in children compared to young adults.
Conclusions:
More frequent visits to physicians, and a visit to dietitians, and psychologists were associated with improved glucose control in individuals with T1D 0 to 25 years. Increased resources, including access to more advanced technologies, may be required in young adults with T1D.
Introduction
Diabetes, including type 1 diabetes (T1D), is associated with the development of both microvascular and macrovascular complications.1,2 These long-term diabetic complications have been associated with significant adverse effects on the quality of life,3,4 as well as an elevated risk of morbidity and excess mortality of individuals with diabetes, 5 and leading to substantial costs to healthcare systems across patients’ lifetimes. 6
The incidence of T1D is increasing worldwide 2 were new cases of T1D in Europe are rising at the rate of 3.4% annually, and if the current trend continues, the incidence is likely to double in the next 20 years. 7 In Sweden, the incidence of pediatric-onset T1D has doubled in the last 40 years to 43.9 per 100,000—the second-highest incidence rate in the world.2,8
The development and implementation of diabetes technology, including digital solutions, are crucial components to support the management of chronic diseases. 9 Technology offers innovative solutions to reduce the burden of chronic disease. Digital solutions can be used to inform the individual with diabetes on therapeutic decision-making and thus lessen the burden of disease. Furthermore, diabetes technology has improved clinical outcomes and reduced healthcare needs. 10 However, insufficient education of patients and health care providers (HCP) and the cost of these digital solutions can be a barrier to the successful implementation of diabetes technology. 11 Within diabetes, where digital tools are frequently used, healthcare payers need evidence to make value-based decisions on digital technology.
Economic analyses are used to support healthcare decision-making. 12 One such method is cost-utility analysis, which provides evidence on health gains and resource implications of specific interventions by comparing the costs of interventions with expected outcomes. 13
For people with diabetes, there are a growing number of digital technologies available that enable optimized monitoring of lifestyle and pharmaceutical interventions and capture accurate data that can aid healthcare professionals in decision-making. 14
Besides Advanced Hybrid Closed Loop (AHCL) systems smart insulin pens are one such digital tools. These devices can record both the timing and dose of insulin delivered. In addition, these devices can be combined with intermittently scanned or real-time continuous glucose monitoring (is-CGM/rt-CGM) data and smartphone applications.
From a patient perspective, insulin pumps and smart insulin pens have the added benefit of capturing data on insulin delivery compared to standard insulin pens. Insulin pumps connected to rt-CGM in T1D are related to an improved glycemic control, and reduced rates of hypoglycemia. 15 Furthermore, rt-CGM has been shown to reduce HbA1c during a 3-year study, regardless of insulin pump or insulin pen treatment. 16 When smart insulin pens were introduced to a cohort of people with T1D already using CGM in Sweden, improved glycemic control (increased time in range, TIR), reduced time in hypoglycemia, and fewer missed bolus insulin doses17,18 were achieved. In the future, smart insulin pens in combination with rt-CGM may lead to further improved diabetes self-management and address an unmet need for patients to become more actively engaged with their diabetes care in this population of people with T1D. 17
It is essential to understand the effects on healthcare costs and the expected health outcomes associated with improvements in glycemic control and increased bolus insulin doses. In addition, as multidisciplinary diabetes teams are involved in the treatment, there might also exist bottlenecks in the healthcare organization or a lack of resources preventing advances in diabetes care and diabetes management. The aim of the study was to describe patterns and predictors associated with changes in glucose control in T1D for different age groups.
Methods
A non-interventional descriptive, retrospective, register study in Region Halland, Sweden, was conducted. The study was in accordance with the World Medical Association Declaration of Helsinki and approved by the national ethical review board (Dnr 2020-05779). All participants signed informed consent before inclusion in the study.
Data Sources
The existing cross-linked individual-level data from the comprehensive database Regional Healthcare Information Platform (RHIP) in Region Halland were used. 18 RHIP is a database containing costs related to each individual, defined diagnoses and pharmacological treatment, allowing long-term health economic evaluation. In addition, data on current medication was retrieved from Swedish Prescribed Drugs Register, and dose dispensing data from the pharmacy Apoteket (Apodos). Data regarding the use of technology were retrieved from the Swedish National Diabetes Registry (NDR).
Study Population
The study cohort consisted of 725 individuals in the age group 0 to 25 years, living in the Region Halland, Sweden, and being registered with the diagnosis T1D according to the International Classification of Diseases version 10 (ICD-10) during the study period 2013 to 2019.
Study Procedure
The study cohort was divided into a pediatric group aged 0 to 17 years, and a young adult group aged 18 to 25 years, both with T1D. Among these patients, the gender, and the individuals’ age at diabetes diagnosis was registered. Patients with T1D diagnosis before 2013 were removed to provide a consistent basis for analysis. In addition, concomitant diseases such as anxiety (ICD-code F41), depression (F32-33), anorexia/bulimia (F50), attention deficit hyperactivity disorder (ADHD) (F90), autism (F84), coeliac disease (K90), and obesity (E66) were registered.
HbA1c was registered for all patients during the study period and followed over time. A HbA1c <57 mmol/mol (7.4%) was considered as good control, and a HbA1c >57 mmol/mol (7.4%) as poor control.
