
Abstract
Background:
Computerized insulin infusion protocols have demonstrated higher staff satisfaction, better compliance with protocols, and increased time with glucose in range compared to paper protocols. At University of California San Diego Health (UCSDH), we implemented an insulin infusion computer calculator (IICC) and transitioned it from a web-based platform directly into the electronic medication administration record (eMAR) of our primary electronic health record (EHR).
Methods:
This is a retrospective analysis of 6306 adult patients at UCSDH receiving intravenous (IV) insulin infusion from March 7, 2013 to May 30, 2019. We created three periods of the study—(1) the pre-eMAR integration period; (2) the eMAR integration period; and (3) the post-eMAR integration period—and looked at the percentage of readings within goal range (90-150 mg/dL for intensive care unit [ICU], 90-180 mg/dL for non-ICU) in patients with and without hyperglycemic emergencies. As our safety endpoints, we elected to look at incidence of blood glucose (BG) readings <70 mg/dL, <54 mg/dL, and <40 mg/dL.
Results:
Pre-eMAR 69.8% of readings were in the 90-150 mg/dL range compared to 70.2% post-eMAR (P = .03) and 82.7% of readings were in the 90-180 mg/dL range pre-eMAR versus 82.9% (P = .09) post-eMAR in patients without hyperglycemic emergencies. Rates of hypoglycemia with BG <70 mg/dL were 0.43%, <54 mg/dL were 0.07%, and <40 mg/dL were 0.01% of readings pre- and post-eMAR.
Conclusions:
At UCSDH, our IICC has shown to be safe and effective in a wide variety of clinical situations and we were able to successfully transition it from a web-based platform directly into the eMAR of our primary EHR.
Keywords
Introduction
The association between inpatient hyperglycemia in patients with and without documented history of diabetes and adverse outcomes has been consistently documented in the literature.1,2 Insulin is the preferred therapy for glycemic management in the inpatient setting because it has no absolute contraindications, it provides rapid and powerful glucose lowering, and it can be titrated in response to glycemic trends and the multitude of changing variables that affect glycemic control. 3 Furthermore, continuous intravenous (IV) insulin infusion is the preferred route of insulin delivery for critically ill patients related to its short half-life and the ability to quickly titrate and achieve glycemic control. 3 Additional indications for IV insulin exist for patients outside of critical care such as in the progressive care unit (PCU), peri-operative unit, reproductive health unit, and emergency department (ED) for treatment of a broad range of conditions including: diabetic ketoacidosis (DKA), hyperglycemic hyperosmolar state (HHS), severe hyperglycemia, prolonged fasting periods in insulin deficient patients, and for dose finding in patients starting continuous parenteral or enteral nutrition. 4
Ideal glycemic targets for patients on continuous IV insulin infusion have been controversial over the past several years. Whether adhering to the recommendations of the American Association of Clinical Endocrinologists (AACE) and American Diabetes Association (ADA) for glycemic targets of 140-180 mg/dL 5 or the Society of Critical Care Medicine (SCCM) recommendations to maintain blood glucose (BG) levels between 100-150 mg/dL, 6 professional bodies agree that glycemic control should be achieved without increased incidence of hypoglycemia.
The methods for administering IV insulin are complex. From a nursing standpoint, workload is increased with frequent glucose monitoring and drip titration and potential hypoglycemia treatment. In the case of paper protocols, nurse workload is further increased when tables are utilized and calculations are required. All of these variables increase the risk of error and possible patient harm. Therefore, safe, simple methods to achieve glycemic control in hospitalized patients on insulin infusion are necessary. Additionally, it is important that the end-users have appropriate education, training and ongoing support.7-9 Several groups have tested various approaches and computer-based insulin infusion guideline implementation has demonstrated that tighter glycemic control can be achieved with faster time to target without increased risk of hypoglycemia compared to paper protocols while also improving nursing workflow and satisfaction.10,11 Computerized insulin infusion guidelines improve nursing staff’s responsiveness in measuring patient blood glucose (BG) levels and increase their ability to provide appropriate insulin doses in response to glucose levels, perhaps more so when the guideline is integrated into the electronic health record (EHR) and therefore the nursing workflow. 12
In 2003, at University of California San Diego Health (UCSDH), we were on our eighth version of an insulin infusion paper protocol; clinicians expressed dissatisfaction with its length and complexity and internal audits found poor protocol compliance and significant incidence of hypoglycemia. Based on these findings, and with no commercial products available at the time, our efforts focused on internal development of an insulin infusion computer calculator (IICC). Our first attempt was a DOS-based program available on bedside workstations. This transitioned into a web-based version with an admission-discharge-transfer (ADT) feed in 2008, but still lacked scalability, access control, ability to collate data; required labor intensive manual adjustment by super-users; and provided only minimal opportunity for feature development. The fact that it existed outside the EHR also led to increased staff workload and risk of medication administration errors due to transcription errors and lack of bar code medication administration (BCMA) workflow. To address these limitations, in 2017 we undertook a collaborative project involving leads from Information Services, Pharmacy, Endocrinology, and Nursing Education, Development and Research to transition the calculator into the medication administration record (MAR) of our primary EHR. The existing algorithm was replicated within a flowsheet in the EHR, allowing for a concurrent review of the insulin infusion order, and supporting BCMA for positive patient identification. In this study, we review the data before and after the transition of our IICC into the electronic medication administration record (eMAR), specifically looking at its performance and safety in both venues.
