
Abstract
Objective:
The primary objective of this analysis was to compare the safety and efficacy of a novel computerized insulin infusion protocol (CIIP), the Lalani Insulin Infusion Protocol (LIIP), with an established CIIP, Glucommander.
Methods:
We conducted a 10-month retrospective analysis of 778 patients in whom LIIP was used (August 18, 2020 to June 25, 2021) at six HonorHealth Hospitals in the Phoenix metropolitan area. These data were compared with Glucommander that was used at those same hospitals from January 1, 2018 to August 17, 2020, n = 4700. Primary end points of the project included average time to euglycemia and average time in hyperglycemia (>180 mg/dL) and hypoglycemia (<70 mg/dL). Additional subgroup analysis was done to evaluate CIIP performance in patients in whom maintenance of euglycemia was more challenging.
Results:
The LIIP had a faster time to euglycemia (191 vs 222 minutes, P < .001) and similar time in hypoglycemia (2.79 vs 2.76 minutes, P = .50) for all patients, when compared with Glucommander. Similar observations were made for the following subgroups: diabetic ketoacidosis/hyperosmolar hyperglycemic state (DKA/HHS) patients, COVID-19 patients, patients on steroids, patients with ≥60 glomerular filtration rate (GFR), patients with renal insufficiency, and patients with sepsis.
Conclusions:
The LIIP is a safe and effective CIIP in managing intravenous insulin infusion rates. Utilization of LIIP resulted in reduced time to euglycemia, P < .001, when compared with Glucommander and did not cause increased hypoglycemia during the project period. Contributing factors to the success of LIIP may include improved clinical workflow, learnability and ease of use, compatibility with the Epic electronic health record (EHR), and its unique, dynamic and adaptive algorithm.
Keywords
Introduction
Hyperglycemia in the critical care setting is associated with increased mortality, and morbidity, including prolonged hospital stay, higher infection rates, and an increased incidence of complications.1,2 Whereas it seems intuitive that patients with diabetes are at risk for hyperglycemic incidents while in the intensive care unit (ICU), patients without diabetes also experience hyperglycemia and its associated negative sequelae. Hyperglycemia in people with and without diabetes may occur because of metabolic and hormonal derangement, and catecholamine release associated with surgery, trauma, stroke, or other stressors. Medications used in the ICU setting may also cause hyperglycemia, including glucocorticoids, inotropes, and vasopressors. Enteral or parenteral nutrition in the critical care setting also affects blood glucose (BG) levels and may contribute to either hyperglycemia or hypoglycemia. 3
To avoid adverse outcomes associated with hyperglycemia in the ICU, it is ideal to carefully control BG levels in critical care patients.2,4 This can be challenging because BG levels in this population tend to be labile because of the severity of illness. In addition, variability in nutritional intake and timing of insulin administration in the ICU may also contribute to lability. This creates challenges to the maintenance of BG levels within the target euglycemic range while avoiding hypoglycemia.5,6 Intravenous (IV) insulin is often preferred over the subcutaneous form in the critical care setting because of its rapid onset and shorter duration of action, allowing for rapid titration and dosing flexibility as glucose levels fluctuate. 7 IV insulin is indicated for glycemic control in a number of clinical scenarios, including hyperglycemia before and after surgery, acute renal failure with hyperglycemia, hyperosmolar nonketotic diabetic coma, diabetic ketoacidosis (DKA), steroid-induced hyperglycemia and the treatment of fluctuating glucose concentrations in insulin-requiring people with diabetes, who have a concomitant infection, requiring hospital admission and IV antibiotic treatment, among others. 8
This project pays particular attention to a new, but now familiar, subset of patients: COVID-19 ICU patients. These patients experience high stress, resulting in stimulation of the hypothalamic-pituitary-adrenal axis and are at increased risk for hyperglycemia. Hyperglycemia in these patients may increase morbidity and mortality because of an impaired immune system and endothelial dysfunction, thereby reducing antioxidant generation in the lungs, and increasing oxidative stress and apoptosis. 9 Therefore, careful glucose management in COVID-19 patients with hyperglycemia through IV insulin therapy is imperative to the reduction of mortality and morbidity and to achieve improved patient outcomes. 10
