
Abstract
Background:
Insulin pumps and continuous glucose monitors (CGM) can improve glycemic control for individuals with type 1 diabetes (T1D). Device uptake rates continue to show room for improvement, and consistent adherence is needed to achieve better outcomes. Diabetes health care providers have important roles to play in promoting device use and adherence.
Methods:
We surveyed 209 clinicians who treat people with type 1 diabetes to examine perceptions of barriers to device uptake, attitudes toward diabetes technology, and resources needed for clinicians to improve device uptake. We compared findings with our survey of adults with T1D.
Results:
Younger clinicians treated more patients using insulin pumps (r = –.26, P < .001) and CGM (r = –.14, P = .02), and had more positive attitudes about diabetes technology (r = –.23, P = .001). The most frequently endorsed modifiable barriers were perceptions that patients dislike having the device on their body (73% pump; 63% CGM), dislike the alarms (61% CGM), and do not understand what to do with device information or features (40% pump; 46% CGM). Clinicians wanted lower cost and better insurance coverage for their patients, and they recommended counseling and education to help address barriers and improve adherence to devices.
Conclusion:
Clinicians perceive many barriers to their patients initiating and adhering to diabetes devices. Findings highlight opportunities for intervention to improve clinician-patient communication around device barriers to help address them.
Keywords
Insulin pumps and continuous glucose monitors (CGM) are increasingly important components of managing type 1 diabetes (T1D) and have been shown to improve glycemic control, health-related quality of life, and treatment satisfaction.1-5 Device users report benefits such as increased flexibility and freedom and decreased stress.6,7 However, consistent adherence to wearing these devices requires a complex set of user behaviors. Device wearers must change insulin pump and CGM sites frequently; order and maintain the proper supplies and prescriptions; calibrate the CGM through regular blood glucose checks; count carbohydrates; and administer boluses.8,9 Table 1 outlines the numerous adherence tasks required for using insulin pumps and CGM, divided by frequency of engagement in each task.
Adherence Tasks for Insulin Pump and CGM Use.
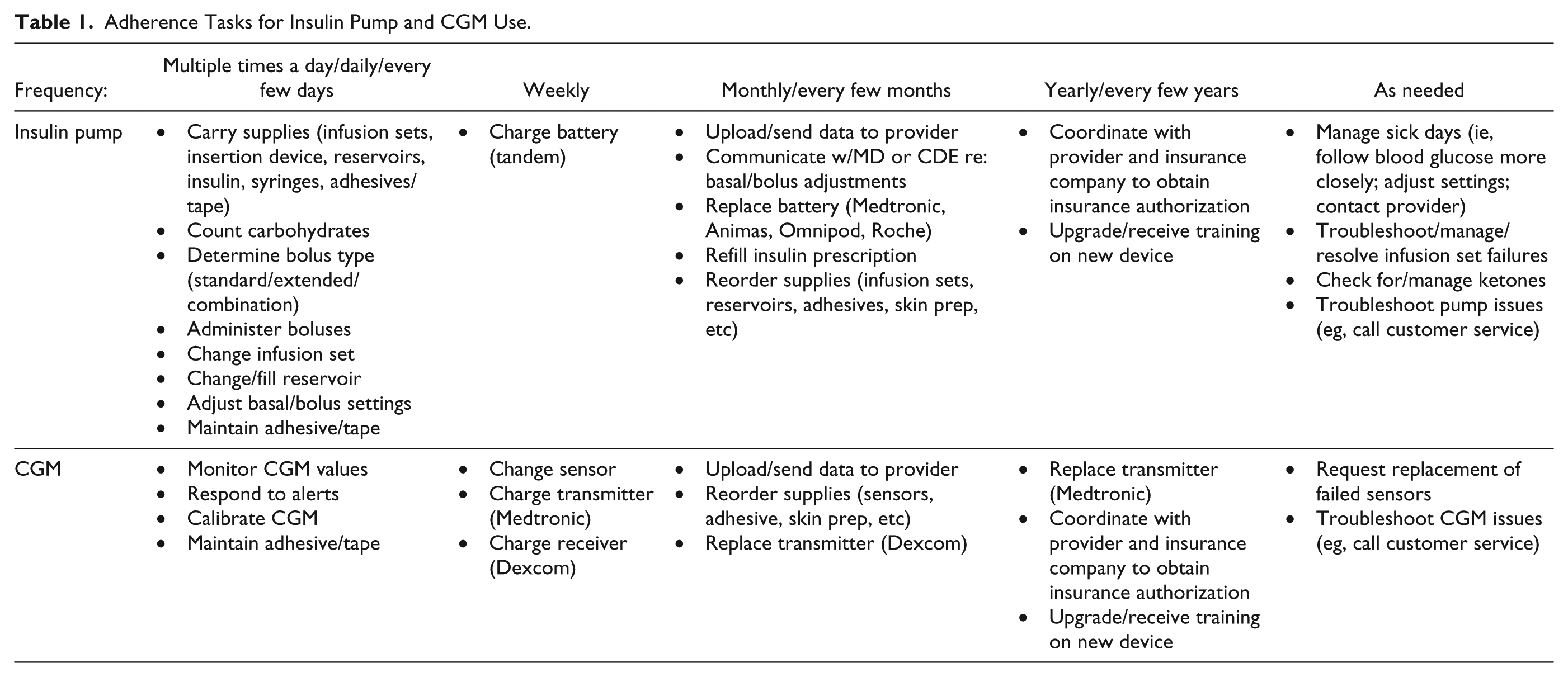
