
Abstract
People with Alzheimer’s disease or related dementias and diabetes mellitus (ADRD-DM) are at high risk for hypoglycemic events. Their cognitive impairment and psychosocial situation often hinder detection of hypoglycemia. Extending use and benefits of continuous glucose monitoring (CGM) to people with ADRD-DM could improve hypoglycemia detection, inform care, and reduce adverse events. However, cognitive impairment associated with ADRD presents unique challenges for CGM use. This commentary proposes applying the human-centered design process to CGM, investigating design solutions or interventions needed to integrate CGM into the health care of patients with ADRD-DM. With this process, we can identify and inform CGM designs for people with ADRD-DM, broadening CGM access, increasing detection and treatment of the silent threat posed by hypoglycemia.
The ADRD-DM Challenge
The combination of diabetes mellitus (DM) and Alzheimer’s disease and related dementias (ADRD) increases the risk of adverse health outcomes. Over six million Americans have ADRD; of those 13% to 20% are estimated to also have DM. 1 DM is associated with a twofold increase in mortality among people with ADRD, and people with ADRD-DM have a high risk of severe hypoglycemia and associated hospitalization. 2 Hypoglycemia is a frequent complication of diabetes that occurs when glucose levels fall below 70 mg/dL. Below 54 mg/dL, hypoglycemia becomes severe. 2 Among people with ADRD-DM, hypoglycemia is associated with falls, macrovascular events, and death.1-3 Decreasing the intensity of DM therapy does not, alone, eliminate the risk of hypoglycemia. Despite hypoglycemic events being often underreported, they are estimated to occur in 10% to 25% of people with ADRD-DM. 1 To improve the quality of life and health of those with ADRD-DM, interventions are needed to improve detection of hypoglycemia and guide modifications to lifestyle or treatment.
