
Abstract
Background:
The COVID-19 pandemic necessitated rapid implementation of continuous glucose monitoring (CGM) in the intensive care unit (ICU). Although rarely reported, perceptions from nursing staff who used the systems are critical for successful implementation and future expanded use of CGM in the inpatient setting.
Methods:
A 22-item survey focused on CGM use was distributed to ICU nurses at two large academic medical centers in the United States in 2022. Both institutions initiated inpatient CGM in the spring of 2020 using the same CGM+point of care (POC) hybrid protocol. The survey employed a 1- to 5-point Likert scale regarding CGM sensor insertion, accuracy, acceptability, usability, training, and perceptions on workload.
Results:
Of the 71 surveys completed, 68 (96%) nurses reported they cared for an ICU patient on CGM and 53% reported they had independently performed CGM sensor insertion. The ICU nurses overwhelmingly reported that CGM was accurate, reduced their workload, provided safer patient care, and was preferred over POC glucose testing alone. Interestingly, nearly half of nurses (49%) reported that they considered trend arrows in dosing decisions although trends were not included in the CGM+POC hybrid protocol. Nurses received training through multiple modalities, with the majority (80%) of nurses reporting that CGM training was sufficient and prepared them for its use.
Conclusion:
These results confirm nursing acceptance and preference for CGM use within a hybrid glucose monitoring protocol in the ICU setting. These data lay a blueprint for successful implementation and training strategies for future widespread use.
Introduction
Uncontrolled blood glucose levels contribute to high morbidity, mortality, and health care costs in the inpatient setting.1 -8 Hypoglycemia is of particular concern and is associated with prolonged hospitalization, high hospital costs, increased inpatient mortality, and high 30-day readmission and post discharge mortality.9,10 The current state of glycemic control in the hospital has widespread implications, given that, currently, 1 in every 4 patients admitted to the hospital has a history of diabetes, 11 with inpatient rates likely to rise as outpatient diagnosis of diabetes continue to climb. 12
Point of care (POC) glucose monitoring has been the standard of care in the inpatient setting for more than 40 years. 13 In stark contrast, glucose monitoring in the outpatient setting is increasingly transitioning to continuous glucose monitoring (CGM). 14 The POC glucose monitoring has advantages in the inpatient setting, including the general ease at which one can interpret discrete glucose values, wide adoption, and accuracy among critical care hospital meters. 15 However, there are significant drawbacks to POC glucose monitoring in the hospital setting, including the painful nature of the procedure for the patient, as well as the time-consuming practice for hospital staff.16,17 The POC glucose monitoring has also demonstrated failure to detect hyperglycemia and hypoglycemia due to the intermittent nature of monitoring. 18 In addition, whereas adoption of POC by health systems has been widespread, frequent missed POC testing and mistiming of POC testing are pervasive issues in the inpatient setting and can lead to improper and missed insulin dosing. In the intensive care unit (ICU), missed or delayed glucose testing is associated with increased hypoglycemia risk during intravenous (IV) insulin infusion, even with the use of computerized algorithms,19,20 whereas more frequent testing may improve overall glucose control.21,22
The COVID-19 pandemic created a need for remote glucose monitoring within inpatient hospital settings, and thus provided the opportunity to examine hospital glucose monitoring solutions beyond standard of care POC testing. In April 2020, the FDA announced that it would not object to the use of CGM systems in the hospital setting to support COVID-19 health care–related efforts, thus opening the door to CGM use in the inpatient setting.23,24 The use of inpatient CGM during the pandemic provided valuable evidence supporting the overall safety of CGM and demonstrated similar glucose control as the standard of care in hospitals.25 -30 In addition, rapid clinical deployment of CGM provided an opportunity to examine implementation strategies, supports, and outcomes. At the authors’ institutions, a similar hybrid CGM and intermittent POC glucose monitoring protocol was implemented for critically ill patients with COVID-19 who were receiving IV insulin. 31 Within the protocol, POC measures were obtained hourly during initial validation, then every 6 hours for ongoing validation. 31 The hybrid protocol was paired with a tailored staff training program for successful deployment and sustained use at both institutions.27,31 A preliminary assessment (N=9) of nursing staff perceptions suggested a high degree of acceptance, a perceived improvement in workload and reduction of burden, and a desire for continued and widespread use of CGM in the future. 31
There is substantial need for continued examination of implementation strategies, barriers, and facilitators for successful long-term use of CGM in the hospital setting. 32 Glucose monitoring has long been in the purview of nursing and nursing perspectives on current CGM use during the COVID-19 pandemic will inform future widespread implementation. We report here results from a 22-item survey focused on CGM use perspectives by critical care nursing staff across multiple institutions.
