
Abstract
Background:
The coronavirus pandemic of 2019 (COVID-19) forced worldwide recognition and implementation of telehealth as a means of providing continuity of care by varied health care institutions. Diabetes is a global health threat with rates that continue to accelerate, thereby causing an increased need for clinicians to provide diabetes care and education to keep up with demand. Utilizing technology to provide education via phone/smartphone, video/audio, web, text message, mobile apps, or a combination of these methods can help improve patient access and clinical outcomes, cut costs, and close gaps in care.
Methods:
While numerous publications have summarized the various tools and technologies available for capturing remote clinical data and their relevance to diabetes care and self-management, this review focuses on self-educational telehealth tools available for diabetes self-management, their advantages and disadvantages, and factors that need to be considered prior to implementation. Recent relevant studies indexed by PubMed were included.
Results:
The widespread use and popularity of phones/smartphones, tablets, computers, and the Internet by patients of all age groups, cultures, socioeconomic and geographic areas allow for increased outreach, flexibility, and engagement with diabetes education, either in combination or as an adjunct to traditional in-person visits. Demonstrated benefits of using health technologies for diabetes self-management education include improved lifestyle habits, reduced hemoglobin A1C levels, decreased health care costs, and better medication adherence. Potential drawbacks include lack of regulation, need for staff training on methodologies used, the requirement for patients to be tech savvy, privacy concerns, lag time with technology updates/glitches, and the need for more long-term research data on efficacy.
Conclusions:
Telehealth technologies for diabetes self-education improve overall clinical outcomes and have come a long way. With increasing numbers of patients with diabetes, it is expected that more optimal and user-friendly methodologies will be developed to fully engage and help patients communicate with their physicians.
Introduction
The prevalence of diabetes is growing exponentially in the United States as well as worldwide, rendering it a persistent global health threat. 1 According to the Center for Disease Control’s 2020 National Diabetes Statistics Report, more than 34 million Americans have diabetes, which is roughly 10.5% of the total population. 2 The worldwide economic burden associated with diabetes and its complications is expected to surpass two trillion dollars by 2030. 