
Abstract

Keywords
Hospital hyperglycemia (HH), defined as blood glucose (BG) levels above 140 mg/dL, is associated with increased morbidity and mortality, regardless of diabetes status. 1 Despite clear guidelines, glycemic management in hospitals remains a challenge due to the complexity of insulin regimens and the limited availability of specialists. 2 Addressing these barriers, we investigated the efficacy and safety of InsulinAPP (http://www.insulinapp.com.br), 3 an electronic glycemic management system (eGMS) designed to assist nonspecialist physicians in managing inpatient insulin therapy.
In our randomized, single-center trial conducted at Hospital Santa Izabel in Salvador, Brazil, we enrolled 75 hospitalized patients with diabetes or stress hyperglycemia. Patients were randomly assigned to the InsulinAPP group, where nonendocrinologists used the app to guide insulin dose adjustments, or the InsulinHAB group, where endocrinologists followed standard insulin protocols. The primary endpoints included BG control, hypoglycemia rates, and insulin regimen selection.
Our findings demonstrated that InsulinAPP is both effective and safe, achieving glycemic control comparable to endocrinologist-directed therapy. Mean BG reductions from admission to discharge were 26.6 ± 47.4 mg/dL in the InsulinAPP group and 19.1 ± 45.9 mg/dL in the InsulinHAB group (P = .54). Notably, hypoglycemia events were rare in both groups, with no significant differences in episodes of BG <70 mg/dL (InsulinAPP 1.4% vs InsulinHAB 1.9%, P = .53). In addition, the InsulinAPP group achieved these outcomes with fewer BG measurements per patient-day compared with the InsulinHAB group (1.8 vs 2.7, P = .01) (Table 1), suggesting that the app’s structured guidance optimized monitoring efforts.
Baseline Demographic Data and Postrandomized Glycemic Control and Insulin Therapy Details.
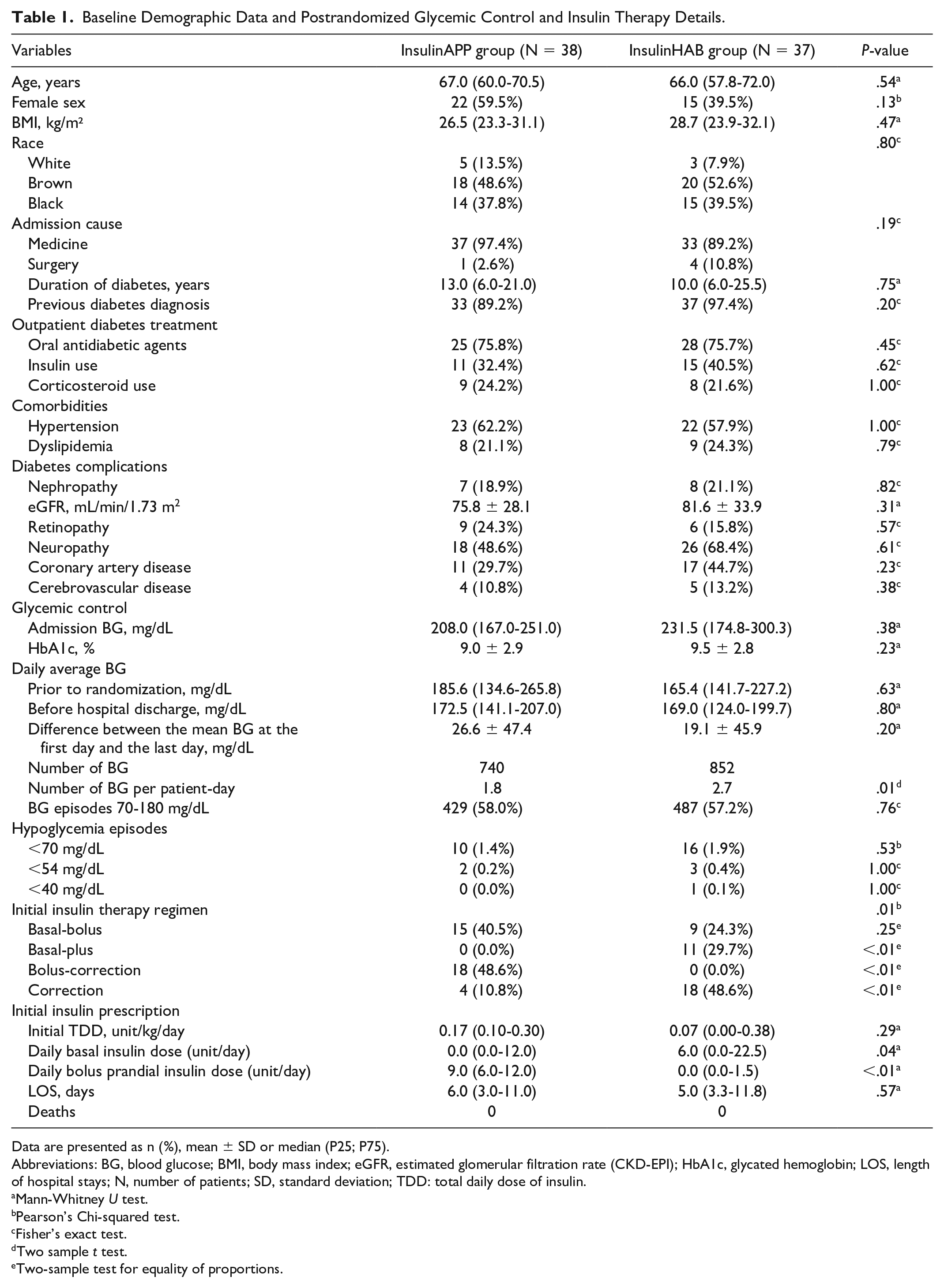
Data are presented as n (%), mean ± SD or median (P25; P75).
Abbreviations: BG, blood glucose; BMI, body mass index; eGFR, estimated glomerular filtration rate (CKD-EPI); HbA1c, glycated hemoglobin; LOS, length of hospital stays; N, number of patients; SD, standard deviation; TDD: total daily dose of insulin.
