
Abstract
Background:
Pandemic circumstances created challenges for doctor of physical therapy (DPT) students to understand social determinants of health (SDH) in clinical rotations. Instead of canceling clinical rotations, a virtual reality cinema (cine-VR) education series was implemented. The purpose of this project is to describe the effect of this simulated immersion on student empathy and attitudes toward diabetes.
Method:
The DPT students (n=59) participated in 12 cine-VR education modules, completing surveys at three time points as part of coursework. The students completed baseline measures of the Diabetes Attitude Scale–Version 3 (DAS-3) and Jefferson Empathy Scale (JES), and then were immersed in 12 cine-VR modules. One week after module completion, students participated in a class discussion about the modules. The students repeated the JES and DAS-3 scales at postclass and six weeks later. Three subscales from the Presence Questionnaire (PQ) were used to measure the virtual experience.
Results:
Student scores on three DAS-3 subscales significantly improved on posttest: Attitude toward patient autonomy, Mean: 0.75, SD: 0.45; t(58) = 12.742, P < .001; Psychosocial impact of diabetes, Mean: −0.21, SD: 0.41; t(58) = −3.854, P < .001; and Seriousness of type 2 diabetes, Mean: −039, SD: 0.44; t(58) = −6.780, P < .001, with lower scores six weeks later. Student scores increased on the JES and remained high (P < .001). High subscale scores on the PQ demonstrated immersion and involvement in the virtual experience.
Discussion:
These modules can allow for a shared student experience that improves diabetes attitudes, increases empathy, and fosters meaningful classroom discussion. The cine-VR experience is flexible, and modules allow students to engage in aspects of a patient’s life that were not available otherwise.
Introduction/Background
Social determinants of health (SDH) are circumstances over the life course that affect functioning and risks related to health outcomes. Disparities are associated with SDH 1 and, although health care and disease prevention strategies have improved, health disparities persist and may intensify for people with chronic conditions such as diabetes. 2 For example, people with diabetes who are experiencing food insecurity may not have healthier food options and the lack of transportation may prevent them from accessing quality health care. In a scientific review of the impact of SDH on care for the chronic condition of diabetes, interventions addressing SDH improved outcomes. 3 Interventions that addressed SDH for people with low literacy/health numeracy improved diabetes self-management for people with type 2 diabetes 3 and can improve diabetes knowledge and self-care 4 To address SDH disparities, another intervention conducted a pilot program providing healthy food, blood glucose monitoring, self-management support, and primary care referrals. Improvements in A1C, fruit and vegetable consumption, increased self-efficacy, and medication adherence were found; 5 comparable results were also found in a randomized controlled trial of the intervention. 6
Social determinants of health are aspects of the patient context that health professionals may not adequately assess during the clinical encounter, despite being essential components of a patient’s overall health status. 7 The need for improved education in SDH and humanistic aspects of health care has been identified as one of the emerging trends critical to the future of health professions education, 8 such as physical therapist practice. 7 Therefore, health professions students must recognize the importance of integrating SDH into clinical care to achieve favorable outcomes; however, simply discussing SDH may not be sufficient to foster awareness and agency.
Broadening the capacity for empathy is recognized as a mechanism to facilitate connection between students and patients. Social empathy allows “the ability to understand people by perceiving or experiencing their life situations and as a result, gaining insight into structural inequalities and disparities.”9 -11 Empathic capacity also enhances therapeutic relationships and patient outcomes 12 by viewing patients as people, not just medical conditions. 13 Amini (2021) argues that minimal understanding of the effects of SDH in dental practice may negatively impact outcomes by causing unconscious bias, and that improving empathy will provide clinicians strategies to mitigate the negative effects of SDH on health. 14 A similar argument is offered by Yeary et al 15 stating that improved empathy can overcome unconscious bias that contributes to health care disparities. Peralta et al 16 offers promising outcomes in describing the effects of an SDH curriculum on empathy levels of medical residents in pediatrics, although data remain unpublished. Because improving empathy in health professions students is challenging, and typically requires exposure to patients in clinical care environments, recent pandemic restrictions necessitated an innovative approach to simulate patient exposure for doctor of physical therapy (DPT) students in lieu of an early clinical rotation.