3 There is an urgent need for educational intervention across the globe to help patients learn to better manage diabetes, prevent its complications, and improve their quality of life. 4 It is recommended by the Association of Diabetes Care and Education Specialists for patients newly diagnosed with diabetes to receive an initial education consultation by a Certified Diabetes Care and Education Specialist (CDCES) and at least annually thereafter to optimize the ability to self-manage. 5
Diabetes self-management education (DSME) is an effective way to help achieve optimal patient clinical outcomes and reduce health care costs. The National Standards for Diabetes Self-Management Education and Support define DSME as “the ongoing process of facilitating the knowledge, skill, and ability necessary for prediabetes and diabetes self-care. This process incorporates the needs, goals, and life experiences of the person with diabetes or prediabetes and is guided by evidence-based standards.” 4 Successful diabetes management depends on consistent daily self-care on the part of patients and their families. A sound educational approach and collaboration with health care practitioners, specifically CDCES, is key to teach patients these critical self-management skills. 6 Unfortunately, the demand for diabetes education and care, due to the continued increasing cases worldwide, can potentially outpace the supply of clinicians available to provide instruction in the next decade. 7
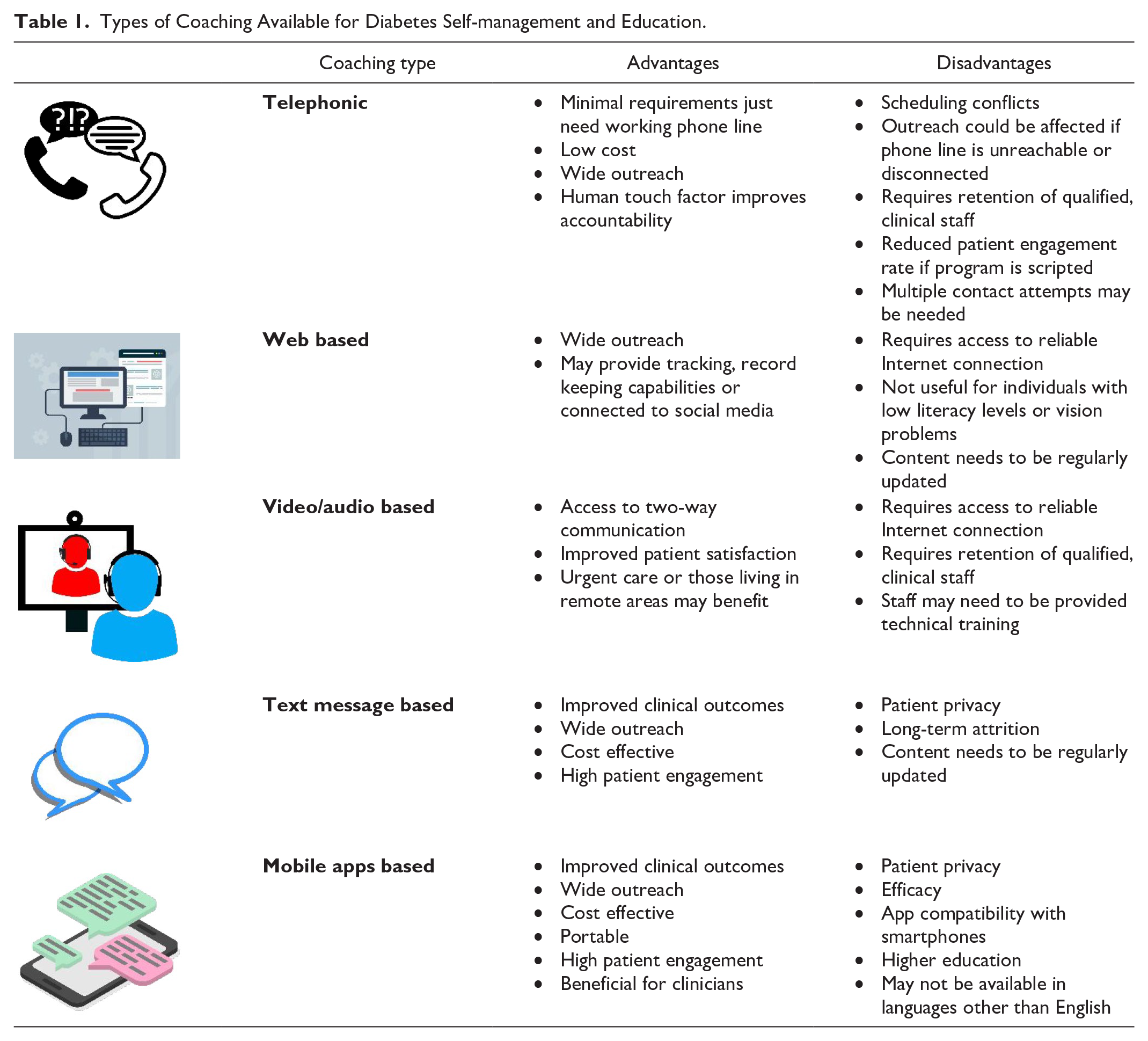
In recent years, technology has been integrated with diabetes education either as an adjunct to or substitution for traditional in-person diabetes education, to improve access, enhance efficacy, and close gaps in care. 7 Using telehealth and digital resources for providing diabetes education has received acceptance by patients and providers alike. Indeed, the advent of the coronavirus disease of 2019 (COVID-19) pandemic has dramatically increased the interest and need for telehealth-based diabetes care and education for preventing delays and gaps in care while allowing for social distancing. The rise and advancements in digital health technology have led to a multitude of modalities to engage and educate patients via telephone/smartphone, video/audio, web, text message, and mobile apps, as well as a combination of any of the above methods. In this narrative review, these various options for utilizing technology to provide diabetes patient education are described and discussed, with specific attention to the benefits as well as the drawbacks 8 of each modality (see Table 1).
Types of Coaching Available for Diabetes Self-management and Education.