Mann-Whitney U test.
Pearson’s Chi-squared test.
Fisher’s exact test.
Two sample t test.
Two-sample test for equality of proportions.
Insulin regimen patterns differed between the groups. The InsulinAPP group primarily utilized bolus-correction regimens 3 (48.6%), while the InsulinHAB group predominantly followed basal-plus protocols 4 (29.7%, P < .01). Despite these differences, both groups achieved similar percentages of BG episodes within the target range of 70 to 180 mg/dL (P = .76) (Table 1), suggesting that InsulinAPP provides a viable alternative for managing HH.
Our findings align with previous studies demonstrating the potential of eGMS in improving glycemic outcomes. A recent study with InsulinAPP in a surgical ward showed enhanced glycemic control and reduced complications.5,6 Collectively, these results underscore the promise of technology in addressing the global shortage of endocrinologists by enabling nonspecialist physicians to deliver safe, effective insulin therapy.
While the study was limited to a single center, our results provide strong evidence supporting the broader implementation of InsulinAPP in hospital settings. Future research should explore its integration with electronic health record systems, its performance in diverse patient populations, and its long-term impact on clinical outcomes and resource utilization.
In conclusion, InsulinAPP represents a significant advancement in glycemic management, offering a scalable solution to improve inpatient diabetes care. We believe that our findings will contribute to advancing knowledge and practice in this critical area.
Footnotes
Acknowledgements
None.
Abbreviations
HH, hospital hyperglycemia; eGMS, electronic glycemic management; BG, blood glucose; BMI, body mass index; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; N, number of patients; SD, standard deviation; LOS, length of hospital stay; TDD, total daily dose of insulin.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.