
Abstract
Background:
Telemedicine holds a potential to strengthen self-management support outside health care settings in the everyday management of type 1 diabetes (T1D). However, existing effectiveness reviews are older or include a relatively narrow focus on specific definitions of telemedicine or included databases.
Objective:
To conduct a systematic review of the effectiveness of telemedicine solutions versus any comparator on diabetes-related outcomes among people with T1D.
Methods:
Studies including adults (≥18 years) with T1D published before October 14, 2020, were eligible. Primary outcome was glycated hemoglobin (HbA1c, %). The Cochrane Library, PubMed, EMBASE, and CINAHL were searched. Meta-analysis based on the mean difference in HbA1c% was used to pool effects. The Cochrane tool was applied to assess risk-of-bias, and the certainty of evidence was graded using the GRADE approach.
Results:
A total of 22 studies were included (with 1615 participants). Treatment effect for HbA1c% favored telemedicine (mean difference of −0.26% [95% confidence interval:−0.37% to −0.15%]) with moderate effect certainty. Heterogeneity was moderate (I2 = 33.30%). Although not significant, secondary outcomes were all in favor of telemedicine except number of severe hypoglycemic events and diabetes knowledge, but the certainty of the evidence for those outcomes was all low or very low.
Discussion:
Reducing average HbA1c% levels are important to combat the risk of diabetic complications and premature death. However, the evidence mostly consist of small studies with a relative short duration and the estimated pooled effect is smaller than could be expected from quality improvement strategies in general for diabetes management.
PROSPERO number:
CRD42020123565.
Introduction
Type 1 diabetes (T1D) is a chronic disease that requires constant decision-making in terms of self-management and monitoring, which often results in poor adherence to recommended guidelines. 1 Self-management is often highlighted as the cornerstone in the management of T1D and has previously been associated with improvements in different health-related outcomes. 1 Self-management consists of different modalities such as educational, psychological, behavioral, and clinical assistance activities to help the patient navigate through his or her condition. 2 Thus, support for self-management is highly encouraged as part of the management of T1D. 1
Application of telemedicine is emerging as a way to strengthen self-management support outside health care settings in the everyday management of diabetes.3,4 Different conceptions of what constitutes the concept of “telemedicine” are common. Sood and colleagues reported 104 different definitions in a review of the term.
5
In this review, we apply the World Health Organization (WHO) definition of telemedicine as the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities.
6
What constitutes the “delivery of health care services” and “valid information for diagnosis, treatment and prevention” is somewhat open for interpretation. Therefore, the definition is further elaborated to include four elements that have been used previously7,8: (1) information are obtained from a patient (whether audio, video, measured physiological data, or written responses) and then (2) electronically transferred over a geographical distance to (3) a health professional who exercise skill and judgment (4) in the provision of tailored feedback to the patient. Both synchronous and asynchronous technologies apply. Asynchronous telemedicine is defined as store-and-forward transmission of patient information with non-real-time communication (eg, email, text messaging, Internet platform), whereas synchronous telemedicine refer to real-time communication and transfer of data. A combination is also applied to include setups where data whereas collected asynchronously, while follow-up communication was conducted synchronously. Wearables and sensors are encompassed within the telemedicine definition, when automated patient-data are transferred over a distance with a health professional at the receiving end, who evaluates the data and gives feedback to patients. Similar conceptualizations of telemedicine that includes sensors can be found, for example, Klonoff and colleagues, who applied a framework that distinguishes between “sensor-based” and “non-sensor-based” telemedicine. 9
A recent systematic review and meta-analysis reported that telemedicine can be considered a safe option for providing self-management support for people with diabetes. 10 However, existing T1D effectiveness reviews of telemedicine lack a meta-analysis or pool results from diverse study designs, 11 include a narrow definition of telemedicine or relatively few data sources, 12 and do not include an assessment of the certainty of the evidence for included outcomes.11-13 The same can be said for reviews pooling both T2D and T1D.14-16 Moreover, because of the rapid development in the field of telemedicine, a new systematic review and meta-analysis within the field is indicated.
The objective of this study is therefore to systematically evaluate the effect on HbA1c% levels and other secondary outcomes found in existing telemedicine solutions versus any comparator without the use of telemedicine among adults with T1D.
Methods
Study Design
This study is a systematic review with embedded meta-analysis, which is conducted and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 17 The study is PROSPERO registered with identification CRD42020123565 on April 2020. A study protocol with comprehensive search protocol covering T1D, T2D, and gestational diabetes mellitus (GDM) has previously been published 18 and summarized below.
Eligibility Criteria
This review considered all studies published prior to October 14, 2020 that included adults (≥18 years), who had a diagnosis with T1D. Studies that reported mixed disease populations (eg, diabetes and chronic obstructive pulmonary disease) and mixed diabetes types were also included if the results related to the population with T1D were reported separately. Studies which only included participants at risk of diabetes or having prediabetes were excluded. Studies were eligible if they included interventions with remote feedback or communication between a patient and health care professionals, either as substitutes or alternatives to usual care. Fully automatic interventions were also considered. The primary outcome was glycemic control measured as change in glycated hemoglobin (HbA1c%). Only randomized controlled trials (RCTs) were considered, both parallel and cross-over designs. Studies published in English, Danish, Norwegian, or Swedish as peer-reviewed full-text papers were included.
Information Sources
The search was performed on October 14 in the Cochrane Library Central Register of Controlled Trials (CENTRAL), PubMed, EMBASE, and CINAHL by two authors (SHL, SH) with the help of a research librarian. Web of Science, SCOPUS, and Google Scholar were applied for additional citation searches.
