
Abstract
Background:
No widely adopted continuous glucose monitoring (CGM)-based insulin titration protocol exists, which may limit the effects of inpatient CGM on glycemic and clinical outcomes. We evaluate the acceptability and operability of the protocol proposed by Olsen et al for inpatients with type 2 diabetes in non–intensive care unit (non-ICU) settings.
Method:
7 inpatient diabetes team members, responsible for daily insulin titration, decided on insulin adjustments for 353 days. The members had the option to follow the CGM-based insulin protocol or override it for basal, prandial, and correctional insulin, separately, in 84 inpatients monitored by CGM. Questionnaires were used to evaluate the protocol’s operability by the teams.
Results:
Of 456 basal insulin titration decisions, 439 (96.3%) adhered to the protocol. For prandial insulin, adherence rates were 83.9% (125/149) for breakfast, 87.2% (130/149) for lunch, and 92.6% (138/149) for dinner (p=0.163). All correctional insulin titrations adhered to the protocol. All team members expressed a preference for having a protocol for CGM-based insulin titration and rated the protocol’s usability on a 1 to 10 scale, with mean scores (SD) of 8.7 (0.9) for basal insulin, 8.3 (1.4) for prandial insulin, and 7.4 (1.9) for correctional insulin.
Conclusions:
The CGM-based insulin titration protocol by Olsen et al has been successfully implemented for titrating basal, prandial, and correctional insulin in inpatients with type 2 diabetes in non-ICU settings. It was highly accepted by inpatient diabetes teams and provides a framework for effective CGM implementation in these settings.
Introduction
Effective management of in-hospital hyperglycemia relies on insulin therapy, yet creating individualized insulin regimens is challenging due to altered glucose metabolism during hospitalization and limited specialized diabetes care across wards. 1 The result is often high glycemic variability, hypoglycemia, and hyperglycemia, which are linked to increased morbidity, prolonged hospital stays, and higher mortality rates.2-4
Inpatient standard-of-care glucose monitoring relies on point-of-care (POC) glucose testing by finger stick, typically performed 3 to 5 times daily, leaving significant data gaps, especially overnight. These gaps complicate insulin titration and increase the risk of dysglycemia and its associated complications. 5 Continuous glucose monitoring (CGM) offers a promising alternative by providing real-time glucose data and a comprehensive glycemic profile. Despite its proven benefits in outpatient settings, CGM has shown limited success in hospitals likely due to lack of diabetes-trained staff, and lack of effective and operational CGM-based insulin titration protocols.6-15
International guidelines advocate for protocolized CGM-based insulin titration, yet no standardized or widely adopted protocols currently exist.13,16,17 This absence may lead to clinical inertia, where health care providers hesitate to make timely insulin adjustments even when real-time CGM data are available. 18 Therefore, an operational CGM-based insulin titration protocol may be critical to realize CGM’s potential to improve inpatient glycemic control and clinical outcomes.19,20
This analysis seeks to evaluate the acceptability and operability of the CGM-based insulin titration protocol by Olsen et al, 18 as previously demonstrated in the DIAbetes TEam and Cgm (DIATEC) trial, which integrated protocolized CGM-based insulin titration with inpatient diabetes teams, resulting in significant clinical and glycemic improvements compared with POC glucose testing. 20 Furthermore, the protocol’s operability as perceived by inpatient diabetes teams is assessed.