Greater CGM adherence—and engagement in the tasks outlined in Table 1—has been linked to optimal diabetes outcomes.10-15 Specifically, wearing a CGM 6 or more days a week, 15 or at least 60% of the time, 14 has been linked to greater improvements in HbA1c compared to wearing a CGM fewer than 6 days a week. More frequent blood glucose monitoring has been linked to greater CGM adherence and greater benefit from CGM. 12 Furthermore, greater adherence to CGM has been linked to better treatment satisfaction; frequent users may focus more on benefits outweighing the hassles while infrequent users focus more on hassles outweighing benefits. 16 Therefore, pre-CGM counseling to establish realistic expectations and provide troubleshooting strategies may address barriers to CGM adherence. 16
Diabetes clinicians—endocrinologists, nurses, diabetes educators, dietitians, and others—have important roles in promoting adherence to devices. Clinicians can suggest and facilitate device initiation. This role is particularly crucial considering that while pump uptake rates are above 60%, only 9% of T1D Exchange registrants were using CGM as of 2014.17,18 Clinicians are also the main source of education, support and troubleshooting for device use. 19 To start insulin pump treatment, for example, patients need comprehensive education that covers using the device itself, counting carbohydrates, checking blood glucose, and managing sick days.20-22 Delivering an ongoing, structured education protocol when starting insulin pump and CGM together has proven effective to introduce these technologies and to help patients benefit from them. 22
Clinicians may also counsel patients experiencing barriers to device use. For the purpose of this paper, we divide barriers to device use into two overarching categories: those requiring policy-level changes (“nonmodifiable barriers,” eg, device cost, insurance coverage, demographic variables, device attributes 23 ) and those able to be modified via clinical intervention. Modifiable barriers may stem from human factors, including patients’ perceptions or beliefs about devices, their attitudes, or their preferences. 24 For example, perceived benefits from devices and ease of use promote CGM adherence.25,26 Meanwhile, “information overload” and lack of trust are major barriers to using CGM. Hassle and dislike of wearing devices and not liking devices on one’s body are major barriers to both CGM and pump use. 27 Those who discontinue using CGM cited reasons including alarms, inaccuracy and life interference.11,27,28 Those who discontinued using insulin pumps cited pain and life interference.19,27 Finally, individuals endorsing more barriers to device use also report more diabetes distress. 27 Thus, many modifiable barriers may be potential targets for intervention to increase uptake and prevent discontinuation.