Because of the inherent difficulty in achieving and maintaining euglycemia, while avoiding hyperglycemia and hypoglycemia, standardized IV insulin infusion protocols (IIIP) are appropriate to reduce glycemic oscillation, and IIIPs also enhance adherence to accepted insulin infusion practices. 11 When such protocols are used, BG concentrations must be measured often, and insulin rates must be adjusted to allow for the maintenance of BG levels in a predetermined range. The IIIP can be paper-based (calculation or nomogram-driven manual protocols) or computerized. Paper-based protocols relying on manual nursing calculations in response to each BG reading can be complex and demand more nursing time and resources than computerized protocols. Computerized protocols have demonstrated a reduction in dose calculation errors due to their ability to eliminate the need for manual calculations, which are prone to human error in paper-based protocols. 12
Studies have shown that, compared with paper-based protocols, computerized insulin infusion protocols (CIIPs) lead to a reduction in time to euglycemia, increased percentage of BG levels within desired range, increased time in desired BG range, and improved clinical workflow without increased risk of hypoglycemia.13 -16 Therefore, institutional implementation of CIIPs in the ICU has increased in recent years. Factors such as electronic health record (EHR) integration, refinements to protocol design to reduce hypoglycemia, and clinical staff training can enhance the benefits of a CIIP.17 -19 Notably, there have been no prior studies comparing patient performance and work staff experience between two distinct CIIPs. 20
The Lalani Insulin Infusion Protocol (LIIP; Endocrine Technologies, Scottsdale, AZ) is a novel CIIP in its commercial prelaunch phase. In its initial phase, LIIP determines optimal insulin infusion rates, using patient characteristics such as body mass index (BMI) and point of care (POC) BG levels. After initiation, LIIP uses an adaptive algorithm to respond to the patient’s insulin sensitivity and adjusts insulin infusion rates accordingly. HonorHealth is a healthcare network with six major hospitals in the greater Phoenix metropolitan area, and it serves a diverse patient population. On average, 30% to 50% of hospitalized patients have diabetes as a primary or secondary diagnosis. Before the introduction of LIIP, the HonorHealth six-hospital network used Glucommander (GC; Glytec, Greenville, SC, USA), a commercially available, cloud-based insulin dosing software. This project aimed to compare the safety and efficacy of LIIP and GC for inpatient IV insulin use. To this end, we carried out a retrospective analysis of 778 patients in whom LIIP was used during an approximate time of 10 months from August 18, 2020 to October 15, 2021. The 10-month data collection time frame was selected to provide an adequate sample to carry out statistical comparisons. For a two-tailed, between-group comparison test with an alpha of .001 (corrected for multiple comparisons), Cohen d of 0.20, power of 0.95, and allocation ratio of .165, a minimum of 5016 cases were needed (4306 and 710 for each group, respectively). These data were compared with GC (January 1, 2018 to August 17, 2020, n = 4700). In addition to comparing outcomes of all patients, we carried out subgroup analyses of clinically complex patient types with varying degrees of renal dysfunction.
Methods
Algorithm Design and Implementation Within Electronic Medication Administration Record (eMAR)
The LIIP is a CIIP designed for use in patients aged 18 years and older who weigh more than 45 kg and consists of two phases in which insulin infusion rates are optimized. In the induction phase, the initial insulin infusion rate is determined based on previously obtained bedside monitoring BG levels and patient weight. Thereafter, LIIP uses a formula that incorporates recent insulin drip rates and BG levels to determine insulin sensitivity and adjusts the insulin infusion rate accordingly. The LIIP permits rapid correction in insulin infusion rates based on specific metabolic needs and is therefore appropriate for critical care patients. Glucommander is a cloud-based insulin dosing system that has been shown to safely and effectively achieve near normoglycemia in hospitalized patients receiving IV insulin. 21 On August 18, 2020, the HonorHealth hospital network made the transition from GC to eMAR integrated LIIP.