Method
Data are from the DIATEC trial. 20 From April 11, 2023, to March 29, 2024, we enrolled 166 non-ICU medical and surgical patients with type 2 diabetes from Copenhagen University Hospital—North Zealand and Herlev-Gentofte Hospital, aged ≥18, and expected to stay in the hospital for at least 2 days. Key exclusions criteria included patients on long-acting basal insulin >24 hours (insulin glargine 300 U/mL or insulin degludec), those on systemic glucocorticoids (prednisone >5 mg/day), or with dialysis or an estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2. Additional criteria are published. 18 In total, 84 patients were randomized to have glucose monitoring by CGM, and 82 patients randomized to have glucose levels assessed daily via POC glucose testing and insulin titration via a CGM- or POC-based insulin titration protocol, respectively. 18
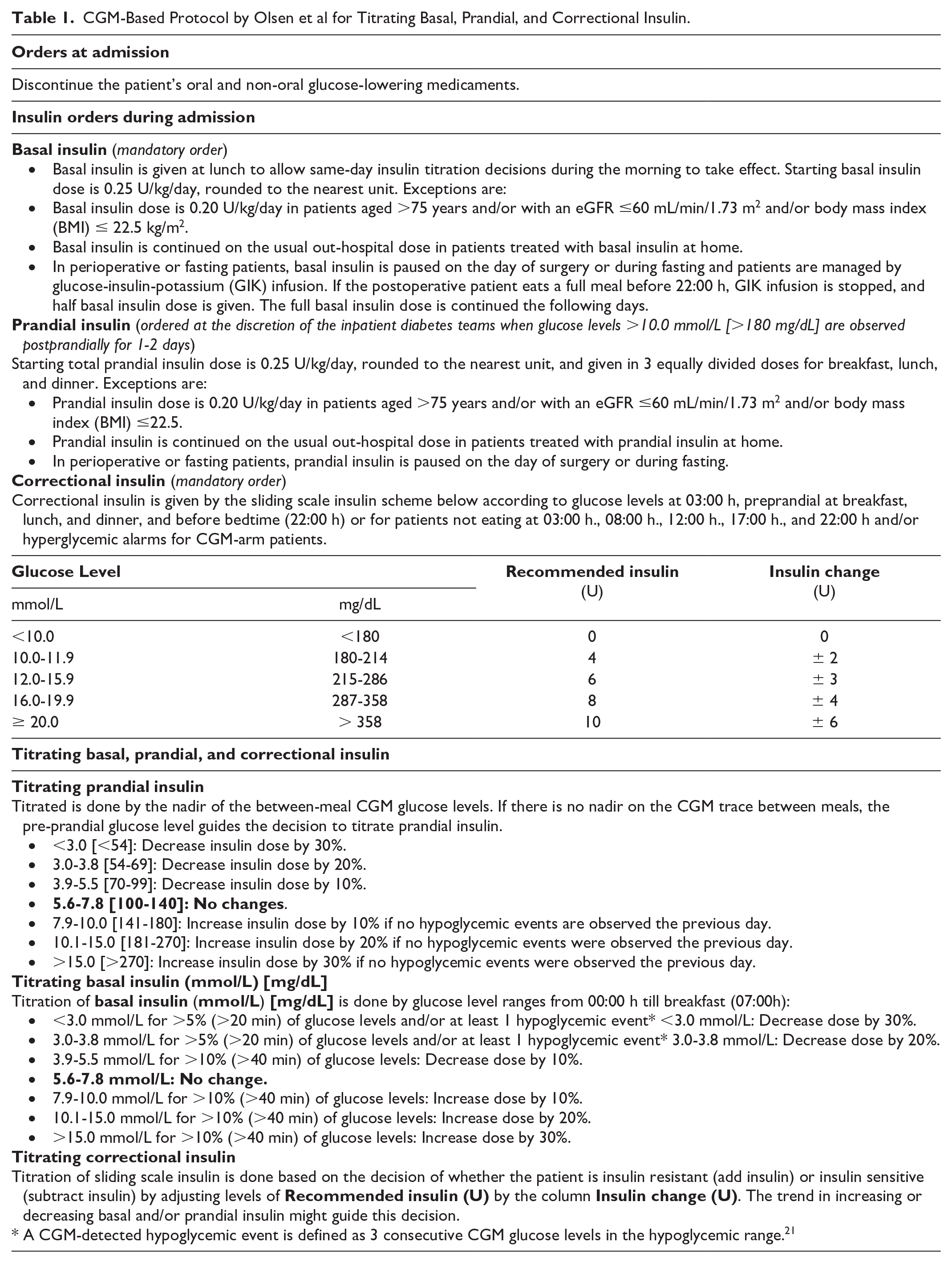
Each day, inpatient diabetes teams were required to decide on insulin titration for basal, prandial, and correctional insulin, using either the Olsen et al protocol (Table 1) or their clinical discretion. We assessed the adherence to the protocol by tracking all decisions related to titration of basal, prandial, and correctional insulin, separately, during hospitalization. We then determined whether these decisions followed the protocol or were modified by clinical discretion. If an insulin dose decision deviated from the protocol and was instead based on clinical discretion, we recorded the difference in insulin units between the recommended dose from the protocol and the actual dose administered. The inpatient team had the option to provide a comment when deviating from the protocol. Seven members of the inpatient diabetes team responsible for daily insulin titration completed questionnaires evaluating the operability of the protocol (Table 2).