Methods
Institutions and Population Description
The study was conducted at The Ohio State University Medical Center and Grady Memorial Hospital, two large academic medical centers in the United States (hereafter referred to as hospitals A and B, respectively). Both institutions initiated inpatient CGM in the spring of 2020 during the COVID-19 pandemic using the same CGM+POC hybrid protocol. Institution A’s medical intensive care unit (MICU) houses 48 critical care beds and employs 152 staff nurses. Institution B has 30 critical care beds and employs 115 staff nurses. The study was approved at the institutional review boards from both academic centers.
Description of CGM Implementation
A comprehensive approach to CGM implementation based on the principles of implementation science was used across the two institutions. Evidence-based strategies from the field of implementation science were selected and tailored at each site based on existing resources and organizational structures. 33 Implementation strategies included stakeholder and leadership engagement; use of educational materials, meetings, and outreach visits; ongoing training; identification of local champions; use of train-the-trainer strategies; establishing a coalition to support implementation; changing the physical structure and equipment in the unit; auditing and feedback; and creating mechanisms to facilitate relay of real-time clinical data to providers. These strategies were operationalized first at institution A, and then used to guide implementation at institution B.
At institution A, implementation was conducted in a scaffolded approach in which nurse practitioners on the diabetes consult service initially trained nursing leaders (ie, nurse managers and clinical nurse specialists) on use of the technology, including CGM sensor insertion, transmitter placement, pairing with receiver/phone, and CGM glucose and trend displays. Upon patient selection, nurse leaders placed CGM devices and then provided one-on-one bedside training for the staff nurse providing patient care. The staff nurse received training on CGM glucose and trend displays, institution-specific electronic health record (EHR) documentation, and CGM+POC hybrid protocol. Staff nurses then trained the incoming nurse at shift change. Nurse leaders huddled daily to address questions and reinforce technology use and protocol fidelity. A detailed description of training at institution A has previously been published. 31 The use of a scaffolded approach allowed training to be conducted very rapidly because only a small group of nurse leaders was required to receive full CGM use training. At institution A, an educational strategy was crafted, materials were created, and nurse leaders were trained in a 2-week period leading up to the initiation of clinical CGM use.
At institution B, implementation procedures modeled those from institution A. Leaders and champions from institution A assisted institution B as they initiated CGM. Members leading training and implementation at institution A met with a core team at institution B and provided insights and training material that have previously been described. 27
The training approach at institution A evolved over time as nurses gained familiarity with CGM. By December 2020, CGM training was incorporated into MICU nursing annual competencies and routine care procedures. All MICU staff nurses received training on CGM placement, use, and the CGM+POC protocol. This evolution allowed staff nurses in the MICU to independently initiate CGM and operate CGM systems as routine care.
Instrument
To evaluate nurses’ acceptance and perspectives of CGM and hybrid protocol use during this implementation period, a 22-item survey was developed (Appendix A). Five items gathered information on nursing tenure and CGM level of experience. Seventeen items utilized a 1- to 5-point Likert scale and were aimed at gathering information on perceived accuracy, workload, acceptability, and usability.
The survey was completed by a total of 71 MICU staff nurses, including 51 nurses at institution A and 20 nurses at institution B. Nurses who had cared for MICU patients using CGM were invited to complete the anonymous questionnaire that was distributed using a REDCap survey link sent through email. The survey was distributed to all 152 MICU staff nurses at institution A in February 2022, approximately 20 months following initial use of CGM. Informed consent was obtained prior to completion of the survey. The survey was distributed to all 115 MICU staff nurses at institution B in May 2022.
Statistical analyses
Demographic and CGM survey data were analyzed using STATA 12.0 (College Station, TX, USA). Descriptive statistics were used to summarize nurses’ responses. In addition, t test/analysis of variance (ANOVA) and chi-square statistics were performed to examine differences between groups.