Health Care Utilization
RHIP assembled data regarding the number of hospital admissions and the number of hospital days regarded as in-patient care (IPC). All the hospital-based Outpatient Procedure Component (OPC) visits were divided into the hospital clinics such as pediatric/adult-, the emergency department (ED), psychiatric-, and other hospital clinics. For all these OPC visits, the number of visits was distributed between physicians, diabetes, and regular nurses within the hospital care. Moreover, visits to paramedical professions such as dietitians, occupational therapists, physiotherapists, and psychologists were registered. Furthermore, the number of telephone- and video contacts was documented. The visits at primary health care were also retrieved and divided between types of visits, physician, nurse, dietitian, occupational therapist, physiotherapist, and psychologist.
Model for Calculating Healthcare-Related Costs
Patient encounter costing (PEC) methodology was used to calculate the resource utilization costs based on data retrieved from the database RHIP. PEC is a modified form of time-driven activity-based calculation of health-related costs that have previously been described by Kaplan.19-21 In this method, all encounter costs are created from the separate billable procedures and the attributable costs (including drugs, radiology examinations, and laboratory tests). Furthermore, the costs are made from the unit costs for each resource and the quantities of the resources used. The separate attributable costs are assigned to each patient encounter based on established abilities of internal Region Halland derived costs, which are applied internally by Region Halland and are updated regularly based on acquired costs. Resource unit costs for not internally assessed services are determined based on total spending for a specific resource divided by that ward or clinic’s actual production. The unit of analysis for IPC was expressed as the number of days spent admitted to the hospital, and for out-patient and PHC number of clinic visits was used. The number of days admitted to the hospital for each specific in-patient ward, and the number of out-patient clinic visits for each specific out-patient clinic were assumed to have the same cost basis. An individual ’‘encounter’s cost was consequently the product of the number of resources used with the unit resource cost, plus all separately costed procedures or other attributable costs. Total healthcare costs were subsequently assessed as the sum of all encounter costs for each patient for each year.
Statistical Analysis
Continuous data are summarized as mean ± SD and categorical data are presented as percentages. For continuous and categorical data, an independent t-test assuming unequal variances and fisher-exact test was used, respectively. For hypotheses testing of continuous data over multiple categorical variables, a 1-way ANOVA test was employed. All P-values were 2-tailed and P < .05 was considered statistically significant. Analysis was performed using SAS, version 9.4 (SAS Institute Inc.).
Results
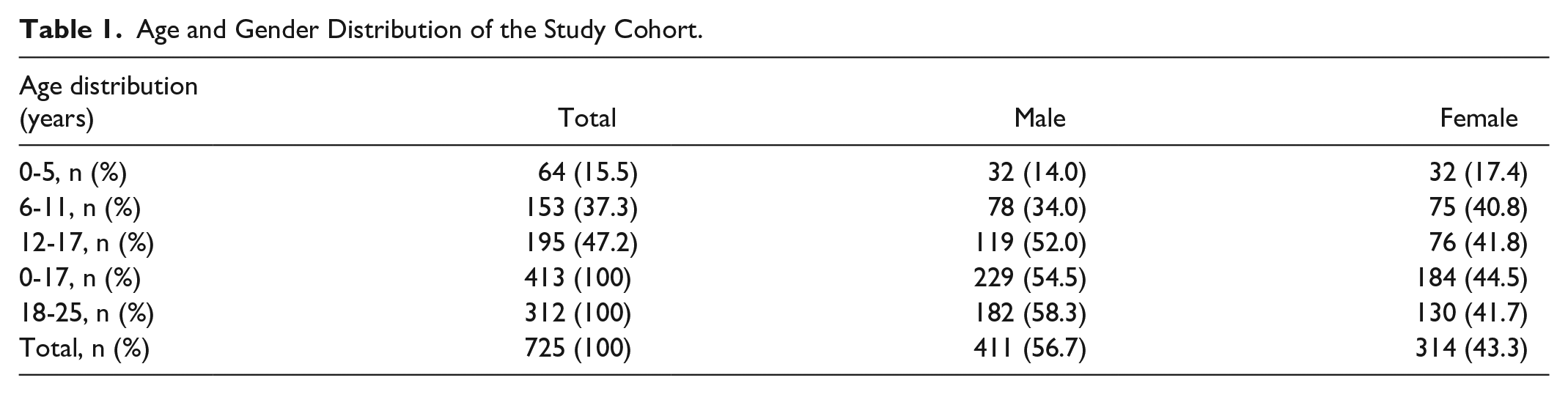
There were a total of 725 patients with T1D aged 0 to 25 years in Region Halland. This group was divided into 2 cohorts, the pediatric (0-17 years), and the young adults (18-25 years), with 413 pediatric and 312 young adult individuals, respectively. Table 1 shows the age and gender distribution, and Table 2 shows the prevalence of concomitant diseases in the cohort. Yearly mean HbA1c was associated with a continuous reduction over time in the pediatric population. In contrast, HbA1c was relatively stable in the young adult population, see Figure 1. In 2019, children were associated with better HbA1c control; 53 mmol/mol (7.0%), compared to 61 mmol/mol (7.7%) (P < .0001) for the young adults. The difference regarding yearly mean HbA1c between children and young adults was consistent and increasing during 2013 to 2019. The yearly mean HbA1c difference was 1 mmol/mol in 2013 and 9 mmol/mol in 2019 with a summarized mean difference of 5 mmol/mol during the 7 years, Table 3.
