
Abstract
Objective:
People with diabetes have an increased risk of depression, intentional self-injury and self-harm (ISI), and suicide compared with the general population. This study aimed to explore experiences and awareness of healthcare professionals (HCPs) regarding depression, ISI, and suicide, and understand resource use and needs among HCPs who care for persons with diabetes (PWD).
Methods:
Healthcare professionals who see children and/or adults with type 1 diabetes or type 2 diabetes anonymously completed an online survey about their experiences, opinions, barriers, and needs surrounding identification and care of PWD with depression, ISI, and suicide.
Results:
One hundred twenty-nine HCPs participated. The majority were medical doctors (MDs) or advanced practice providers (APPs). Only a quarter of MDs and APPs felt very comfortable asking about ISI or suicidal ideation (SI), whereas 20% felt they had received appropriate training to support those with ISI or SI. The primary needs reported include more training on how to ask, respond, and support those expressing ISI and SI. Healthcare professionals reported wanting better access to resources for PWD.
Discussion:
The HCPs tend to underestimate SI in the diabetes population and rates of training were low. Areas to address include providing education and training to HCPs to improve identification and management of ISI and suicide risk. These data can inform the development of mechanisms to improve discussions of depression and suicide and of resources to help HCPs support PWD.
Introduction
People with diabetes have an increased risk of depression and suicide compared with the general population.1,2 The prevalence of depression is approximately three times higher for people with type 1 diabetes (T1D) and nearly twice as high for people with type 2 diabetes (T2D) compared with those without diabetes. 3 Depression is more common among suicide victims with diabetes compared with suicide victims without diabetes. 4 Furthermore, suicidal ideation (SI) and intentional self-injury and self-harm (ISI) are more prevalent among people with diabetes compared with those without diabetes.5 -7
Depression has been associated with suboptimal glycemic levels among people with T1D and T2D.8 -10 Furthermore, worsening glycemic management, longer duration of diabetes, and use of insulin therapy have all been identified as clinical characteristics that are associated with an increased risk of SI and suicidal behaviors among people with diabetes.11,12 Use of insulin therapy may increase suicide risk by providing access to a potentially lethal suicide method. Results from a population-based study of suicide victims indicated that nearly a quarter of those with T1D who committed suicide did so through the use of insulin as the suicide method. 4 However, intentional insulin overdoses are likely underreported and may explain a significant proportion of people with diabetes who present to emergency departments with hypoglycemia of “unknown” etiology.13,14 There is reason to hypothesize that rates of suicide and ISI among people with diabetes are underestimated due to underreporting of acts of ISI and suicide attempts. 15
Healthcare professionals (HCPs) who care for persons with diabetes (PWD) should be aware of the increased risk for ISI and suicide in this population. Screening for depression is recommended by international associations, including the American Diabetes Association (ADA) and International Society for Pediatric and Adolescent Diabetes (ISPAD).16,17 Although studies have reported the implementation and use of depression screening in diabetes care, 9 ,18 -20 many HCPs are hesitant to implement screening for depression and suicide if they feel unequipped to respond when their patients screen positively or feel they do not have the appropriate resources to provide patients when they report depressive symptoms, SI, or ISI. Primary care studies have evaluated HCPs’ opinions of mental healthcare and specifically suicide risk screening.21,22 These studies found that HCPs felt screening was important but were concerned about poor access to mental healthcare, disruption to clinical flow when someone screened positive, and overall concern that patients would not attend when a referral was placed. Within diabetes care, studies have shown that in those with positive mental health screening who are referred to mental healthcare, approximately 50% attend a mental healthcare appointment.23,24 Studies specifically within diabetes care have not explored HCP awareness, knowledge, comfort level, and resource needs in terms of depression and suicide risk in those with diabetes. Given that depression and suicide are more common in this population, it is imperative to determine from HCPs what the unmet needs are and how best to provide the education and resources so HCPs can intervene effectively when an individual reports depression, ISI, or SI.
The aim of this study was to understand HCP perspectives regarding depression and suicide among people with diabetes. Through a brief online survey, we sought to examine HCP awareness of the higher prevalence of depression, ISI, and SI in this population as well as HCP experiences encountering these concerns in clinical settings. Furthermore, we aimed to understand barriers to identification, access to resources, and other unmet needs.