Results
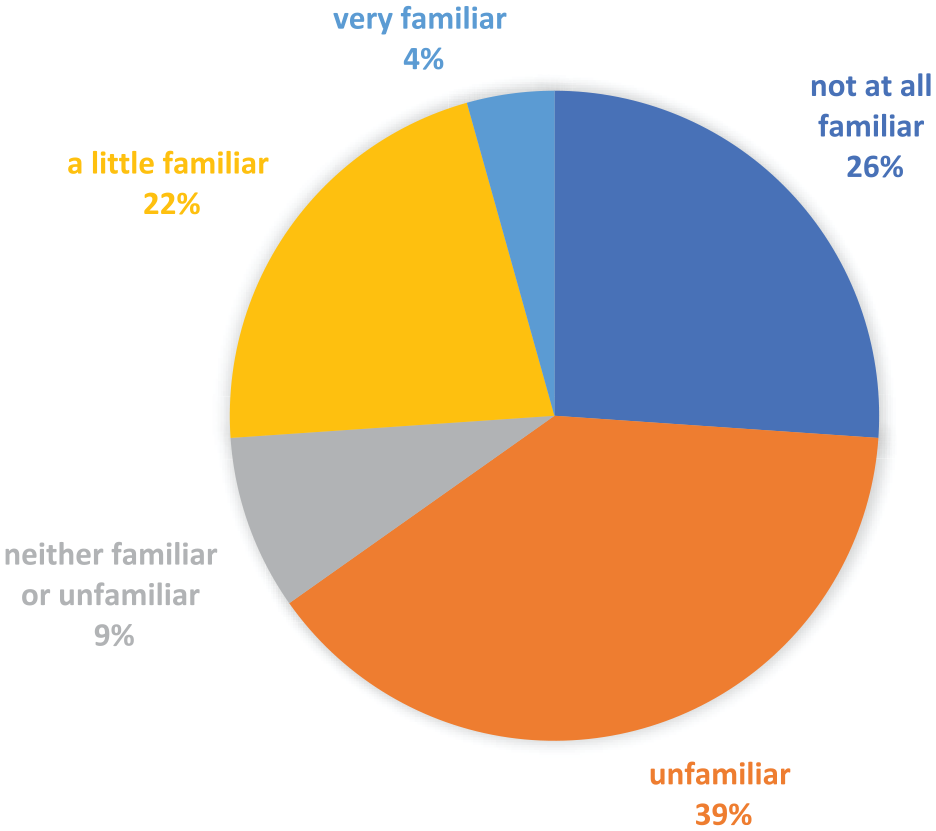
A total of 71 MICU nurses completed the survey, including 51 nurses from institution A and 20 nurses from institution B. Three nurses indicated they had never cared for a patient on CGM and therefore did not complete the remainder of the survey. Participants had a mean 10.6 years of nursing experience (range, 1-38 years); (10.8 years [range, 1-37 years], 11.8 years [range, 1-38 years], institution A and B, respectively) and 7.1 years of ICU nursing experience (range, 1-30 years); (7.7 years [range, 1-30 years], 7.0 years [range, 1-27 years], institution A and B, respectively). Among the staff nurses who had cared for patients on CGM (n=68), 43% (n=29) had cared for patients on CGM during >10 shifts, 19% (n=13) on 7 to 10 shifts, 22% (n=15) on 4 to 7 shifts, and 16% (n=11) for only 1 shift. Nurses had a low degree of previous exposure to CGMs, with 65% (45/69) reporting they were previously either “unfamiliar” or “not at all familiar” with CGM technology (Figure 1).
Nurses felt well trained and prepared to use continuous glucose monitoring.
Use of CGM
Of the nurses surveyed, 53% (31 nurses [62%] at institution A, 5 nurses [29%] at institution B), t(65) = 2.4, P = .020, reported they had independently performed CGM sensor insertion. Of these nurses who started a sensor, 77% (23/30) did not believe the process was difficult at institution A, whereas, only 40% (2/5) of nurses at institution B believed the process was not difficult, t(33) = −1.4, P = .176. When asked whether they were able to use the CGM glucose values as a replacement for POC glucose, 94% (64/68) agreed or strongly agreed with the statement. The majority of nurses at both institutions (81%, 57/70), found the process of documenting CGM glucoses in the EHR to be easy. Results on the use of trend arrows to make dosing decisions were mixed, with nearly half of nurses (49%, 33/67) reporting they did consider use of trend arrows in dosing. Interestingly, nurses at institution B reported they were more likely to consider use of trend arrows in their insulin dosing decisions: 76% (13/17) versus 40% (20/50) at institution A, t(65) = −2.6, P = .013.
Continuous Glucose Monitoring on Workload
The overwhelming majority of nurses at both institutions, 92% (61/66), felt that CGM reduced their workload. Similarly, 93% (62/67) of nurses reported that the use of CGM reduced the frequency of their entrances into the patient room.