Project Methods
We conducted a retrospective analysis of 778 patients in whom LIIP was used from August 18, 2020 to June 25, 2021 at six HonorHealth Hospitals in Arizona. These data were compared with GC (January 1, 2018 to August 17, 2020, n = 4700). This analysis included all patients in the ICU requiring IV insulin therapy for hyperglycemia management during the study period. Before August 18, 2020, HonorHealth Hospitals exclusively used GC for IV insulin dosing. On August 18, 2020, HonorHealth Hospitals switched to using LIIP as their sole IV insulin dosing software. For analysis, euglycemia was defined as glycemic concentrations between 70 and 180 mg/dL. Primary end points include time to euglycemia and time in hypoglycemia. All POC BG obtained at hourly intervals during the insulin run were extracted from the EHR and displayed and reported on a Microsoft Power BI dashboard. In addition to analyzing the broader patient populations receiving IV insulin during the given time interval, patients were divided into subgroups based on their primary diagnosis, renal function, and steroid usage. The following subgroups were analyzed: DKA/hyperosmolar hyperglycemic state (HHS) Patients, COVID-19 Patients, patients on steroids, patients with varying degrees of renal dysfunction, and patients with sepsis. Steroid use was defined as administration of parenteral or oral glucocorticoids throughout the period of IV insulin therapy. Renal insufficiency was defined as a glomerular filtration rate (GFR) value below 60 mL/min at the start of IV insulin therapy.
Statistical Methods
Using a convenience sample, this retrospective causal comparative investigation evaluated differences in patients’ time to euglycemia, time in euglycemia, hypoglycemia, and hyperglycemia between patient groups managed through the GC and LIIP. Subgroup analyses included comparisons of time to euglycemia and time in hypoglycemia across patients with ≥60 GFR, renal insufficiency, sepsis, COVID-19, undergoing steroid treatment, and diabetic ketoacidosis, and hyperosmolar hyperglycemic syndrome. Chi-square was used to evaluate the observed frequency of time in euglycemia between groups, and independent measures t tests and z tests (for known variances) were used to evaluate differences in average times between groups. All data were extracted, entered, and analyzed using IBM SPSS Version 27. Data were evaluated and met parametric statistical test assumptions. The alpha level was set at .05, and the Bonferroni adjustment was applied (.05 / 16) to correct the experiment-wise error rate for multiple tests resulting in an adjusted alpha of .00312.
Results
All Patients
Prior to the implementation of LIIP, hospitalized patients receiving IV insulin using GC reached euglycemia in 222 minutes on average. During the 10-month period following LIIP’s integration within the eMAR of the HonorHealth Hospital network, patients in the LIIP group achieved euglycemia faster (mean = 191, SD = 43.5) than those patients in the GC group (mean = 222, SD = 64.5), 6258) = 37.52, P < .001 (Figure 1a). In addition, patients in the LIIP group spent significantly less time in hyperglycemia (mean = 187, SD = 71) than those in the GC group (mean = 211, SD = 64.5), t(6, 258) = 12.24, P < .001 (Figure 1b). No differences were observed in percentage of time in euglycemia between groups, χ2(1, N = 6258) = 0.089, P = .77, and there was no significant difference in average time between patient groups in hypoglycemia, t(6258) = 0.67, P = .50 (Figure 1c).