Age and Gender Distribution of the Study Cohort.
The Distribution of Concomitant Diseases and Gender in Pediatric Population (Aged 0-17 years) and in the Young Adult Population (Aged 18-25 years).
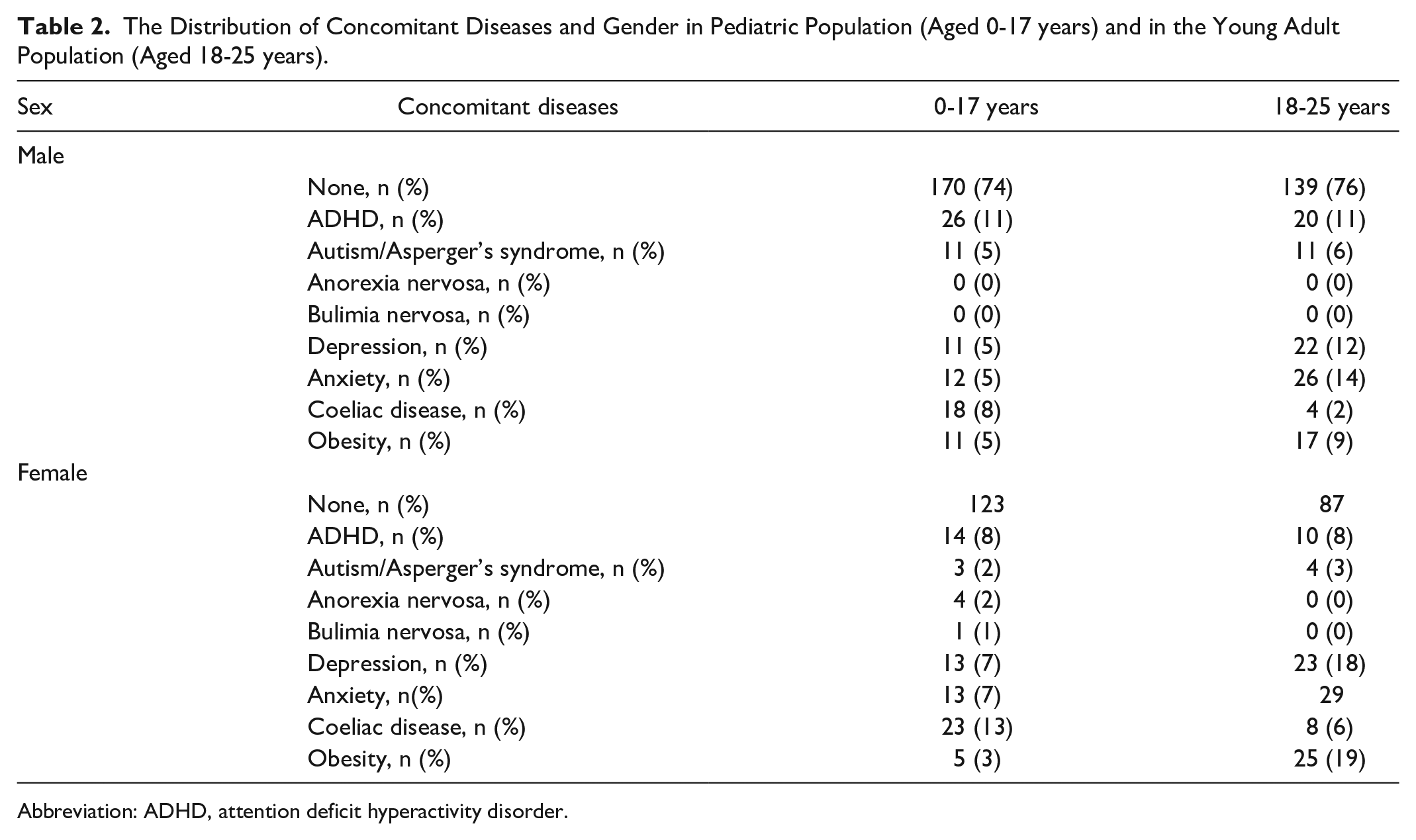
Abbreviation: ADHD, attention deficit hyperactivity disorder.
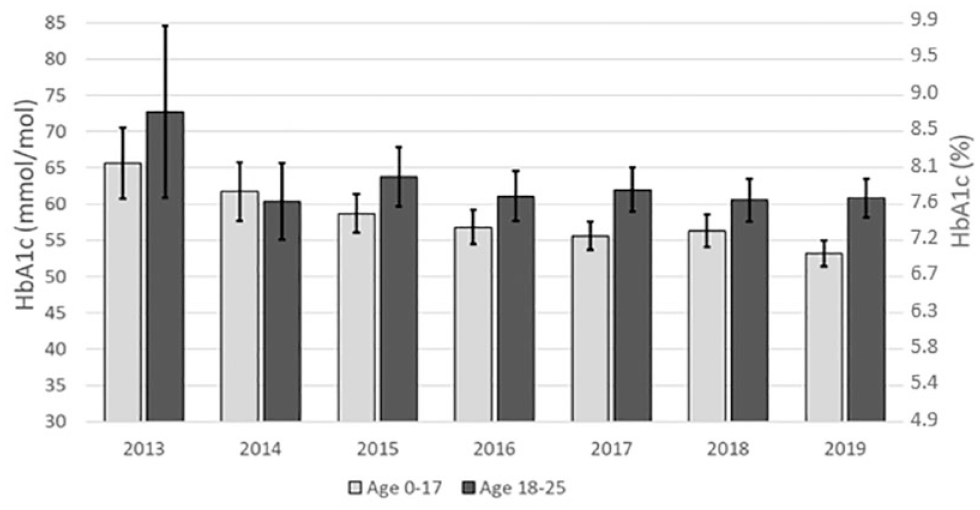
The mean HbA1c for each year of the study period for the pediatric population (light gray) and for the young adults (dark gray). Patients with index for diabetes diagnosis before 2013 and/or diabetes duration <3 months are excluded. Error bars show 95% confidence interval for the mean HbA1c values.