Methods
The study was approved by the Colorado Multiple Institutional Review Board (COMIRB), the institution hosting the survey. A brief description of the study and an invitation to participate was sent through electronic mail to different diabetes centers and through social media platforms, and the survey remained open for approximately 2 months. All HCPs involved in T1D or T2D care were eligible to complete the anonymous survey. Postcard consent was used, meaning that the consent was written at the beginning of the survey and it was noted that continuing onto the survey indicated that the participant was providing consent to be part of the study, which was provided at the beginning of the survey. Given the anonymous nature of the survey, and how it was distributed, we were not able to calculate response rates.
Measures
The survey was administered by Research Electronic Data Capture (REDCap), 25 a secure online research management platform, where data were also collected and stored. The survey was critically reviewed by six HCPs who provided feedback and minor edits to wording of questions. Following revisions, the survey was disseminated globally to HCPs in May 2021, by outreach, to multiple clinics by the coauthors of this study with a request to those clinics to further outreach to other clinics. Thus, it is unclear as to how many HCPs received the e-mail invitation to complete the survey. The HCPs who opted to participate filled out the online survey, taking approximately five minutes to complete.
The survey included 10 demographic and practice characteristics questions and 22 survey questions (Supplemental Table 1). The questions included knowledge questions about rates of suicide, self-injurious behaviors, and depression in T1D and T2D, as well as questions surrounding HCP experiences and beliefs around mental healthcare in the clinic setting. Questions were set in Likert scale, multiple-choice, or free text. The HCPs were able to submit the survey without completing all questions.
Data Analysis
The HCPs who did not complete all questions were included in the analyses for only the questions to which they provided a response. Of the 16 participants who did not complete the survey, only seven provided demographic data; three additionally answered T1D estimates of rates questions (eg, estimate of percentage of people with T1D who have experienced depression); four answered the above and additionally answered T2D estimates of rates questions; one answered the above and additionally answered whether they believed there was a correlation between glycemic control and SI or ISI, what activities relating to diabetes management are considered self-harm behaviors, and belief of professional responsibility to ask patients about depression, SI, ISI, or suicide attempt; and one answered the above and additionally answered questions surrounding comfort in asking patients specific questions, and the question on whether they had received any postgraduate training on how to support patients engaged in ISI or suicidal acts. Any questions that were answered were used in analysis. Descriptive analyses were conducted in SPSS to analyze survey results. Free-text responses were not formally coded; however, they were used to elicit further explanation for categorized response questions.
Results
One hundred twenty-nine HCPs participated in the survey, with 113 HCPs completing the full survey, and 16 completing part of the survey. Demographic data are presented in Table 1. The participants had a mean age of 45.8 years, were majority female (87.6%), and the majority identified as White (84.5%). Medical doctors (MDs) or advance practice providers were the largest professional representation (40.3%) along with other survey respondents, including certified diabetes care and education specialists (CDCESs; formerly called certified diabetes educators), psychologists and other professionals. Respondents worked a mean of 13.9 years in diabetes care. The majority worked in secondary specialist centers (22.5% at an adult center and 51.2% at pediatric centers) and at either a public (28.7%) or private (21.7%) academic medical center that provided healthcare to >200 patients with diabetes (84.9%). Almost all respondents practiced in the United States (81.7%) or United Kingdom (14.3%).
Demographic Characteristics and Clinic/Practice Details.