Wellbery asserts that educational curricula must develop new methods of engaging students in the care of vulnerable groups as the effects of SDH on health disparities and outcomes are increasingly understood. 17 Virtual reality and simulation have been effective teaching modalities to increase empathy toward older adults across several health professions programs, including physical therapy education.18,19 Specifically, virtual reality cinema (cine-VR) has been used as an innovative approach to improve diabetes attitudes among health care practitioners and administrators. 20 Virtual reality cinema provides an opportunity to interact with a patient and to observe how the environment is related to the patient’s values and health behaviors. Moreau recommends storytelling as a powerful tool to facilitate student immersion in another’s experience. 21 Digital storytelling in health professions education may facilitate development of several skills, such as (1) understanding diversity, oppression, and social justice issues; (2) conceptualizing patient-centered care; (3) caring for underserved populations; and (4) caring for those with chronic health conditions. 21 To provide DPT students a meaningful connection with a patient’s lived experience, digital storytelling was implemented using cine-VR modules as an innovative alternative to direct clinical exposure to allow students to envision the effect of SDH on health decisions, improving empathy and attitudes toward the patient experience and needs. 20 This project’s purpose is to describe the effect of the cine-VR virtual immersion on DPT students’ empathy and attitudes toward diabetes.
Methods
Overview
This project received exempt approval from the academic institution’s institutional review board (IRB). A mixed-methods convergence design with qualitative data interpreting the quantitative findings was employed.
Recruitment
Students were recruited from a second semester DPT course, Psychosocial Aspects of Healthcare, designed to provide foundational knowledge and application of the behavioral sciences to clinical practice. Students develop professional identity and role with others to enhance interactions with patients/clients, family, caregivers, and providers. Students also engage in self-assessment and exploration of personal beliefs, biases, and judgments related to human interactions required of a health care professional, identifying critical issues influencing health beliefs and behaviors in the larger contextual framework of practice including SDH.
Students were sent surveys at three time points: baseline, post assessment, and six-weeks after the postsurvey. The first survey asked for permission to use their responses for our study and all students agreed.
Power Analysis
An a priori power analysis using Statulator, 22 an online statistical calculator, estimated need for a total sample size of 34 participants to achieve 80% power at a 5% significance level (P < .05) and to detect an effect size of 0.5 between two pairs.
Cinematic 360° Virtual Reality Simulations
The simulated patient encounter utilized a professionally produced, 360°, virtual reality cinematic (cine-VR) video designed to educate students about diabetes and SDH. Students viewed 12 cine-VR, such as 360° audio and visual simulations, giving the viewer a sense of physical presence in the space, observing interactions between the main character and their primary care physician, pharmacist, family, and community. The cine-VR simulations are described in detail elsewhere.20,23 The main character is Lula Mae, a 72-year-old woman with type-2 diabetes experiencing the negative effects of SDH on health care access and decisions. Lula Mae is a primary source of support for her extended family; therefore, her own health care needs are deferred to meet the daily needs of the people she loves. Strong subthemes include provider burnout, challenges with managing the health care system, and the importance of compassion in health care. Especially pertinent to DPT students are vignettes that highlight fall risks in the home and a developing foot ulcer, coupled with Lula Mae’s hesitancy to consult her physician.
Measures
Quantitative measures were administered at three time points: baseline, post-cine-VR intervention, and 6 weeks after the initial postassessment.
Diabetes Attitude Scale–Version 3
The Diabetes Attitude Scale–Version 3 (DAS-3) 24 is a 33-item scale that measures diabetes-related attitudes with five discrete subscales: (1) Need for special training (Cronbach’s α=.67), (2) Seriousness of type 2 diabetes (Cronbach’s α=.80), (3) Value of tight glucose control (Cronbach’s α=.72), (4) Psychosocial impact of diabetes (Cronbach’s α=.65), and (5) Attitude toward patient autonomy (Cronbach’s α=.76). Health care professionals are asked to rate their level of agreement on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The scale demonstrates good internal consistency and high content validity. 24 Sample statements include the following: “People who do not need to take insulin to treat their diabetes have a pretty mild disease”; “Diabetes affects almost every part of a diabetic person’s life”; and “Tight control is too much work.”