Telephonic Coaching
Research indicates that patients with diabetes who receive live telephonic coaching for a targeted period of time can benefit through regular monitoring of health status, thereby improving self-efficacy and overall health outcomes. The scope of these types of programs can vary based on the goals and objectives. Several health insurance plans, wellness programs, and pharmaceutical and medical device companies have started offering telephonic support in an attempt to help bridge the gap between patients and their health care providers.9-12
Generally, telephonic support programs involve 15- to 30-minute duration weekly, biweekly, or monthly telephone calls offered by a health coach, registered dietitian (RD), registered nurse (RN), or CDCES. The calls focus on helping improve patient’s understanding of disease, identifying SMART goals, troubleshooting, and addressing any potential barriers. 13 Reduction of hemoglobin A1C levels has been a significant positive impact that has been accomplished through telephonic support.12,14 Support can also lead to reduced hospitalization rates, surgery cost, and overall health care cost. 15 The requirement for this type of support is very minimal, mainly the presence of a working landline or cell phone connection. In addition, some programs use platforms integrated with the health care provider’s database that can enable timely updates and remedial measures from the provider. Coaching usually occurs remotely and may or may not incorporate the use of several technological components such as text, e-mail, video conferencing, and other modalities that use artificial intelligence (AI). 13 Some telephonic programs focus on improving diabetes self-management outcomes by monitoring medication adherence; however, they may be very scripted and therefore limited in providing support. Other programs may incorporate a pre-determined curriculum that covers various aspects of diabetes and chronic disease management that are less scripted, thus helping patients close any gaps in care.16-18
Due to their relatively lower cost, wide outreach, and opportunities to provide an interactive platform, telephonic support programs are gaining momentum in today’s real-world setting. Patients living in remote areas, elderly individuals, those with limited literacy, vulnerable populations, or those who have limited access to health management services could benefit extensively by participating in these types of programs.19,20 Some patients feel that the human factor makes them accountable to the diabetes coach and this helps them stay motivated and on track to achieve outcomes. 16
Just as with any other program, telephonic support programs have certain drawbacks that must be kept into account. Scheduling conflicts could potentially lead to patients dropping out of the program. Phone-based programs require retention of qualified, trained clinical staff, which, over the long term, can add to the cost of running the program. Cost efficacy also depends on the number of attempts made to reach the patient, number of connected calls, as well as the duration of the calls. 21 In addition, phone programs could experience reduced patient engagement rate over a period of time, especially if the program is very scripted and not creating a significant, positive impact in the patient’s disease management skills. Keeping this limitation in mind, it is important to develop curricula and lesson plans that patients find interesting and motivating.22,23 Several phone plans are prepaid or pay-as-you-go plans; disconnected phone service could lead to abrupt discontinuation from the program. Due to this, the program may not be able to deliver to its full potential and the clinician or health coach may not receive professional satisfaction either.20,22
Video-/Audio-Based Coaching
In recent years, social media platforms, streaming services, and Web sites that upload and post diabetes self-management–related content have been trending. Video-based diabetes education can be a very effective method for assisting patients either by directing them to on-demand video links uploaded on a digital platform or by providing them with an opportunity to connect with a live coach.24,25 In the past, video support was largely incorporated in the form of CDs and DVDs wherein lesson plans and educational content were recorded. Since the onset of COVID-19, in an attempt to maintain social distancing and to assist with regional or national lockdown measures, use of virtual platforms such as Zoom, WebEx, Microsoft Teams, Google calls/chat, TeamViewer, and many others has been adopted by many. 26 These communication platforms have improved the scope for virtual diabetes well visits, follow-ups with clinicians, and assistance with real-time troubleshooting. 27 Virtual platforms such as Zoom have been very helpful, especially during the COVID-19 pandemic; however, some of these platforms did not offer end-to-end encryption, thus making them non-compliant with Health Insurance Portability and Accountability Act (HIPAA) regulations. Regular upgrades to the software, setting a password required for manual admission of users to the meeting, using virtual area networks, and dual authentication when logging into the device are all ways to reduce cyber security risks. 28 To ensure compatibility with HIPAA guidelines and data security, it is also important to train providers and implement a robust endpoint security feature. 29
Some diabetes education programs may provide web links that direct to prerecorded videos on the company’s Web site or links to videos housed in YouTube, Box, or other platforms. Virtual, live coaching programs provide real-time access to a diabetes clinician who could be a pharmacist, nurse, diabetes education specialist, dietitian, exercise physiologist, therapist, or the physician. These programs offer support either by integrating communication platforms or by using specialized video software. The range of services can vary from counseling, medication adjustments, and overall diabetes management to troubleshooting glucometers, insulin pens and pumps, trackers, and other wearable devices. 30 Using video games to promote diabetes education such as by creating interactive quizzes and trivia questions is becoming increasingly popular especially among adolescents and young adults. 31 A study conducted by Gupta et al compared the effectiveness of video-based, interactive diabetes education program with usual care and concluded that video-based programs improve glycemic control and hemoglobin A1C reduction. 32 Another study conducted by Hansen et al demonstrated that video consultations were highly beneficial in decreasing hemoglobin A1C by an average of 0.69% compared with clinic-based care alone. 33