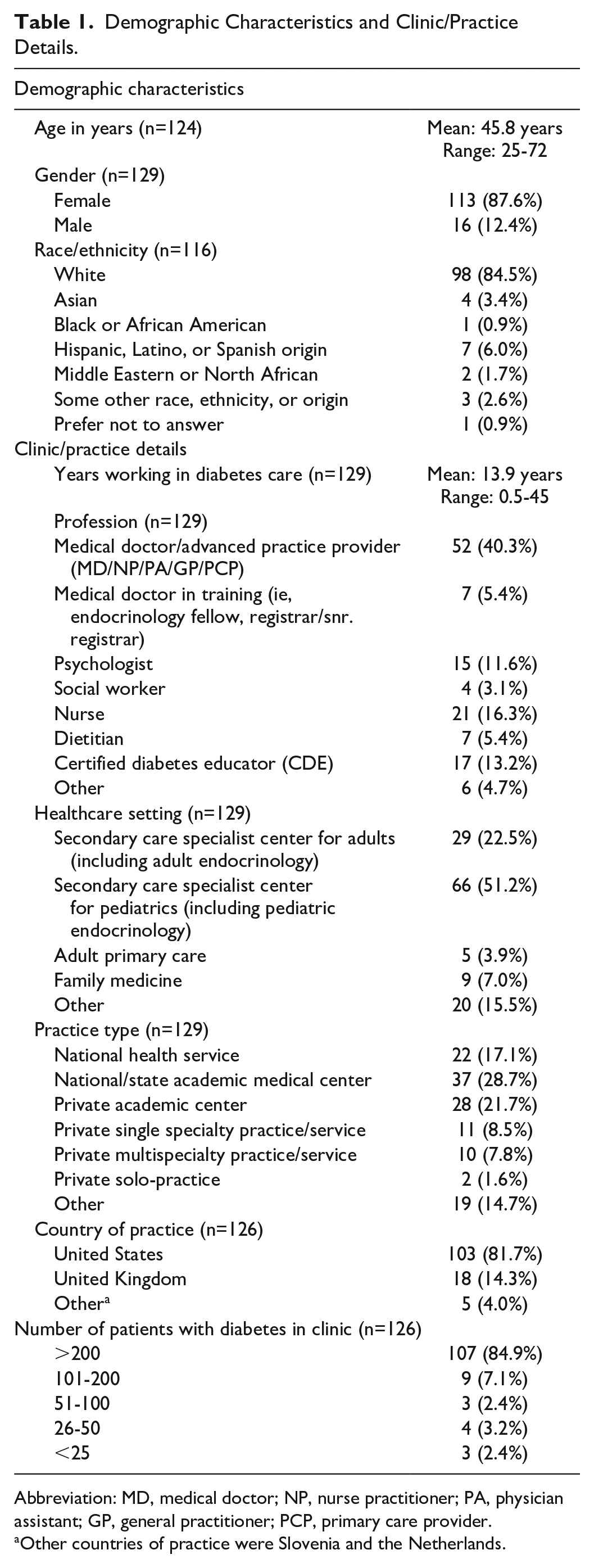
Abbreviation: MD, medical doctor; NP, nurse practitioner; PA, physician assistant; GP, general practitioner; PCP, primary care provider.
Other countries of practice were Slovenia and the Netherlands.
Awareness of Depression, ISI, and Suicide Risk Among People With Diabetes
Based on their clinical experiences, HCPs were asked to estimate the percentage of people with T1D and T2D who have experienced depression, had SI, deliberately injured themselves, and attempted suicide (Table 2). The HCPs suspected higher prevalence of depression among people with T2D compared with people with T1D. When asked about what percentage of individuals with T1D have had SI, deliberately injured themselves, or attempted suicide, the majority of HCPs estimated prevalence at less than 10%. The results were similar for those with T2D (Table 2). In a multi-select question, HCPs were asked which behaviors relating to diabetes management they thought should be categorized as ISI for people with T1D. The following are listed in order from most to least frequently recognized by HCPs as self-harm (ISI) behaviors: (1) insulin omission (96.3%); (2) over-bolusing (80.7%); (3) binge eating to purposefully increase blood sugars (61.5%); (4) “rage bolusing,” defined as bolusing multiple times in short succession to bring elevated blood sugars down into range (47.7%); and (5) other (12.8%). Other behaviors that HCPs described as ISI among people with T1D included intentional hypoglycemia, self-injurious behaviors with diabetes supplies (eg, needles), and purposefully not wearing medical devices or not checking blood glucose levels.
Healthcare Professional Estimates of Percentage of People With Diabetes Having Experienced Depression, Suicidal Ideation, Intentional Self-Injury, or Attempted Suicide.