CGM-Based Protocol by Olsen et al for Titrating Basal, Prandial, and Correctional Insulin.
Questions for the Inpatient Diabetes Teams on the Operability and Efficacy of the Olsen et al 18 CGM-Based Insulin Titration Protocol.
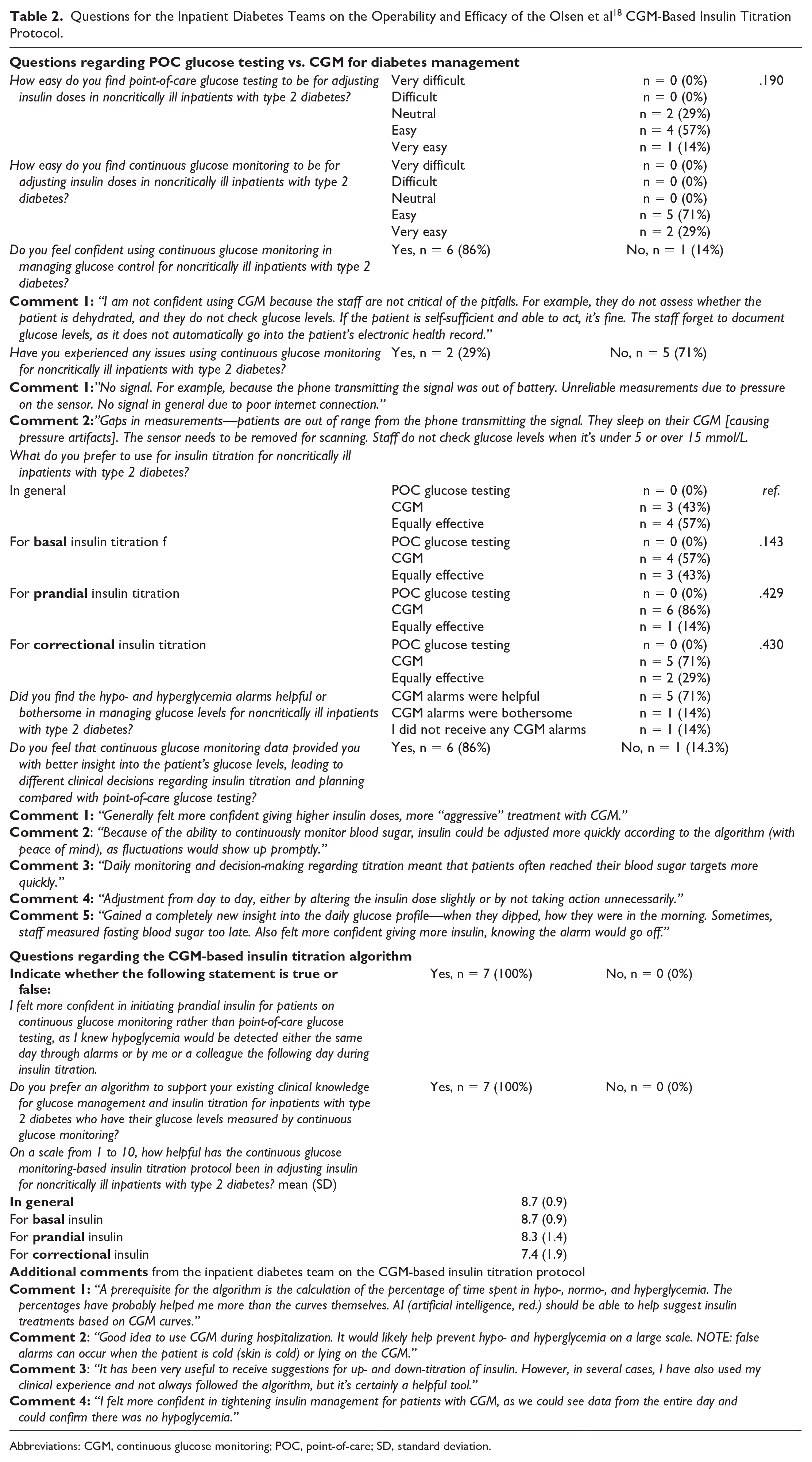
Abbreviations: CGM, continuous glucose monitoring; POC, point-of-care; SD, standard deviation.
Outcomes
The primary outcome in this analysis was to assess the degree of adherence to the Olsen et al CGM-based insulin titration protocol. Secondary outcomes included a questionnaire-based evaluation (Table 2) of the protocol by the inpatient diabetes teams applying the protocol.
Description of the CGM-Based Insulin Titration Protocol
At admission, noninsulin antidiabetic medications were discontinued, and patients were initiated on a basal-bolus insulin regimen of 0.4 to 0.5 U/kg/day distributed equally between basal insulin and prandial insulin for the 3 main meals.18,22 Prandial insulin was ordered at the discretion of the inpatient diabetes teams when glucose levels >10.0 mmol/L were observed postprandially for 1 to 2 days. Correctional insulin was also administered.
In general, daily insulin adjustments adhered to the recommendations from the Olsen et al protocol, though the recommendations could be overruled at the clinical discretion of the inpatient diabetes teams when deemed necessary. Basal insulin was increased for sustained fasting (nighttime) hyperglycemia, and prandial or correctional insulin was initiated