Counseling and troubleshooting support may improve adherence, prevent discontinuation, and increase device users’ quality of life by helping to navigate hassles and increase benefits. How users engage with CGM data may determine the extent to which they benefit. For instance, a qualitative study of CGM users found that those who benefitted had social support and engaged with CGM data by examining patterns over time rather than responding in each moment. 29 Furthermore, clinicians’ communication style—for example, adopting a motivational interviewing approach rather than being directive—may encourage continued device use. 30 This approach may be helpful for patients who are considering discontinuing CGM use despite knowledge that it may improve glycemic control. 28
Clinicians have an instrumental role in promoting and sustaining device use. Therefore, the goals of this study were to understand relationships between clinician attributes; their perceptions about barriers to device use; and device uptake among their patients to inform intervention development to address barriers and increase uptake and adherence. The specific aims were to (1) examine relationships between clinician attributes (eg, demographics, practice settings) and rates of device uptake among their patients; (2) describe clinician-perceived barriers to device use; (3) compare these results to our survey of adults with T1D; 27 and (4) describe resources clinicians need to overcome barriers. To address these aims, we developed an electronic survey for clinicians who treat youth and/or adults with T1D.
Methods
We surveyed diabetes providers from two different study recruitment sources during the first half of 2016: the T1D Exchange Clinic Network, which includes 75 endocrinology centers in the United States, and dQ&A, a diabetes market research company that surveys panels of diabetes providers. Clinicians could be adult and/or pediatric providers. Clinicians were contacted via email to participate in a web-based survey. Participants provided electronic informed consent prior to taking the survey. The survey took approximately 45 minutes. Participants received a $75 gift card and had the option to donate this money to a diabetes charitable organization of their choosing. Methods and results for our survey of adults with T1D were previously reported elsewhere. 27 The Stanford University IRB approved all study procedures.
Measures
Demographic and clinical practice characteristics
Participants provided demographics (eg, age, race/ethnicity, gender); clinical practice characteristics (eg, provider type, years in practice, practice setting); and patient population characteristics (eg, percentage of patients with T1D, adults vs pediatrics, percentage using diabetes devices).
Clinician perceptions of barriers to device use
We presented a list of 19 possible barriers to using devices separately for insulin pumps and CGM. Literature review, market research, and findings from our T1D adult survey informed the development of this list. 27 Clinicians could select as many barriers as applied. The list included nonmodifiable barriers (eg, costs, insurance) and modifiable barriers (eg, not liking devices on their body, nervous to rely on technology). Clinicians then ranked the top 3 barriers and described resources they needed to overcome these barriers.
General and diabetes technology attitudes
Six items about technology in general (eg, “Technology has made my life easier” and “I am lucky to live in a time with so much technology”) and 5 items about diabetes technology (eg, “Diabetes technology has made my patients’ lives easier” and “My patients are lucky to live in a time with so much diabetes technology”) assessed clinicians’ technology attitudes. Items were rated on a Likert scale (1 to 5) and summed separately to create two total scores (possible range of 6-30 for general technology; 5-25 for diabetes technology); higher scores indicate positive technology attitudes. Internal consistency for the current sample was .86 for general technology attitudes and .83 for diabetes technology attitudes.
Analytic Plan
Descriptive statistics described characteristics of clinicians, their practices, and patients. For aim 1, bivariate correlations explored relationships between clinician, practice and patient variables. t-tests examined differences in device uptake and technology attitudes by practice setting. To address aim 2, we calculated frequencies of barriers to device use for insulin pump and CGM. To address aim 3, t-tests compared clinician-endorsed barriers and results from our survey of adults with T1D. For aim 4, we coded survey responses to the open-ended question about resources needed to address barriers to insulin pump and CGM. Three coders created a list based on responses from clinicians. Coders met weekly to refine and adjust the code list and resolve discrepancies. We calculated frequencies for each code.