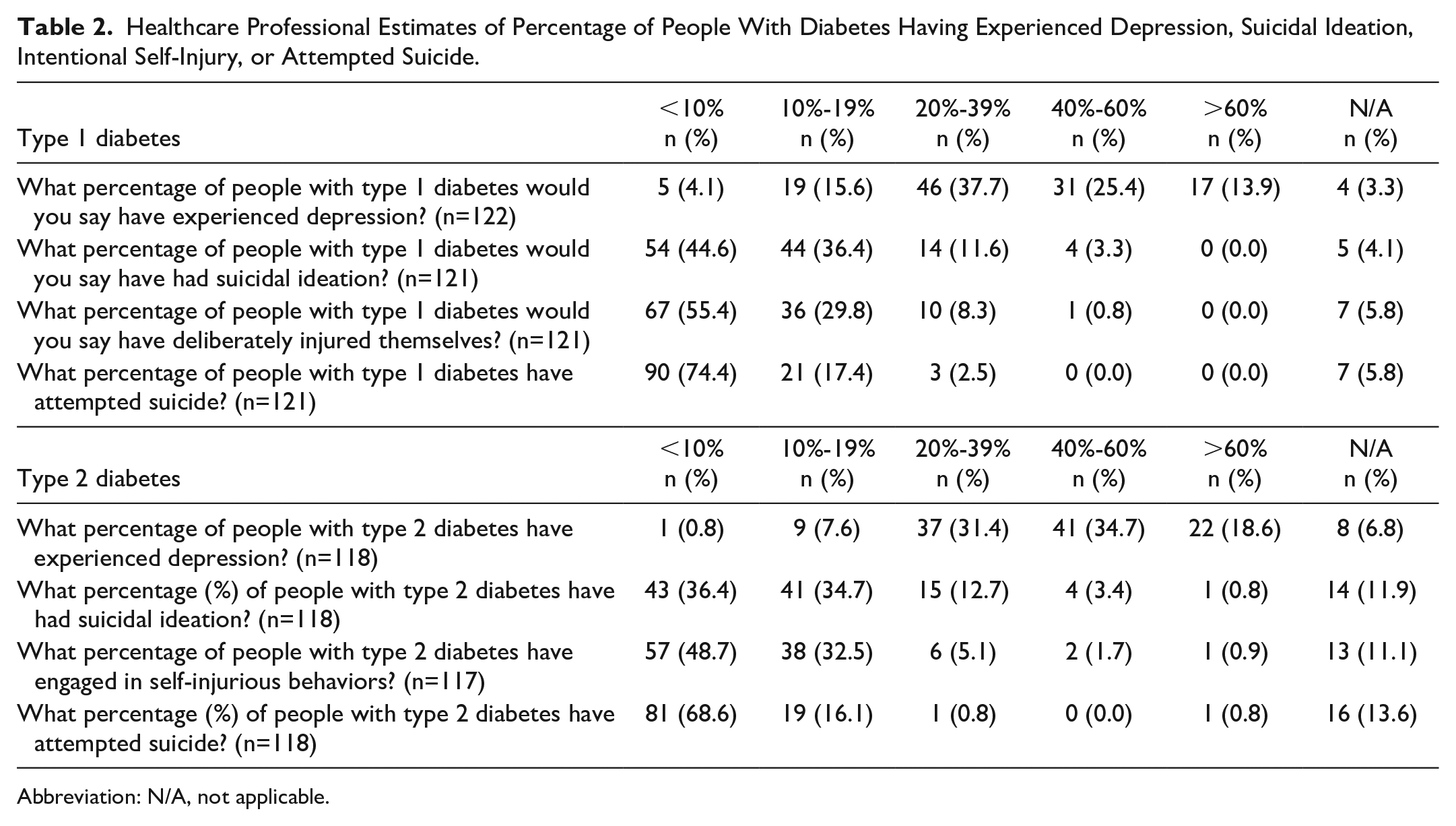
Abbreviation: N/A, not applicable.
Asking PWD Seen in Clinic About ISI and SI
The majority (94.7%) of HCPs believed it was their professional responsibility to ask patients about depression, ISI, or suicide. When asked whether during a routine visit it is appropriate to discuss about depression or SI, 41.6% responded that it was appropriate to have these discussions at every visit, whereas 52.2% believed it was appropriate only during some visits. Whereas 2.7% felt these conversations were not appropriate at routine diabetes visits, the remaining 3.5% stated they did not know. Among HCPs who felt such a discussion was appropriate at some visits, many elaborated in free-text responses that they believed the frequency should vary depending on individual characteristics, such as history of depression or whether the patient shows indications of depression. One commented, “I only discuss depression initially and if a person shows indications, which is probably not frequent enough,” whereas another mentioned a more structured process with the use of depression screening: “At our center we screen starting at age 12. Subsequent frequency is dependent upon score on PHQ-9. Low—annually; Moderate—6 months; High—repeat at next visit in 3 months.”