Jefferson Empathy Scale
The Jefferson Empathy Scale (JES) is a valid scale used to measure empathy in health professions education. Empathy is conceptualized as “A cognitive (as opposed to affective) attribute that involves an understanding of the inner experiences and perspectives of the patient, combined with a capability to communicate this understanding to the patient.”25,26 Sample questions include the following: “I try to think like my patients to render better care” and “Empathy is a therapeutic skill without which success in treatment is limited.”
Presence Questionnaire
The 32-item Presence Questionnaire (PQ) 27 was used at postassessment and measures the subjective experience of being in a virtual environment when a person is physically situated in another. It uses a seven-point scale, ranging from 1 (not at all) to 4 to 7 (completely). We used a subset of 15 questions from the questionnaire (Cronbach’s α=.88) and calculated our own internal consistency for each subscale using a reliability analysis. There were three subscales: (1) Involvement, (2) Sensory Fidelity, and (3) Adaptation and Immersion. Involvement measured the participants’ sense of being a part of the environment (Cronbach’s α=.81). Sample questions included the following: “How natural did your interactions with the environment seem?” and “How much did your experiences in the virtual environment seem consistent with your real-world experiences?” Sensory Fidelity measured how well the participant perceived a sensory experience (Cronbach’s α=.72). Sample questions included the following: “How well could you identify sounds?” and “How closely were you able to examine objects?” Adaptation and Immersion measured how well the participant adapted to the immersive environment (Cronbach’s α=.77). Sample questions included the following: “How quickly did you adjust to the virtual environment experience?” and “Was the information provided through different senses in the virtual environment (eg, vision, hearing) consistent?”
Data Collection
The DPT students completed baseline assessments prefaced with informed consent prior to viewing the 12 modules introducing them to their patient, Lula Mae. Baseline assessment included demographic questions, the DAS-3, and the JES. The students viewed all modules, which were 12 individual video lessons, taking about 70 minutes to view. During a subsequent class, students were given time to reflect upon the cine-VR using a clinical narrative process. 28 Students were provided with the link to the post assessments for the three scales, including their identifier, to ensure proper matching. Six weeks after post assessment, students were emailed the final assessment.
Classroom Debriefing
Classroom discussion occurred one week after the reflection exercise and initial post assessment. Discussion was facilitated by the instructor and recorded using Zoom conferencing. Semistructured questions were used to prompt discussion, such as understanding personal stressors for Lula Mae, food insecurity, transportation challenges, paying for prescription medication, understanding and navigating the broader health care system, provider burnout, and comorbidities associated with diabetes. This convenience sample included all students who chose to take part in the discussion.
Data Analysis
Quantitative data
Statistical analyses were completed using SPSS Version 27.0. 29 Baseline and post assessment data were matched using student identifiers. Paired t tests were conducted to determine differences in scales and subscales from baseline to post assessment scores. Repeated measures analysis of variance (ANOVA) determined differences among baseline, post assessment, and six-week assessment data.
Qualitative data
Recorded narrative data were transcribed verbatim, yielding low-inference data. Additional standards of verification were employed to enhance the study’s methodologic rigor. 30 Two coders triangulated data sources during the open coding phase, assisted by use of the software program MAXQDA Version 20.1.1. 31 During this process, a project team member who was involved in development of the virtual modules (E.B.) and a project investigator (J.W.) reviewed all transcripts and coded independently. Investigators then examined, compared, expanded, or condensed all codes until saturation was reached and themes were sufficiently categorized. When discrepancies were found, the negative cases were analyzed to determine whether additional codes were needed. Finally, rigor was enhanced by an external audit of the data analysis performed by a project investigator with expertise in qualitative methods, but who had not participated in initial phases of data reduction and analysis (T.C.). The selected quotations best represent the resultant themes from the narrative data.
Quantitative Results
Demographics
All participants were first-year DPT students. Most students were white (82.6%) and female (68.9%). Most of the students were on the urban campus in Omaha (81.5%), versus the rural campus in Kearney (18.5%). In addition, 52.5% of students indicated they had a close friend or family member with diabetes.
Baseline assessments included all 121 students from both campuses. Post assessment included 93 students (76.9% response rate), resulting in 93 matched surveys from baseline to post assessment. The 6-week post survey included 58 (47.9% response rate) matched assessments across all three time points.