Methods
Algorithm Design
The algorithm utilized in our IICC is an insulin sensitivity coefficient (ISC)-based algorithm utilizing BG value and rate of change to adjust the coefficient. Coefficient-based algorithms are more dynamic than traditional column-based protocols and were originally chosen to better fit our critically ill patients with changing insulin sensitivities.7,13 With the most recent eMAR integration, the algorithm remains largely unchanged, but we were able to expand feature development and address the top three scenarios requiring manual adjustment of the ISC in our web-based platform: interruption in nutrition, prolonged DKA/HHS, and highly insulin sensitive patients. Interruption in nutrition was by far the most common indication for manual adjustment of the ISC and to address this, as well as create a prompt for nurses to recognize the interruption in nutrition in a timely manner, we added a required step to indicate whether or not there had been a decrease in nutrition since the last entry into the IICC, which then automatically adjusts the ISC accordingly. To address the final two challenging scenarios, we added a button to set goal BG range to 200-250 mg/dL for prolonged DKA/HHS and a “high sensitivity” button for patients highly sensitive to insulin such as patients with type 1 diabetes and end stage renal disease (ESRD) with very low insulin requirements. Figure 1 is a screenshot of the IICC integrated into the eMAR of our primary EHR and outlines the general workflow. Figure 2 shows a screenshot of the additional special situation buttons created as above.
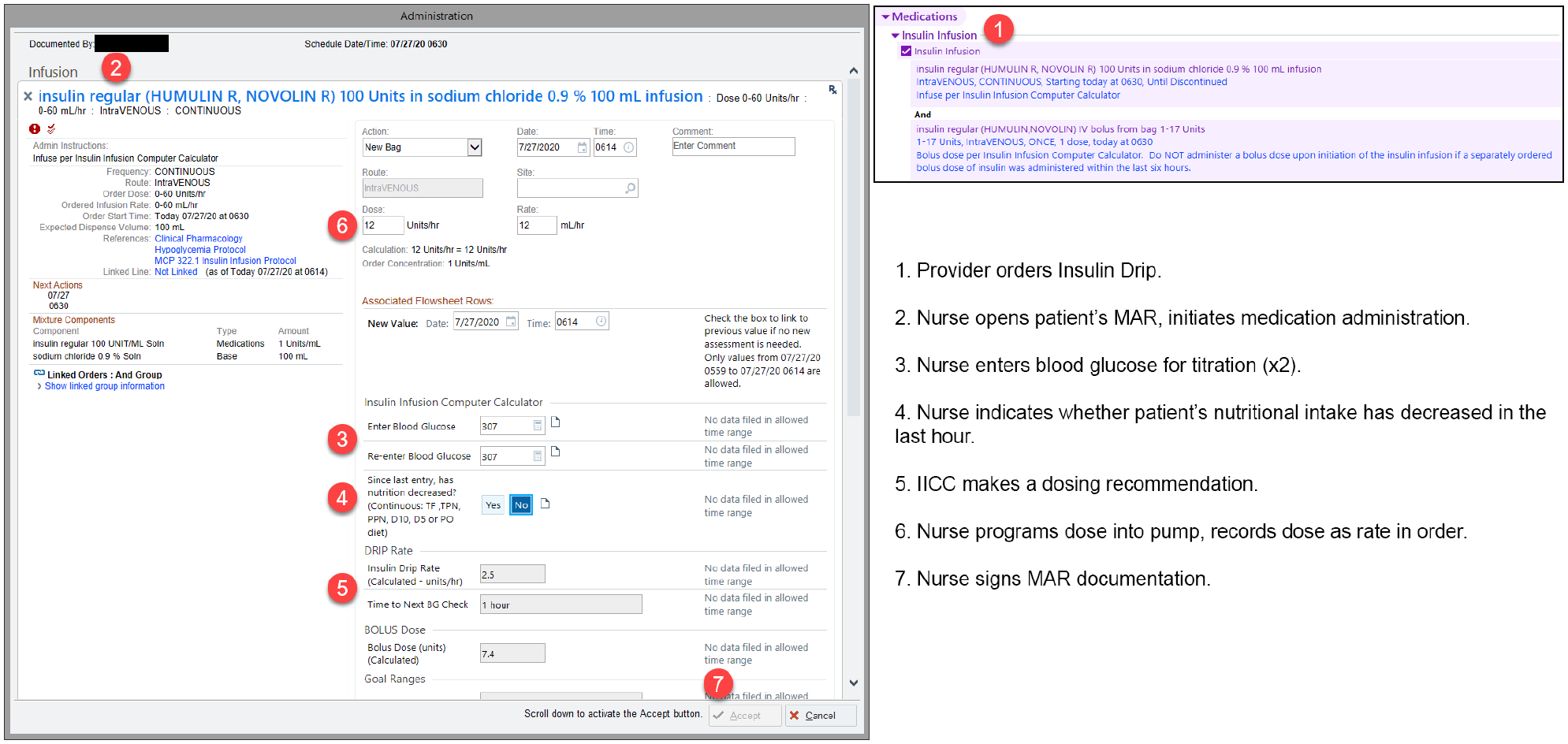
Screenshots of the insulin infusion order and the IICC in the eMAR of our primary EHR with outline of general workflow. EHR, electronic health record; eMAR, electronic medication administration record; IICC, insulin infusion computer calculator.