More HCPs felt moderately comfortable (48.2%) asking patients about whether they have conducted any acts of ISI, and moderately comfortable (43.0%) asking patients whether they have had thoughts of killing themselves. Only 20% of MDs or advanced practice providers felt very comfortable asking about ISI, whereas 26% felt very comfortable asking whether patients have had thoughts of killing themselves. Dietitians and certified diabetes educators (CDEs) were more likely to feel moderately or very uncomfortable asking either question. Those with fewer years of experience in diabetes care were more likely to report feeling very comfortable asking about ISI and SI compared with HCPs with more years of experience working in diabetes care.
The HCPs who felt moderately uncomfortable or very uncomfortable asking patients about ISI or SI were asked to describe in free-text responses why they felt uncomfortable. Responses included feeling that ISI/SI questions are difficult or intrusive to ask, that they did not know how to respond if individuals report concerns, and that they lacked the resources needed to respond. The HCPs who felt moderately uncomfortable or very uncomfortable asking about ISI or SI were further prompted to describe what would help them become more comfortable. Several HCPs expressed a desire for more training or guidance on how to provide support. Several HCPs wrote about needing more resources, including referral pathways or access to mental health professionals.
Training and Resources to Support Individuals Reporting ISI and SI
About one quarter (24.6%) of HCPs reported that they had received specific postgraduate training on how to support patients who may be engaged in ISI or suicidal acts. Approximately, half of them were social workers or psychologists. The remaining professions were less likely to have had training.
Table 3 reports whether HCPs feel they have the resources needed to provide support to those who report depression or SI. About three fourths of HCPs felt they have the resources needed if someone reports concerns about depression during their visit. A similar proportion (74.3%) felt they have the resources needed if someone reports SI during their visit. In the United States, 77.7% felt they had the resources needed to provide support for individuals reporting depression, while 75.5% felt they had the resources needed to provide support for individuals reporting SI. In comparison, the rates in the United Kingdom who felt they had the resources needed were lower (53.8% depression; 53.8% SI). Of all professions surveyed, CDCESs were most likely to report not having the resources needed if someone reported depression (56.3%), and nurses were most likely to report not having the resources needed if someone reports SI (57.1%). More HCPs working in secondary care specialist centers for pediatrics felt they had the resources needed if someone reports depression (85.0%) or SI (83.3%) compared with HCPs practicing in secondary care specialist centers for adults (60.0% and 52%, respectively). The vast majority (95.0%) of HCPs practicing in secondary care specialist centers for pediatrics had access to social workers compared with less than half (44.0%) of HCPs practicing in secondary care specialist centers for adults. Furthermore, a greater proportion of HCPs practicing in secondary care specialist centers for pediatrics reported access to psychologists compared with HCPs practicing in secondary care specialist centers for adults (60.0% vs 32.0%).
Presence of Resources if Depression or Suicidal Ideation is Reported (by Country of Practice, Profession, and Healthcare Setting).