or increased for hyperglycemia during the day. CGM-detected hypo- (<3.9 mmol/L) and hyperglycemia (>13.9 mmol/L for 2 hours) alarms were activated and notified the inpatient diabetes teams. POC glucose testing was used to verify hypoglycemia due to reduced CGM sensor accuracy at lower glucose levels. 23 CGM trend arrows were not considered. The full CGM-based insulin titration protocol by Olsen et al is outlined in Table 1.
Rules for CGM-Based Insulin Titration
Two rules applied to CGM-based insulin titration in a prioritized order.
Rule of the lowest
Prioritizes low glucose levels when both low and high glucose levels occur during a titration period, provided both exceed the percentage-based thresholds in Table 1. This rule directs a reduction in basal and/or prandial insulin to prevent hypoglycemia.
Rule of the extremes
Extreme glucose levels that deviate from the titration range of 5.6 to 7.8 mmol/L (100-140 mg/dL)—whether consistently below, consistently above, or partially within and outside the titration range—are prioritized, for example, level 2 (>13.9 mmol/L) over level 1 (10.0-13.9 mmol/L) hyperglycemia, as the first range represents a more significant (“extreme”) deviation from the target range.
Ethical Statement
Before enrollment, all subjects provided informed written consent. The Ethics Committee of the Capital Region of Denmark approved the study (journal number 2301240). The DIATEC trial was prospectively registered with ClinicalTrials.gov as NCT05803473.