Results
Sample Characteristics
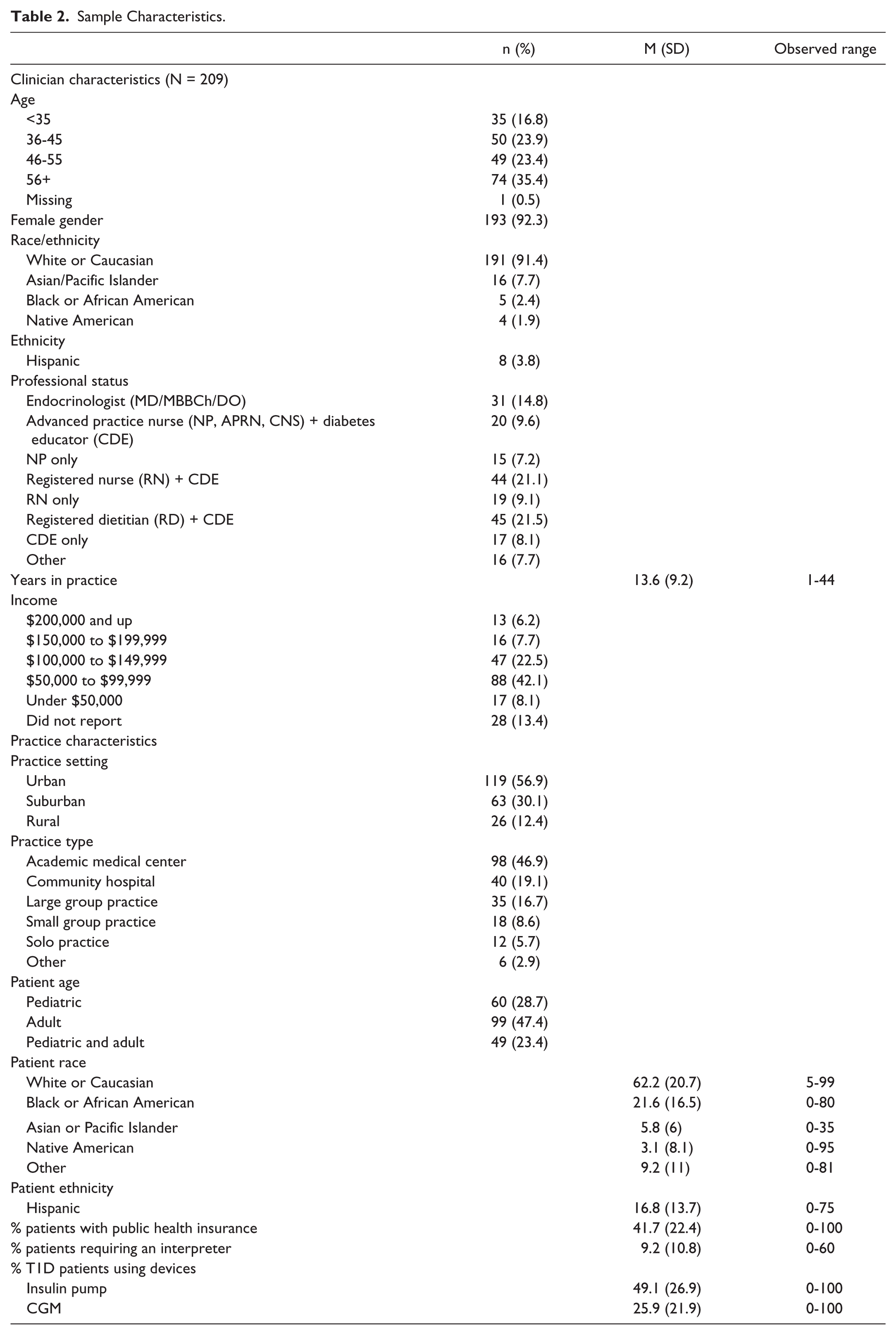
Table 2 presents clinician and practice setting characteristics (N = 209; 92% female; 59% over 45 years old; practice duration mean = 14 years, SD = 9). The most common professional statuses included certified diabetes educator (CDE)/registered dietitian (22%), CDE/registered nurse (21%), and endocrinologist (15%). Most clinicians practiced in urban settings; and nearly half worked in academic medical centers. Half worked with adults, 29% with youth, and a quarter treated both adults and youth. Clinicians estimated that, on average, half their T1D patients use an insulin pump and a quarter use CGM. They reported that CDEs were the most common pump trainers (74%) followed by contracted pump trainers (19.7%).
Sample Characteristics.
