
Abstract
Background:
Few studies have examined the use of continuous glucose monitoring (CGM) devices in the general wards. The aim of this pilot study was to examine whether CGM readings can be successfully transmitted from the bedside to a central monitoring device in the nursing station, and whether a glucose telemetry system can prevent hypoglycemic events.
Methods:
We present pilot data on 5 consecutive insulin treated general medicine patients with type 2 diabetes (T2DM) whose glucose values were observed with CGM (DEXCOM) and the results were transmitted to a central nursing station monitoring system using DEXCOM Follow and Share 2 software. CGM alarms were set-up at glucose <85 mg/dl.
Results:
Duration of CGM observation was 4.0 ± 1.6 days (mean ± SD). During CGM, the overall time spent within blood glucose (BG) target of 70-179 mg/dl was 64.68 ± 15% (mean ± SD), on hypoglycemia (<70 mg/dl) was 0.30% ± 0.39, and time spent on hyperglycemia (≥180 mg/dl) was 35.02% ± 15.5. Two patients had 3 actions of prevention of potential hypoglycemia (CGM BG <70 mg/dl for >20 minutes) captured by alarm. No patients had CGM glucose value <54 mg/dl.
Conclusions:
This pilot study indicates that the use of CGM values in hospitalized patients can be successfully transmitted to a monitoring device in the nursing station, improving patient surveillance in insulin treated patients with diabetes.
More than 25% of the patients admitted in the general wards/non–intensive care unit (non-ICU) setting have history of diabetes mellitus (DM). 1 Inpatient hyperglycemia is associated with prolonged length of stay, increased mortality and increased incidence of infections.1-6 While hyperglycemia has known deleterious effects, profound hypoglycemia can cause neurological damage, 7 as well as induce fatal arrhythmias in patients with preexisting coronary artery disease.8,9 Hypoglycemia in the inpatient setting is common with reported prevalence rates among medical and surgical patients as high as 30%.10-14 Hypoglycemic events in the hospital have been associated with adverse outcomes such as increased mortality and prolonged length of stay. 15
Medical centers have implemented protocols designed to prevent and treat inpatient hypoglycemia and its potentially serious complications. 16 Existing hypoglycemia protocols for the general wards are however limited by the infrequency of point-of-care (POC) capillary glucose testing leading to gaps where low glucose values may be undetected/undocumented.
Several studies have evaluated the use of continuous glucose monitoring (CGM) devices among hospitalized patients with DM. 17 The majority of these studies have been conducted in the intensive care unit (ICU) setting and only a few have examined the use of CGM devices in patients with DM in the non-ICU setting.17-19 Previous inpatient studies conducted in the general wards reported that CGM devices detected more hypoglycemic episodes than POC capillary glucose testing.17,18,20,21 Despite providing a better assessment of glycemic control, the use of CGM has not been widely adopted as prospective studies using real-time glucose monitoring are currently lacking. Previous studies have been conducted in the general wards using “blinded” CGM and therefore interventions to prevent impending hypoglycemia were not performed.17,18,20,21 Another major limitation of CGM technology is that glucose values are captured in the CGM device and not transmitted to the nursing station to allow nursing staff and providers to detect and prevent hypoglycemia. Even with un-blinded/real time CGM use, hypoglycemia alarms are only visible and audible at bedside and as a result nurses need to frequently enter the patient’s room to monitor glucose values on the CGM receiver. Without this information being readily available to nursing staff in a centralized location, CGM technology is likely not a practical or efficient way to monitor a large number of hospitalized patients with diabetes.
We previously reported the first case of un-blinded, real-time CGM (RT-CGM) in general wards. 22 In that case report, we used a DEXCOM CGM G4 device, which was placed next to the patient’s bedside. We have further examined ways by which CGM glucose values could successfully be transmitted to a monitoring device in the nursing station. This novel system would be like a “cardiac telemetry” and could potentially prevent hypoglycemia without increasing significantly nursing work load.
In this pilot report we describe the feasibility of a glucose telemetry system (GTS), which may facilitate glucose monitoring of patients at high risk for hypoglycemia in general medicine services.