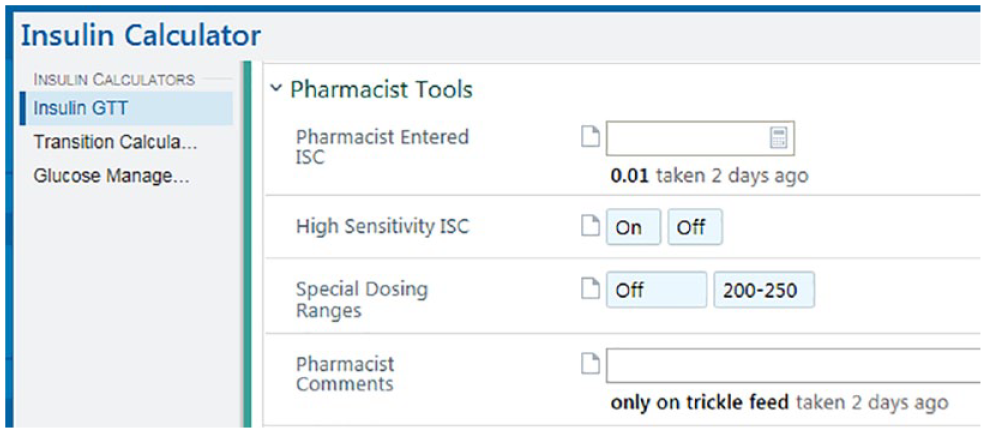
Screenshot of pharmacist tools including manual adjustment of ISC, high sensitivity button, and special dosing range used in our institution for prolonged DKA/HHS. DKA, diabetic ketoacidosis; HHS, hyperglycemic hyperosmolar state; ISC, insulin sensitivity coefficient.
Implementation Within eMAR
Once the initial programming of the algorithm was complete on a proof-of-concept basis, we performed regression testing and validation of calculator outputs against data from the existing calculator in our designated testing environment. Validation was performed independently by both members of the Information Services department as well as clinical subject matter experts. Training materials for clinical staff, in the form of a web-based interactive learning module, were updated and assigned to nursing staff house-wide. Upon completion of testing and validation, the EHR-integrated model was piloted on the Trauma/Surgical ICU and the Burn ICU; those units were selected due to an increased prevalence of insulin infusions. The pilot was expanded to the Cardiovascular ICU after four weeks to ensure usability at both UCSDH inpatient sites. Feedback was solicited from nursing and pharmacy staff, both in-person and via email, and patient charts were reviewed for appropriateness and accuracy of dosing recommendation. Transition to the new model institution-wide was coordinated with Pharmacy, Nursing, and Information Services staff to ensure safe transition off the web-based system. This was accomplished without incident on the originally scheduled date. See Figure 3 for a timeline of transition of the IICC into eMAR.
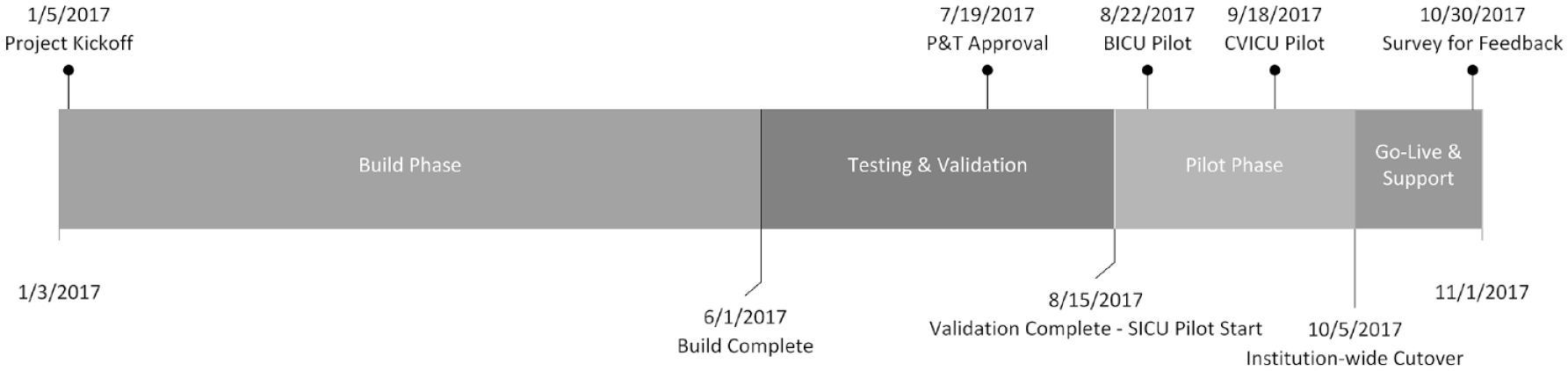
Timeline of transition of the insulin infusion computer calculator (IICC) into the electronic medication administration record.