Glucose Control and Use of Diabetes Technology at Pediatric and Adult Diabetes Centers Region of Halland, 2013-2019.
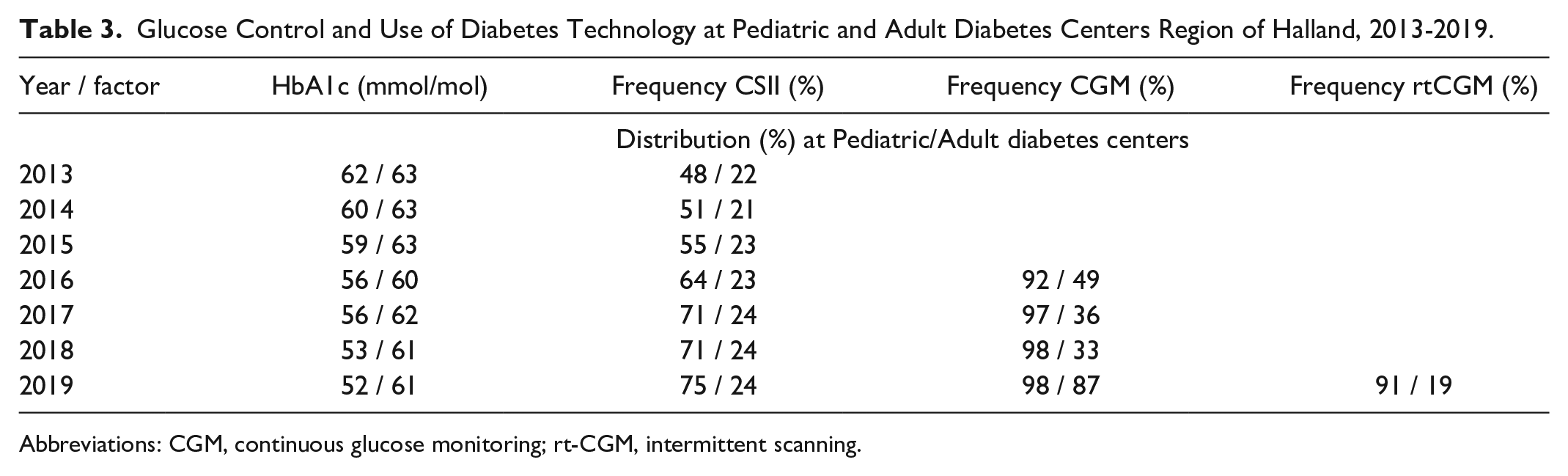
Abbreviations: CGM, continuous glucose monitoring; rt-CGM, intermittent scanning.
The proportion of individuals achieving good glucose control, defined as HbA1c <57 mmol/mol (7.4%) during each separate year, was higher in the pediatric population compared with the young adults as illustrated in Figure 2.
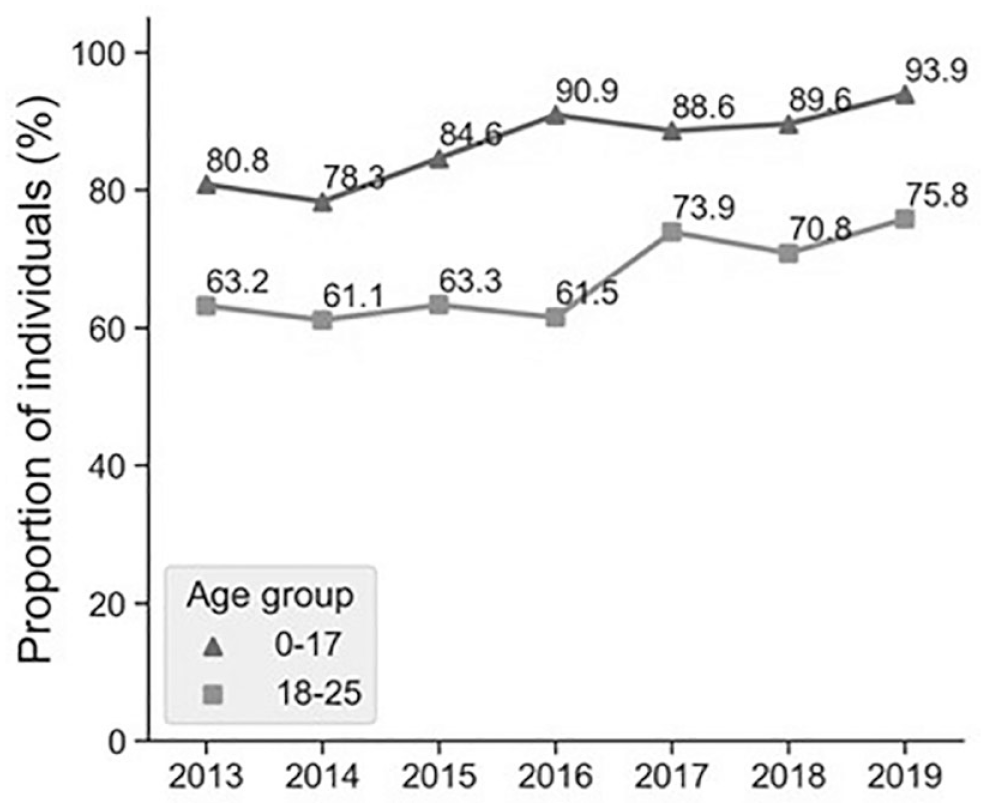
Proportion of individuals, pediatric and young adults, reaching HbA1c <57 mmol/mol 1 year after diabetes diagnosis.