Methods
We recruited adult patients (>18 years old) with type 2 diabetes mellitus (T2DM) at higher risk for hypoglycemia, who were admitted to general medicine service at the Baltimore Veterans Affairs Medical Center (BVAMC) and who were expected to stay in the hospital for longer than 2 days. Patients were considered to be at higher risk for hypoglycemia if they had 1 or more of the following risk factors of hypoglycemia:23-26 outpatient insulin use > 0.6 u/kg/day, age ≥ 67, body mass index (BMI) ≤ 27, chronic kidney disease (serum creatinine > 2 mg/dl), history of liver failure, active malignancy, congestive heart failure, cerebrovascular event, or sepsis. The ethics committees of the University of Maryland and BVAMC approved the study protocol.
The GTS is described in Figure 1. After informed consent was obtained, a DEXCOM G4 CGM (DEXCOM, San Diego, CA, USA) sensor and transmitter were placed within 24 hours of hospital admission. Through use of Bluetooth technology and the DEXCOM Share2 application (DEXCOM, San Diego, CA, USA) glucose values were sent from the RT-CGM to an Apple iPhone located in the patient’s room which served as an intermittent transmitting (routing) device. Using a commercially available wireless internet network (Verizon) and the DEXCOM Follow application (DEXCOM, San Diego, CA, USA) glucose values from the iPhone were then transmitted wirelessly to the iPad located centrally at the nursing station on the same floor.
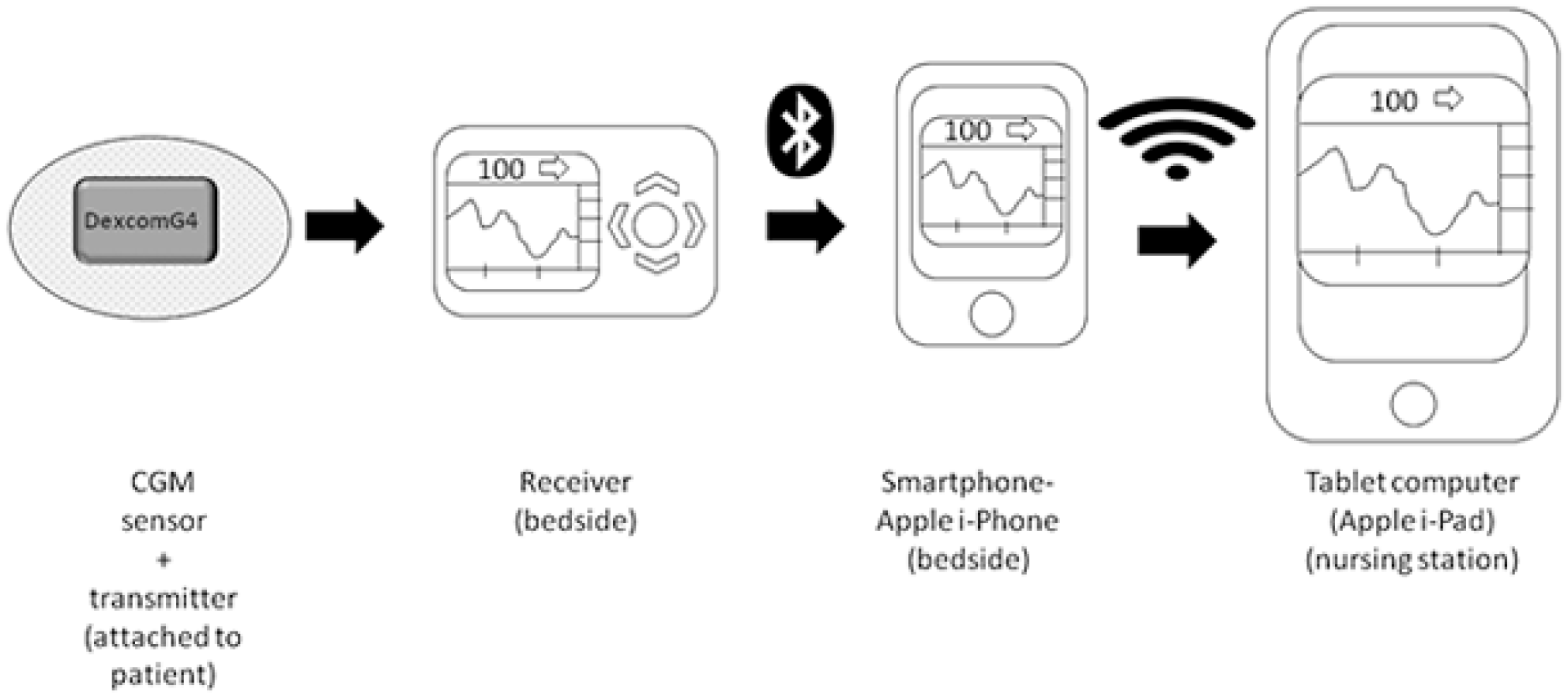
Description of glucose telemetry system (GTS).