Diabetes Attitude Scale–Version 3
Mean and standard deviation scores for the five DAS-3 subscales were calculated (Means are shown in Table 1). Students agreed with Need for special training (Mean: 4.65, SD: 0.32), Seriousness of type 2 diabetes (Mean: 4.04, SD: 0.49), Value of tight glucose control (Mean: 3.88, SD: 0.41), Psychosocial impact of diabetes (Mean: 4.22, SD: 0.44), and Attitude toward patient autonomy (Mean: 3.98, SD: 0.43). After viewing the 12 modules, four of the DAS-3 subscales significantly increased: Seriousness of type 2 diabetes, Mean: 4.32, SD: 0.46; t(59) = −4.936, P < .001, Value of tight glucose control, Mean: 4.01, SD: 0.48; t(59) = −2.547, P = .013, Psychosocial impact of diabetes, Mean: 4.62, SD: 0.39; t(59) = −6.807, P < .001, and Attitude toward patient autonomy, Mean: 4.22, SD: 0.36; t(59) = −5.604, P < .001. No significant change in Need for special training was observed. Results include 59 student responses matched across all three time points. Three domains significantly increased from baseline assessment at the six-week time point: Attitude toward patient autonomy, Mean: 0.75, SD: 0.45; t(58) =12.742, P < .001, Psychosocial impact of diabetes, Mean: −0.21, SD: 0.41; t(58) = −3.854, P < .001, and Seriousness of type 2 diabetes, Mean: −039, SD: 0.44; t(58)= −6.780, P < .001, indicating a sustained effect over time. However, Value of tight glucose control, Mean: 0.92, SD: 0.34; t(58) = 20.764, P < .001, significantly decreased. Need for special training, Mean: 0.05, SD: 0.36; t(58) = 1.158, I = .25, was not significantly different from baseline assessment to 6-week follow-up due to the ceiling effect.
Mean Differences in Diabetes Attitude Scale–Version 3 Subscales Premean and Postmean.
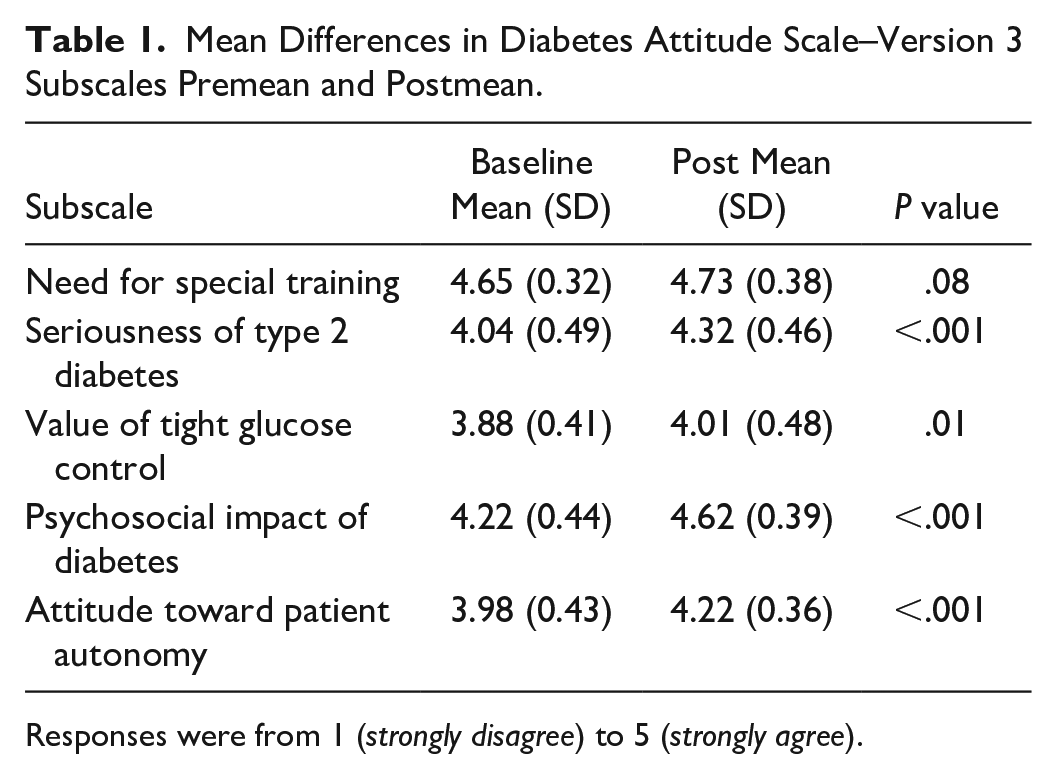
Responses were from 1 (strongly disagree) to 5 (strongly agree).