Search Strategy
The search protocol covering T1D, T2D, and gestational diabetes is presented in Appendix 1. To qualify the systematic search, an initial unstructured search to identify relevant terms was performed in PubMed and CINAHL. The search strategy in the following systematic search was thereafter adapted for each database. Search terms included different synonyms, near-synonyms, acronyms, and spellings for all index terms and keywords. Thesaurus, Boolean operators, abstract/title/keywords, phrase, truncation, free text, and advanced search were utilized. With an eye to identifying additional studies, citation searches were applied.
Study Selection
All eligible studies were uploaded into RefWorks (Refworks, RefWorks-COS, ProQuest RefWorks 2.0, 2010) where duplicates were removed using the functions Exact duplicates and Close duplicates. Two authors (SH, JA) then screened title and abstracts with respect to adherence to the eligibility criteria of the review. Three authors (SH, SHL, JA) then conducted a full review of the remaining studies. Any disagreement between the three authors was resolved through discussion or by inclusion of other authors resulting in a final sample of studies. Reasons for exclusion of studies in the full review were recorded.
Data Extraction
A standardized worksheet in Microsoft Excel (2016) was applied by three authors (SHL, SH, JA) to extract data from studies. These included trial characteristics (author, publication year, country, sample size, study duration), patient characteristics (age, gender, body mass index [BMI]), and HbA1c outcomes. Furthermore, the characteristics of the telemedicine interventions were extracted including the purpose of the different components (general glycemic improvements, diet, exercise, medication, fatigue, diabetes education, and prevention of hypo- or hyperglycemic events), the type of peripherals (eg, blood glucose monitors), involved health professions in the delivery of telemedicine, synchronous or asynchronous implementation, and implementation context (eg, hospital, specialized diabetes clinic, university, community, or cross-sectional). Authors resolved potential disagreements through discussion with an option to include additional authors. If studies reported other measures than means and standard deviations (eg, medians and confidence intervals [CIs]), these were transformed by traditional methods19,20 and scaled to HbA1c% when relevant (eg, if outcomes was reported as mmol/mol).
Assessment of Methodological Quality
Two reviewers (JA, FWU) assessed the risk of bias of all included studies independently using the revised Cochrane tool 21 and potential disagreements were resolved by discussion.
Data Synthesis
An overall treatment effect was estimated with a meta-analysis based on the mean difference (MD) from each study. I2 tests were used to assess heterogeneity. Results were combined with either a random or fixed effects model (depending on if the I2 statistic was higher or lower than 50%, respectively). Results were subject to post hoc subgroup analysis of all extracted study and participant characteristics (continuous variables were binary divided into groups based on variable means). Sensitivity analyses were applied to investigate the impact on results by excluding potential study outliers. Visual inspection of the funnel plot and Egger’s test were used to evaluate publication bias. Analyses were all performed in Stata 16 (StataCorp).
Certainty Assessment
A Summary of Findings (SoF) Table was created using GRADEPro GDT 2015 (McMaster University, ON),22,23 which presents the absolute effect for the groups (treatment and control) and ranking of the quality of the evidence for each included outcome. In the handbook for GRADE, 24 these are based on overall judgments of the risk of bias, 25 indirectness, 26 imprecision, 27 inconsistency, 28 and risk of publication bias. 29
Results
Figure 1 is a flowchart overview of the selection of studies. From the systematic search, 16 309 studies were identified (11 062 after duplicate removal) of which 1125 studies were full-text assessed after screening titles and abstracts. Finally, 22 articles met the inclusion criteria.
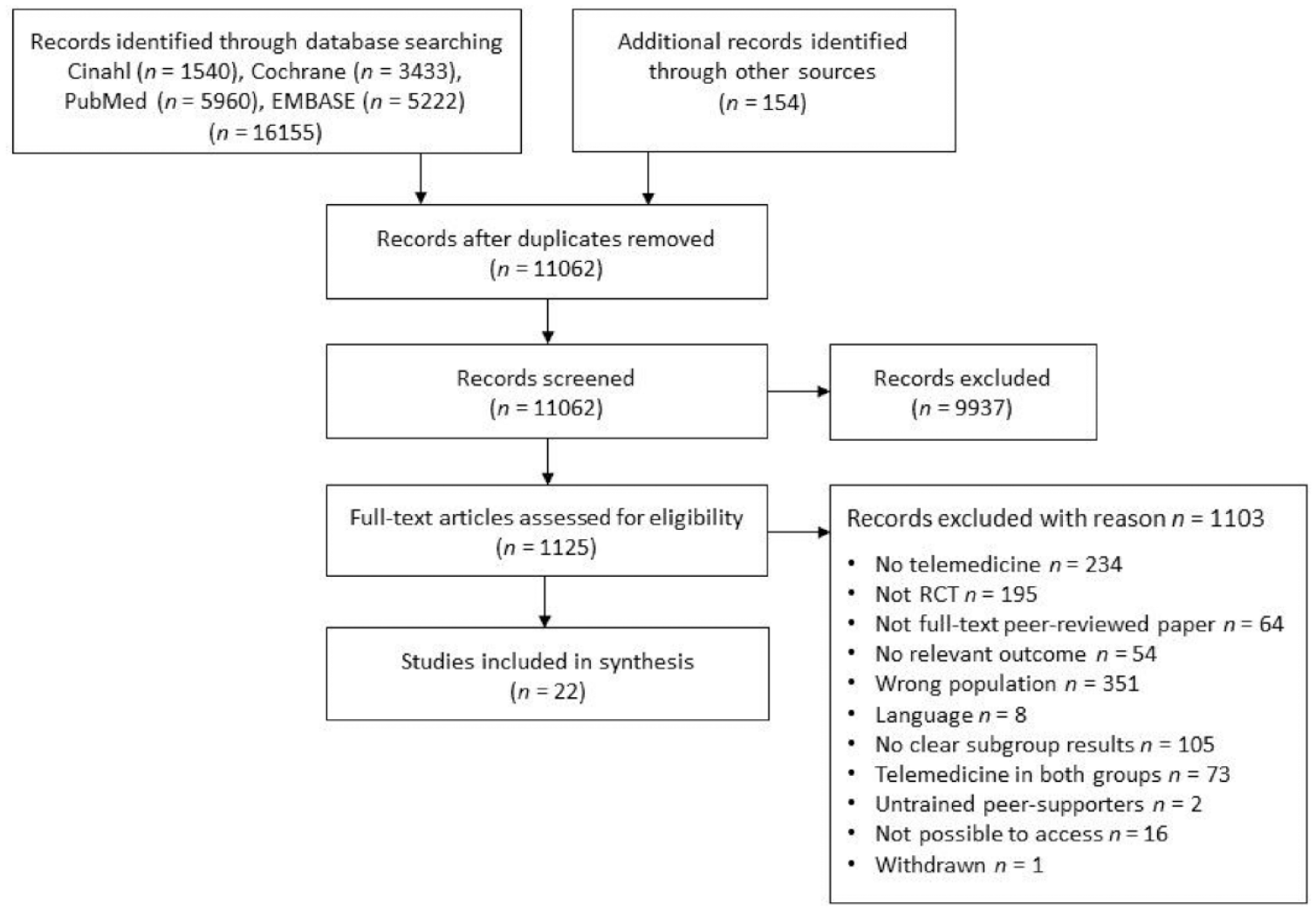
Selection of studies.