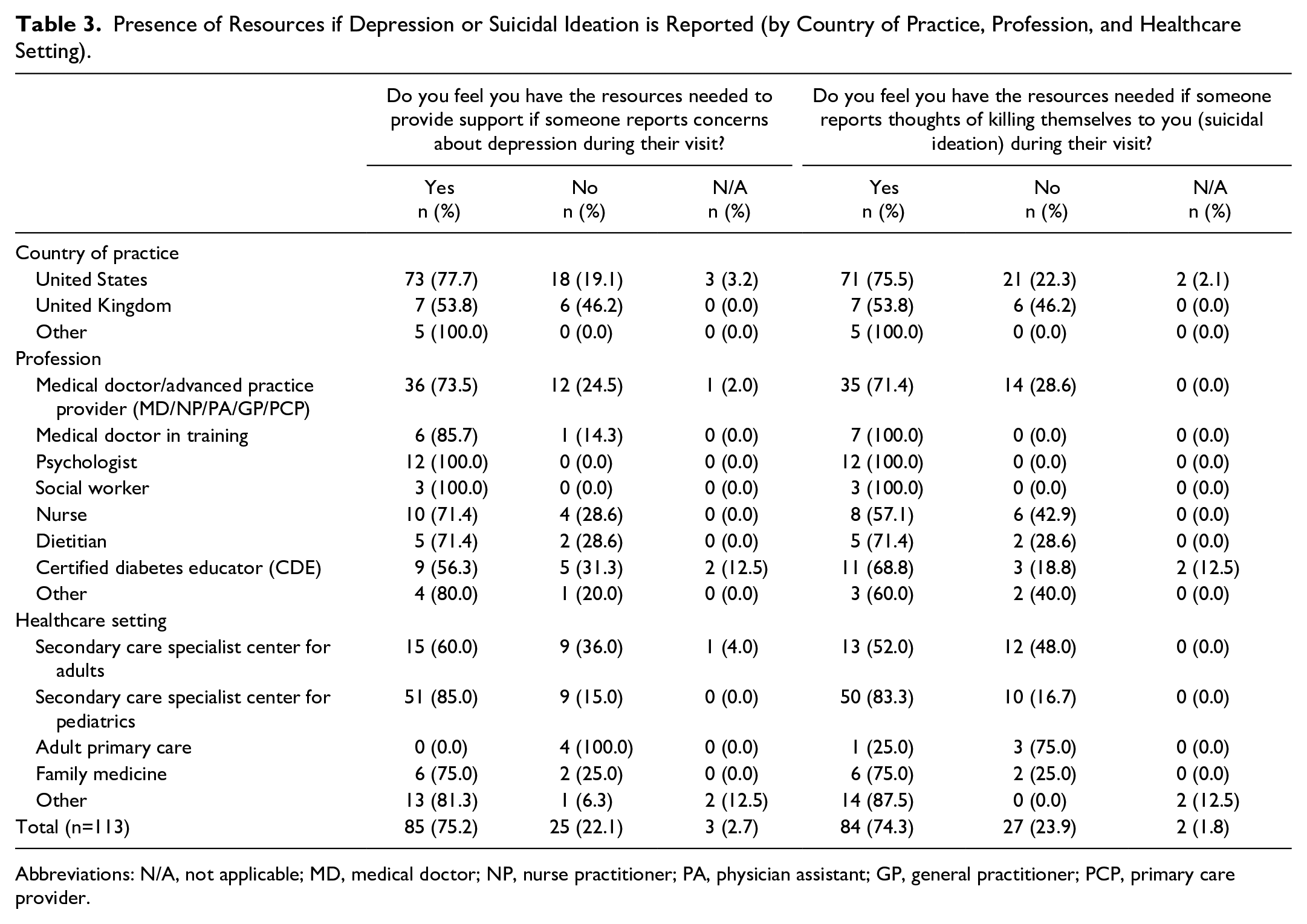
Abbreviations: N/A, not applicable; MD, medical doctor; NP, nurse practitioner; PA, physician assistant; GP, general practitioner; PCP, primary care provider.
The HCPs who felt they did not have the resources needed to provide support if someone reports depression were prompted to specify what resources would be helpful. Referrals or access to mental health professionals were frequently mentioned in free-text responses (77% of those who provided a free-text response). Furthermore, HCPs who reported they did not have resources to address SI felt that on-site or timely access to mental health professionals would be helpful (67% of those who provided a free-text response). When specifically asked which resources respondents felt they needed to adequately help patients who report ISI or SI during their visit, 75% answered “mental health resources,” 71% answered “community support options,” 70% answered “social work in the office/within service,” and 70% answered “psychologist in the office/within service.”