Study Methods
This is a retrospective analysis of adult patients at UCSDH receiving IV insulin infusion from March 7, 2013 to May 30, 2019. Data were obtained from the EHR via extraction to ensure all point-of-care blood glucoses were collected, as it is likely that not all blood glucoses were entered into the web-based insulin calculator. Results are reported in aggregate, so an exempt research application was applied for and approved by the investigational review board. Hourly BG measurements were obtained from arterial or capillary fingerstick sampling, performed on Accu-Check Inform II Blood Glucose Monitoring System. We extracted the date, time, and result value of all BG point-of-care tests (POCT) performed while on an insulin infusion. For an additional clinically relevant means of characterizing the data, we looked at drip runs on the insulin infusion. Drip runs were defined based on a “start” MAR action and a “last” MAR action for insulin infusion medication record using a “lag” time of 720 minutes between previous MAR last and start to determine if the infusion was on a single run. The data elements extracted for each “run” included: (1) start and end time/date, (2) unit of initiation, and (3) preceding serum creatinine. For each drip run, we determined whether that patient encounter included a hospital diagnosis of a hyperglycemic emergency, defined as DKA or HHS. We also determined whether the patient had impaired renal function, which we defined as a most recent serum creatinine ≥1.5 mg/dL.
Statistical Methods
We created three periods of the study: (1) the pre-eMAR integration period (August 2013-September 2017); (2) the eMAR integration period (October 2017-December 2017); and (3) the post-eMAR integration period (January 2018-May 2019). We categorized the unit of drip initiation into: Emergency Department (ED), Progressive Care Unit (PCU), Intensive Care Unit (ICU), Peri-operative (PeriOp), and Obstetric Unit (OB). For each glucose value, we determined which hour into the drip run it was measured.
We generated descriptive statistics for the pre- and post-eMAR integration periods for the proportion of glucose values within a variety of ranges used in prior published studies. We looked at the percentage of readings within goal range (90-150 mg/dL for ICU, 90-180 mg/dL for non-ICU). As our safety endpoints, we elected to look at incidence of BG readings <70 mg/dL, <54 mg/dL, and <40 mg/dL. We stratified these results based on presence or absence of a hyperglycemic emergency, presence or absence of impaired renal function, and OB versus non-OB cases. We performed Fisher’s Exact Test calculations to assess differences in distributions of proportions in glucose ranges 90-180, 90-150, <70, <54, and <40 mg/dL. For each hour of drip runs across patients within the pre- and post-eMAR integration periods, we calculated the median, first quartile, and third quartile glucose values. We stratified these per-hour results based on the presence or absence of hyperglycemic emergency. All analyses were performed using SAS version 9.4 (SAS, Inc., Cary, NC). A survey was also performed several weeks after transition to the eMAR IICC to evaluate nursing satisfaction with the new platform.
Results
We compiled BG POCT readings from 6306 patients receiving an insulin infusion per our IICC at UCSDH between 2013 and 2019. Over this 67-month time frame, we collected 274,314 BG POCT readings from patients in either the ICU or non-ICU setting admitted with non-hyperglycemic emergencies and 16,404 BG POCT readings from patients admitted with a hyperglycemic emergency. We compared BG POCT readings before and after transition of our algorithm into the eMAR and excluded the three-month time frame during transition, October through December 2017. In general, our ICU goal range remained 90-150 mg/dL and non-ICU goal range 90-180 mg/dL for the majority of this time period.
Figure 4(a) shows the percentage of BG POCT readings in range as well as percent of readings with hypoglycemia both pre- and post-transition of algorithm directly into eMAR in patients without hyperglycemic emergencies. Pre-eMAR 69.8% of readings were in the 90-150 mg/dL range compared to 70.2% post-eMAR (P = .03) and 82.7% of readings were in the 90-180 mg/dL range pre-eMAR versus 82.9% post-eMAR (P = .09). Rates of hypoglycemia with BG < 70 mg/dL were 0.43%, <54 mg/dL were 0.07% and <40 mg/dL were 0.01% of readings pre- and post-eMAR; see Figure 4(b). For patients admitted with a hyperglycemic emergency, 46.8% and 45.9% of readings were in the 90-150 mg/dL range pre- and post-eMAR (P = .30) and 61.6% versus 61.7% of readings in the 90-180 mg/dL range pre- and post-eMAR (P = .90), respectively; see Figure 5.