Aim 1: Clinician and practice attributes associated with device use
Older age of clinician was associated with having fewer patients using insulin pumps (r = –.26, P < .001) and CGM (r = –.14, P = .04), and having more negative attitudes about diabetes technology (r = –.23, P = .001). Having positive attitudes about diabetes technology was associated with having more patients on insulin pumps (r = .15, P = .03) and CGM (r = .29, P < .001), and seeing more patients under the age of 18 (r = .15, P = .04). Providers at academic medical centers treated more patients using insulin pumps (53.4%) and CGM (29.9%) compared to providers in other settings (pumps 45.2%; CGM 22.4%), pump: t(207) = 2.29, P = .02; CGM: t(207) = 2.52, P = .01. Providers at academic medical centers also had more positive attitudes toward diabetes technology (mean = 20.8, SD = 2.7), but not general technology, compared with other providers (mean = 19.8, SD = 2.8), t(207) = 2.68, P = .008. Providers in urban settings treated more patients using CGM (29.3%) than suburban and rural providers (21.5%), t(207) = 2.58, P = .01. Pump use and technology attitudes did not differ significantly between urban, suburban, and rural settings.
Aim 2: Clinician-reported barriers to device uptake
Clinicians reported a mean of 7.2 (SD = 3.5) barriers to insulin pump use and 7.4 (SD = 4) barriers to CGM use. Table 3 presents the complete list of clinician-reported barriers alongside our findings from the T1D adult survey. The most commonly reported barriers to insulin pump and CGM were nonmodifiable (insurance coverage; costs). The most frequently endorsed modifiable barriers to pump use were clinicians perceiving that patients dislike having the device on their body (73%); dislike the number of alarms (40.7%); and do not understand what to do with the pump’s information or features (40.2%). Similar to the pump, clinicians most often endorsed modifiable CGM barriers related to perceiving that patients dislike having the device on their body (63%); feel there are too many alarms (61%); and do not understand what to do with the CGM’s information or features (46%).