Statistical Analyses
Categorical variables were compared with the chi-squared test and presented as n (%). A generalized estimation equation model was applied to test whether there was a development over time in whether the CGM-based insulin titration protocol was followed or overruled by clinical decisions. As the inpatient diabetes teams were off shifts during weekends, and no insulin titration decisions were made, only insulin titration decisions from weekdays were analyzed. Linear mixed regression models were used to model the impact of nonadherence to basal and/or bolus (prandial) insulin titration on changes in consensus CGM-outcomes 13 compared with within-subject glycemic periods when insulin titration adhered to the protocol. Consensus CGM-outcomes included time in range (TIR), 3.9 to 10.0 mmol/L; 3 levels of time above range (TAR) 10.0 to 13.9 mmol/L, >13.9 mmol/L, and >10.0 mmol/L; 3 levels of time below range (TBR) 3.0 to 3.9 mmol/L, <3.0 mmol/L, and <3.9 mmol/L; mean glucose level; standard deviation (SD) of the CGM glucose distribution, and coefficient of variation (CV. hypoglycemic events were not modeled due to zero-inflation of the outcome. For basal insulin titration nonadherence, glycemic status from the following night was paired with the preceding nonadherence event, and periods of protocol adherence were also paired accordingly. Similarly, for bolus (prandial) insulin nonadherence, glycemic status from the subsequent 4-hour period was paired with the nonadherence event, with protocol-adherent glycemic periods following the same structure. The linear mixed regression analyses were adjusted for the day of admission. Statistical significance was set at a 2-sided P-value ≤.05.
Results
Baseline of Inpatients With Type 2 Diabetes
Baseline characteristics are published elsewhere. 20 Briefly, 84 subjects were managed by CGM during hospitalization with a mean (SD) age of 76.6 (9.5) years, of which 52 (61.9%) were males. The duration of diabetes was on average (SD) 13.0 (8.6) years and 17 (20.2%) were treated with insulin therapy before hospitalization.
Baseline Characteristics of the Inpatient Diabetes Teams
Two individuals (29%) were from the Copenhagen University Hospital—North Zealand, and 5 individuals (71%) were from Herlev-Gentofte Hospital with an average (SD) experience of 16.0 (4.9) years as working with inpatient diabetes management being employed at the current workplace of 10.9 years (4.2) and with 8.0 (4.6) years as an inpatient diabetes specialist.
Evaluation of CGM-Based Insulin Titration Protocol
Among 456 basal insulin titration decisions made for 84 subjects during hospitalization, 439 (96.3%) adhered to the protocol. The decisions that deviated from the protocol regarding basal insulin were, on median (IQR), 2.3 (4.0) U lower than the amount proposed by the protocol (Table 1) and the mean (SD) dose of basal insulin was 17.6 (9.7) U/day. Out of 149 prandial insulin decisions made for breakfast, lunch, and dinner in 41 subjects, the protocol was followed in 125 (83.9%), 130 (87.2%), and 138 (92.6%) instances, respectively (P = .163). The decisions that deviated from the protocol regarding breakfast, lunch, and dinner prandial insulin, respectively, were median (IQR) 1.0 (1.0) U, 1.0 (1.0), and 2.0 (1.0) lower than the amount proposed by the Olsen et al protocol and the mean (SD) dose of basal insulin was 5.8 (3.7) U/day. All correctional insulin doses adhered to the protocol. All deviations from the protocol regarding prandial and basal insulin were due to fear of hypoglycemia as expressed by the inpatient diabetes teams.
There was no development over time in whether the Olsen et al protocol was followed or overruled by clinical decisions regarding basal insulin (P = .954), breakfast prandial insulin (P = .941), lunch prandial insulin (P = .702), and dinner prandial insulin (P = .338). The same pattern was observed with no statistically significant differences across both sites and between surgical and medical wards (data not shown). No significant differences were observed in outcomes, including TIR, TAR, TBR, mean glucose, SD, or CV, when comparing glycemic periods with protocol adherence to those with nonadherence (all P > .05, data not shown).