Study references and characteristics are shown in Table 1. Two studies were published prior to 2000 (9%), eight in the 2000s (36%), and 12 in the 2010s (55%). One study was multinational (5%), whereas 14 studies were from Europe (64%), four from North America (18%), two from Asia/Middle East (9%), and one from Australia/New Zealand (5%). Size of studies varied from 10 to 158 participants averaging 73 per study. Mean study duration was six months ranging from one to 12 months. Mean proportion of men was 26% (range 0%-67%), average age 35 (range 24-44), mean baseline BMI was 24.9 (range 22.78-26.10), and average baseline HbA1c% was 8.7% (range 7.35%-10.89%).
Study and Participant Characteristics.
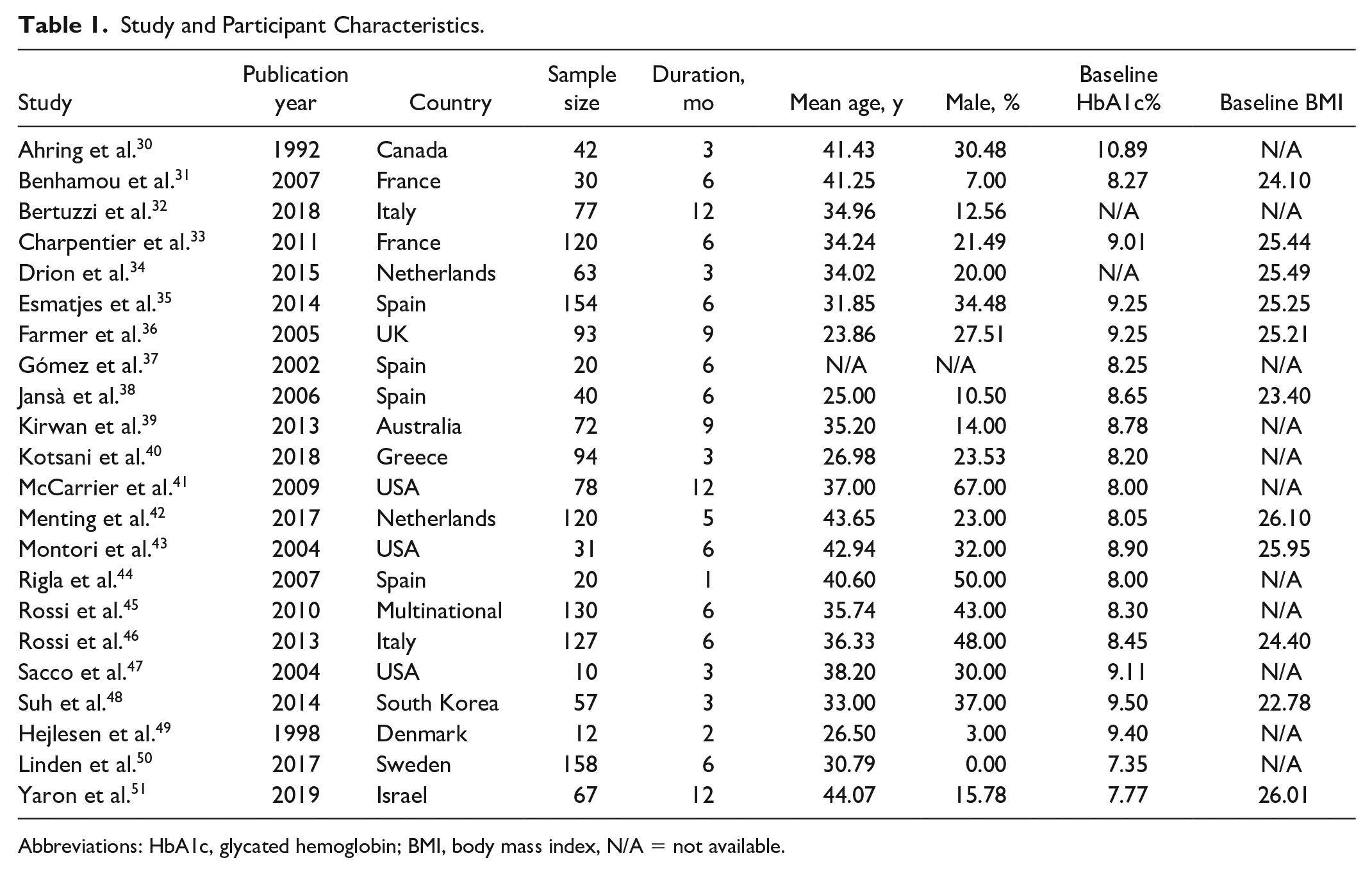
Abbreviations: HbA1c, glycated hemoglobin; BMI, body mass index, N/A = not available.