Jefferson Empathy Scale
Students scored moderately high on the JES baseline assessment (Mean: 81.87, SD: 3.93) and higher after viewing the modules, Mean: −080, SD: 4.31; t(59)= −1.437, P < .078.
Six weeks following postassessment, students received the link with the DAS-3 (Figure 1) and JES (Figure 2).
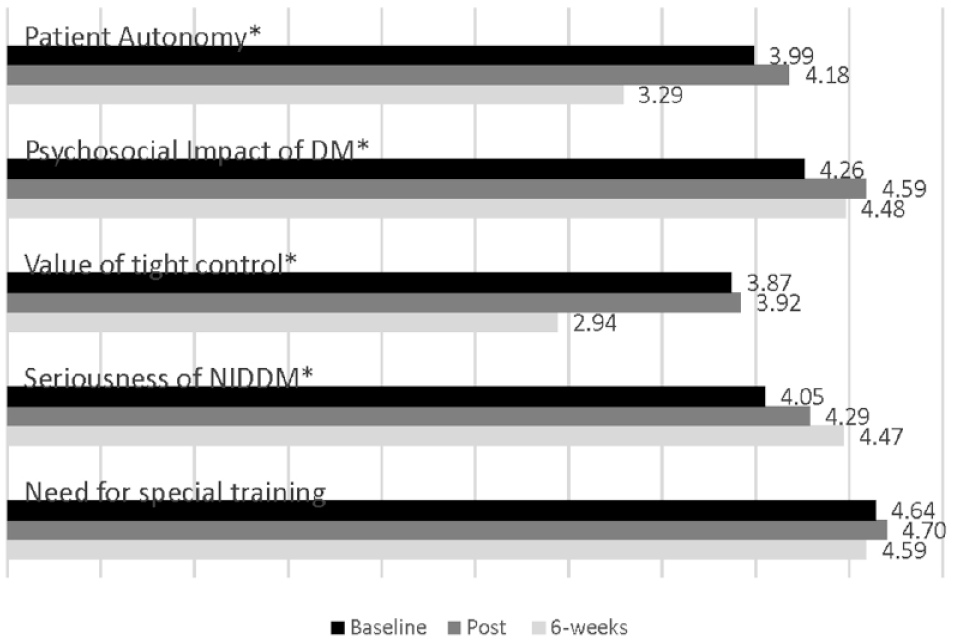
Differences in DAS-3 subscales at baseline, post assessment, and 6 weeks (n = 59).
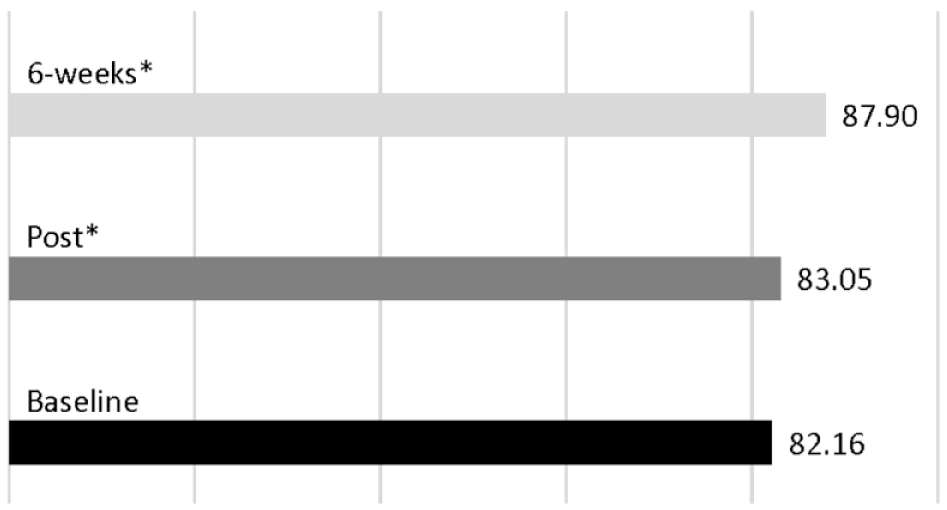
Jefferson Empathy Scale (n = 58) baseline, post assessment, and six weeks.