CGM alarms for hypoglycemic events (<3.9 mmol/L) occurring prior to the usual time stamps for POC glucose testing with corrective insulin were triggered in 12 patients in the CGM arm (14.3%). Among these, 5 patients had 1 alarm, 4 had 2 alarms, 2 had 4 alarms, and 1 had 8 alarms. For hyperglycemic events (>13.9 mmol/L lasting at least 2 hours), alarms were triggered in 22 patients (26.2%), with 12 patients having 1 alarm, 4 having 2 alarms, 3 having 3 alarms, 1 having 4 alarms, and 2 having 6 alarms.
Experience From the Inpatient Diabetes Teams With the CGM-Based Insulin Titration Protocol
The results are summarized in Table 2. All 7 (100%) inpatient diabetes team members preferred having a protocol for CGM-based insulin titration. They rated its usability for titrating basal, prandial, and correctional insulin on a 1 to 10 scale on average (SD) as 8.7 (0.9), 8.3 (1.4), and 7.4 (1.9), respectively. The inpatient diabetes team found the Olsen et al protocol as easy to use as the POC glucose testing-based insulin titration protocol (P = .190).
Six inpatient diabetes team members (86%) expressed confidence in using CGM for managing glucose control in inpatients with type 2 diabetes, although signal loss in the telemetric CGM-setup 24 was mentioned in the commentaries as a primary issue with inpatient CGM use (eg, due to Bluetooth disconnections between the CGM and the smartphone running the Dexcom G6 app, internet connectivity issues between the smartphone and the Dexcom Clarity webpage, sensor or transmitter malfunctions, etc.) Preferences for CGM over POC glucose testing were observed in 4 (57%) inpatient diabetes team members for basal insulin, 6 (86%) for prandial, and 5 (71%) for correctional insulin titration. The remaining inpatient diabetes team members found CGM and POC equally effective in titrating basal, prandial, and correctional insulin, with no one favoring POC over CGM.
Five inpatient diabetes team members (71%) found hypo- and hyperglycemia alarms helpful in managing glucose levels, and 6 (86%) agreed that CGM data provided better insights into glucose patterns, influencing insulin titration and clinical planning. All inpatient diabetes team members reported feeling more confident initiating prandial insulin for patients monitored with CGM than POC glucose testing.
Discussion
In this study, we aimed to evaluate the Olsen et al CGM-based insulin titration protocol for inpatients with type 2 diabetes in non-ICU settings. Adherence to the protocol (Table 1) was consistently high (around 90%), reflecting strong alignment between the recommendations of the CGM-based protocol and the clinical judgment of inpatient diabetes teams regarding insulin titration. The protocol was well-received, deemed easy to implement, and preferred by inpatient diabetes teams who appreciated having a structured approach for CGM-based insulin titration.
There was no significant change over time in the degree to which the protocol was followed or overridden by clinical decisions for basal, prandial, or correctional insulins. This consistency indicates the protocol’s robustness and reliability, as it remained a trusted tool throughout the testing period of 353 days, even as the inpatient diabetes teams gained greater familiarity and expertise with CGM-based insulin titration and glucose management. No significant differences in glycemic outcomes were observed when comparing periods of protocol adherence to nonadherence, suggesting that minor deviations from the protocol (approximately 2 U/day for basal insulin and 1-2 U per meal for bolus/prandial insulin) did not result in harm. However, a CGM-based protocol for inpatient insulin titration may still be essential for optimizing the overall effectiveness of inpatient CGM. 19
The DIATEC trial is currently the only trial showing clinically significant glycemic and clinical benefits of CGM over POC in inpatient non-ICU settings, which may be attributed mainly to the CGM-based insulin titration protocol by Olsen et al 20 The findings from the present analysis highlight the critical importance of an operational CGM-based insulin titration protocol if CGM in an inpatient setting is to have clinical and glycemic benefits compared with standard-of-care POC glucose testing.