Acceptance of CGM
Nearly all nurses, 93% (65/70), reported that they preferred to use a hybrid CGM plus POC rather than POC testing alone and 97% (68/70) indicated that they would like to use CGM in their non-COVID MICU patients. Nurses felt CGM improved the care of their patients (90% [63/70]) and felt that using CGM along with POC testing made their patients safer (89% [62/70]). Perceived accuracy was very high at both institutions, with 93% (62/67) reporting they felt the CGM system to be very good. Nurses with more years of experience and those with more ICU experience were more likely to prefer hybrid CGM over standard of care POC alone (R=0.6401 and R=0.4712, respectively). In addition, nurses who cared for patients on more shifts were more likely to prefer CGM χ2(12, N=70) = 21.1, P = .049 and more likely to feel CGM made their patients safer χ2(8, N=70) = 18.6, P = .017.
Continuous Glucose Monitoring Training
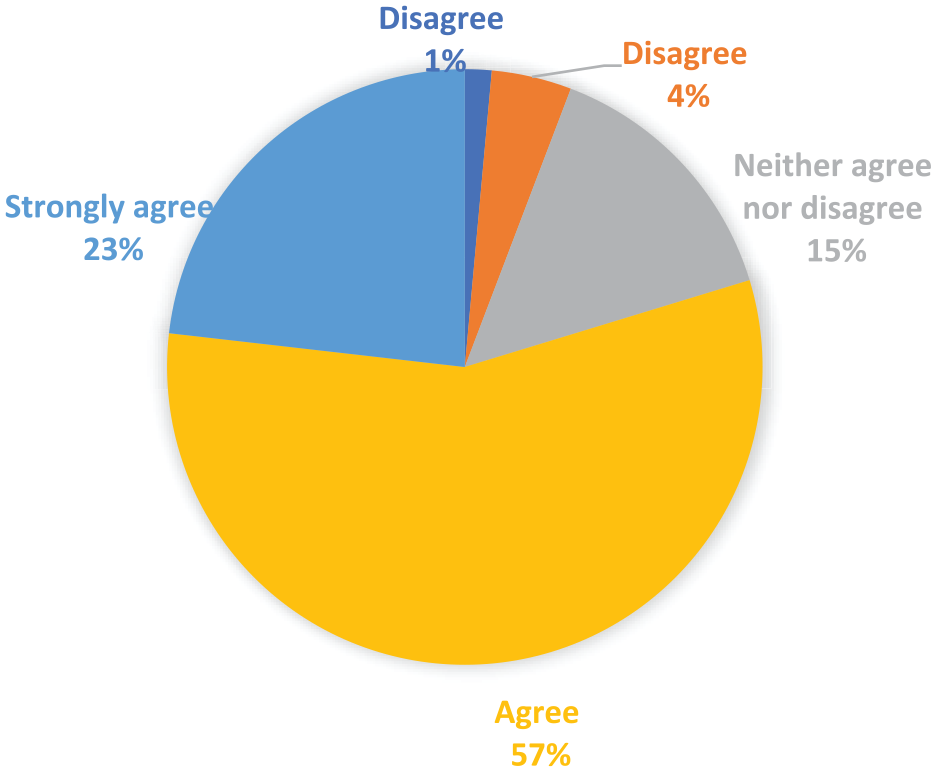
Nurses reported receiving training through multiple modalities, including from their MICU-certified clinical nurse specialist (CNS) or nurse manager (74%), from another staff nurse who was familiar with the CGM systems and protocol (60%), by reading the protocol and training materials (51%), from an MICU charge nurse (14%), and from online/app videos (14%; Figure 2). Reported education did significantly differ by institution, with 49% (25/51) reported receiving training as part of their annual nursing competencies at institution A versus only 12% (2/17) at institution B (P = .0019; Figure 2). When asked about the total amount of time they had received in training, 47% (33/70) of nurses believed they received approximately 15 to 45 minutes of training, whereas 34% (24/70) stated they had received 10 to 15 minutes of training (Figure 3). Nurses at institution A reported they received more time in training than institution B (P = .2303). The vast majority, 80% (55/69), of nurses believed the CGM training they received was sufficient and had prepared them to use the CGM and the Hybrid CGM+POC protocol (Figure 4).