The major benefit of video-based coaching is providing access to a two-way communication platform. 24 On the other hand, audio streaming in the form of podcasts has provided patients the opportunity to tune in and listen to diabetes self-management topics of interest. However, this only facilitates one-way communication and may be largely tapped into by patients who are extremely self-motivated. Some studies have found that video-based coaching can be a very cost-effective option and the personal interaction with this type of coaching can lead to improved patient satisfaction.34-36 Urgent care needs and patients living in remote areas with access to Internet may greatly benefit from video coaching.34-36 For patients living in remote areas, video-based telehealth programs have been shown to improve access to diabetes care, reduce health care expenses, and improve health outcomes. 37 In addition, it can help reduce expenses associated with travel as well as any inconvenience related to being away from home or work. 37 Telemedicine diabetes consultations are cost-effective, and benefits are similar to conventional treatment. Providers have also reported improved quality of clinical care, better continuity of services, and improved coordination. 37 Not surprisingly, a major shortcoming expressed by patients was a lack of physical contact (“human touch”) with the provider normally experienced during an in-person consult. 34
Both video- and audio-based programs require the availability of trained, clinical staff to deliver content through prerecorded lessons or live coaching. To provide live coaching, staff need to be provided with technical training. 38 It is also important to maintain a secure environment and ensure access to adequate space for setup. Patients need access to reliable Internet connection as well as secure space when using live coaching. Technological issues can sometimes lead to frustration and thereby increased patient dropout rates.39,40
Web-Based Diabetes Education
Web-based education is an effective tool for facilitating diabetes self-management. Some Web sites solely offer diabetes-related content and resources while others also offer an opportunity to interact with a coach. 41 Many diabetes telehealth programs are based on Diabetes Prevention Program (DPP) and require coaches to possess DPP lifestyle certification. Coaches are credentialed as RDs, RNs, exercise physiologists, or social workers and may, in addition, possess a masters or doctoral degree. 42 Diabetes Prevention Program offers their diabetes curriculum using a web-based platform. 43
Diabetes-related Web sites offer a plethora of information that may include prerecorded videos or interactive lesson plans to enhance diabetes education and self-management.
Some Web sites also offer online record keeping tools where patients can track and monitor their diet, physical activity routine, as well as print reports or logs. 44 Many Web sites include blogs, healthy recipes, menus, and holiday meal planning guides. Some of the clinical web-based supportive educational tools include virtual chatting, message boards, e-mailing options, or options to connect with a live diabetes coach. Technologically advanced Web sites are linked to social media platforms or integrated with glucometers, pedometers, continuous glucose monitoring (CGM) devices, and other wearable devices that allow for real-time glucose monitoring. Incorporating analysis of patient-generated health data (PGHD) from such devices can enhance patient education and counseling. Providing the patient with specific data, such as trends in glucose values, logged dietary habit changes, and steps counted, can help pinpoint areas that need improvement, as well as provide documentation of lifestyle and treatment goal attainment. Indeed, a study conducted in young adults and adolescents newly diagnosed with diabetes and using CGM devices found that web-based training improved health outcomes and adherence. 44 Similarly, another prospective study that focused on individuals diagnosed with type 2 diabetes and prescribed real-time continuous glucose monitoring system reported that remote personalized coaching in combination with video-based coaching decreased HbA1c by 1.6% compared with baseline levels. 45
Interactive Web sites can tremendously assist patients in diabetes self-management by offering them tools and resources that improve knowledge, and by providing online tutorials and training for remote device initiation and usage. Web-based diabetes education is cost-effective 46 and is capable of disseminating information to a vast majority of the population. They can also help monitor or maintain a database of clinical outcomes.47-49 Many Web sites nowadays include content and resources in regional languages other than English to reach out to diverse populations.50-52
One of the most important requirements for diabetes-related informative Web sites is to ensure that the information is regularly updated with the most current information. The content needs to be credible and backed by scientific-based evidence. From the host standpoint, this also means they need to regularly maintain and upgrade their servers. Computer programmers and web developers can assist in this task. From the end-user standpoint, access to secure Internet connection, through cell phone, tablet, or computer, is required. 53
Web sites that provide tracking or monitoring tools that save the patient’s personal information need to ensure that data are not compromised and are compliant with HIPAA guidelines where applicable. Web sites that include message boards and online forums may require the presence of a moderator who can monitor content or comments being posted. The layout of the Web site, text font, and design also needs to be user-friendly. Web sites that integrate with a live coach or clinician need to ensure adequate staffing and coverage by an expert for the available support hours as listed on the Web site. Despite its far-reaching scope, web-based education is not beneficial for those with low literacy levels, for those with limited Internet access, or for those individuals with poor vision. Myers et al 54 sought to address the issue of disparity by providing patients with an electronic device equipped with Internet connectivity during the study period. They reported that end users needed to be trained on the appropriate use of the device and its features for attaining optimum benefit. 54 For patients with visual impairment, more frequent telephone calls and onsite visits can improve overall treatment satisfaction and outcomes.