All participants were managed with a basal-bolus insulin regimen with glargine (Lantus, Sanofi Aventis, Gentilly, France) once daily and aspart (Novolog, Novo Nordisk, Bagsvaerd, Denmark) before meals. Initiation and titration of basal and bolus insulin was based on previously published studies. 27 Nurses were educated daily about the features of the GTS and trained to calibrate the CGM devices as well as when and how to remove the CGM sensors and transmitters (if required). Low alarm threshold was set on the iPad at glucose value < 85 mg/dl, resulting in an audible alarm from the central iPad device. As the Follow application provides the opportunity to choose an alarm from many different types, we allowed the nursing staff to select which type of alarm would like to use. By placing the iPad on a central location at the nursing station, even nursing staff that were not involved in the care of the study participants were able to notify the assigned nurse, when the alarm activated. Nurses were instructed to perform a POC capillary glucose testing to confirm hypoglycemia and to provide at least 10 grams of carbohydrates to the patient when CGM alarmed a glucose value <85 mg/dl, as a preventive action of hypoglycemia.
The primary outcomes of interest were number of hypoglycemic episodes, hypoglycemic event rate (defined as hypoglycemic episodes/per patient-per days under CGM) and time spent in hypoglycemia. Hypoglycemic episodes, clinically significant hypoglycemic episodes and severe hypoglycemic episodes were defined as glucose concentrations detected by CGM <70 mg/dl, <54 mg/dl and <40 mg/dl, respectively, for at least 20 minutes.6,28
Results
In this pilot study we describe our experience with 5 insulin treated patients with T2DM, whose glucoses were monitored by the GTS. Table 1 summarizes baseline characteristics, of the participants and outcomes of interest. Overall participants were elderly with an average age of 70.8 ± 6.2 (mean ± SD), BMI: 33.1 ± 9.3 kg/m2, with duration of T2DM of 22 ± 12.9 years, and with multiple DM complications.
Baseline Characteristics and Glycemic Values Based on CGM Measurements (N = 5).
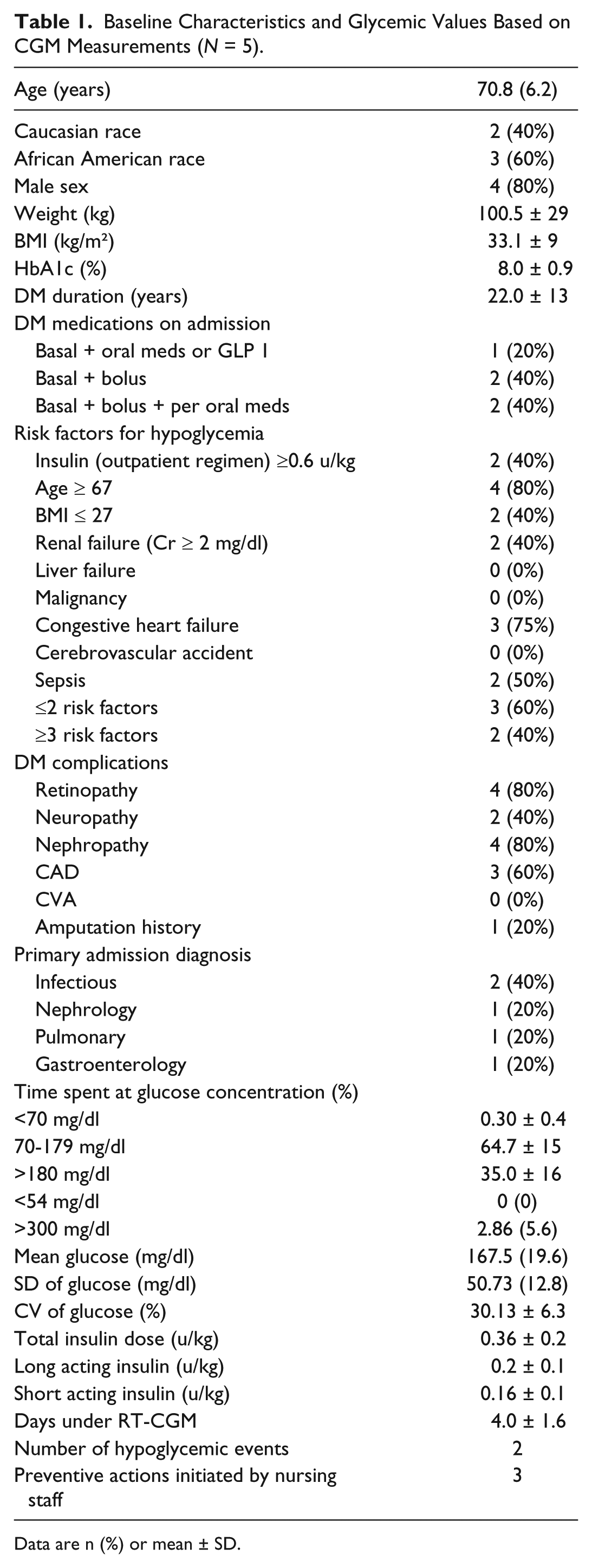
Data are n (%) or mean ± SD.