Repeated measures ANOVA with Greenhouse-Geiser correction determined that JES scores differed significantly among the three time points, F(1.941, 11.682) = 48.796, P < .001. Post hoc analysis with a Bonferroni correction adjustment revealed that JES statistically increased from baseline to post assessment, 5.74 (95% confidence interval [CI]: [4.30, 7.19]), P < .001, from baseline to six weeks, 0.90 (95% CI: [−611, 2.40]), P < .001, and from post assessment to six weeks, −0.90 (95% CI:[ −2.40, 0.61]), P < .001. These data suggest that the cine-VR 12-module simulation had a sustained impact on students’ empathy.
Presence Questionnaire
Following the virtual patient encounter, we observed mean scores ≥5.08 from a maximum score of 7.0, for all three subscales: Involvement (Mean: 5.41, SD: 0.83), Sensory Fidelity (Mean: 5.12, SD: 0.92), and Adaptation and Immersion (Mean: 5.08, SD: 0.64. The high subscale scores demonstrate favorable perceptions of the technology and sense of presence in the cine-VR simulations.
Qualitative Results
Seventeen students actively participated in the focus group discussion. The following themes emerged from data analysis (refer to Table 2 for additional rich quotes):
Representative Quotations from the Classroom Discussion.
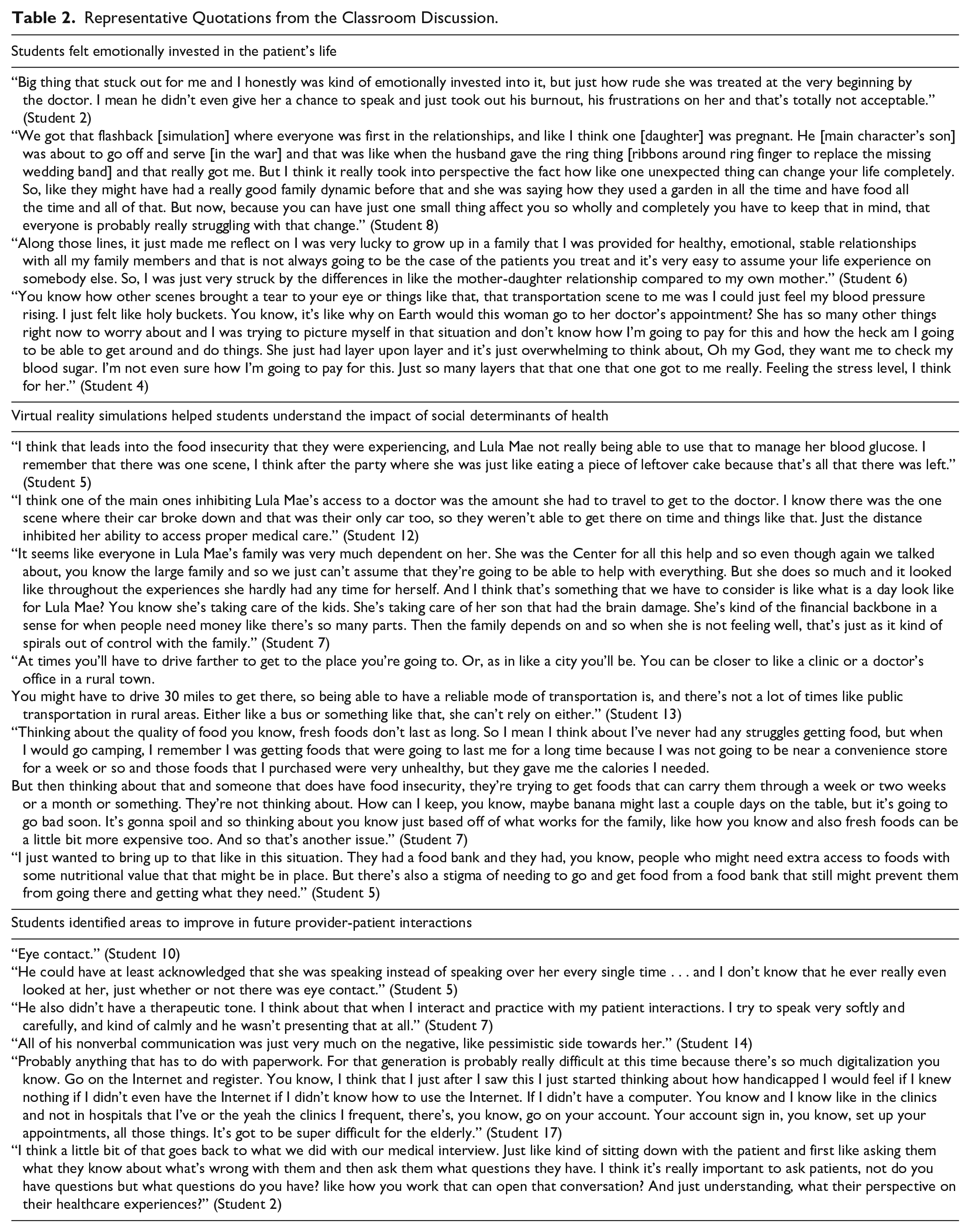
Feeling of Emotional Investment in Patient’s Life
When reflecting on the cine-VR simulations, many students commented on the emotional impact of their experience, acknowledging their emotional connection with the main character, Lula Mae, and how she was treated by providers and family members.