Clinician- and Patient-Reported Barriers to Device Use.
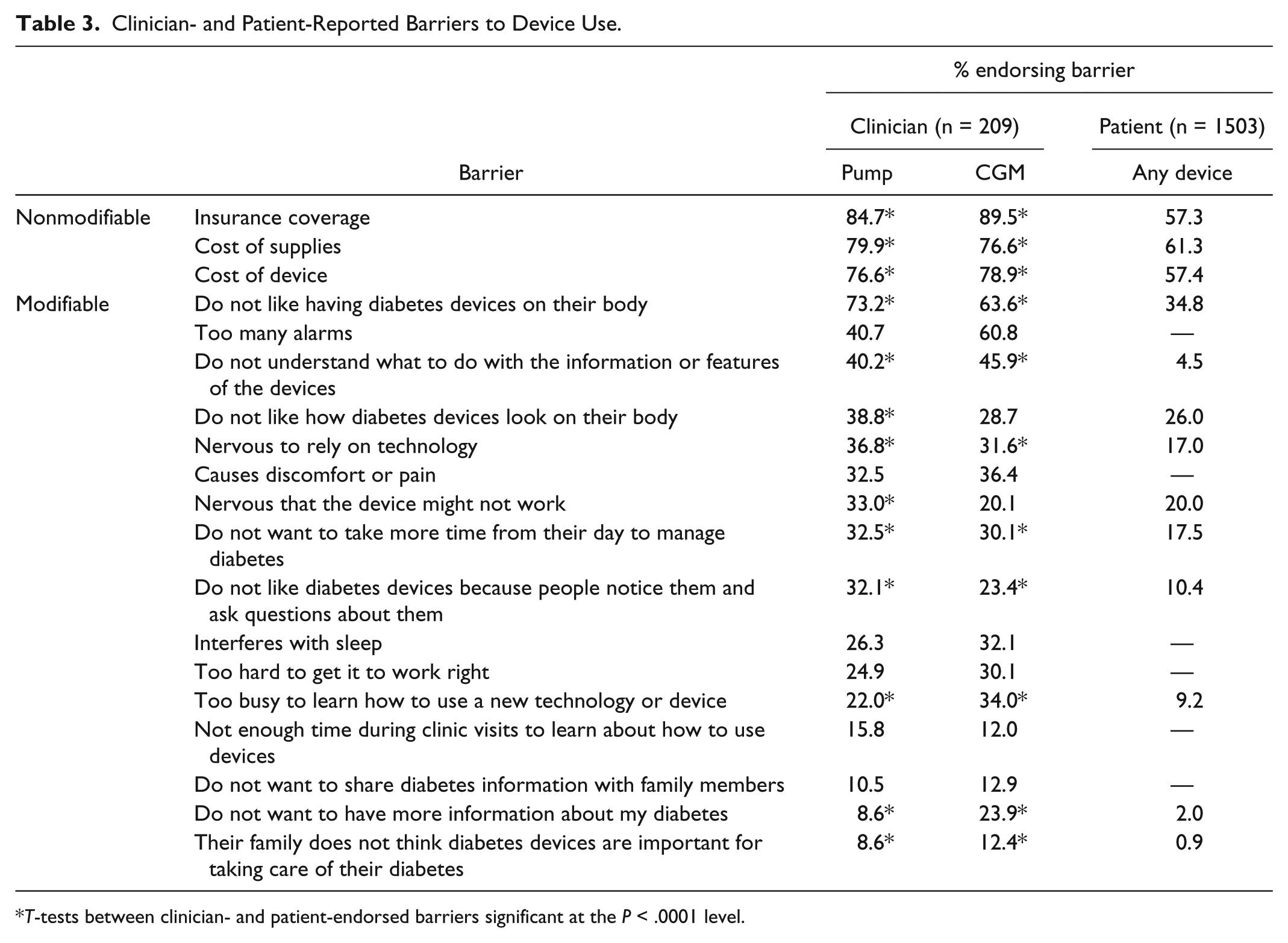
T-tests between clinician- and patient-endorsed barriers significant at the P < .0001 level.
When asked to rank the top three barriers to device use, clinicians most often cited cost (insurance coverage, cost of device, cost of supplies) as the top barrier to using both insulin pumps (49%) and CGM (66%). For insulin pumps, clinicians most often said the second top barrier to pump use was patients not wanting to take more time out of their day to manage diabetes (14%) and the third top barrier was patients not having sufficient education or understanding how to use the device (12%). For CGM, clinicians said the second top barrier to device use was their patients not having sufficient education or understanding of how to use it (12%). Sounds and alerts presented the third top barrier to CGM use (8%).
Aim 3: Comparisons between clinician- and adult-reported barriers
Across the board, clinicians endorsed barriers more frequently than adults with T1D (N = 1,503; mean age = 35.3, SD = 14.8) (Table 3). The largest difference was seen for the barrier “Do not understand what to do with the information or features of the devices.” Nearly half of clinicians (40-46%) thought this barrier applied to their patients while only 4.5% of adults with T1D endorsed it. For “Do not like having diabetes devices on their body,” 64-73% of clinicians endorsed this barrier while 35% of adults with T1D endorsed it. Clinicians also thought more often that their patients’ “nervousness to rely on the technology” was a barrier to CGM and pump use (32-37%) compared to adults with T1D (17%).
Aim 4: Resources needed for clinicians to address device uptake
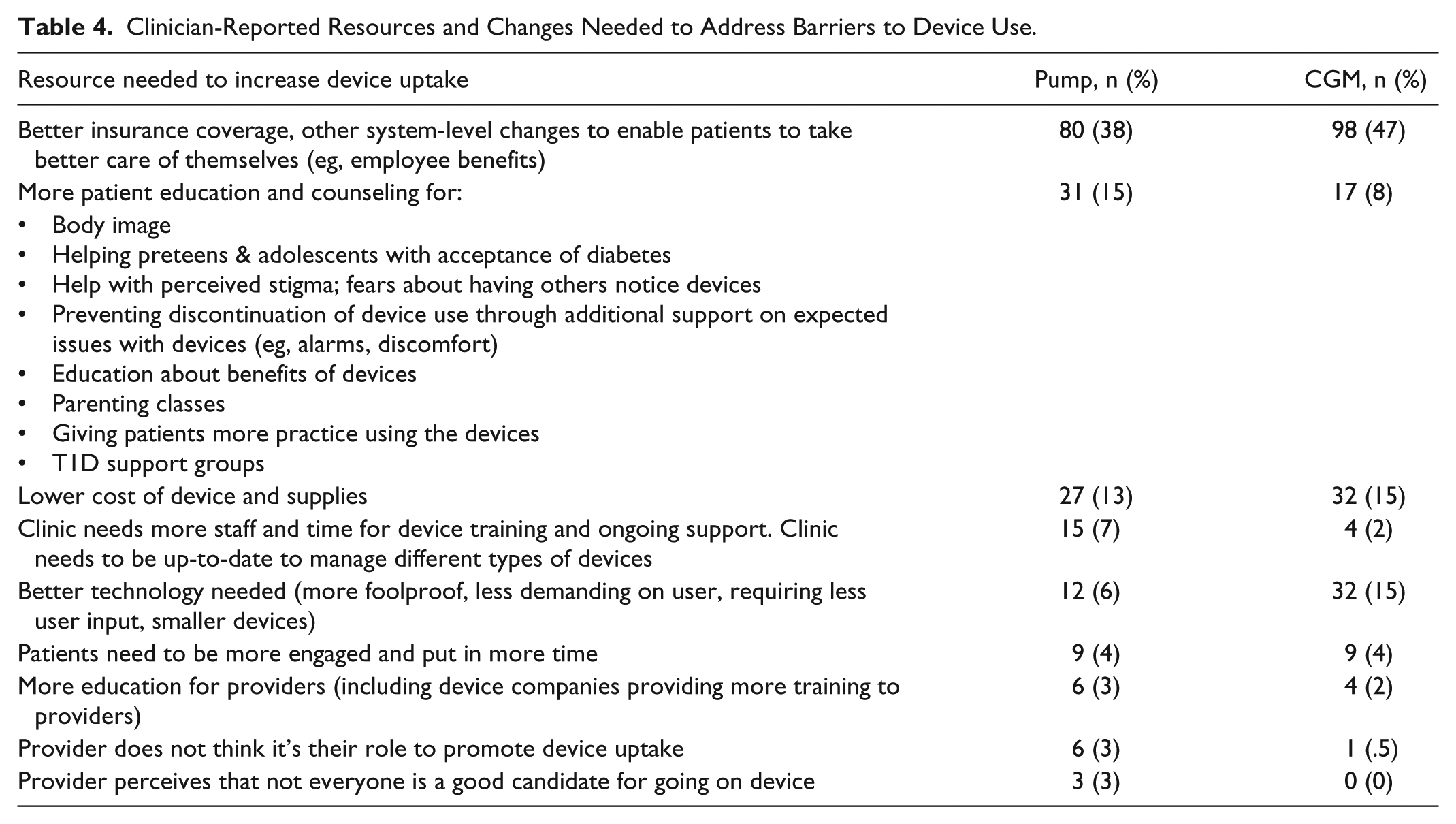
Table 4 presents the list of resources or changes clinicians desired to improve rates of uptake of insulin pump and CGM. Clinicians most frequently requested better insurance coverage and employee benefits for their patients for both pump (38%) and CGM (47%). They also desired improved patient education and counseling around device use and related issues (pump: 15%; CGM: 8%). Finally, some mentioned wanting more staff, more clinic time for device training, and improved technology.