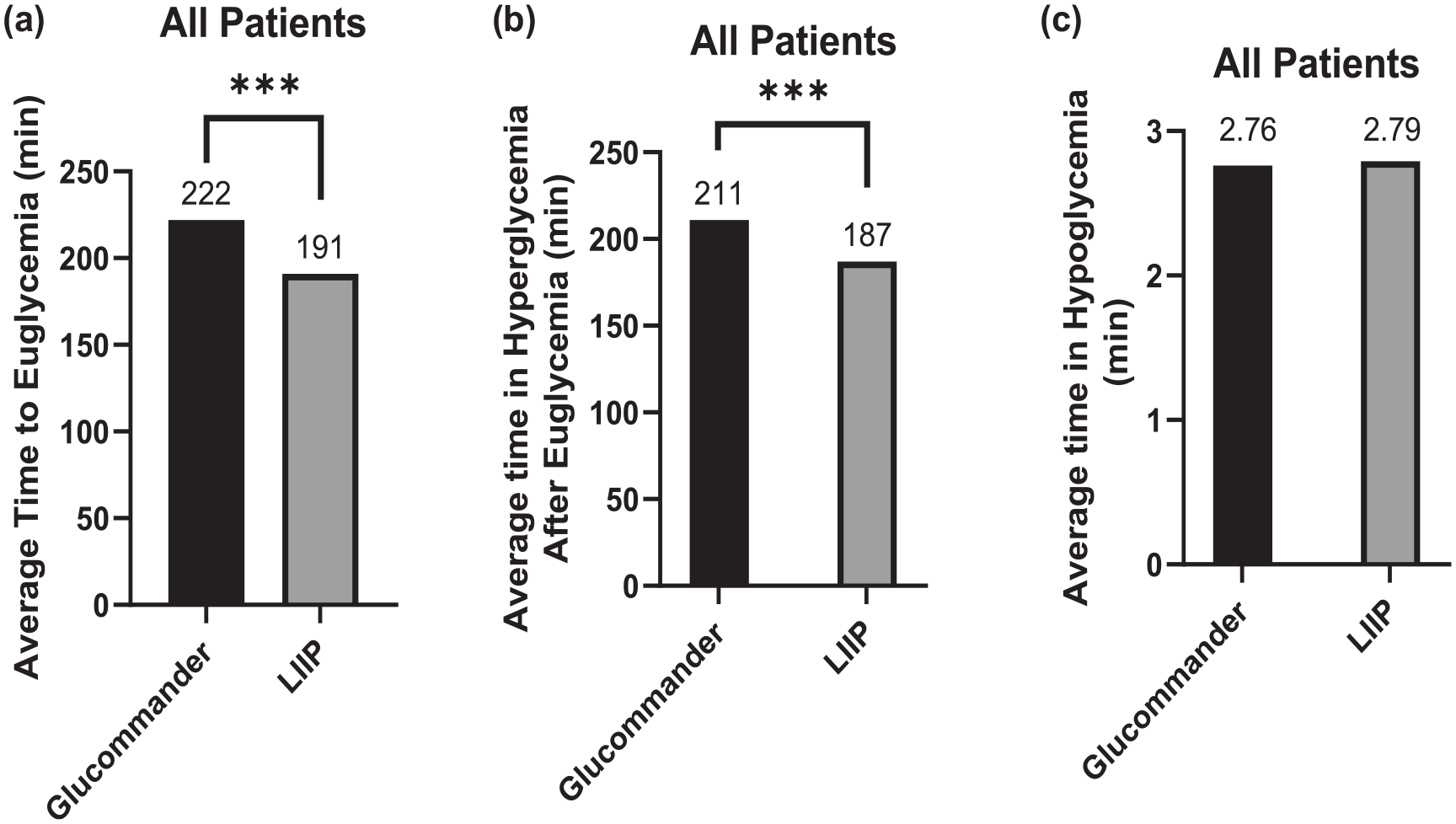
All patients. (a) Average time to euglycemia (70-180 mg/dL) for hospitalized patients receiving IV insulin during study period. (b) Average time in hyperglycemia (>180 mg/dL) for hospitalized patients receiving IV insulin during project period. (c) Average time in hyperglycemia (<70 mg/dL) for hospitalized patients receiving IV insulin during study period.
Subgroup Analysis
After filtering for hourly BG measurements from patients with DKA/HHS, the average time to euglycemia for patients in the GC group was 372 minutes. The DKA/HHS patients in the LIIP group reached euglycemia statistically faster at an average time of 252 minutes, t(1312) = 31.01, P < .001 (Figure 2a). No group differences were observed between percentage of time in hypoglycemia, z = 0.04, P = .84.