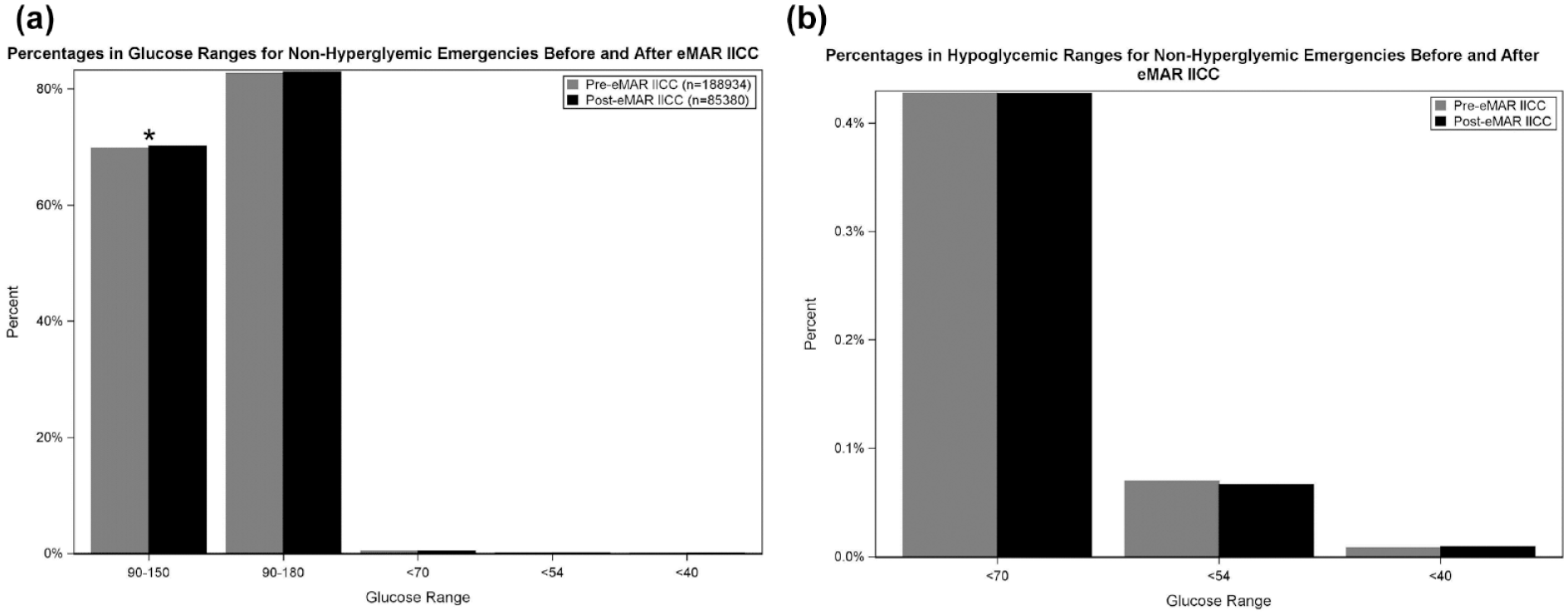
(a) Percentage of BG POCT readings in range and percent of readings with hypoglycemia both pre- and post-transition of algorithm directly into eMAR in patients without hyperglycemic emergencies. * indicates statistical significance. (b) Hypoglycemia pre- and post-transition of algorithm directly into eMAR in patients without hyperglycemic emergencies. BG, blood glucose; eMAR, electronic medication administration record; POCT, point of care test.
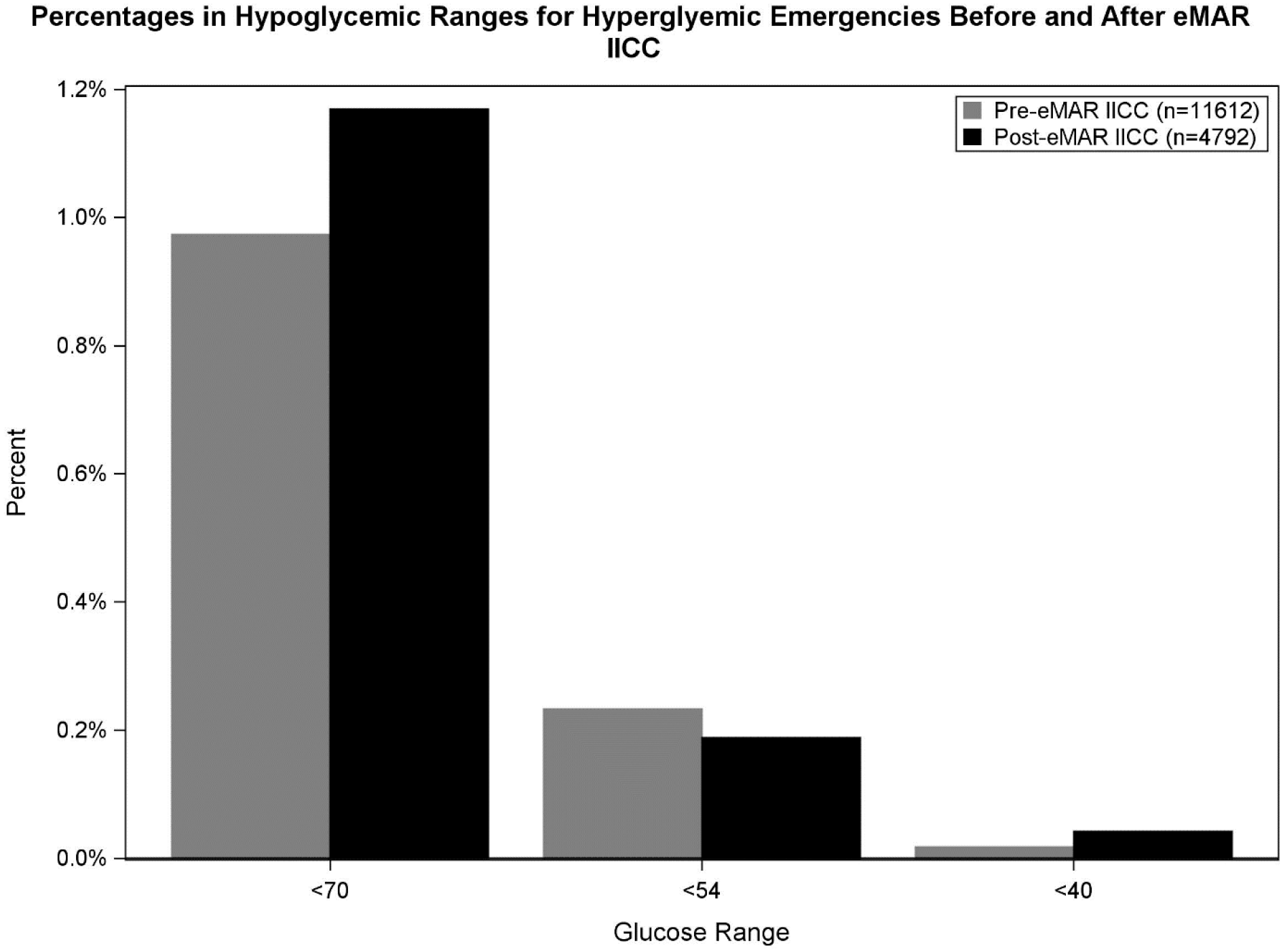
Percentage of BG POCT readings in range and percent of readings with hypoglycemia both pre- and post-transition of algorithm directly into eMAR in patients with hyperglycemic emergencies. BG, blood glucose; eMAR, electronic medication administration record; POCT, point of care test.
