
Abstract
The way diabetes patients cope with their disease in day-to-day routines is decisive for the development or the prevention of medical complications. Smartphones have created the ubiquitous environment to support health care with mobile applications (mHealth). This article comments on the publication by Offringa et al in JDST, which is one of few studies that tries to isolate the effects of a diabetes app. At the same time, it is a good example to discuss general aspects of mHealth in diabetes care. Treatment context, eHealth literacy, interoperability, and efficiency will determine the success of diabetes apps. The development has not yet reached its end. A triple quality feedback loop linking persons with diabetes, health care providers, and mHealth providers is suggested.
In chronic diseases such as diabetes mellitus patients are on their own most of the time. In the long run, self-management determines the individual fate of the persons with diabetes. The widespread use of smartphones has created the ubiquitous environment to support health care with mobile applications (apps). This has led to the development of a vast number of mobile software intended to support diabetic persons and physicians as well. Oftentimes, this has been referred to as mHealth. 1
The present article comments on the publication by Offringa et al published in the Journal of Diabetes Science and Technology. 2 This publication, as others before, demonstrated small but consistent improvements in glycemic control of patients with type 1 and type 2 diabetes. This is one of a few studies that isolated the effect of a diabetes app. The company behind the study seeks scientific evidence and does not advantageously select people with diabetes. This is pleasant.
At the same time, this paper is a good example and occasion to discuss general aspects of investigating the outcome of mHealth in diabetes care.
Context
Most of the mHealth approaches focus on a behavioral change in lifestyle aiming at modifiable risk factors for diabetes and its related complications. 1 Yet, persons with diabetes are already under treatment, and diabetes apps come on top of it, resulting in small achievable deltas for health gains. Chain smokers with diabetes might gain much greater life expectancy from a smoking cessation app than from a diabetes app. 3 For others, this will be a sleep awareness app, 4 and so on. Finding the right patient for the right app is essential. A healthier lifestyle is not restricted to apps or to better diabetes management, 5 but most likely will affect the success of any diabetes treatment. In such a situation, it is hardly possible to control confounders in cross-sectional or retrospective analyses, a fact that was mentioned and discussed by Offringa et al.
In this context, significance must not be mixed with clinical relevance. In general, we see stunning P values in studies analyzing glucose levels. This is easily explained by a large number of data points distributed on a ratio scale.
The bundling of measures hampers the attribution of success. A glucose management app that provides also nutritional advice makes it impossible to say what of the both parts is the more effective intervention. This is not a problem in this case. The goal is not to evaluate a cause-effect relation, but to maximize health outcome for persons with diabetes. It is righteous to apply proven principles and to combine them to maximize effects.
eHealth Literacy
Also in this study, app users are younger than nonusers, and experience from earlier trials shows that oftentimes this fact results in cohorts that are hardly comparable. One of the most important underlying causes is missing eHealth literacy that leads people not to use software or to use it in an inefficient way. 6 In many mHealth publications, also in the Offringa et al study, infrequent users are excluded from the studies. Nielsen has pointed out that the acceptance and use of software depends on an interactive interface that follows basic principles: 7
Visibility of system status
Match between system and the real world
User control and freedom
Consistency and standards
Error prevention
Recognition rather than recall
Flexibility and efficiency of use
Aesthetic and minimalist design
Help users recognize, diagnose, and recover from errors
Help and documentation
Unfortunately, there is no standard for publishing apps. When it comes to supporting self-management, these aspects could be helpful.
Economic Aspects
From an economic perspective mHealth represents a disruptive innovation because new markets are being created. From a medical view-point the diabetes situation is not that clear. Small improvements in reducing glucose and HbA1c levels have been demonstrated so far, 8 but to date the cause-effect relation of apps on the development of long-term outcomes is subject to ongoing assessment. 9
If patients exhibit poor treatment results, treatment intensification such as increasing insulin dosage or adding other medication is recommended. This will increase the treatment costs, but with a reasonable prospect of preventing costly late outcomes. Higher SMBG test rates and lacking cost-relevant outputs leave room for skepticism. Apart from HbA1c as the central surrogate indicator for improved diabetes care, it is prevented hypoglycemia that could be economically attractive in persons with type 1 diabetes. The economic perspective should be extended to the societal interests because health care payers in most cases do not consider loss in productivity due to diabetes or the value of the ability to work as such. 10
Interoperability
Most app based empowerment strategies fail when it comes to the showcase field of computer sciences: IT system integration. Double documentation hampers adherence and leads to decreasing quality of data over time.