Characteristics of the telemedicine technologies are illustrated in Table 2. One study had daily contacts (5%), eight biweekly (36%), six weekly (27%), three studies a monthly contact (14%), and one study (5%) less frequent (twice in the study period). Across studies, 13 used a web portal (59%), nine included a blood glucose meters (BGMs) (41%) (one study also supplemented with a continuous glucose monitor, (CGM) [5%]), eight a telephone (36%), six a smartphone or tablet application (27%), six mail correspondence (27%), and four applied SMS communication (18%). Two studies applied a synchronous setup (9%), nine an asynchronous (41%), and 10 studies a combination of synchronous follow-up communication with asynchronous monitoring data transfer (45%). The purpose of intervention components were glycemic improvement (19 studies, 86%), dietary support (17 studies, 77%), medication support (17 studies, 77%), exercise support (13 studies, 59%), educational (11 studies, 50%), prevention of glycemic events (hypo- or hyperglycemia) (five studies, 23%), and fatigue improvement (one study, 5%). The telemedicine interventions were staffed by physicians in nine studies (41%), diabetes nurses in five studies (23%), coaches or psychologists in four studies (18%), a diabetes team in three studies (14%), and a research team in one study (5%). One study used the same health care professions to staff the control group (5%), three did not (14%), whereas 18 studies did not report sufficient details (82%).
Telemedicine Intervention Characteristics.
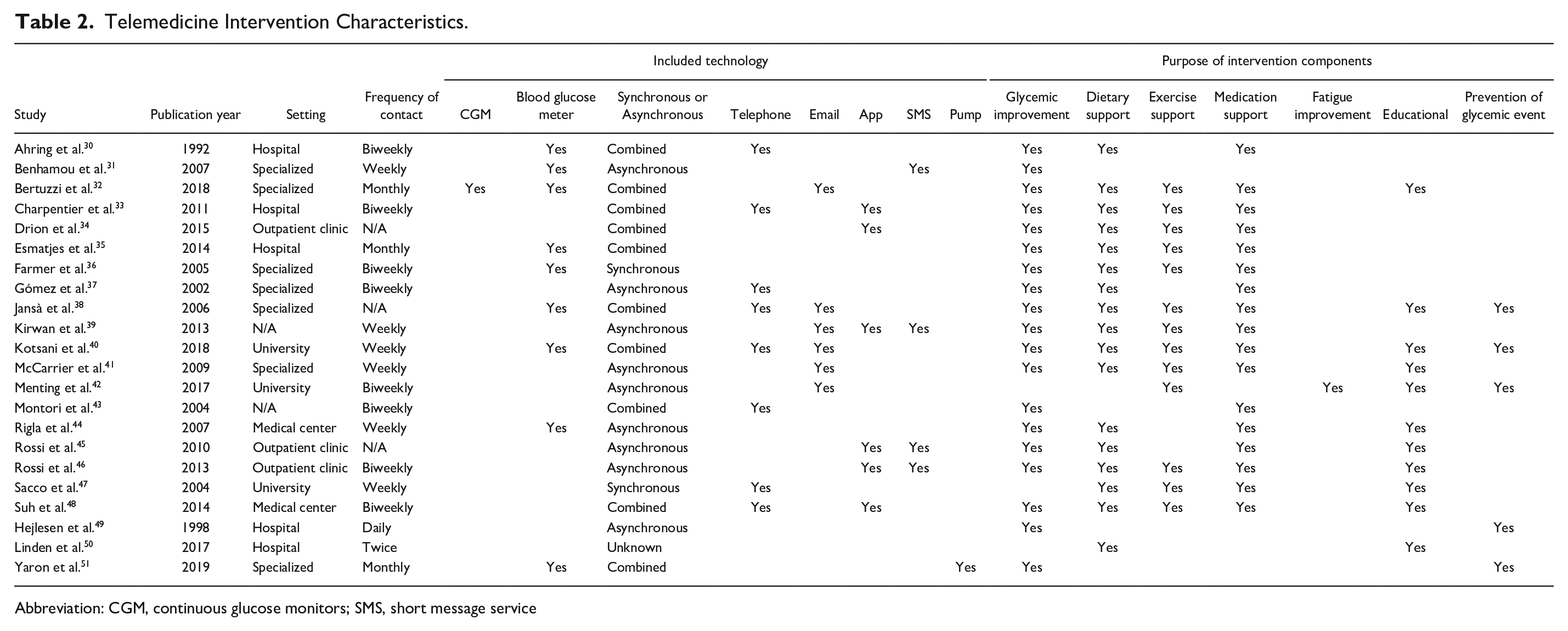
Abbreviation: CGM, continuous glucose monitors; SMS, short message service
Figure 2 presents the result of the risk of bias assessments across studies (Appendix 2 contains individual study assessments). Overall, a high risk of bias was evaluated in 50% of the included studies, moderate in 41%, and low in 9%. This is primarily due to missing outcomes at follow-up. A high proportion of studies (59%) reported results of complete case or per-protocol analyses without appropriate consideration of the potential impact of missing data when loss-to-follow-up are unbalanced or drop-out reasons are different across allocation (ie, testing the missing data mechanism or assuming missing at random followed by imputation and/or tests for association with baseline variables and missingness and/or performing sensitivity and/or adjusted analyses).