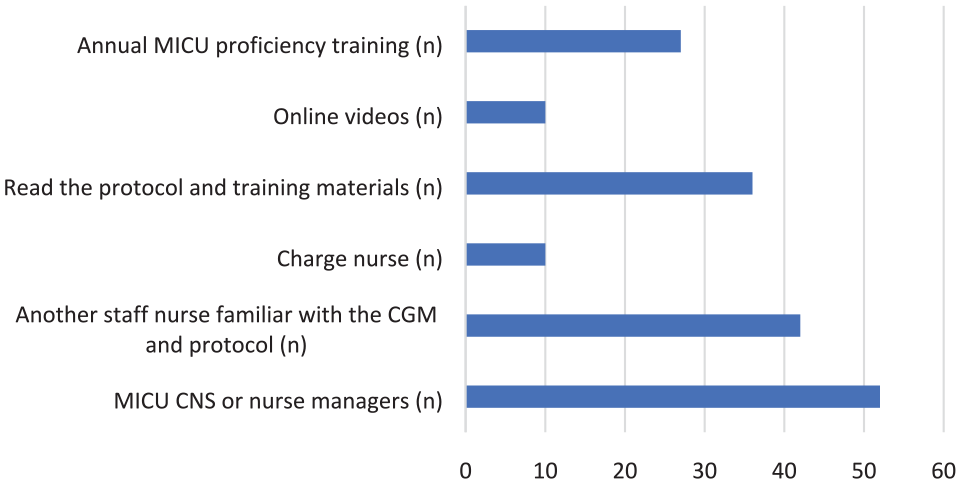
How nurses received CGM training.
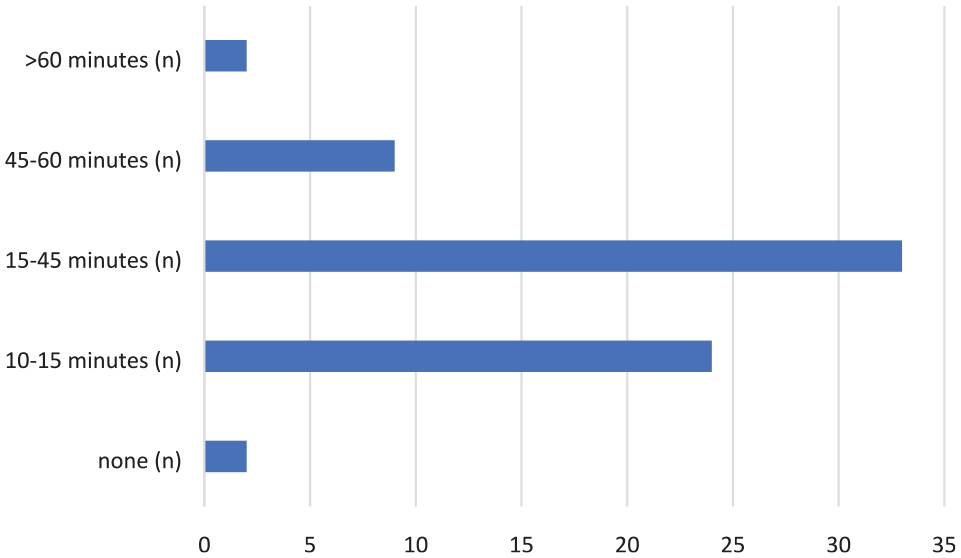
Nursing time spent training.
Nursing familiarity with CGM prior to utilizing CGM hospital protocol.
Discussion
This multisite study presents novel findings regarding use of a hybrid CGM+POC glucose monitoring protocol in a critical care environment. Nursing acceptance of CGM as an alternative to POC testing was very high and there was a strong desire at both institutions for continued use of CGM and expansion to non-COVID-19 populations. This sentiment was likely aided by a high degree of perceived CGM accuracy and a general perception that CGM decreased nursing workload.