Text Message–Based Education Programs
Smartphones continue to rise in popularity with an estimated 290 million users as of 2021. 55 One of the primary and most popular capabilities of smart phones, text messaging, has shown a great deal of promise in being utilized for mobile health (mHealth) education and promotion. 56 Text message–based health education can be implemented in a wide variety of patient populations with multiple intervention capabilities and has been shown to improve outcomes in a range of chronic diseases, including diabetes. 56
Text messaging can help provide and reinforce DSME, addressing key areas including diet, medications, physical activity, and motivation for self-care and behavior change. 56 There is ample evidence to suggest that text message interventions can lead to improved blood glucose levels, decreased hemoglobin A1C, and weight loss, as well as increased medication adherence.1,57-59 In addition, text message–based education has been associated with improved health behaviors such as dietary change, increased physical activity, better quality of life, and enhanced health literacy in patient users.59-62 Moreover, text messaging is a very prevalent, universally accepted mode of communication. Research indicates that text messaging is successful for educational outreach in multiple age groups, ranging from adolescents to the elderly, and in patients with varied socioeconomic and cultural backgrounds.1,43,61,63
There are many benefits associated with using text messaging as a method of educational intervention, leading to its well-documented efficacy in changing health outcomes in variety of populations as listed above.1,56-59,61,63,64 Test messaging is a cost-effective, wide-reaching, easy-to-use means of providing education. It can be used as a stand-alone intervention or as an adjunct to in-person counseling, alongside virtual, Internet, and smartphone app–based education programs. 56 Use of text messaging may be favorable to clinicians because it can be pre-developed as an automated system of educational messages at predetermined intervals and the educational intervention can be generalized or individualized as desired. 64 Providers can opt to use one-way delivery or instead employ two-way text communication allowing the patients to interact, ask questions, and provide needed feedback. Little technical expertise is required by the patient and messages are often read immediately, with the information coming directly to them, rather than the patient having to take time to seek it out. 64 Text messages can provide succinct, useful tidbits of information, helpful reminders, and promote goal-oriented behavior, providing new material or reinforcing education already provided in an in-person or virtual coaching session. Previous research has revealed high patient engagement and satisfaction rates with text-based education.64,65
Certain limitations and practical considerations must be recognized when opting to use text message–based education methods. Some health barriers and challenges cannot be addressed by text messages alone, namely via one-way text, and need to be combined with additional interventions, such as in-person or virtual counseling. 66 Although text message–based programs have the potential for high participation and engagement, it is important to address known issues such as maintaining enrollment as well as attrition in the long term during program creation. 67 When developing a messaging program, many aspects need to be considered including the target audience, education and behavioral change objectives, the framework of the program such as the timing and frequency of messages sent, desired customization, and the degree of interaction allowed (one way vs two way). 68 Patient privacy must also be addressed, with the primary concern being transmission and storage of protected health information and following HIPAA Security and Privacy rules. In contrast to simple personal text messaging, larger scale operations for health care require more complex and specialized application software and services. Selecting a particular platform to run the education program will depend on the needs associated with the intervention, desired degree of customization, price point, and the amount of organizational resources available for start-up.