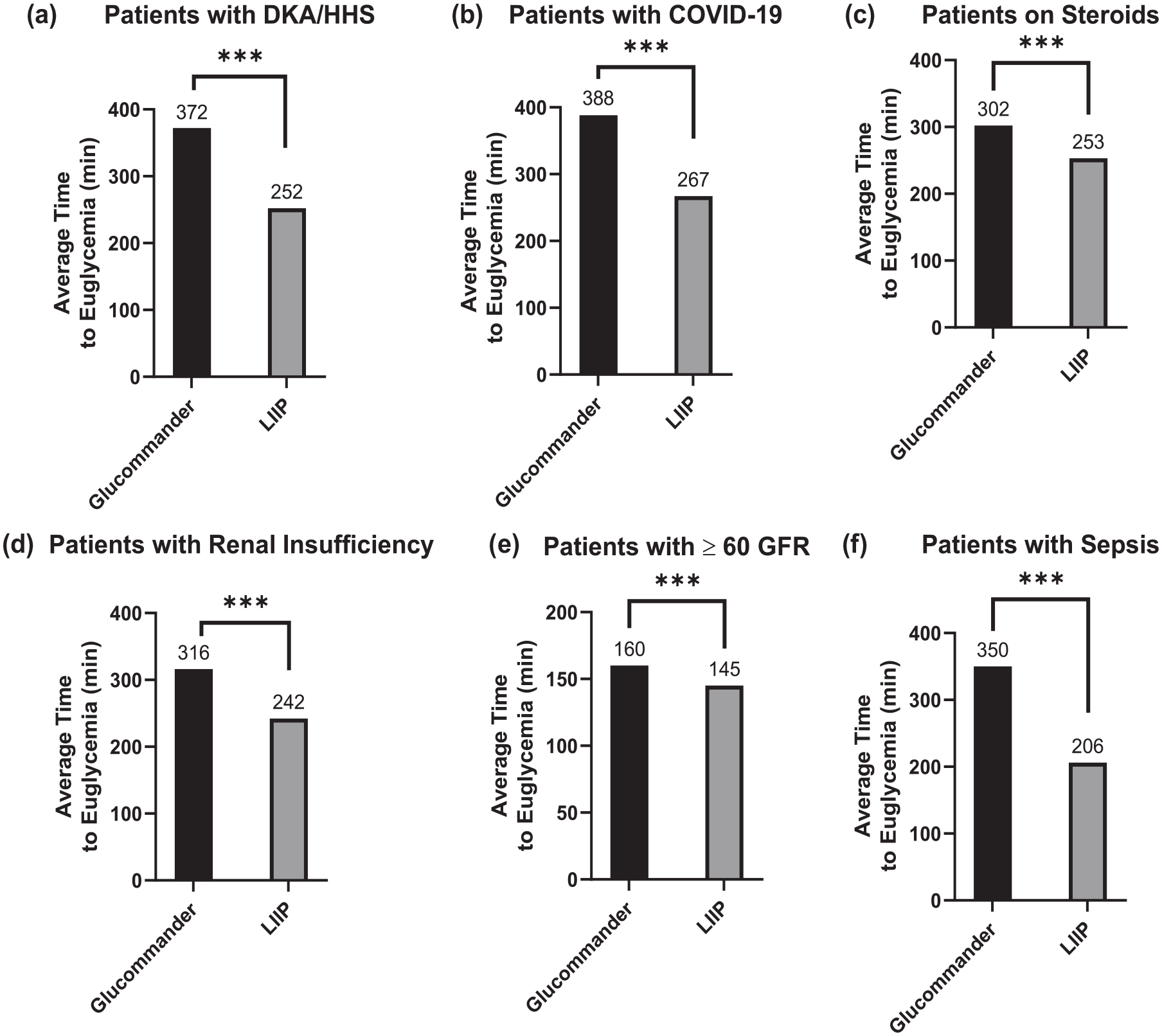
Subgroup analyses time to euglycemia. (a) to (f): Average time to euglycemia (70-180 mg/dL) for patients with DKA/HHS (a), patients with COVID-19 (b), patients on steroids (c), patients with renal insufficiency (d), patients with ≥60 GFR (e), and patients with sepsis (f).