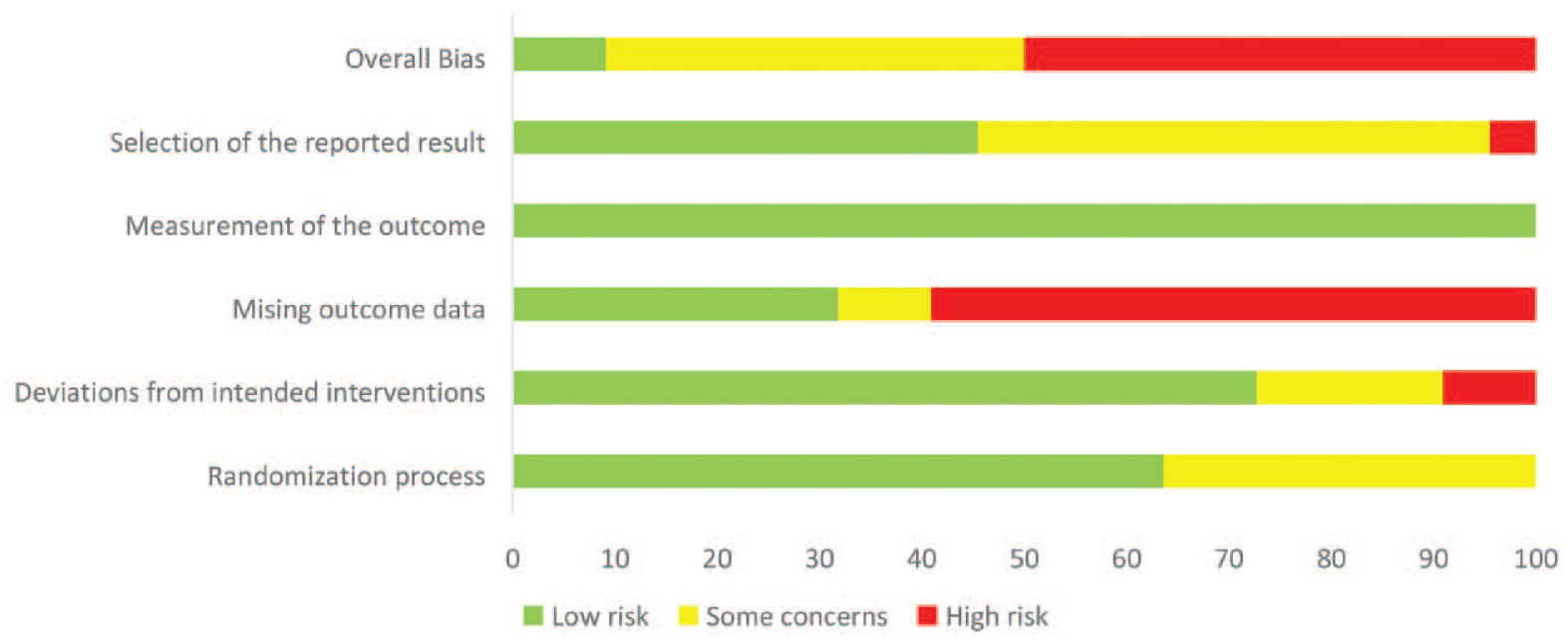
Overview of the risk of bias assessments.
Effect on HbA1c%
The results from the meta-analysis and individual studies are shown in Figure 3. The MD for HbA1c% was −0.26 (95% CI: −0.37 to −0.15) favoring telemedicine. Heterogeneity was moderate (I2 = 33.30%). Studies published in North America (MD −0.71 [95% CI: −1.12 to −0.30]) or Australia/New Zealand (MD −0.78 [95% CI: −1.23 to −0.33]) and studies with no educational component (MD −0.39 [95% CI: −0.54 to −0.23]) or a proportion of man lower than 26% (MD −0.38 [95% CI: −0.54 to −0.21]) exhibited significantly larger HbA1c% treatment effects as shown in Appendix 3. Removing study outliers (Sacco and colleagues and Ahring and colleagues), because of a combination of an old publication date and relatively large treatment effects, decreased the MD to −0.25 (95% CI: −0.40 to −0.10) as seen in Appendix 4.