See Figures 6 and 7 for glucose values by hour into drip run for patients with and without hyperglycemic emergencies pre- and post-transition to eMAR IICC. Average time to BG range 90-180 mg/dL and 90-150 mg/dL was 2.3-4.2 hours in non-HGE patients and 5.0-6.8 hours in patients admitted with a hyperglycemic emergency.
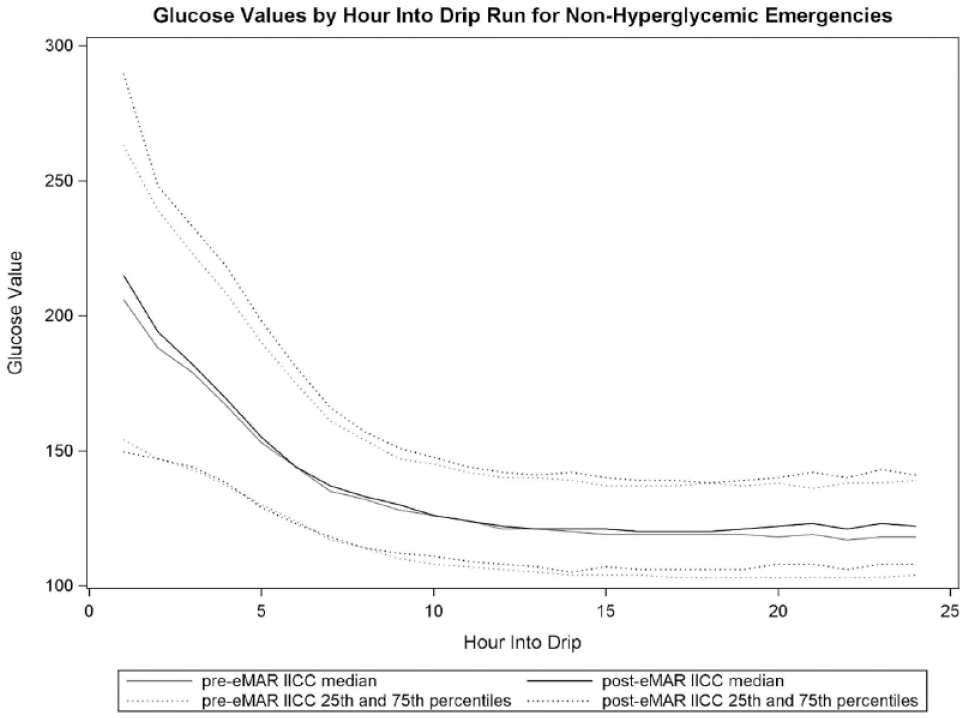
Glucose values by hour into drip run for non-hyperglycemic emergencies pre- and post-transition to eMAR IICC. eMAR, electronic medication administration record; IICC, insulin infusion computer calculator.