For patients and caregivers, ADRD-DM presents unique challenges for detecting and preventing hypoglycemia. 2 This population relies primarily on self-monitoring blood glucose testing (“finger sticks”), manually logging information about glucose values and daily activities, and automatically storing blood glucose monitor values in their monitor or a personal website. The cognitive impairment associated with ADRD, however, makes consistent and effective glucose monitoring and management more challenging. The bidirectional relationship between cognition and hypoglycemia hinders self-care,1,2 and often results in poor health outcomes and reduced quality of life for patients,2,4,5 who find blood glucose monitors uncomfortable and intrusive.4,5 As a result, less frequent glucose monitoring may occur, decreasing the likelihood of identifying hypoglycemia or increasing hypoglycemia unawareness. 6 Better hypoglycemia awareness could improve prevention and management in patients with ADRD-DM, especially those who are using oral hypoglycemic agents or insulin. 2
The Continuous Glucose Monitoring Challenge
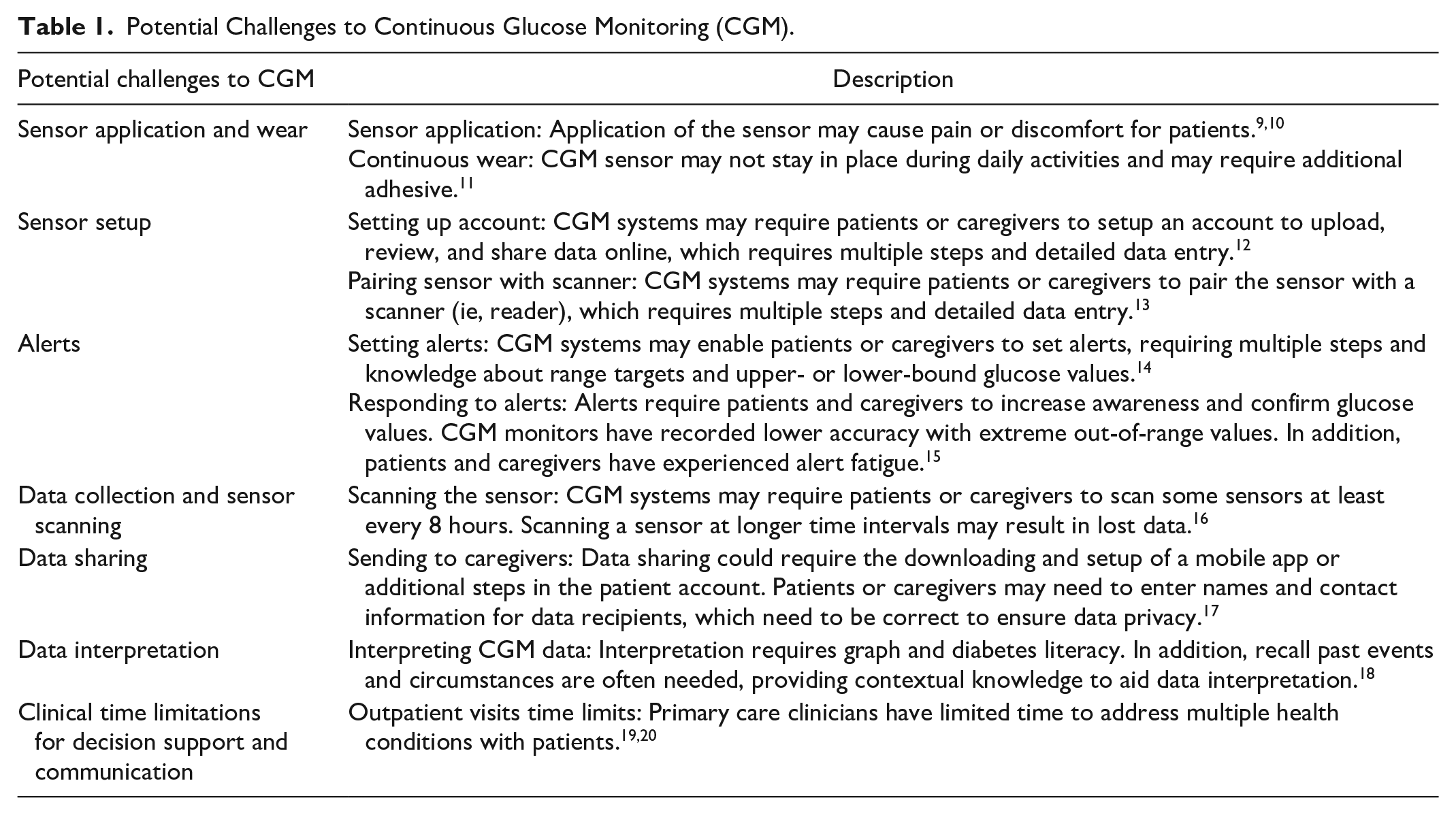
Although continuous glucose monitoring (CGM) is an effective method for detecting hypoglycemic events, 7 only a limited number of reports of CGM’s effectiveness for patients with ADRD-DM are in the medical literature.1,8 Patients and caregivers with normal cognitive function experience challenges with CGM (see Table 1).9,21 These challenges are expected to be escalated for patients with ADRD-DM and could affect safety and feasibility of CGM in this population. Commonly, CGM is ordered for up to 14 days. Afterward, clinicians and patients review a narrative, tabular, or graphical summary of glucose values. Patients are expected to recall circumstances related to out-of-range glucose measurements, but cognitive impairment associated with ADRD presents unique challenges with this approach. Moreover, introducing CGM into geriatrics and primary care settings presents another challenge. Although DM is typically managed in primary care, limitations of time and decision support for communication about hypoglycemia contribute to low utilization and slow implementation of recommended guidelines for tailoring ADRD-DM treatment. Investigation into CGM solutions for patients with ADRD-DM is needed to implement care guidelines in geriatrics and primary care settings. 22
Potential Challenges to Continuous Glucose Monitoring (CGM).