The difference of the proportion achieving HbA1c <57 mmol/mol between children and young adults was in mean 21.4% during the 7 years (range: 15%-31%), Figure 2.
Analyses regarding the use of technology reveal that in children the use of CSII increased from 48% to 75%. The respective proportion using CSII among young adults was 22% (2013) and 24% (2019) shown in Table 3.
The registration in NDR regarding the use of CGM was started 2016, and the registration of the distribution between is-CGM and rt-CGM started 2019. In children 92% used CGM in 2016, and 98% in 2019. In young adults, the respective proportion was 49% in 2016, and 87% in 2019. A clear difference was noted in 2019 regarding the distribution between is-CGM and rt-CGM with 91% of the children respective 19% of the young adults using rt-CGM, Table 3.
There was an association of elevated HbA1c in all age intervals with coexisting neuropsychiatric disorders ADHD and autism. Whereas celiac disease was associated with elevated HbA1c values in young adults, this pattern was not seen in children. The mean HbA1c individuals having co-morbidity is shown in Table 4.
Individuals With T1D in Different Age Strata With Concomitant Diseases and Corresponding Mean HbA1c Value (SD) in IFCC mmol/mol and NGSP%.
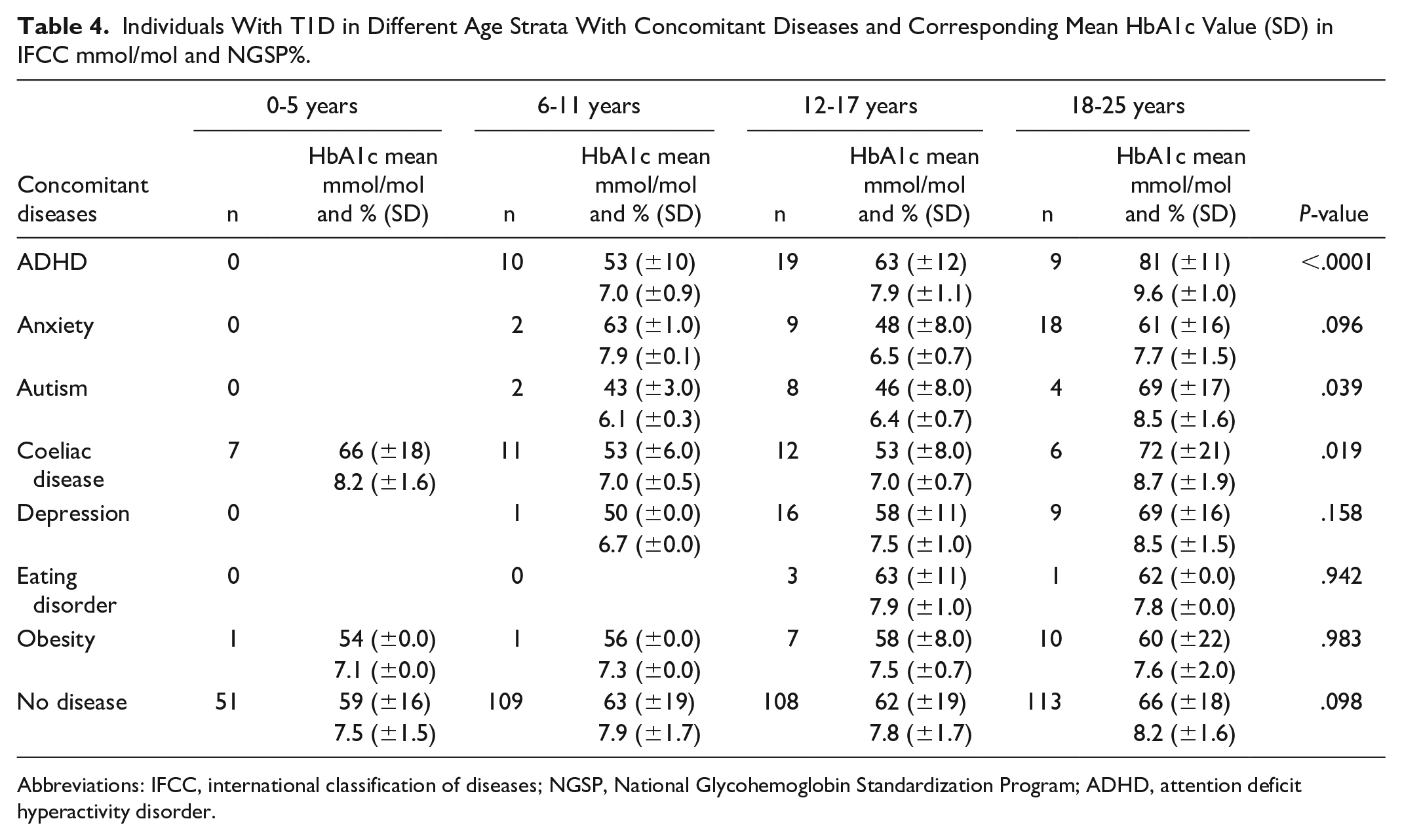
Abbreviations: IFCC, international classification of diseases; NGSP, National Glycohemoglobin Standardization Program; ADHD, attention deficit hyperactivity disorder.