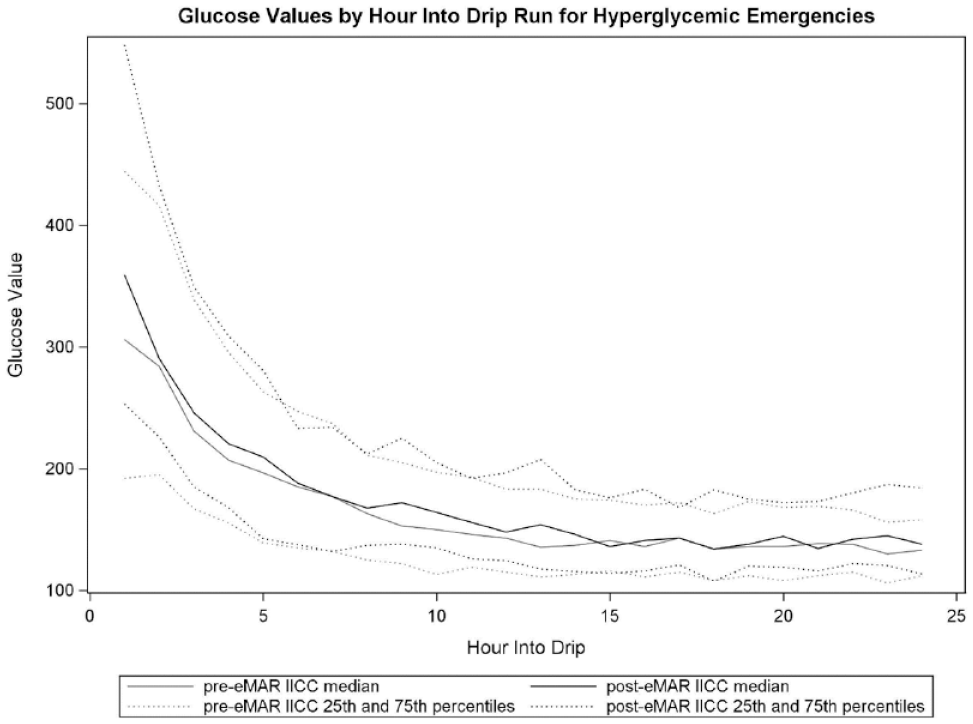
Glucose values by hour into drip run for hyperglycemic emergencies pre- and post-transition to eMAR IICC. eMAR, electronic medication administration record; IICC, insulin infusion computer calculator.
Within vulnerable patient populations including obstetrics and those with impaired renal function, we measured rates of hypoglycemia in non-HGE cases. In the OB population, rates of hypoglycemia <70 mg/dL were 1.39% and 1.47% (P = .83), <54 mg/dL were 0.24% and 0.36% (P = .45) and <40 mg/dL were 0% and 0.1% (P = .06) of readings, respectively, pre- and post-eMAR; see Figure 8(a). For patients with impaired renal function, rates of hypoglycemia <70 mg/dL were 0.44% and 0.42% (P = .65) and <54 mg/dL were 0.07% and 0.06% (P = .66) of readings, respectively, pre- and post-eMAR; see Figure 8(b). Rates of hypoglycemia <40 mg/dL were 0.01% of readings pre- and post-eMAR (P = .47).
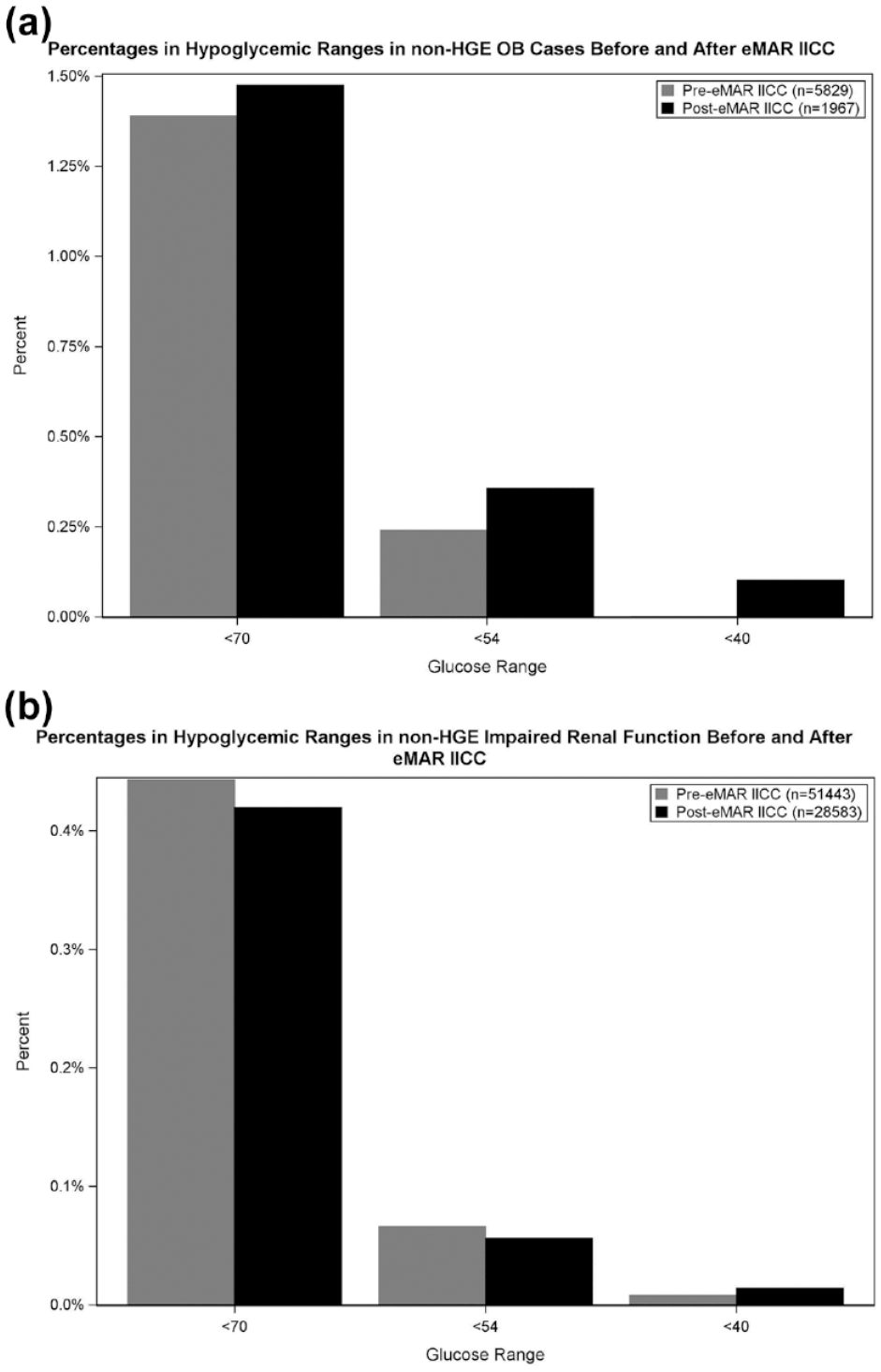
Special populations: (a) Rates of hypoglycemia in OB patients with no HGE pre- and post-eMAR IICC implementation. (b) Rates of hypoglycemia in patients with impaired renal function and no HGE pre- and post-eMAR IICC implementation. eMAR, electronic medication administration record; HGE, hyperglycemic emergency; IICC, insulin infusion computer calculator; OB, Obstetric Unit.