Applying Human Factors Engineering
Human factors engineering (HFE) can be used to investigate CGM for ADRD-DM care. Human factors is a discipline combining engineering and behavioral science, to study and improve work systems comprising interactions between people and their tasks, tools, and environments. 23 HFE applies scientific methods, international standards, and established frameworks to identify problems and opportunities in those interactions and to foster design and evaluation of evidence-based solutions. A key application of HFE in health care is the design, implementation, and evaluation of human-centered health information technology. 24 Focused on users and their needs, human-centered design is an iterative process with four phases: specify the context of use, specify requirements, design, and evaluate (Figure 1). 25 The first two phases are often combined into a needs assessment.26,27 Multiple HFE methods can be applied in each phase (Table 2). A review concluded that human-centered design improves the usability (ie, effectiveness, efficiency, and satisfaction) of mobile health applications (apps) for older adults, 30 but a review of ADRD apps reported highly variable and often unacceptable usability and quality. 31 Up to 42 barriers have been identified that adversely influence adoption of mobile apps by older adults. 32
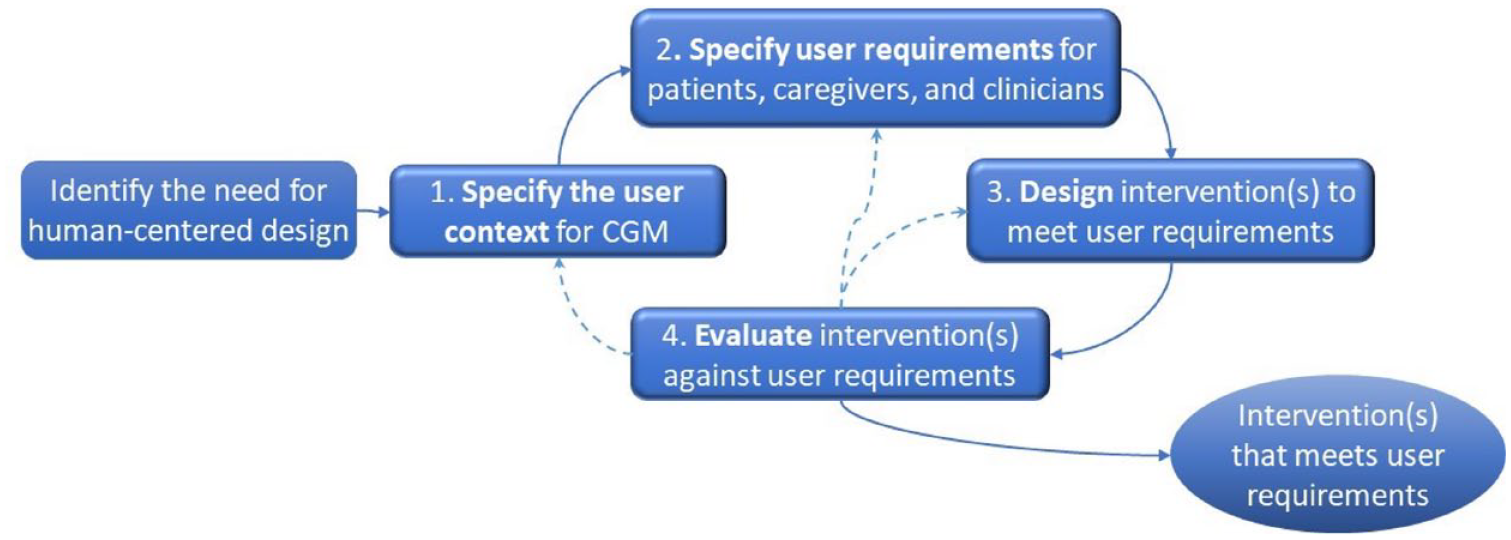
Human-centered design process. 25 Adapted from ISO 9241 210 2010.
Human-Centered Design Process. 25 Phases, HFE Methods, and Their Potential Application in the Redesign of CGM for Patients With ADRD-DM, Caregivers, and Clinicians.
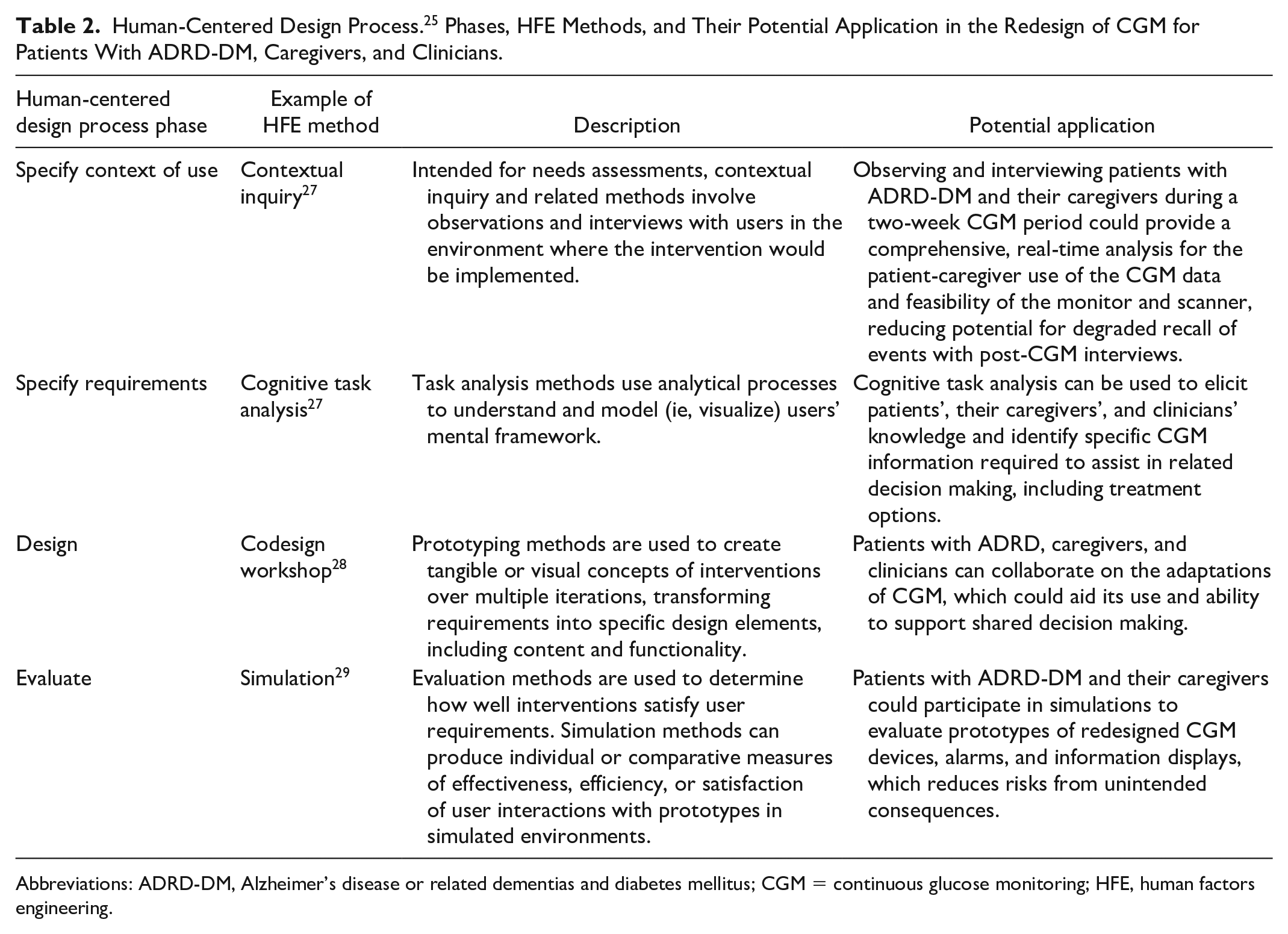
Abbreviations: ADRD-DM, Alzheimer’s disease or related dementias and diabetes mellitus; CGM = continuous glucose monitoring; HFE, human factors engineering.
Human-centered design can be applied to identify and address unique challenges and needs of patients, caregivers, and clinicians in the capture and interpretation of CGM data. HFE methods can facilitate needs assessments for integrating CGM into daily lives and workflows. It can also yield participatory design of intuitive information displays and can aid evaluation of DM management before and after CGM.
Needs Assessment: Patients, Caregivers, and Clinicians