Clinician-Reported Resources and Changes Needed to Address Barriers to Device Use.
Discussion
Results from our survey of diabetes clinicians who treat individuals with T1D demonstrate that clinicians perceive many barriers to their patients using and adhering to diabetes devices. Clinicians reported that about half of their patients with T1D currently used an insulin pump while a quarter used CGM. We observed that younger clinicians treated more patients who were using devices, and held more positive attitudes about technology compared with older clinicians. The top modifiable barriers clinicians endorsed were that patients do not like having devices on their body, do not understand what to do with information or features of the devices, and do not like the frequency of alarms from the devices.
Another purpose of this survey was to compare clinician-endorsed barriers with the results from our previous survey of adults with T1D. We observed that clinicians endorsed more barriers to device use than adults with T1D. Clinicians and adults with T1D agreed that cost and insurance were the biggest obstacles, but clinicians more frequently endorsed these barriers. A larger proportion of clinicians also thought not liking devices on one’s body was a barrier compared with adults with T1D. We observed a large disparity between clinicians and adults with T1D regarding the barrier of not understanding what to do with information or features of the devices. Nearly half of clinicians endorsed this barrier while only a small percentage of adults with T1D endorsed it. The reason for this disparity may be due to actual differences (ie, patients have knowledge that clinicians think they lack) or perceived differences (ie, patients do not know what information they lack, while providers have greater awareness of this). The lack of alignment of provider and patient perceptions of barriers may impact uptake and adherence to diabetes devices. If clinicians anticipate greater barriers to device uptake than their patients do, they may be reluctant to encourage uptake.