After a visit to a dietician HbA1c was significantly improved over the study period, with a mean difference (SD) -11.1 (19.1) mmol/mol and -16.2 (26.6) mmol/mol in individuals 0 to 17 years and 18 to 25 years, respectively (Figure 3).
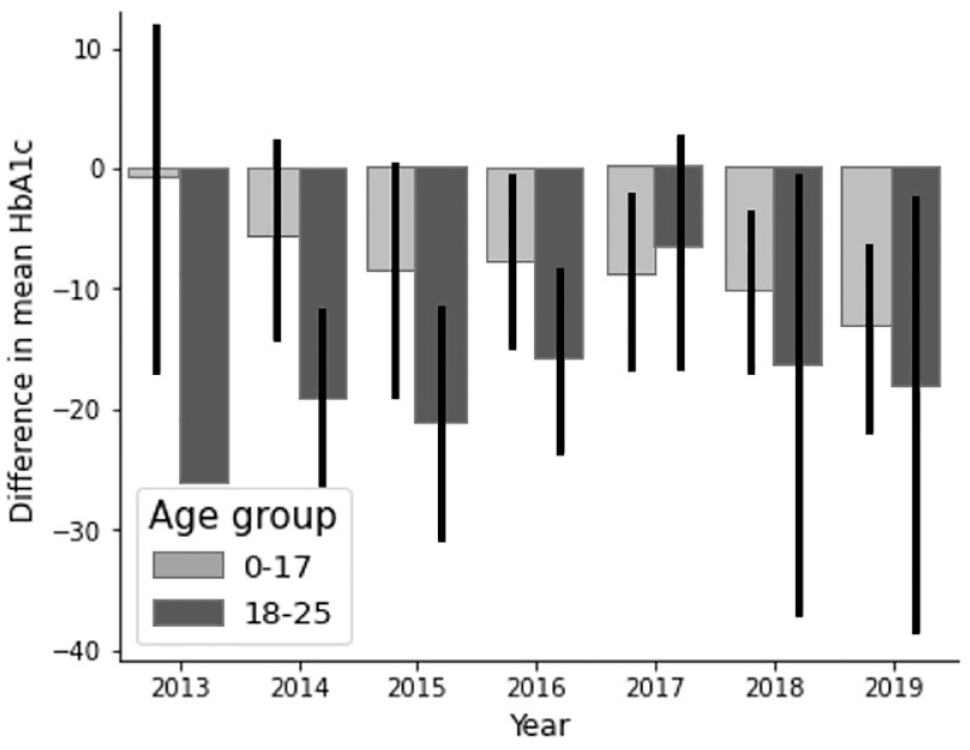
Change in HbA1c after visit to dietician. Mean difference (SD) in HbA1c -11.1 (19.1) mmol/mol and -16.2 (26.6) mmol/mol in individuals 0 to 17 years and 18 to 25 years respectively.
The same pattern was noted after a visit to a psychologist with a difference in mean HbA1c (SD) -9.25 (24.9) mmol/mol and -6.21 (21.7) mmol/mol in individuals 0 to 17 years and 18 to 25 years, respectively (Figure 4).