Among patients with ADRD-DM, severity of cognitive impairment and behavioral and psychological symptoms are important characteristics to consider in investigating CGM design. Across the ADRD spectrum, these characteristics may influence the involvement and capacity of caregivers to support safe CGM use. Although these caregivers will have varying levels of responsibilities and skills related to glucose management, caregivers’ needs and characteristics must be studied, including task-induced burden and management of personal health. An HFE method called contextual inquiry could provide a comprehensive, real-time analysis of patient and caregiver use of CGM data. This method would involve patient and caregiver interviews and observations in the home where the intervention would be used. 33 Because the inquiry occurs while CGM is in use, this method does not rely solely on the patient’s or caregiver’s ability to recall hypoglycemic events. Observing the use of CGM monitors and readers (device scanners) and mobile apps for presenting data would allow researchers to capture nuances that patients or caregivers may not be able to articulate, and to gather insights into factors (eg, other tasks, people, environment) that may affect CGM use. This could inform products that guide design. For example, a journey map captures the patient’s and caregiver’s CGM experience in a timeline, with facilitators and barriers marked along the way. Among patients’ journey, a high variability of symptoms and problems extending beyond memory (eg, changes in personality, impulsive behavior, impaired judgment, and limited motor skills) may require different CGM design solutions or intervention implementations. HFE methods could inform recommendations for effective and safe CGM considering patient profiles (ie, personas) and use cases.
The needs assessment should involve patients’ primary care clinicians and geriatricians, if they are involved in care. Complex routines and regimens for tighter glycemic control with medications increase the risk of hypoglycemia. Information in electronic health records is often incomplete, hidden, or fragmented across screens, 34 complicating recognition and interpretation of hypoglycemia risk factors. 21 HFE can leverage opportunities to integrate CGM into the electronic health record 17 and introduce data into care processes and workflows of geriatricians, primary care physicians, pharmacists, and nutritionists. The CGM data are expected better inform clinical decisions related to patients as ADRD progresses, especially related to hypoglycemic events. Team-based task analyses could be used to visualize and better understand clinicians’ mental frameworks, including their goals, performance of routine tasks, decision-making process, and information needs.