I was very emotionally invested in this, and I think I was in tears in the first 5 minutes. As we went along, I was just shocked at how her daughter treated her and they were definitely not helping.
Students described intense reactions to simulations that emphasized the barriers Lula Mae faced trying to manage type-2 diabetes. Students expressed feelings of overwhelm, anger, and frustration in watching Lula Mae struggle with these challenges. Students connected to their own family relationships and how similar or different those relationships were in the simulation.
Virtual Reality Simulations Helped Students Recognize Potential Impact of SDH
The cine-VR simulations offered students a glimpse into the home life of Lula Mae. Students observed how SDH interfered with her diabetes self-care. Students readily identified the different aspects of SDH, such as financial insecurity, food insecurity, transportation barriers, medication and supplies cost, and lack of social support:
I think a big one’s economic stability. If I remember right, they’re in Appalachia, right? So, that’s a very low-income part of America and so just being in that area usually the economic problem and then also education, the literacy could be a little bit lower than in other economically stable places.
Regarding lack of social support, students observed that having a large family did not always translate into support.
I was just really surprised that everybody kept saying, “Oh she’s got a big family. They’ll take care of her.” The pharmacist said it. The mechanic said it. The physician said it. Everybody said the family will help and obviously the family was not helping as much as they thought they were . . . We can’t just assume that family members will take care of our patients for us once they leave the clinic.
Students Identified Areas to Improve in Future Patient-Provider Interactions
The cine-VR series portrayed problematic visits between Lula Mae and her physician and pharmacist through two interactive guided simulations of a private conversation with the provider and a re-creation of Lula Mae’s challenging visits with the physician and pharmacist. The goal was to help students recognize strategies to improve the patient-provider relationship. Students identified eye contact, therapeutic tone of voice, nonverbal communication, and interruption as areas of providers’ communication deficits. In addition, students identified failure of providers to advocate for Lula Mae in negotiating the health care system, especially when there were obvious signs that she needed assistance:
Another thing that kind of surprised me was how the people that were giving her medical care, the pharmacist, and the doctor, weren’t willing to take that extra step of asking why she was late or why have you not filled out these forms in order to get this? Or help with payment and things like that. They weren’t going that extra step in helping her.
Discussion
Principal Findings
This study assessed DPT students’ empathy and attitudes toward diabetes before and after immersion in a 360° cine-VR patient encounter. After viewing the interactive modules, significant differences in empathy levels (JES) and diabetes attitudes in four DAS-3 subscales were found, such as Seriousness of type 2 diabetes (Mean: 4.32, P < .001), Value of tight glucose control (Mean: 4.01, P = .013), Psychosocial impact of diabetes (Mean: 4.62, P < .001), and Attitude toward patient autonomy (Mean: 4.22, P < .001). No significant change in Need for special training was observed.
To determine whether these results lasted beyond the immediate postassessment, DAS-3 and JES were measured at the six-week time point. Significant increases in the subscales Attitude toward patient autonomy (Mean: 0.75, P < .00), Psychosocial impact of diabetes (Mean: −0.21, P < .001), and Seriousness of type 2 diabetes (Mean: −039, P < .001); and significant decreases in the DAS-3 subscale Value of tight control (P < .001) were observed at six weeks, with no significant difference in Need for special training (P = .25). However, significant increases in JES were maintained throughout (P < .001), indicating that the cine-VR 12-modules had a sustained impact on students’ empathy up to six weeks after intervention. Finally, high scores on the PQ indicated a sense of being immersed in technology.