Two different patients had a total of 3 alarm events (Table 1), when CGM glucose values were <85 mg/dl. In each case, nursing staff provided treatment per the hypoglycemia prevention protocol and were successful in preventing hypoglycemia <70 mg/dl. Both patients received oral carbohydrates as per protocol. In one patient who had 2 episodes, CGM readings revealed decreasing glucose levels for a total 30 minutes reaching a nadir of 71 mg/dL, before eventually increasing after treatment. In both occasions POC capillary blood glucose revealed blood glucose of 75 mg/dl and 83 mg/dl. The second subject had 1 episode of glucose value was 83 mg/dl at 00:38
Two patients experienced a single hypoglycemic event despite GTS monitoring (Table 1). The first episode occurred after a patient received prandial insulin and was transferred to radiology for an imaging study interrupting his meal. Duration of hypoglycemia was 25 min, which included the time when the patient became hypoglycemic, time until he received treatment and the time until hypoglycemia resolved. Glucose values from CGM were found to be as low as 68 mg/dl (POC capillary glucose testing was 63 mg/dl at that the same time). The second case occurred post dinner due to decreased appetite and poor nutritional intake. Hypoglycemia alarm went off, however nursing staff failed to act, as she was involved in the management of another patient that required emergency treatment. In this case the patient was hypoglycemic for 50 minutes. CGM recorded glucose values as low as 56 mg/dL with a POC capillary blood glucose value of 55 mg/dL, which was checked at that time. The overall hypoglycemia event rate was 0.1 events per patient-per days under CGM. Neither of the participants experienced clinically significant hypoglycemic or severe hypoglycemic episodes. Overall time spent in hypoglycemia <70 mg/dl was 0.30% ± 0.39, time spent within BG target of 70-179 mg/dl was 64.68% ± 15.39, and time spent in hyperglycemia ≥180 mg/dl or and ≥300 mg/dl was 35.02% ± 15.5 and 2.86% ± 5.6, respectively. There were no CGM glucose value below 54 mg/dl in any of the participants. Average glucose and coefficient of variation (CV) were 167.5 ± 19.6 mg/dl and 30.13% ± 6.26, respectively.
Two patients required more than 1 sensor during their hospital stay. One of them required the sensor to be removed due to a CT scan imaging procedure—as per manufacturer recommendations—and the other patient experienced sensor failure. Overall each participant required 1 or 2 (mean 1.4) sensors during the entire hospital stay. Overall participants were monitored with CGM for an average of 4 ± 1.6 days, requiring an average total daily dose of insulin of 0.36 units/ kg ± 0.23 units/kg.
Discussion
The results of this preliminary study indicate that hospital glucose values from CGM devices can be successfully transmitted to a monitoring device located at a central nursing station. By setting the lower BG alarms at 85 mg/dl, the GTS using RT-CGM technology can detect trends in lowering glucose readings leading to preventive actions of impending hypoglycemia. The GTS overcomes some of the major limitations cited in recent clinical guidelines regarding the use of CGM in the hospital setting19,29 providing prospective real-time glucose measurements to be transmitted directly to a central nursing station and allowing interventions to prevent and treat hypoglycemia.
