
Abstract
Untreated gestational diabetes mellitus (GDM) is a leading cause of maternal and fetal morbidity and mortality. 1 Current guidelines recommend self-management of blood glucose (SMBG) fasting and one or two hours postprandially.1-3 Use of continuous glucose monitoring (CGM) during pregnancy in women with GDM has the potential to reduce burden and improve fetal outcomes; however limited data are available on its use.4-6 Intermittently scanned continuous glucose monitoring (isCMG) may be an appealing choice for GDM.
Women with GDM diagnosed after 24 weeks gestation were recruited. Participants were trained on SMBG (FreeStyle Lite) with recommendation to check fasting and one-hour postprandial and if symptoms of hypoglycemia unless otherwise instructed by their usual care providers. Nutritional counseling was provided. Participants were randomized to adjunctive use of isCGM (FreeStyle Libre). Blinded-CGM was placed for participants in the SMBG-group for 2 weeks at enrollment, 32 weeks, and 36 weeks gestation. Participants were contacted weekly. Hemoglobin A1c (HbA1c) and maternal/fetal outcomes were recorded. Target glycemic range was defined as 63 to 140 mg/dL. Results were analyzed for participants who returned any devices for download. Descriptive statistics of demographics, glycemic metrics, and outcomes are reported.
Thirteen women were enrolled. One participant withdrew consent, and two did not return devices. Data for ten women were obtained (age 33 ± 4 years, 40% non-Hispanic white; Table 1). Enrollment and follow-up were limited due the COVID-19 pandemic. One woman in the SMBG group had a history of polycystic ovarian syndrome. Eight women were diet-controlled, and one in each group was managed with medication. Mean HbA1c was 5.4% ± 0.3%.
Participant Demographics, Glycemic Metrics, and Outcomes.
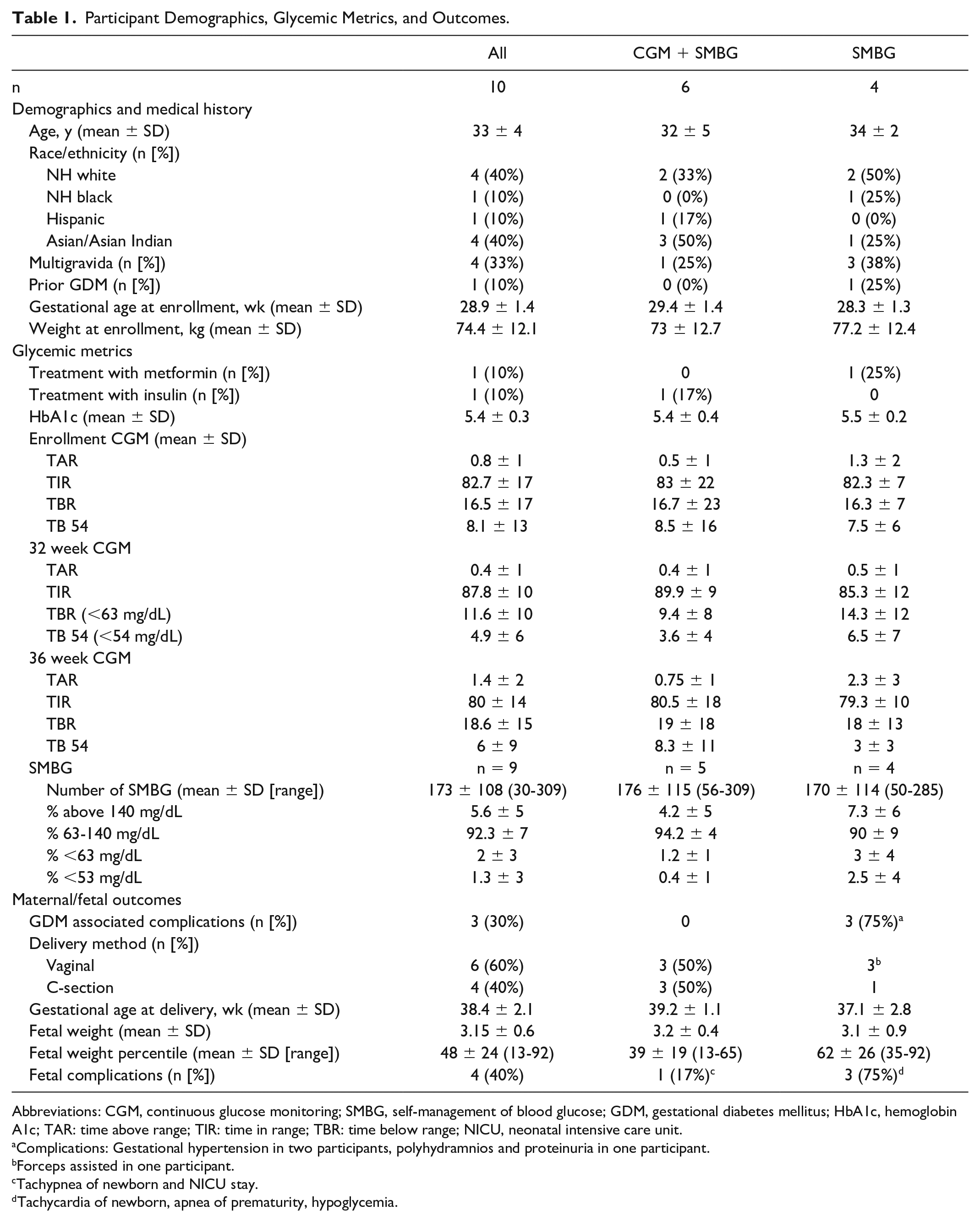
Abbreviations: CGM, continuous glucose monitoring; SMBG, self-management of blood glucose; GDM, gestational diabetes mellitus; HbA1c, hemoglobin A1c; TAR: time above range; TIR: time in range; TBR: time below range; NICU, neonatal intensive care unit.
Complications: Gestational hypertension in two participants, polyhydramnios and proteinuria in one participant.
Forceps assisted in one participant.
Tachypnea of newborn and NICU stay.
Tachycardia of newborn, apnea of prematurity, hypoglycemia.
Mean time in range (TIR) was 82.7% at enrollment, 87.8% at 32 weeks, and 80% at 36-weeks, and was similar between groups. Compared with overall fingerstick testing, CGM data reported lower time above range (TAR) and higher time below range (TBR). Two of the SMBG-group and one of the CGM-group had >10% of SMBG >140 mg/dL. One infant was >90th percentile (mean weight 3.15 kg).