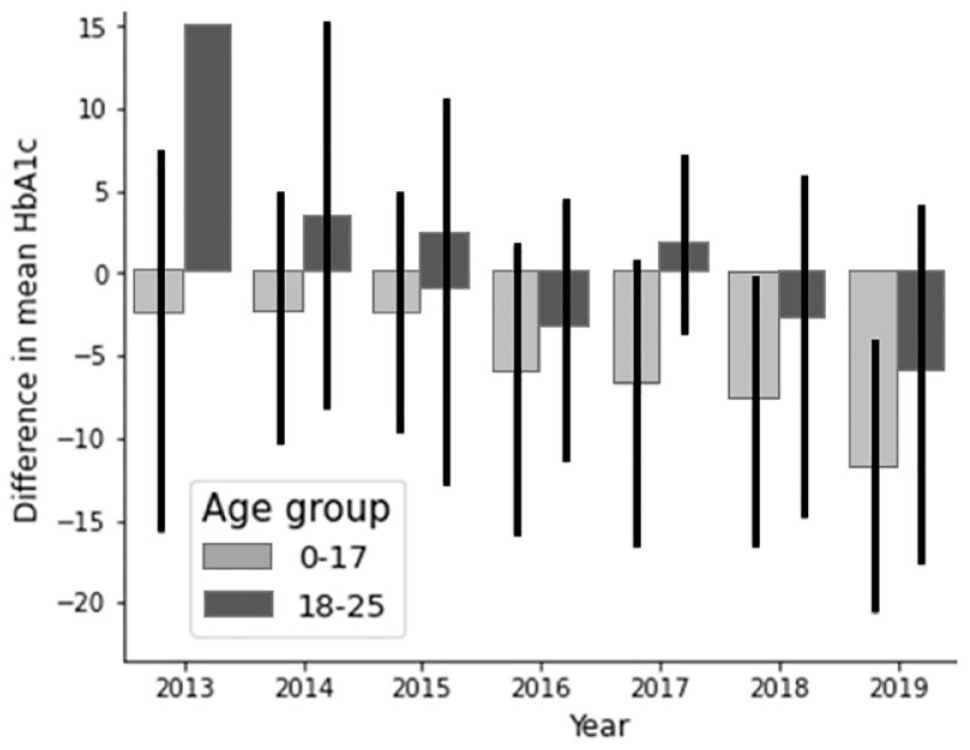
Change in HbA1c after visit to psychologist. Mean difference (SD) in HbA1c after visit -9.25 (24.9) mmol/mol and -6.21 (21.7) mmol/mol in individuals 0 to 17 years and 18 to 25 years respectively.
Costs
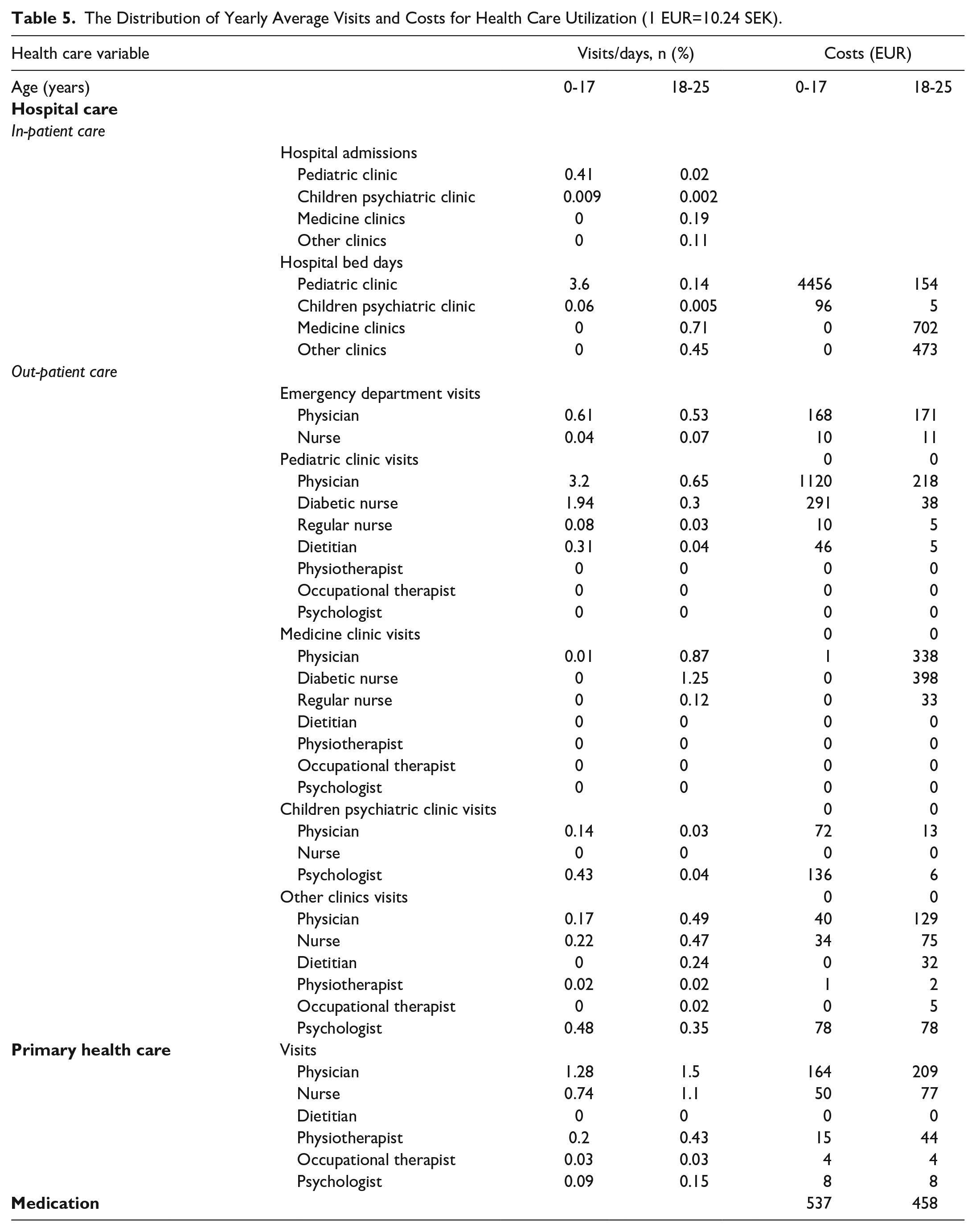
The health care utilization is presented in Table 5 and illustrates the average number of yearly visits for each healthcare provider and is separated into the different age groups. The children, 0 to 17 years, had a total of 3.6 average hospital days, and the corresponding numbers for the young adults, 18 to 25 years, is 1.3 days. The major cost driver was the duration of hospitalization, especially among the age group 0 to 17 years, whose hospitalization cost on average was 4.661 EUR while the young adult’s annual average hospitalization cost was 1.365 EUR. Attributed costs for hospital in-patient care were significantly higher for children compared to young adults, shown in Table 5.