The proposed GTS aimed to prevent hypoglycemia in the general wards in high risk individuals. The CGM system has the potential to detect early not only hypoglycemic events as well as worsening hyperglycemia. 19 However, treating in “real time” hyperglycemic excursions in the general wards may be more complicated than the proposed hypoglycemia prevention strategy that can be easily adopted by the nursing staff. The success of the CGM systems largely depends in the correct interpretation of the data. 19 Training of the nursing staff is needed to prevent errors and wrong interpretation of glycemic trends, which may lead to frequent dosing of insulin (insulin “stacking”), leading to hypoglycemic events. 19 Our pilot study indicates that the real-time CGM system combined with a simplified hypoglycemia protocol can be easily managed by the nursing staff reducing the risk of hypoglycemia.
To our knowledge this is the first report where glucometric values were successfully conveyed to a display device at the nursing station in non-ICU settings. Our study adds to the increasing number of studies indicating the beneficial role of CGM technology in the hospital environment. 19 In the ICU setting, the Medtronic Hospital Glucose Management System (renamed Sentrino CGM) has been approved in Europe for CGM in critical care patients. 30 This wired system is limited by the fact that the display device must be placed at the bedside, which represents an important barrier and could increase nursing work load if used in non-ICU settings.
Future studies should determine the appropriate population who would benefit from inpatient CGM use. We believe that insulin-treated patients at a higher risk for hypoglycemia, either DM1 or DM2 patients, with comorbidities such as chronic kidney disease or liver failure, may benefit the most from CGM. In the general medicine and surgery wards, there is less frequent patient surveillance and glucose values are usually checked only a few times per day compared to the critical care environment where BG levels are checked even hourly, which may obviate the need for subcutaneous CGM. Previous CGM studies conducted in the non-ICU setting were retrospective and used blinded CGM technology.17,18,20,21 In these studies, CGM use was found to be superior in detecting hypoglycemia compared to POC capillary blood glucose testing. In addition, the proposed GTS allows not only detecting patients at risk of hypoglycemia but also the opportunity to intervene early detecting trends in low glucose readings, which may prevent clinically significant hypoglycemia. Furthermore, the GTS allows providers to modify the lower glucose alarms, choosing higher hypoglycemic prevention alarms (90 mg/dl or 100 mg/dl), which may be appropriate in patients with DM who are at greater risk for hypoglycemia or who have rapidly decreasing glucose values.
We report, that despite CGM system, some patients experienced hypoglycemia. This emphasizes the need of nursing education and the challenges that patients with diabetes experience in the inpatient setting. We have initiated a randomized clinical study (NCT02904512) aiming to compare the benefits in assessing glycemic control and in preventing hypoglycemia between real time CGM technology in general medicine services. This study will assess whether the GTS using a simplified hypoglycemia protocol will prevent the number of hypoglycemic episodes and its complications compared to current standard of care using POC glucose testing.
Conclusions
We report the development of a GTS, as a feasible means of glucose monitoring in the general wards. We believe that our initial experience shows the potential of future wider use of CGM in hospitalized patients at high risk for hypoglycemia.
Footnotes
Abbreviations
BG, blood glucose; BMI, body mass index; BVAMC, Baltimore Veterans Affairs Medical Center; CGM, continuous glucose monitoring; CV, coefficient of variation; DM, diabetes mellitus; GLP 1, glucagon-like peptide-1; GTS, glucose telemetry system; ICU, intensive care unit; POC, point of care; RT-CGM, real-time CGM; SD, standard deviation; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EKS has received research support (CGM supplies) that were needed for the conduction of the study. JS was supported by P30AG028747, P30DK072488, and by the Baltimore Geriatrics Research, Education and Clinical Center. GEU is partly supported by research grants Public Health Service Grant UL1 RR025008 from the Clinical and Translational Science Award program, and 1P30DK111024-01 from the National Institutes of Health and National Center for Research Resources. GEU has received unrestricted research support for inpatient studies (to Emory University) from Merck, Novo Nordisk, AstraZeneca, Boehringer Ingelheim, and Sanofi. JCF is partially supported by research grants from the National Institutes of Health: R34DK102177-01, R01 HL127422, and R18 DK110955.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DEXCOM provided the necessary CGM supplies for the conduction of the study.