Findings point to several implications and areas for future investigation. One area for further study and possible intervention is the introduction of devices. In other words, how do clinicians become educated about devices and then decide to suggest devices to their patients? How do they evaluate readiness for device initiation? How do they approach resistance? As noted earlier, the nature of these conversations may influence a person’s openness to regimen changes. In particular, a collaborative, motivational interviewing approach could be more effective when educating patients about a new device and exploring barriers. 30 Furthermore, clinicians may have limited time with each individual to discuss pros and cons of devices and to evaluate readiness and potential barriers to uptake and adherence. Therefore, future efforts could focus on developing brief, standardized methods for assessing readiness for device initiation to help guide patient-provider conversations within a limited time frame. Once clinicians identify the biggest barriers for a particular patient, it will also be important to have tailored intervention strategies available to address those barriers. Addressing barriers upfront and on an ongoing basis may promote uptake and increase future adherence when challenges arise. Given that provider engagement with technology and patients’ diabetes data has been shown to encourage patients’ use of the technology,31,32 availability of ongoing provider support and involvement will be important to ensure adherence to devices.
Limitations
As this was an online survey, it may have selected for more technologically savvy responders and may not generalize to all clinicians working with patients with T1D. One limitation of this survey is that the majority of respondents were CDEs and either registered nurses or dietitians; endocrinologists made up less than a quarter of the sample. Respondents were also almost all women. Therefore, these results may not be representative of all types of diabetes health care providers, including male providers. Clinicians also estimated that a quarter of their patients used CGM, which is higher than the 2014 T1D Exchange rate of 9%, 17 but lower than what we found in our 2015 survey of adults with T1D. 27 This increase may be in part due to increasing rates of CGM use in the past two years as well as this sample of clinicians treating more technologically savvy patients. In addition, the cross-sectional, correlational study design precluded drawing causal relationships between clinician age, device use, and technology attitudes. We found significant, but somewhat small, associations between clinician characteristics and patient device uptake. Therefore, more research is needed to understand the impact of technology attitudes, patient and clinician characteristics, and other unmeasured factors on the likelihood of suggesting that patients initiate device use. Furthermore, clinicians surveyed were not necessarily those providing care to those in our adult survey, which could contribute to some lack of alignment between the two groups. It is also possible that children and adolescents with T1D, and their parents, may experience different or greater barriers than adults that may be more aligned with barriers endorsed by clinicians in the present survey. Future analyses should compare parent and/or youth-endorsed barriers with clinician perspectives. In addition, we separated barriers by CGM and insulin pump for the clinician survey and they were combined in the adult survey. Thus, we cannot conclude that clinician-reported barriers necessarily apply directly to adult respondents.
Conclusions
Clinicians who treat individuals with T1D have important roles to play in promoting uptake and adherence to insulin pumps and CGM among the individuals they treat. Our results show that clinicians perceive many barriers to device uptake and adherence—more so than adults with T1D. Beyond wanting lower costs and better insurance coverage for devices, clinicians identified educational and counseling targets to address barriers to uptake and sustained device use, such as addressing perceived stigma, enhancing education on the benefits of devices, and providing ongoing support for device users to troubleshoot problems that come up and reduce device discontinuation. In an ongoing trial, we are testing interventions that aim to reduce distress and optimize device use. Clinicians may benefit from similar in-service training on how to help their patients experience more benefits from devices. Finally, some providers noted that support from other device users could be beneficial. Due to the complex adherence tasks involved in device adherence, a combination of psychoeducation, practical support (eg, remote monitoring; check-ins between medical visits), and emotional support may encourage adherence to diabetes devices. Successful interventions may need to target clinicians as well as potential device users to maximize impact.
Footnotes
Acknowledgements
The authors are grateful to Bianca Agustin and Hillary Kroll for their assistance with data analysis.
Abbreviations
CDE, certified diabetes educator; CGM, continuous glucose monitor; HbA1c, hemoglobin A1c; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by The Leona M. & Harry B. Helmsley Charitable Trust.