It is possible that concurrent curricular exposure to the pathophysiology of diabetes in a different course may have influenced the student perception of Value of tight control as students received this instruction between postassessment and six-week assessment.
Qualitative analysis provided insight into student learning that stimulated emotional reactions, discerned “patient” context and effect of SDH on health status, and identified provider errors that jeopardized patient-provider interaction. We believe these insights may explain JES scores in students.
Similar to our study’s purpose, research in pediatrics has explored the effect of a curriculum in SDH on empathy levels in residents, and favorable outcomes in dentistry exist when using virtual reality to improve students’ empathy by simulating care for families with language barriers and limited resources. This study, however, is the first to measure empathy and attitudes specific to diabetes in physical therapy students following a virtual reality immersion to facilitate understanding of the influence of SDH on health access and decisions. In addition, implementation of the cine-VR modules in the DPT curriculum addressed several educational needs, such as student engagement in a shared “patient” experience, appreciating multiple perspectives as >60 students were immersed and filtered information differently. Debriefing was a critical reinforcer for communication and perspective in team dynamics. The modules deepened an understanding of SDH by artfully introducing into the context a “real” individual and how she, her providers, family, and community are intertwined in simultaneous navigation of a chronic health condition embedded in complex social circumstances. The cine-VR technology provided a window into areas of a patient’s life that practitioners may not recognize in routine patient care visits, whereas students can better appreciate the patient’s challenge to manage diabetes within her family and community contexts. The immersive technology also allowed a realistic “patient” encounter during a time of clinical disruption owing to COVID-19 restrictions, confirming cine-VR’s utility to enhance flexible learning experiences. In addition, students who participated in this experience independently recalled and applied Lula Mae’s situational factors during a health promotion course two years later in the DPT curriculum (fall, 2022).
Limitations
This is a small study in one DPT course over two years at a Midwestern university with two campuses; thus, there is a selection bias in not expanding to other programs and areas of the country. We note this is a homogeneous sample of DPT students in terms of race/ethnicity and may affect their responses. While identifiable student data were not shared with the instructors, students may have felt the need to respond in a socially desirable way, which could bias results. There was no control group and other classes, and experiences may have affected student responses; therefore, student attitudes may not be solely due to the intervention. The lack of matching data throughout the six-week period is a limitation as only 47.9% of students completed all three surveys.
Conclusions
The cine-VR technology can provide an engaging and enduring learning experience for students, as evidenced in this project focused on diabetes management. Using cine-VR modules as a clinical exposure has the additional advantage of flexibility within the context of a busy student schedule. Although not a substitute for direct patient interaction, these modules may augment the clinical rotation and allow for a shared experience among students that enables in-depth classroom discussion. The cine-VR technology provides realistic engagement with the “patient” context, illustrating effects of SDH on health decisions that prevent management of diabetes. This learning experience could be easily tailored for the education of health professions beyond physical therapists and complex, chronic conditions other than diabetes. Because the effects of SDH and chronicity are multifactorial and require expertise beyond individual professions, this immersive learning experience also offers a dynamic platform for interprofessional learning and a focus on meaningful change in community health promotion and disease prevention initiatives to prevent chronicity. Practitioner attitudes and empathic capacity are fundamental to patient empowerment for self-care.
Footnotes
Acknowledgements
The authors thank Dr Elizabeth Beverly for allowing them to use the module that she and her team had created. Lula Mae has been inspirational to so many students and faculty.
Abbreviations
cine-VR, virtual reality cinema; DAS-3, Diabetes Attitude Scale–Version 3; DPT, doctor of physical therapy; JES, Jefferson Empathy Scale; PQ, Presence Questionnaire; SDH, social determinants of health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was part of the Medicaid Equity Simulation Project funded by the Ohio Department of Medicaid and administered by the Ohio Colleges of Medicine Government Resource Center. Views expressed in this publication about the cine-VR simulations are solely those of the creators and do not represent the views of the state of Ohio or federal Medicaid programs.