Management of GDM can be burdensome. In a relatively short time period, multiple lifestyle changes, monitoring, and potentially medications are initiated. Continuous glucose monitoring has the potential to facilitate robust data gathering in a short time, and use during pregnancy is recommended by many consensus guidelines. The group enrolled in this study had relatively well-controlled GDM. The TIR was similar between groups. When compared with SMBG, there were more low and fewer high glucose levels detected by CGM. Given that only one participant was using insulin (who had 8% TBR, 2% TB54), the clinical relevance of these lower levels is uncertain. The international consensus on TIR determined there was not enough data to make recommendations for goal TIR or TAR for GDM; however, observational studies have shown that limiting TAR to <10% should be achievable. 4 This feasibility study was not powered to make comparisons between groups or study outcomes, but does highlight the potential use of CGM during GDM and the need for more studies. Newer CGM with lower mean absolute relative difference (MARD), especially in the lower ranges, would be useful to clarify the high rates TBR seen in our cohort.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of Natalia Viera Feliciano, MD, and Laura Kovacs, CDCES, for participant recruitment.
Abbreviations
CGM, continuous glucose monitors; GDM, gestational diabetes mellitus; HbA1c, hemoglobin A1c; isCGM, intermittently scanned continuous glucose monitoring; MARD, mean absolute relative difference; SMBG, self-management of blood glucose; TAR, time above range; TBR, time below range; TIR, time in range.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GOM receives research support from Tandem Diabetes, Dexcom, and Abbott-Diabetes paid to her institution. EN has no disclosures to report. SO receives research support from Tandem Diabetes, Dexcom, and Abbott-Diabetes paid to her institution. CL receives research support from Tandem Diabetes, Dexcom, and Abbott-Diabetes paid to her institution. CJL receives research support from Tandem Diabetes, Dexcom, and Abbott-Diabetes paid to her institution and has served as a consultant and CME speaker for Dexcom and as a consultant for Eli Lilly.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded as an investigator-initiated study for which device and research team support was provided by Abbott-Diabetes.