The Distribution of Yearly Average Visits and Costs for Health Care Utilization (1 EUR=10.24 SEK).
Discussion
This study indicates a difference in the glucose control achieved among children (0-17 years) compared with young adults (18-25 years). Children were associated with a better glucose control compared to young adults, where the average difference amongst the groups was 8 mmol/mol (0.8%) during the study period.
The diabetes management at the pediatric clinics has steadily showed improved glucose control year by year in Sweden, while this is not seen among young adults. Improvements are seen both as reductions in HbA1c and the proportion of patients achieving good glucose control, HbA1c <57 mmol/mol, (7.4%). This difference between age groups could be associated with the increased use of rt-CGM and CSII among children compared to more stabile use of these devices in young adults.
Among both children and young adults, the detrimental effects of neuropsychiatric illnesses such as ADHD and autism affect all age groups. Visits to a dietitian and psychologist appear to be associated with prolonged improvements in glucose control. Psychology support to the young adults seems to have an even better than technology regarding glucose control. However, in the study, the visits of both dietitians and psychologists were unchanged during the study period, which may be linked to limited resources or the need for better selections of the individuals that require dietitian or psychologist contact.
When access to more advanced technology in diabetes is analyzed, there is a difference between children and young adults. Among children, rt-CGM is associated to a greater use compared to young adults. This increased use can also be defended via the recently published review, including 37 recommendations related to advanced technology in diabetes treatment. 22
In this study, we have analyzed costs overall and their relationship to various resources within the diabetes care management team. Differences are seen above all regarding the number of visits to physicians each year. The differences are also seen regardless of the severity of diabetes, indicating that the resources are limited. Unfortunately, the difference seen in glucose control leads to an increased risk of long-term diabetes complications.
Study limitations: This study is a retrospective, descriptive, register study covering a period between 2013 and 2019. Technology has developed significantly during the same period and has also been applied differently in the 2 age groups we analyzed in the study. However, the study’s strength is that we have been able to use the RHIP database to clarify the differences in resource utilization and costs.
The 2 age groups are heterogeneous and many factors apart for age differs, such as a higher prevalence of obesity, anxiety, and depression in the older group, therefore, it is difficult to compare these 2 age groups. Furthermore, it is not possible with the current study design to identify if it was the number of visits or use of diabetes technology that was associated with the reduction in HbA1c.
Measures to reduce the differences between use of diabetes technology in the 2 age groups can thus be justified. A transition to equal and improved diabetes care could be done by increasing resources and perhaps by creating a new form of diabetes clinic for young adults aged 18 to 25 years. This should be done with adequate resources and implementation of methods at the diagnosis of diabetes and follow-up the use and efficacy of advanced diabetes technology, similar to what is done at the pediatric diabetes clinics.
Conclusions
This study indicates differences in the effectiveness of diabetes care between children and young adults. Bearing in mind the difficulties of achieving good glucose control, adequate support is needed regardless of age or comorbidities.
Previously, puberty has been associated with impaired glucose control. Now, with the differences demonstrated in this study, young adults aged 18 to 25 years arise as “the new puberty” in the field of diabetes care. The results of this study call for an effort to improve glucose control and health among young adults with type 1 diabetes.
A diabetes team for young adults could be implemented to mitigate this inequality between age groups found in our study. Increased resources and strategies to improve glucose control will likely lead to numerous positive effects, with a reduction in burden of disease, and reduced long-term costs in T1D, but this has to be shown in clinical studies.
Footnotes
Acknowledgements
We would like to thank Hallandia V AB for licenses to perform data extraction from the Regional Healthcare Information Platform.
Abbreviations
(ADHD) Attention Deficit Hyperactivity Disorder, (ATC codes) Anatomic Therapeutic Chemical classification system, (ED) Emergency Department, (is-CGM) intermittent scanning Continuous Glucose Monitoring, (rt-CGM) real-time Continuous Glucose Monitoring, (HCP) Health Care Provider, (ICD) International Classification of Diseases, (IFCC) International Federation of Clinical Chemistry, (IPC) Inpatient Care, (NGSP) National Glycohemoglobin Standardization Program, (OPC) Outpatient Procedure Component, (PEC) Patient Encounter Costing, (RHIP) Regional Healthcare Information Platform, (T1D) Type 1 Diabetes, (TIR) Time in Range, (QALY) Quality Adjusted Life Years
Authorship
All named authors meet the International Committee of Medical Journal Editors criteria for authorship of this article, and take responsibility for the integrity of the work, and have given their approval for this version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Air Liquid and by Nordic Infucare.