Data filtering was performed in five additional subgroups. The average time to euglycemia for COVID-19 patients in the GC group was 388 minutes. The COVID-19 patients in the LIIP group reached euglycemia statistically faster at an average time of 267 minutes, t(331) = 12.01, P < .001 (Figure 2b). No group differences were observed between percentage of time in hypoglycemia, z = 0.06, P = .81.
The average time to euglycemia for patients undergoing steroid treatment in the GC group was 302 minutes. Patients on steroids in the LIIP group reached euglycemia statistically faster at an average time of 253 minutes, t(1336) = 3.29, P < .001 (Figure 2c). For patients undergoing steroid treatment, no differences were observed between the proportion of time in hypoglycemia for the GC (N = 944, mean = 0.11%) and LIIP groups (N = 394, mean = 0.17%), z = 0.9, P = .37.
The average time to euglycemia for patients with renal insufficiency in the GC group was 316 minutes. Patients with renal insufficiency in the LIIP group reached euglycemia statistically faster at an average time of 242 minutes, t(2657) = 33.85, P < .001 (Figure 2d). No difference was seen between patients in the GC (N = 1937, mean = 0.15%) and LIIP group between the time in hypoglycemia following euglycemia (N = 722, mean = 0.28%), z = 2.20, P = .0314.
Patients in the LIIP group with a GFR value of 60 mL/min or greater reached euglycemia statistically faster (mean = 145 minutes) than patients in the GC group (mean = 160 minutes), t(3604) = 15.02, P < .001 (Figure 2e). For patients with a GFR value of 60 or greater, no differences were observed between the proportion of time in hypoglycemia for the GC (N = 2763, mean = 0.15%) and LIIP groups (N = 843, mean = 0.13%), z = 1.40, P = .15.
The average time to euglycemia for patients with sepsis in the GC group was 350 minutes. Patients with sepsis in the LIIP group reached euglycemia statistically faster at an average time of 206 minutes, t(740) = 8.31, P < .001 (Figure 2f). For patients with sepsis, no differences were observed between the proportion of time in hypoglycemia for the GC (N = 565, mean = 0.20%) and LIIP groups (N = 177, mean = 0.23%), z = 1.55, P = .94. Figure 3 outlines subgroup comparisons on average BG readings in the hypoglycemia range. Notably, no statistically significant differences were found in the percentage of time spent in hypoglycemia across all subgroups analyzed.