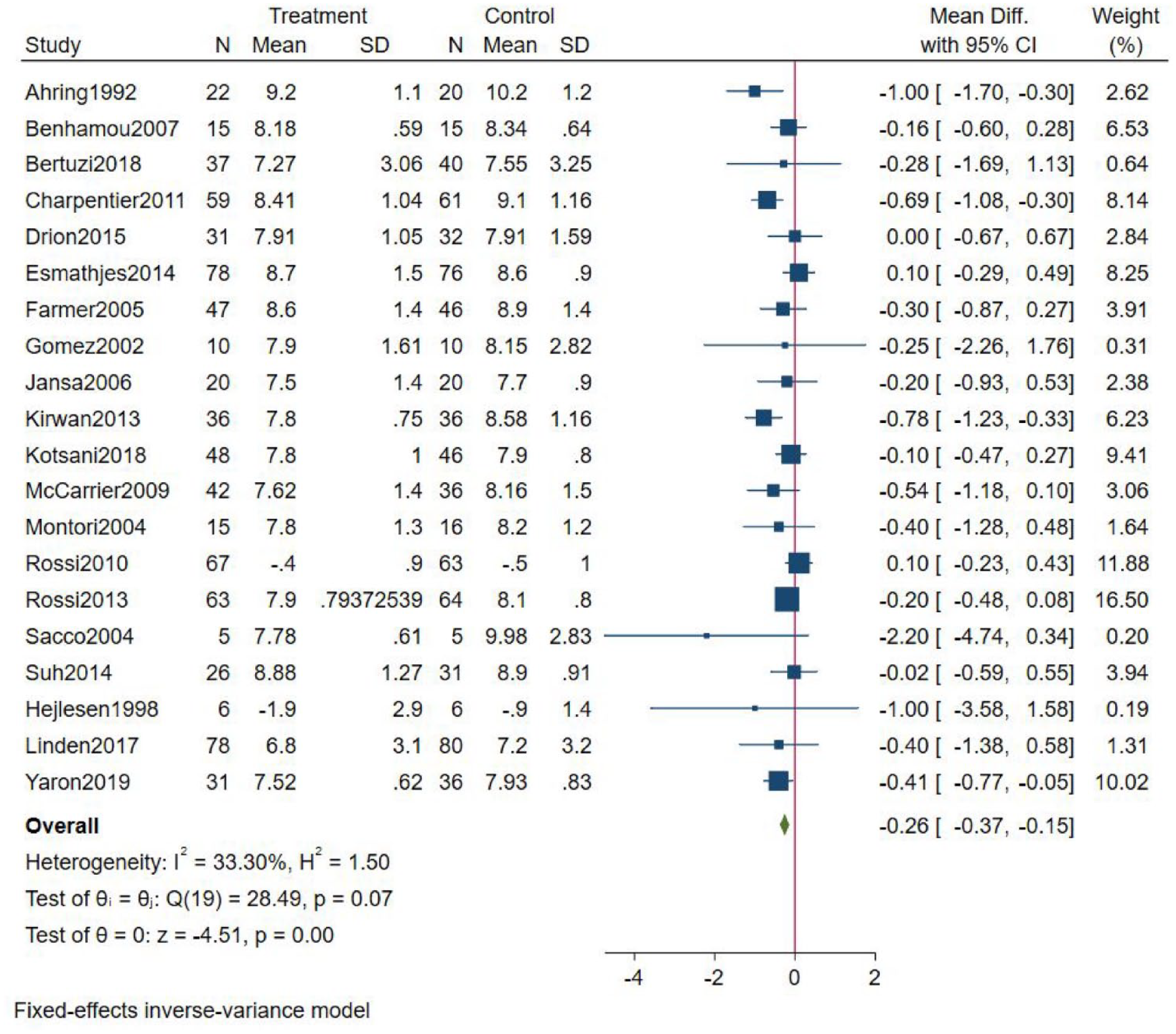
Results from the meta-analysis.
Secondary Outcomes
Included secondary outcomes were weight loss, fasting blood glucose, the number of severe hypoglycemic events, diabetes knowledge, systolic and diastolic blood pressure, total cholesterol, high- and low-density lipoprotein, and triglycerides (Appendix 5). All outcomes favored telemedicine except the number of severe hypoglycemic events and diabetes knowledge, which was slightly in favor of the comparator, but none are statistically significant (at a 5% level).
Certainty of Findings
The certainty of evidence of the calculated treatment effect of HbA1c% was judged as moderate due to serious problems with risk of bias (Table 3). Inclusion criteria for this review were broad and evidence were therefore not downgraded due to indirectness, although studies have a relatively short follow-up. The overall effect size was statistically significant and passed the optimal information size criteria. Publication bias was not strongly suspected. The funnel plot (Figure 4) was somewhat asymmetrical favoring telemedicine and Egger’s test was insignificant (P = .1499). Industry sponsorship was declared or unknown in 14/22 studies (in 12 of these cases private companies supplied the telemedicine equipment only) and there was no relation between presence of industry sponsorship, study size, or estimated average treatment effect. No upgrades to the evidence were made. The certainty of the secondary outcomes was low for severe hypoglycemic events and weight loss and very low for fasting blood glucose, diastolic and systolic blood pressure, total cholesterol, low- and high-density lipoprotein, triglycerides, and diabetes knowledge.