Mobile App–Based Diabetes Education
Mobile health apps have grown exponentially in the last decade, with an estimated 350 000 medical and wellness applications available in the health care and consumer marketplace. 69 Smartphones are most commonly used platforms for mHealth. Apps range from simple text message interventions to more sophisticated versions available for variety of purposes in diabetes self-management including monitoring of blood glucose, medication and dosing of insulin, and tracking weight, diet, and physical activity. Thus, mHealth apps enhance patient-practitioner communication and allow for remote patient monitoring as well as delivering health education.70,71
Mobile heath apps for diabetes education serve the purpose of increasing patient knowledge, skills, and abilities to promote optimal self-management. Education-focused apps can range from providing general diabetes education to supporting more individualized and personalized instruction and interventions. General diabetes education on topics such as basic lifestyle and self-care guidelines, namely food and activity regimen information, can be provided via messages, videos, reminders, and interactive educational games or quizzes.71,72 In addition to stand-alone apps that provide education and information, more in-depth and personalized app programs exist. These apps integrate PGHD such as weights, blood glucose values, and food/activity information habits provided by the patient. Patient-generated health data are manually entered by the patient via the app and in some cases data automation is an option via Bluetooth technology and cable connections to provide data capture of blood sugar values and physical activity from CGM devices, blood sugar meters, and pedometers. 71 Some apps offer communication features whereby data from the mobile device are e-mailed to clinicians for review who can then contact patients for subsequent follow-up education and instruction. Other apps use decision support and AI to provide education in response to patient-entered data such as carbohydrate intake, blood glucose values, and medication usage. Mobile diabetes management software that incorporates a feedback algorithm can send educational messages to patients after receiving their data. 73 Additional oversight via clinician coaching (virtually or telephonic) can be delivered concurrently with the mobile app. 73
Education via mobile apps, especially when personalized, has shown to improve dietary habits, increase physical activity, 74 lead to better medication adherence, 75 and promote self-blood glucose monitoring. 76 Decreased hemoglobin A1C in response to mobile apps–based diabetes education has also been demonstrated. A pilot study conducted by Kim et al 77 revealed that use of a patient-centered, android smartphone app–based diabetes care system, which integrated patient data from a Bluetooth-connected glucometer, a digital food diary, and a wearable activity monitoring device to provide patients with blood glucose alerts, need-based provider communication, and diet/activity/self-management educational modules, resulted in significant decreases in fasting blood glucose and hemoglobin A1C values.73,77,78 Mobile health apps can be an affordable, portable, easily available, and user-friendly means of providing diabetes education and encourage a healthy lifestyle. Their popularity and high user satisfaction have been demonstrated in age-groups ranging from adolescents to the elderly and in both patients with type 1 and type 2 diabetes. Such apps are, therefore, important adjuncts to enhance and reinforce diabetes education provided by clinicians.71-73,77,79
Mobile health apps also have limitations and concerns. Out of the thousands of apps available to consumers, many are oversimplified, lack long-term clinical data on efficacy, and are not formally evaluated for safety, accuracy, and data privacy.70,80 There is no standardized process by which mHealth apps are reviewed and monitored and not all apps are cleared by regulatory agencies. Mobile health apps such as those that perform insulin-dosing calculations are regulated by the European Medicines Agency and the US Food and Drug Administration. 80 Consistent and clear criteria for evaluating app features designed for diabetes education, along with their potential efficacy in improving patient outcomes, need to be developed. A recent study suggested that a helpful means of evaluating apps for use in diabetes education is to compare their features with the evidence-based American Association of Diabetes Educators’ seven self-management behaviors, a well-known framework for achieving behavior change. 81 The analysis revealed that the majority of diabetes self-management apps have features supporting healthy eating, blood glucose monitoring, taking medications, and being active, whereas many were lacking in promoting healthy coping, problem-solving, and reducing risks (as these are areas often covered by more direct interaction with a health care provider). Efficacy of diabetes app use has been evaluated in several studies by demonstrating improvement in health-related outcomes, such as lower hemoglobin A1C, fasting blood glucose values, and increase in self-care behaviors, in both type 1 and type 2 diabetes patient populations, although data have been mixed. The overwhelming number of apps and their subsequent technological updates, along with the lack of structured guidelines for assessment and categorization of health apps, can prove difficult for consumers and clinicians to keep up with the latest availability to make informed recommendations and choices.69,82 Apps that require manual data entry on the part of the patient can require significant effort and time commitment to receive educational benefits which can lead to user fatigue and higher drop-off rates. 82 App compatibility with specific smartphones and technical glitches can also be a concern for usability. Other barriers to adoption of mHealth include needing a higher education level and English language competency (as many apps are English only). 83 Mobile apps do show promise in aiding diabetes education and self-management; however, those that provide more comprehensive educational approaches, integrated with PGHD, and have sound data on efficacy are more often developed and used in the research setting and less widely available for consumers.51,69,80,82,84,85
Future and Combined Technologies for Diabetes Education
One future technology that is becoming more prevalent in diabetes care and education is AI.86-88 Artificial Intelligence is defined as “the science and engineering of making intelligent machines, especially intelligent computer programs. It is related to the similar task of using computers to understand human intelligence.” Artificial Intelligence is currently being used for diabetes education and will continue to develop to aid in the areas of diabetes prediction, more personalized dissemination of education that may be linked to patient adherence and clinical outcome, lifestyle guidance, insulin injection and dosing suggestions, blood sugar monitoring, and screening/surveillance of complications.