The use of a similar hybrid protocol combining CGM+POC glucose monitoring at both institutions presented the opportunity to examine additional organizational differences in implementation of CGM, including protocol and CGM training. Training differed between institutions, with institution A adopting nursing education over time, transitioning from a scaffolded educational approach to incorporation of full CGM training into MICU annual nursing competencies. The differences in training likely influenced some differences seen in nursing use of the system between the two institutions. More nurses at institution A reported performing sensor insertion and set up, 62% compared with 29% at institution B. This is not surprising, given that nurses at institution A received training specific to independent sensor insertion and CGM start-up. In addition, of the few nurses who did perform sensor insertion at institute B where insertion-specific training was not provided, only 40% found the process to be easy, compared with 77% at institution A. Few other studies have mentioned training specifically on CGM sensor application.34,35
Nurses’ use of trend arrows was of particular interest, especially given the fact that neither institution formally trained nurses on their use and the hybrid protocol did not incorporate the use of trend arrows. In previous work by Wollersheim (2016), glucose trends were included in nursing training and protocol design. 36 Despite the lack of formal training on trend arrows at institution A or institution B, nearly half (49%) of nurses reported that they considered trend arrows in their dosing decisions. Interestingly, institution B uses an insulin titration software for IV insulin, meaning nurses are not independently titrating IV insulin doses. It is therefore possible that nurses at institution B were using trend arrows when administering subcutaneous correction or prandial insulin doses rather than in the titration of IV insulin. However, this detail was not solicited in the questionnaire. Nurses’ organic use of trend data in dosing decisions deserves further inquiry as their formal inclusion in dosing guidelines could improve glycemic control in the future.
Despite the incorporation of CGM training into annual MICU competencies at institution A, the most cited modes of training were still training from nursing leaders (74%), closely followed by training from another staff nurse with CGM experience (60%). In fact, only 49% of nurses at institution A reported their annual competencies as a source of training. It may be that nurses at institution A had built a strong knowledge of CGM over the initial 6 months of use prior to the incorporation of training into annual competencies and, therefore, felt their training had been solidified in other ways, or it may be that formalized training was perceived to be less effective than informal bedside just-in-time training. Other studies have found just-in-time training to be highly effective in the ICU environment.37,38 Leopold (2016) incorporated just-in-time sessions along with group education into nursing training for a clinical trial on the use of a microdialysis-based CGM system. 39
The amount of time nurses received for CGM training differed between institutions, with 47% of nurses at institution A more likely to report receiving 15 to 45 minutes of training, whereas 50% of nurses at institute B reported receiving 10 to 15 minutes of training. Certainly, the addition of training to nursing annual competencies could explain the discrepancy in overall training time. Despite the differences in training time and modalities, nurses as both institutions overwhelmingly (80%) felt the training they had received sufficiently prepared them to use CGM and the hybrid protocol. These data certainly provide insights into a broad spectrum of CGM training modalities; however, additional systematic inquiry is needed on training approaches and how these approaches and modalities may differ by institutional type and resources. Despite such differences in training approaches, overall satisfaction with the technology was high at both institutions. It is also important to note that both institutions are large academic medical centers with established dedicated endocrinology/diabetes consult services. Although the specific influence of these services and embedded experts was not studied, their likely contribution to successful implementation should be underscored. For example, institution B also included remote monitoring by endocrinology for all patients; the support of the subspecialty team on the nursing staff perspectives was not assessed. Therefore, these data may not be generalizable to nonacademic health systems or rural hospitals. There is substantial need for data examining implementation factors and use across a diverse group of health systems and hospitals.
Intrinsic limitations to this type of report include potential participation, selection, and recall bias. In addition, the questionnaire was created to specifically evaluate CGM use in a novel inpatient environment, and therefore was not a validated measure. This survey was, however, anonymous, delivered to all nurses, and was conducted in a time where patients with COVID-19 were still being admitted at both institutions. The survey was distributed to all MICU nurses; however, only nurses who cared for patients on CGM were asked to complete the survey. While this likely limited the pool of respondents, we do not know the actual number of nurses who cared for patients on CGM and therefore it is difficult to gauge a true response rate.
Conclusion
The insights obtained from this analysis provide very relevant information related to CGM implementation and use by nursing staff in critical care units. This technology was not previously used in the ICU before COVID-19 and its rapid adoption with high levels of satisfaction speak to the promising potential of diabetes technology to transform inpatient diabetes care, affecting positively both patients and hospital staff.
Footnotes
Abbreviations
CGM, continuous glucose monitoring; CNS, clinical nurse specialist; EHR, electronic health record; ICU, intensive care unit; IV, intravenous; MICU, medical intensive care unit; POC, point of care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.F. discloses research support with Dexcom Inc and Insulet; and honorarium from Medscape. K.D. discloses research support from Novo Nordisk, Sanofi, Viacyte, and Abbott; consulting with Eli Lilly, Novo Nordisk, Boehringer Ingelheim, Insulet, and Tolerion; and honorarium from UptoDate, Medscape, and Elsevier. F.J.P. discloses unrestricted research support from Insulet, Dexcom, and Ideal Medical Technologies; and personal fees from Boehringer Ingelheim, Dexcom, and Medscape for consulting activities.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.