In a survey to evaluate nursing satisfaction conducted a few months after transition to the eMAR IICC, 75 out of 79 responses stated they liked the eMAR IICC more or the same as the previous workflow in the web-based IICC with only four responders noting they liked the new calculator less.
Discussion
Over the last 16 years, at UCSDH, our IICC has transitioned from a bedside DOS-based program, to a web-based version that included an ADT interface to its current version embedded directly into the eMAR of our primary EHR. The algorithm remains largely unchanged and has demonstrated durability through multiple computer systems, patient populations, and unit types. It has also been shown to be safe and effective in a wide variety of clinical settings including hyperglycemic emergencies, critical care hyperglycemia, noncritical care hyperglycemia, and diabetes in pregnancy with data comparable to commercial products.7,9,14-19 The percent of readings within range was high and consistent through transition of our algorithm into the eMAR in 2017 with no significant differences pre- and post-implementation other than a trend in favor of the eMAR IICC at the 90-150 mg/dL range for non-HGE patients. Rates of hypoglycemia also remained low through this transition, including high-risk patient populations such as OB and patients with impaired renal function with no significant differences pre- and post-transition into eMAR. Nursing satisfaction was very high with the transition to the eMAR IICC with 95% of nurses responding to a survey stating they liked the new eMAR IICC more or the same as the previous web-based IICC.
Time to BG in range was 2.3-4.2 hours for patients without hyperglycemic emergency and slightly longer for patients with hyperglycemic emergencies explained by HGE patients usually presenting with higher initial BG values and the addition of dextrose containing IVFs to keep BG >200 mg/dL until resolution of DKA/HHS per our standard DKA/HHS guideline.
While our IICC algorithm has demonstrated safety, efficacy, and versatility in our hospital system over many years, implementing such a tool is not a simple task and requires careful planning, coordination with stakeholders, rigorous processes to validate the programming, educational support for rollout and maintenance, as well as processes in place to fine-tune details along the way. The details of operationalizing rollout of such a tool are just as important as the details of the programming itself. At UCSDH, we have maintained pharmacists as our super-users through each computer platform and utilized additional programming capabilities in each system to help reduce necessary human intervention. In addition, tracking glucometrics, medication error reports, and feedback from end users, including nurses and providers, have been instrumental to the success of our IICC.
This work does have several limitations. First, it is a retrospective analysis and therefore results before and after the algorithm’s integration with the eMAR could have been influenced by secular trends. However, only minor changes were made to our DKA/HHS guidelines since the transition, and none of which we would expect to affect the overall results. Second, the goal ranges were 90-150 mg/dL in the ICUs and 90-180 mg/dL in the non-ICU setting for the most part over the course of this study; however, there were slight modifications over this time period for some of the units. For example, the burn ICU unit modified their goal range to 100-180mg/dL and while these patients accounted for a very small percentage of the overall total number of patients and readings, it remains a limitation of the analysis. Finally, this was a single center study, and it is unknown whether our IICC would perform similarly in other institutions or with other operational support.
Conclusion
Computerized insulin infusion protocols have demonstrated higher staff satisfaction, better compliance with protocols, increased time with glucose in range with more standardization, and less glucose variability compared to paper protocols. At UCSDH, we have implemented an IICC utilizing an ISC-based algorithm that is safe and effective in a wide variety of clinical situations and successfully transitioned it from a web-based platform and integrated it directly into the eMAR of our primary EHR.
Footnotes
Acknowledgements
We acknowledge the additional assistance of Raul Coimbra, MD (Trauma Surgeon who supported the initial project in 2004), Dale Fortlage (original programmer), Marc Sylwestrzak (initial web-based programmer and ADT interface), Greg Hartman (EHR analyst), Roma Gianchandani, MD (endocrinology collaborator at University of Michigan), and Mohammad Ateya (programmer at University of Michigan who assisted with EHR code) as well as the nursing staff, pharmacists, and physicians at UC San Diego Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.