Summary of Findings (GRADE Profile).
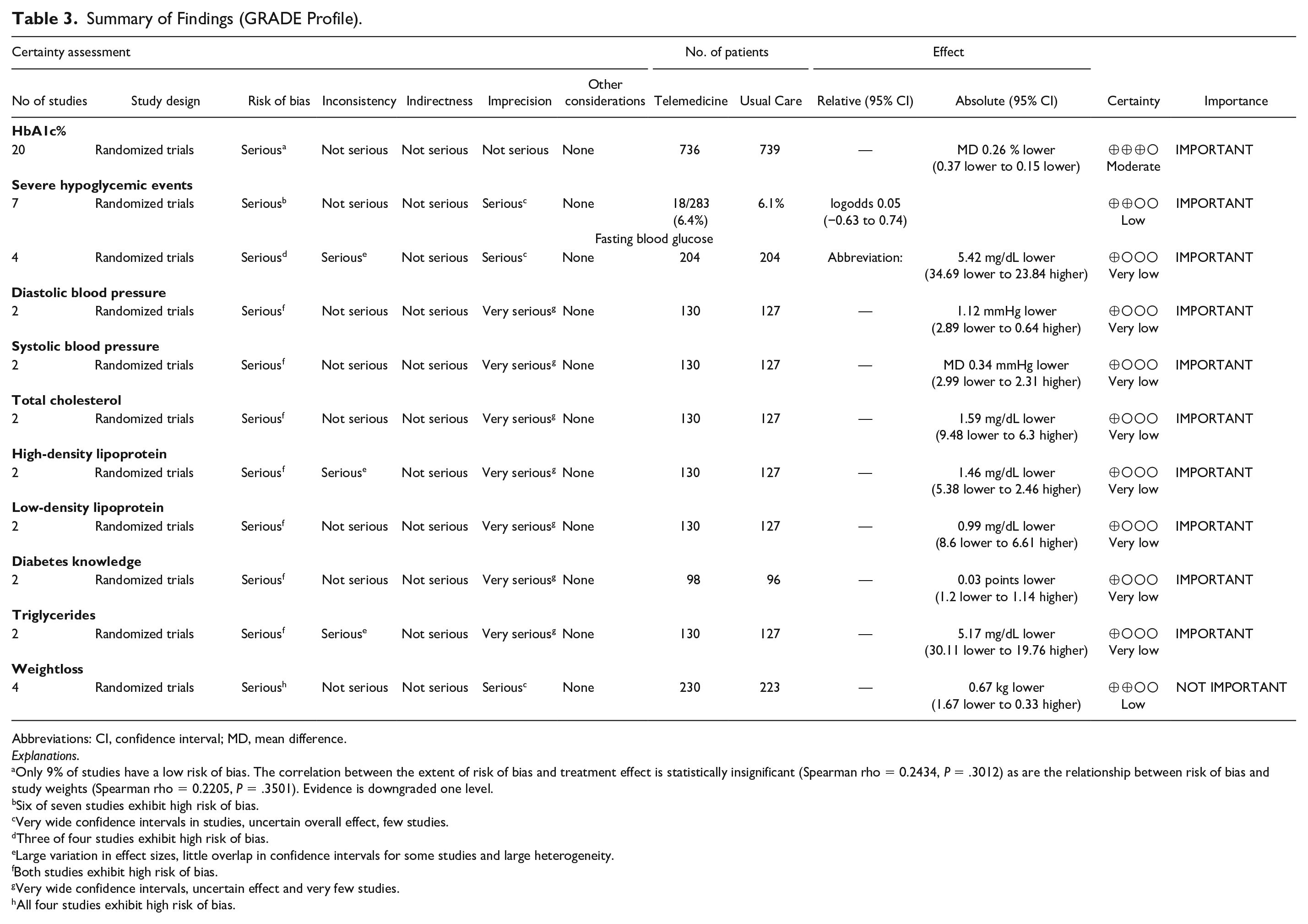
Abbreviations: CI, confidence interval; MD, mean difference.
Only 9% of studies have a low risk of bias. The correlation between the extent of risk of bias and treatment effect is statistically insignificant (Spearman rho = 0.2434, P = .3012) as are the relationship between risk of bias and study weights (Spearman rho = 0.2205, P = .3501). Evidence is downgraded one level.
Six of seven studies exhibit high risk of bias.
Very wide confidence intervals in studies, uncertain overall effect, few studies.
Three of four studies exhibit high risk of bias.
Large variation in effect sizes, little overlap in confidence intervals for some studies and large heterogeneity.
Both studies exhibit high risk of bias.
Very wide confidence intervals, uncertain effect and very few studies.
All four studies exhibit high risk of bias.
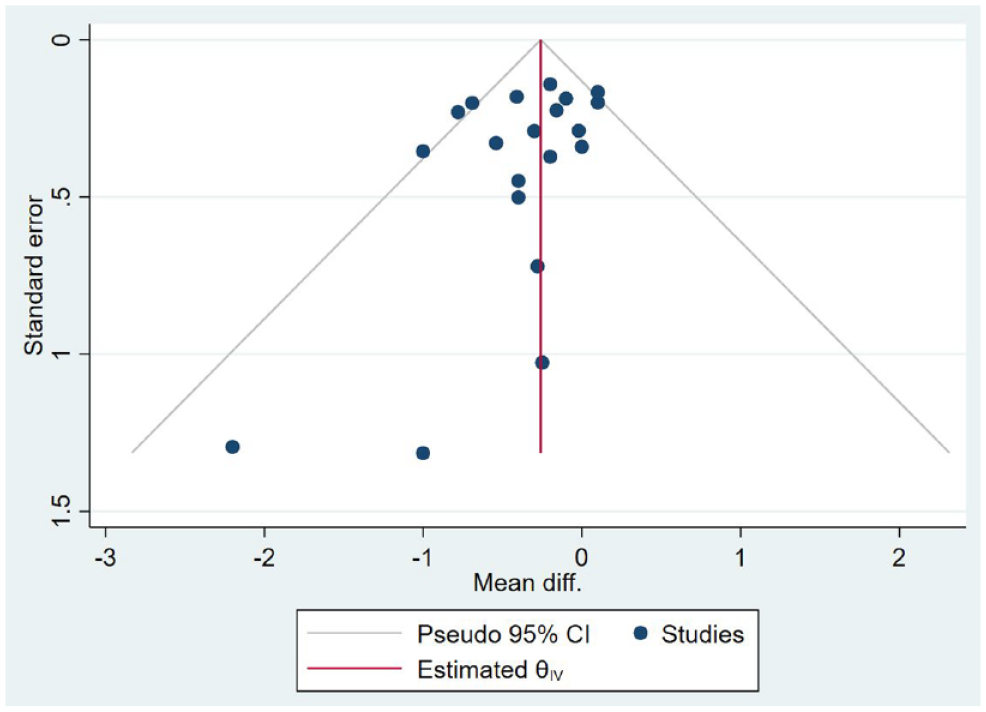
Funnel plot. Abbreviation: CI, confidence interval.
Discussion
The pooled results of this review favored telemedicine (MD −0.26 [95% CI: −0.37 to −0.15]) and were robust to outliers. A moderate heterogeneity was found (I2=33.30%). Subgroup analyses revealed that studies with a relatively low proportion of men or with no educational component as well as publications from North America and Australia/New Zealand reported significantly larger effects of telemedicine. Secondary outcomes mostly favored telemedicine, but none were significant. Current evidence certainty on the primary effect on HbA1c% was moderate and lower for all secondary outcomes.