Discussion
This is the first study to date to investigate HCPs’ opinions on depression, SI, ISI, and suicide specifically in diabetes clinics and barriers to care. Previous studies that note mental healthcare concerns in primary care21,22 are echoed here by diabetes HCPs, including difficulty referring to mental health providers, lack of access, and lack of confidence in asking about mental health concerns. Similar to primary care studies, the majority of diabetes HCPs found that it is important to ask about depression and suicide and want to have more training on how to ask appropriate questions, how to quickly assess risk in clinic, and what to do after an individual reports depression or SI. In primary care settings, suicide-related training and education have been associated with improved knowledge and attitudes in working with patients with SI and a perception of greater skill and self-efficacy with working with suicidal individuals,26 -28 which is promising for expansion of this work to diabetes HCPs, especially given that PWD often visit diabetes clinics with more frequency than their primary care providers.
The HCP estimates of the prevalence of depression, SI, and suicide attempts in people with diabetes differed from what has been reported in the literature. Many HCPs believed the proportion who experienced depression to be higher than figures reported in published research, particularly for T2D. In a large systematic review of observational studies, the prevalence of depression in people with T2D was estimated at 28%. 29 However, over half of HCPs believed the percentage of people with T2D who have experienced depression to be 40% or greater. Moreover, many HCPs underestimated the frequency of SI or suicide attempts, particularly among people with T1D. Studies from the literature have estimated the prevalence of SI for people with T1D to be around 15%.5,30 Yet nearly half of HCPs believed that less than 10% of people with T1D had experienced SI. Furthermore, whereas a study of African Americans with T1D found that 13.3% had attempted suicide, 31 three fourths of HCPs believed that less than 10% of people with T1D have attempted suicide. Overall, HCPs seemed to overestimate the prevalence of depression and underestimate the prevalence of SI and suicide attempts among people with diabetes.
Individuals may also choose not to disclose SI with their healthcare team for various reasons, which may lead to HCP underestimation of its prevalence. Stigma and fear of judgment may prevent individuals experiencing SI from speaking with their healthcare providers about these feelings. Stigma toward SI or behaviors can make it difficult for individuals to tell others about suicidal thoughts. 32 Previous experiences receiving negative or judgmental reactions when disclosing SI or behaviors to professionals may undermine willingness to seek help for current concerns. 32 Moreover, people with diabetes who are experiencing SI might not discuss this with their HCPs if they are not aware of the resources that HCPs have available to help them. Overall, the relatively low estimates of SI and suicide attempts reported by HCPs compared with what has been published in the literature highlight the importance of ensuring that HCPs not only have resources available but are also able to identify those in need of support.
The HCPs noted at a high rate (74.3%) that they felt they had the resources needed if someone reports SI during the visit. Further review shows that this was driven more so by pediatric secondary care center respondents (60% of those who felt they had resources). Pediatric secondary care centers also had the highest report of having access to social workers (95% of centers) and psychologists (60% of centers), compared with other healthcare setting respondents. Many (N=79) respondents also noted that the resources they felt necessary to help patients included presence of social workers and psychologists in the office or within their service. This may be one of the reasons behind why respondents felt they had the resources to treat SI and ISI. The HCPs are reporting a clear need for the presence of behavioral healthcare specialists (eg, licensed social workers, psychologists) who can be easily accessible or within the clinic setting to provide appropriate follow-up care needed after positive screening. The presence of integrated behavioral healthcare within diabetes clinics can help patients who are screening positive for mental health comorbidities, including depression, SI, and ISI. To do this, there needs to policy changes and insurance changes to increase the number of trained behavioral healthcare specialists and improve reimbursement for behavioral healthcare in countries that have poor coverage for this type of care.
Most HCPs outside of behavioral health disciplines report not having sufficient training in mental health, which is likely a contributing factor to the discomfort HCPs feel in discussing ISI and suicide with their patients. Those who did feel comfortable had fewer years of experience in diabetes care, which may point toward an increase in emphasis more recently on mental healthcare education as part of healthcare education. This can be a key area of emphasis for improving identification of ISI and SI in patients by providing mental healthcare education (eg, CME) to healthcare providers throughout their training. In addition, HCPs described lack of mental health support as a barrier in discussing ISI and suicide with their patients. The ADA Mental Health Provider Diabetes Education Program 33 has developed a provider directory list of mental health providers with diabetes knowledge. A certificate program has also been created for mental health providers to provide education and guidance on treating PWD, which can help them identify mental health providers who also understand the challenges of managing diabetes. 33
There are clear inequalities among people with diabetes in terms of access to healthcare therapies and technologies.34,35 No data exist on prevalence of ISI or suicide in relation to these inequities in diabetes; greater understanding of these complex issues is crucial to effectively support individuals across all ethnicities, socioeconomic status, and education level, and should be a focus of future research. Future research should focus on qualitative investigation into the experiences of HCPs and how that has potentially affected their care delivery. Novel interventions to aid identification and provide appropriate and timely support to people with diabetes at risk should also be developed.