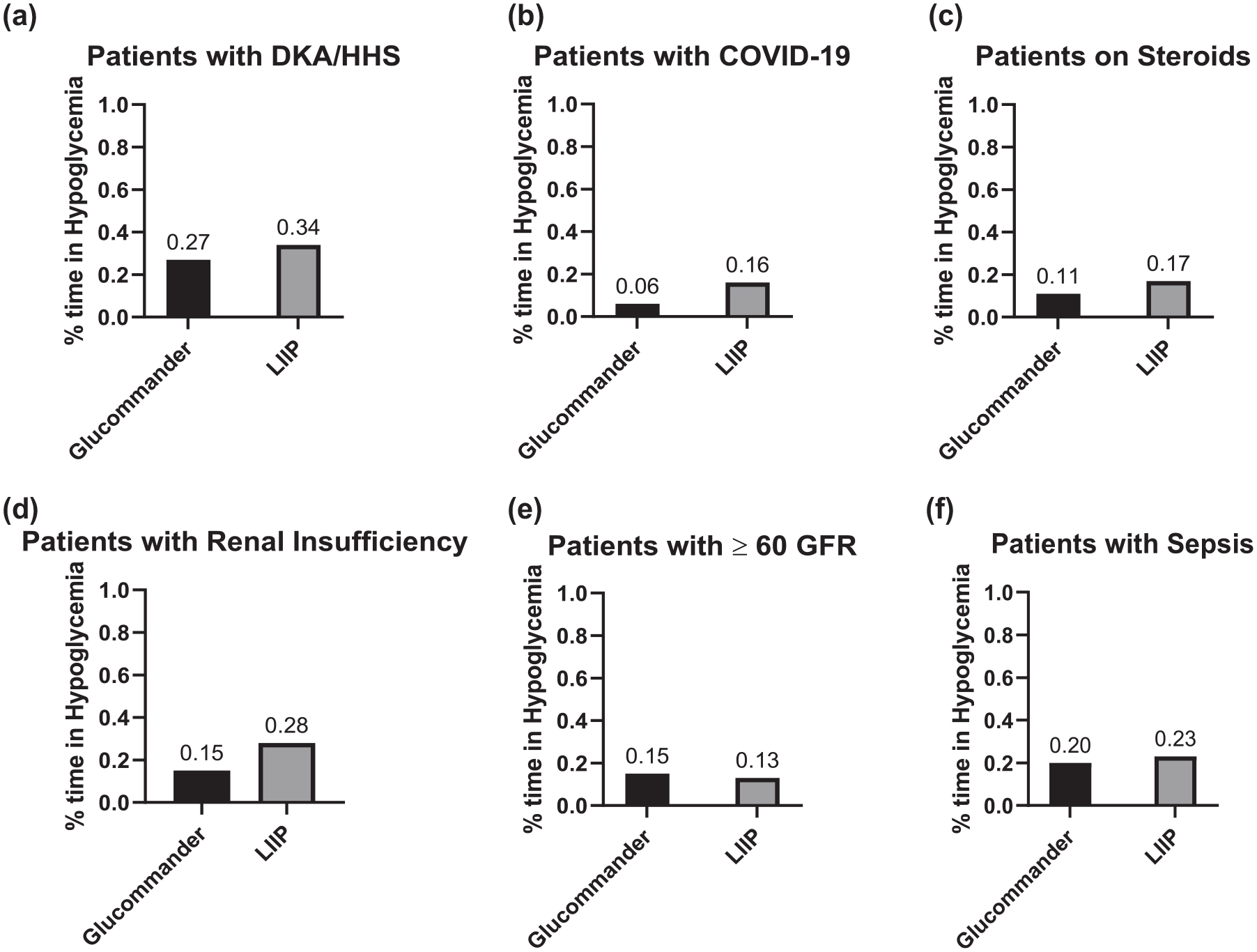
Subgroup analyses percentage of time in hypoglycemia. (a) to (f): Average percentage of time hypoglycemia (<70 mg/dL) for patients with DKA/HHA (a), patients with COVID-19 (b), patients on steroids (c), patients with renal insufficiency (d), patients with ≥60 GFR (e), and patients with sepsis (f).
Discussion
Prior to the turn of the century, hyperglycemia was thought of as a protective mechanism during illness. Over the past two decades, however, it has been clearly established that control of blood sugars during hospitalization leads to improved outcomes. This effort to control hyperglycemia in the hospital sparked a debate over the optimal target of glycemic control. In 2001, Van den Berghe et al suggested that tight control of blood sugars leads to improved survival in critically ill patients in the surgical ICU. Since then, many studies done in other patient groups failed to reproduce a similar benefit, mainly due to the increased risk of hypoglycemia that tight BG control poses. In 2009, much of the debate was put to rest with the publication of the NICE sugar study whose results showed that tighter blood sugar control was responsible for detrimental outcomes and recommended moderate control of hyperglycemia in the critical care setting.
In the ensuing years, several academic institutions developed various paper-based protocols to achieve this control. However, these were cumbersome, highly complex, and time-consuming, demanding workflow modifications that limited their popularity and widespread use. These protocols often demanded extensive nursing clinical expertise, thus stretching the borders of their scope of practice. The recent trend of adopting CIIPs in the hospital is exciting because of the potential to achieve better glycemic control while minimizing hypoglycemia in various hospital systems with differing resources and expertise. By automating insulin dosing calculation, we can factor in the complex and unique glycemic variance of a patient while also improving the nursing workflow. An ideal CIIP is one that is easily learned, easily incorporated into the EHR, effective in various difficult-to-treat conditions encountered in the critical care setting, and which achieves euglycemia as rapidly as possible without risking hypoglycemia.