An effective approach to diabetes education can also be achieved by combination of two or more technologies for a more comprehensive intervention. Mobile health (text messages and apps), web-based, and telephonic methods for educating can be used together and in conjunction with in-person or virtual counseling. 89 Examples of mixed methods approaches include the use of telephonic counseling with follow-up text messages or web-based educational video modules in combination with virtual or telephonic counseling. Mobile apps can be employed for capturing PGHD; the resultant data can be analyzed and used for education via AI-based decision support such as feedback text messages in combination with personalized counseling via a web portal. Programs that offer telephone visits, text messages, and access to information via Web sites, as well as the opportunity for capture/transmission of personal health data, can be useful for interventions in both in-person and group counseling sessions as an adjunct to office visits. 90 Increasing the number of interactions with patients, namely using text messages, helps keep patients engaged and does not place a heavy burden of participation on the patient as the messages come to them and are accessible anywhere. 91
Conclusion
The growing numbers of patients diagnosed with diabetes and other chronic diseases have the potential to overwhelm the health care system. Lack of accessibility to resources as well as financial and food insecurity will only further exacerbate it. Diabetes coaching programs that incorporated various digital health technologies for providing self-management education have been shown to help improve overall clinical outcomes by empowering patients and providing them with tools, resources, and support for efficiently managing their chronic disease conditions. In addition, implementation of telehealth technologies enables patient outreach on a larger scale compared with traditional diabetes self-management programs. Importantly, many of the tools developed can also be used for managing other chronic conditions and comorbidities.
The advent of COVID-19 has further promoted the use of telehealth for connecting with patients. Challenges faced during the COVID-19 pandemic in terms of in-person meeting with patients required expansion of the scope of practice, adoption of innovative modalities, and development of effective telehealth tools and programs that could be used exclusively or added on to traditional diabetes self-management programs.
While the use of telehealth in DSME has come a long way, several key issues need to be addressed. Incorporating risk reduction and problem-solving capabilities while tracking behavioral change will help further optimize these programs. Providing adequate training to health care professionals and patients, as well as integrating HIPAA compliant security features, will enhance effective usage of these tools, resulting in improved outcomes. Adequate funding for implementation of the programs including reimbursement criteria by insurance providers needs to be established. 92 As discussed in this review and shown in Table 1, each telehealth tool has its pros and cons that need to be evaluated carefully in context of the business or clinical practice model to be adopted.
With advancing technologies and implementation of AI in almost every health care–related specialty, it is anticipated that that telehealth-based diabetes education will also undergo continuous research to find optimal ways for engaging patients, addressing potential limitations and barriers for using them, and developing interfaces that allow better communication between patients and their physicians.
Footnotes
Abbreviations
AADE, American Association of Diabetes Educators; ADCES, Association of Diabetes Care and Education Specialists; AI, artificial intelligence; CDCES, Certified Diabetes Care and Education Specialists; CGM, continuous glucose monitoring; COVID-19, coronavirus disease of 2019; DPP, Diabetes Prevention Program; DSME, diabetes self-management education; HIPAA, Health Insurance Portability and Accountability Act; mHealth, mobile health; PGHD, patient-generated health data; RD: registered dietitian; RN, registered nurse; RT-CGM, real-time continuous glucose monitoring system.
Author Contributions
R.S. and V.S. conceptualized the idea for this article; V.S. and M.F. wrote the article; R.S. reviewed and edited the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.