In other published CGM-based insulin titration protocols in non-ICU settings,14,24-30 the Olsen et al 18 protocol stands out as being the only protocol making rules for how to act when glucose levels were both below, within, and above the target range in a single titration period, such as overnight for basal insulin titration by defining the “rule of lowest” and “rule of the extreme.” This may significantly guide decision-making, as healthcare providers otherwise may be unsure whether to decrease, maintain, or increase insulin, respectively.
The Olsen et al protocol also has a potential advantage in incorporating percentage-based thresholds for time spent within specific glycemic ranges before insulin titration is adjusted. This contrasts with the traditional 1-dimensional approach in other protocols,14,24,29-31 which rely solely on glucose level cutoffs (eg, “if fasting glucose is 10.1-15.0 mmol/L, increase basal insulin by 20%”). Instead, the Olsen et al protocol adopts a 2-dimensional approach that considers both glucose levels and the percentage of time spent within these ranges (eg, “if fasting glucose is 10.1-15.0 mmol/L for ≥10% of readings, increase basal insulin by 20%”). The latter approach most likely enables more standardized insulin titration by viewing CGM data as time series data and not dichotomous data.
Strengths, Limitations, and Future Directions
We evaluated a CGM-based insulin titration protocol in a 2-center randomized controlled trial setup in different inpatient medical and orthopaedic settings, increasing the external validity of our findings.
Our study has limitations, including a lack of recruitment of patients receiving nutritional therapies or glucocorticoids during hospitalization, all populations which might be at great risk of developing dysglycemia during hospitalization 32 and, therefore, could have altered the adherence to a fixed CGM-based insulin titration algorithm. Additionally, the mean (SD) age of participants, 76.1 (9.8) years, may limit the generalizability of these findings to younger hospitalized patients with diabetes. Also, the acceptability of the proposed CGM-based insulin titration protocol should be evaluated in other settings and by more inpatient diabetes teams.
Conclusion
The Olsen et al 18 CGM-based insulin titration protocol has been successfully evaluated for titration of basal, prandial, and correctional insulin for inpatients with type 2 diabetes in non-ICU settings. The protocol was highly accepted by inpatient diabetes teams and offers a framework for effectively implementing CGMs in non-ICU inpatient settings, leading to significant clinical and glycemic improvements in outcomes compared with POC glucose testing.
Footnotes
Abbreviations
BMI, body mass index; CGM, continuous glucose monitoring; DIATEC, DIAbetes TEam and Cgm; eGFR, estimated glomerular filtration rate; GIK, glucose-insulin-potassium; ICU, intensive care unit; IQR, inter quartile range; POC, point-of-care; SD, standard deviation.
Author Contributions
MTO conceptualized, designed, and conducted the DIATEC trial with assistance from UPB, CKK, BL, JAA, HG, SL, KBH, and PLK. SHJ and LMT assisted in data collection. MTO drafted the first version of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JAA: Has received speakers fees from Juzo, Mediq, KCI, and AstraZeneca. UPB: Has received speakers fees from Sanofi and Novo Nordisk and has served on advisory boards for Sanofi, Novo Nordisk, and Vertex. Additional authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Novo Nordisk Foundation (grant no. NNF20SA0062872), Vissing Fonden, Jascha Fonden, Copenhagen University Hospital North Zealand Research Grant, Fru Olga Bryde Nielsen Fonden, PhD-START- puljen North Zealand Hospital, A.P. Møller Fonden til Lægevidenskabens Fremme, A & J C Tvergaards Fond, Læge Inger Goldmanns Fond, Ellen Margrethe Cramers Fond, and Torben og Alice Frimodts Fond.
Availability of Data and Materials
The data sets generated and/or analyzed during the DIATEC trial are available from the corresponding author upon reasonable request.