The LIIP is a proportional integral derivative (PID)-based dosing calculator that employs multiple glucose values and prior responses, as well as time intervals between glucose concentration tests, to generate tailored dosing recommendations. The system leverages minimal patient-specific data at the outset and rapidly adapts to the unique needs of each individual. It employs a fast initial induction phase designed to achieve quick euglycemia, followed by a maintenance phase to sustain glycemic control. To circumvent hypoglycemia risks associated with aggressive IIPs, a more gradual phase bridges these two phases. In addition, the protocol features the capacity to control the duration of the initial induction phase, providing more flexibility for care. The protocol challenges the use of more intricate models, such as model predictive controls (MPCs), as increased parameter usage for initial dose recommendations and for predicting the effects of glucose variances may be achieved readily through greater glucose sampling, such as in continuous glucose monitoring systems. The study also evaluated GC, another PID system. Specifically, GC is a cloud-based system that integrates with the EHR and employs sequential multipliers to attain glycemic control.20,21 In addition, the integration of the LIIP system directly into the eMAR of the EHR streamlined the data entry process for nursing staff as they only needed to input data in one place. In contrast, the workflow of the GC system requires multiple data entries. This difference may have contributed to a simpler workflow with the LIIP system.
To date, this is the first comparative analysis of the performances of two CIIPs. This was a unique opportunity to perform this retrospective comparative analysis as part of HonorHealth’s quality improvement in operations when HonorHealth transitioned from GC to LIIP on August 18, 2020. The results showed that patients on LIIP achieved euglycemia quicker than those on GC while maintaining similar, low times in hypoglycemia. Furthermore, results within various clinical subgroups produced similar findings.
It is worth noting that the transition from GC to LIIP occurred during the COVID-19 pandemic, and that in COVID-19 patients who were hospitalized and receiving critical care, LIIP achieved euglycemia statistically faster than GC. This group of patients represented the sickest of all cases as they presented with a picture of severe sepsis, most of them had diabetes, and they received high doses of steroids.
This project had several limitations. First, there was no subgroup analysis performed for patients with different routes of nutritional administration. Moreover, it was a retrospective analysis of the safety and efficacy of two CIIPs over two different time intervals. By the nature of the availability of computerized systems in any hospital or network system, it is not possible to do a prospective randomized analysis of this kind. The project time frame was a continuum over a transition from one to the other protocol within the same network of hospitals and so it did represent real-life comparative scenarios with similar resources, expertise, nursing involvement, POC glucose testing method, and patient demographics.
Conclusion
As CIIPs become the standard of care for IV insulin dosing, we present the first retrospective comparison of two distinct computerized protocols: LIIP and GC. The LIIP was implemented into the primary eMAR at HonorHealth hospitals and led to a faster average time to euglycemia without an increased risk of hypoglycemia for patients receiving IV insulin. Additional subgroup analysis revealed that these benefits were found in harder-to-control patients, such as patients with COVID-19, patients on steroids, and patients with DKA/HHS. Contributing factors to the success of LIIP could be its ease of use and learnability, its ability to be incorporated into the eMAR, and its unique, dynamic, and adaptive algorithm.
Footnotes
Acknowledgements
The authors acknowledge the additional assistance of Debra Hay, RN, CDCES, Brian Sidoti, MD, Mark Slater, PhD, Kiran Avancha, PhD, and HonorHealth Research Institute staff as well as the nursing staff and diabetes team at HonorHealth Hospitals.
Abbreviations
BG, blood glucose; BMI, body mass index; CIIP, computerized insulin infusion protocol; DKA, diabetic ketoacidosis; EHR, electronic health record; eMAR, electronic medication administration record; GC, Glucommander; GFR, glomerular filtration rate; HHS, hyperosmolar hyperglycemic state; ICU, intensive care unit; IIIP, IV insulin infusion protocol; IV, intravenous; LIIP, Lalani Insulin Infusion Protocol; MPC, model predictive control; PID, proportional integral derivative; POC, point of care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Atul Lalani has an ownership stake in Endocrine Technologies and is employed at HonorHealth where the research was conducted. Data were analyzed by Dr. Gosselin who is a third-party consultant with HonorHealth Research Institute and has no equity stake in Endocrine Technologies.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.