A key strength of this study is the range of perspectives obtained as HCPs from various professions and practice settings participated. This study also addresses an important issue in diabetes care from a healthcare perspective and identifies important areas where intervention can improve identification and support for people with diabetes. There are limitations to the study as well. Although efforts were made to distribute the survey through existing networks internationally, the study is limited by the online survey and recruitment methods used as they may have limited participation by a larger number of HCPs who do not routinely access the Internet for information such as this. In addition, selection bias is possible as HCPs could choose whether or not to complete the survey. The respondents are a convenience sample, with more female health providers (88%) and white providers (85%) taking the survey. This could affect the generalizability of the results. The survey design may have limited participants’ ability to provide more detailed or nuanced responses, despite free-text options being available for some questions. Respondents were also more likely to be working in an academic center or with National Health Services, so the results may not be as generalizable to those in private practice.
Conclusion
This is the first study to date to investigate HCPs’ perspective on mental healthcare in their patients with diabetes, specifically focused on experiences and barriers to care in depression, SI, ISI, and suicide risk in diabetes clinics. The results show that many HCPs believe that these topics should be asked and discussed in their clinical settings and desire increased knowledge and resources. We are currently conducting a survey of people with diabetes to better understand experiences and to determine unmet support needs from HCPs during routine care. These data, in conjunction with data from the HCP survey will be used to develop interventions and training materials, such as continuing education courses, to better identify and support incidences of depression, ISI, and suicide among this population.
Supplemental Material
sj-docx-1-dst-10.1177_19322968231171616 – Supplemental material for Healthcare Professional Experiences and Opinions on Depression and Suicide in People With Diabetes
Supplemental material, sj-docx-1-dst-10.1177_19322968231171616 for Healthcare Professional Experiences and Opinions on Depression and Suicide in People With Diabetes by Shideh Majidi, Lauren Cohen, Richard I. G. Holt, Mark Clements, Simon O’Neill, Eric Renard, Doug Tynan, Diana Naranjo, Laurel H. Messer, David C. Klonoff and Katharine Barnard-Kelly in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors are deeply grateful to the healthcare professionals who participated in this study.
Abbreviations
ADA, American Diabetes Association; APP, advanced practice provider; CDE, certified diabetes educator; CDCES, certified diabetes care and education specialist; HCP, healthcare professional; ISI, intentional self-injury and self-harm; ISPAD, International Society for Pediatric and Adolescent Diabetes; MD, medical doctor; PWD, persons with diabetes; REDCap, Research Electronic Data Capture; SI, suicidal ideation; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L. H. Messer has received speaking/consulting honoraria from Tandem Diabetes and Dexcom, Inc and also consults for Capillary Biomedical and Beta Bionics. Her institution receives research/project grants from Medtronic, Tandem Diabetes, Beta Bionics, Dexcom, Abbott, and Insulet Corp. R. I. G. Holt received fees for lecturing, consultancy work, and attendance at conferences from the following: Boehringer Ingelheim, Eli Lilly, Janssen, Lundbeck, Novo Nordisk, Novartis, Otsuka, Sanofi, Sunovion, Takeda, and MSD. E. Renard has received speaking/consulting honoraria from A. Menarini Diagnostics, Abbott, Adelia Medical, Air Liquide SI, Astra-Zeneca, Asten, Bastide Médical, Becton-Dickinson, Boehringer-Ingelheim, Cellnovo, Dexcom Inc, Eli-Lilly, Hillo, Insulet Inc, Johnson & Johnson (Animas, LifeScan), Medtronic, Medirio, Nestlé Home Care, Novo-Nordisk, Orkyn, Roche, Sanofi-Aventis, and VitalAire, and received research support from Abbott, Dexcom Inc, Insulet Inc, Roche, and Tandem.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.