Personalized diabetes management (PDM) has shown effectiveness in self-management of blood glucose values, for instance in the STeP trial or in the ProValue study program.11,12 PDM always uses software, one more clue that health care provider feedback and supporting professionals as well as integration into existing ICT environments are essential for designing successful apps. 13
PDM focuses on the establishment of structured communication between patients and doctors in a quality feedback loop that in the latter comprises
Structured education/selection of structured SMBG regimen
Initiate structured SMBG: the patient will perform his or her structured SBMG regimen as instructed
Data upload/documentation
Data analysis: diabetologists will review the data
Personalized treatment: individual treatment plan
Treatment efficacy assessment
Triple Feedback Loop
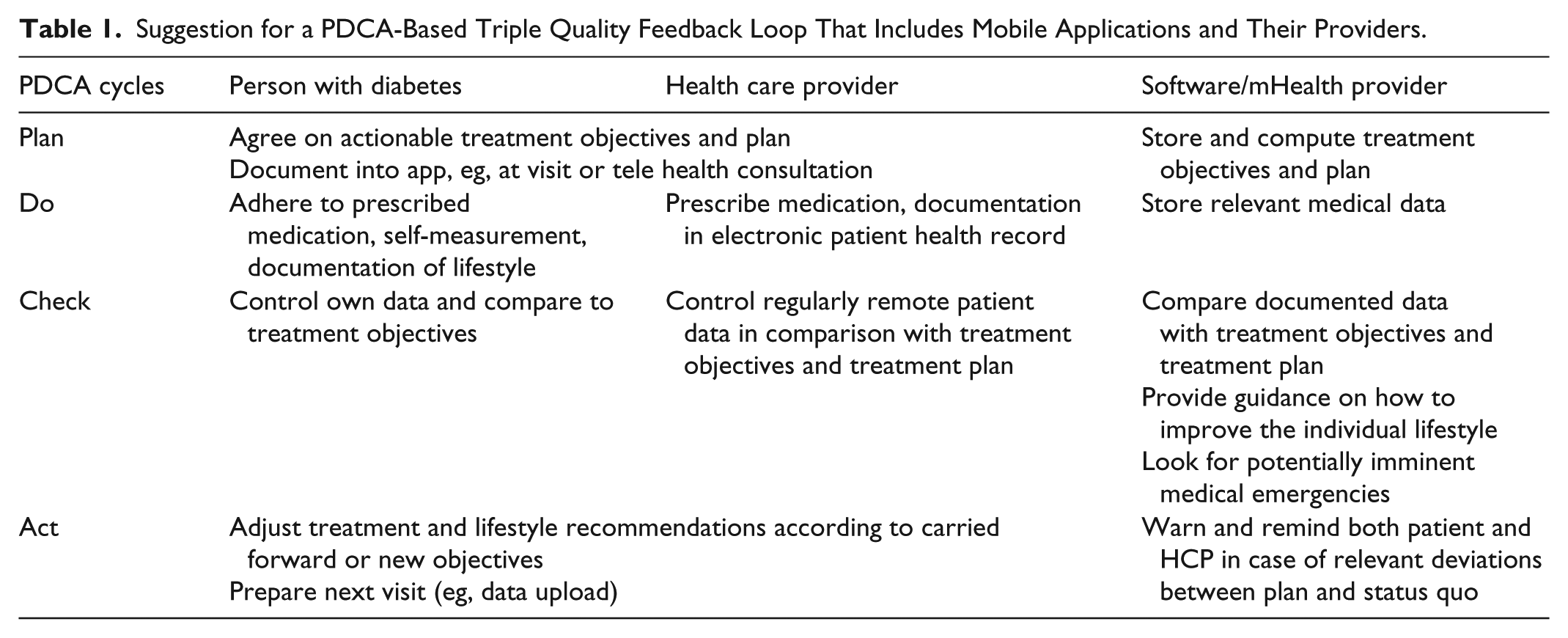
When generalizing this principle of therapeutic advancement by continuously circling medical quality assurance, 14 it appears logical to speak of a triple quality feedback loop. A successful software should accompany the change in treatments over a patient career, and therefore should be able to adapt and develop. Table 1 illustrates what a PDCA circle that integrates the three players could look like.
Suggestion for a PDCA-Based Triple Quality Feedback Loop That Includes Mobile Applications and Their Providers.
Additional success factors are adherence to evidence-based treatment guidelines, external quality management, and the reliability of the care process as such.
Conclusion
Much is to be learned about the influence of mHealth on diabetes-related outcomes. Possibly the ideal treatment setting is still to be found. Doctors, persons with diabetes, and mHealth providers should team up to design even more successful diabetes apps, so to write their joint trilateral serial.
Footnotes
Abbreviations
App, mobile application; ePHR, electronic patient health record; HCP, health care provider; IT, information technology; mHealth, health support by mobile apps; PDM, personalized diabetes management; SMBG, self-measurement of blood glucose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.