Design: Involving Patients, Caregivers, and Clinicians
Patients with ADRD-DM and their caregivers or clinicians could collaborate on the design of CGM adaptations for supplemental data collection methods and role-based information displays or dashboards. HFE design methods involve users of a tool in the creation of tangible or visual prototypes over multiple iterations. These prototypes serve as a focal point of communication for transforming users’ requirements into specific interface content and functionality. 35 Codesign workshop is one example of an HFE design method, involving both users and professional designers to promote an open process of collaborative design. For example, a codesign workshop could focus on designing mobile apps with intuitive information displays for caregivers that provide glucose measurements, highlighting patterns among out-of-range glucose values and recommending resources. Involving patients and their caregivers in the design of novel CGM information displays is also likely to enhance their involvement in shared decision making and health care coordination.
Evaluation: Before and After Implementation
HFE evaluation methods are used to determine how well interventions satisfy user requirements both in simulations of prototypes and in research after implementation of the redesigned product. Individual or comparative measures of effectiveness, efficiency, or satisfaction can be assessed while users interact with prototypes in simulated environments. These environments support usability testing with a controlled level of realism, which reduces risks from unintended consequences. Patients with ADRD-DM and their caregivers could evaluate prototypes of redesigned CGM devices, hypoglycemia alarms, and information displays. This would provide insights into how users of the prototype understand and react to out-of-range glucose levels in a safe environment. 36
Moreover, in situ usability evaluations integrated with clinical trials or implementation studies should be used to guide continuous human-centeredness and quality. Evaluations after implementation are essential to identify the need and support for additional adaptations caused by disease progression, patient-caregiver sociodemographic variability, and sociotechnical changes in clinical settings.
Potential of CGM for Detecting Hypoglycemia in ADRD-DM Populations
There is a pressing need to study and support interactions of patients and their caregivers and clinicians for hypoglycemia management. HFE can help to investigate an existing, effective hypoglycemia detection method for people with ADRD-DM. Extending CGM to patients with ADRD-DM is consistent with recent calls for increased attention to multiple chronic conditions in dementia care and expanded use of smart home monitoring technologies for older adults. 37 CGM also aligns with aims to confer agency on patient-caregiver dyads by providing information and supporting decision making. 38 CGM data can supplement care measures in a population at need while minimizing discomfort and caregiver burden, 39 facilitating clinical decisions, and addressing needs for behavior and medication changes, specialty referrals, and education.
Hypoglycemia in older adults with ADRD-DM is a significant problem and cause of morbidity and mortality. Appropriately designed CGM systems for this population can detect and prevent hypoglycemia. HFE methods can identify and inform CGM designs for the ADRD-DM population, broadening CGM access to increase detection of the silent threat posed by hypoglycemia.
Footnotes
Acknowledgements
We acknowledge Lynn Whittaker for her assistance with editing.
Abbreviations
ADRD, Alzheimer’s disease or related dementias; ADRD-DM, Alzheimer’s disease or related dementias and diabetes mellitus; CGM, continuous glucose monitoring; HFE, human factors engineering.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael Weiner reports stock ownership in AbbVie Inc, Amgen Inc, Boston Scientific Corporation, Bristol-Myers Squibb Company, IBM, Integer Holdings Corp, Johnson & Johnson, Mallinckrodt PLC, Mead Johnson & Company, LLC, Medtronic, Mylan N.V., Novo Nordisk A/S, Perspecta Inc, Pfizer Inc, Roche Pharmaceuticals, Senseonics, Stryker Corp, Teva Pharmaceutical Industries Ltd, and Walgreens Boots Alliance, Inc. Rich Holden provides paid scientific advising to Cook Medical. April Savoy reports stock ownership in Pfizer Inc. and GSK (GlaxoSmithKline) Plc. David Klonoff is a consultant to Eoflow, Fractyl Health, Lifecare, Integrity, Rockley Photonics, and Thirdwayv. All other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Savoy is supported by a Career Development Award from the National Institute On Aging of the National Institutes of Health under Award Number K01AG076971. Dr Savoy was also supported in part by the following grants KL2TR002530 and UL1TR002529 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. Drs Savoy and Weiner are supported in part by VA Health Services Research and Development Center for Health Information and Communication (CIN 13-416). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, National Center for Advancing Translational Sciences, or Department of Veterans Affairs.