Comparison With Other Reviews
Results are comparable with the two most recent systematic reviews of telemedicine for patients with T1D. Operating with a much narrower definition of telemedicine and without certainty assessment, Wang and colleagues 12 found a similar effect in a 2019 study (MD −0.25 [95% CI: −0.41 to −0.09]) including eight RCTs from three databases. Lee and colleagues 13 have estimated a lower treatment effect (MD −0.18 [95% CI: −0.33 to −0.04]) with a different target T1D population. They included 28 RCTs published up to 2016 that, in addition to our study, also included studies from PsycInfo. Furthermore, they concluded that the evidence of effect on HbA1c% was more uncertain (very low) because of serious problems with risk of bias, inconsistency, and indirectness. We did not find critical problems with heterogeneity and, on the balance, we conservatively did not downgrade HbA1c% for indirectness, as we found no statistically significant differences across studies with different lengths of follow-up and intervention characteristics.
Implications
The treatment effect demonstrated in this study is slightly less than could be expected of other quality improvement strategies for diabetes management (MD −0.37, derived from 120 studies). 52 Thus, there might be other initiatives that will lead to a higher effect on participant blood glucose levels. In addition, published studies are small with a relatively short duration. As telemedicine studies are unblinded, there is a risk that treatment effects are subject to a Hawthorne effect, 53 which might explain a higher effect in the telemedicine group. However, if a Hawthorne effect was present, it could be expected that treatment effects would diminish over time, which cannot be confirmed (although not statistically significant, the subgroup of studies in Appendix 3 with a follow of 12 months or more report higher average effects than studies with shorter duration [effect on HbA1c% levels are −0.43 vs −0.23, respectively]). Should the average effect be maintained, important gains could be made by the estimated effect of telemedicine. A large prospective study has estimated that lowering average HbA1c levels by 1% would lead to a projected 37% reduction in long-term microvascular complications and a 21% lower mortality in people with type 2 diabetes (T2D). 54 Could these effects be transferred to T1D, telemedicine technologies could hold a potential to reduce microvascular complications by 9.6% (95% CI: 5.6%-13.7%) and mortality by 5.5% (95% CI: 3.3%-7.8%).
A plausible explanation for the higher effect in studies with a lower proportion of men could be that women have been shown to prefer more interactive diabetes resources, because they are more prone to disclose disease to their surroundings. 55 Lower effect of telemedicine with an educational component has previously been linked to the presence of various barriers. 56 However, there is no simple explanation for higher treatment effects in studies published in North America compared with Europe, other than it might just be because of the limited number of studies. Alternative causes could be variations in health care design and structure, technology maturity across markets, participant motivation not reported in the studies, and so on.
Limitations
This study has limitations. First, the limited size of the evidence base combined with a broad definition of telemedicine made it difficult to make firm conclusions about treatment effects especially in subgroups (nonsignificance) and in grading indirectness (studies implemented a variety of concrete technologies under the umbrella-term telemedicine). Second, we have included studies reported before the COVID pandemic. We acknowledge that the pandemic has led to an increased use of video technology and CGMs and that recent experience of telemedicine effectiveness during the pandemic has been published. However, including studies from the pandemic would change the scope for the review. More ad hoc implementation of telemedicine would be expected, when organizations were forced to find new ways of delivering health care leading to results (high or low treatment effects) that might not be generalizable to a context post-COVID (eg, if extraordinary resources were assigned to telemedicine operation, broader target populations were included, assigned health professionals were different). Third, data extraction could have included more baseline data from studies such as time since diagnosis, blood pressure, cholesterol levels, and medication. However, reported baseline data varied considerably and would have led to a relatively large proportion of missing study data. Fourth, for two studies, we did not have data to calculate an MD in HbA1c% because of the lack of outcome data.
Future Research
Telemedicine to people with diabetes is a complex intervention with different purposes of included components, different peripherals, mode, and frequency of contact and patient group characteristics. Moreover, telemedicine is implemented in various sectors and organizational settings. Consequently, experimental evaluation has been criticized for not being able to understand or sufficiently describe which mechanisms and contexts that would make these complex interventions lead to desired outcomes for patients—both average population effects and individually. 57 To accommodate this criticism, a qualitative strategy to increase certainty of T1D outcomes is to conduct more RCT studies that explicitly describe the background for the chosen technology configuration and a theory for how context and mechanisms could lead to which outcomes.
Future reviews should utilize that more RCTs testing CGMs compared with BGMs have been published from 2021 and onward. CGMs provide both people with T1D and health care professionals’ real-time access to glucose information, which recent meta-analyses have associated with some improvement in HbA1c% compared with BGMs.58,59 As previously discussed, careful preplanned subgroups of studies implemented during the pandemic are suggested. Evidence grading is important, because existing CGM evidence within diabetes management in general reported a high heterogeneity, a short study duration, and comprehensive industry sponsorship. 59
Conclusions
There is moderate evidence that telemedicine lead to reduced HbA1c% levels for adults with T1D. This is important to reduce the risk of diabetic complications and premature death. However, the estimated pooled effect is smaller than could be expected from quality improvement strategies in general for diabetes management. Some additional benefits of telemedicine might exist, but the evidence for all secondary outcomes were low or very low.
Supplemental Material
sj-docx-1-dst-10.1177_19322968221076874 – Supplemental material for The Effectiveness of Telemedicine Solutions in Type 1 Diabetes Management: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-dst-10.1177_19322968221076874 for The Effectiveness of Telemedicine Solutions in Type 1 Diabetes Management: A Systematic Review and Meta-analysis by Flemming Witt Udsen, Stine Hangaard, Clara Bender, Jonas Andersen, Thomas Kronborg, Peter Vestergaard, Ole Hejlesen and Sisse Laursen in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors would like to thank research librarian, Connie Skrubbeltrang, who assisted in search of literature.
BGM, blood glucose meter; BMI, body mass index; CENTRAL, Cochrane Library Central Register of Controlled Trials; CGM, continuous glucose monitor; CI, confidence interval; GDM, gestational diabetes mellitus; HbA1c, glycated hemoglobin; MD, mean difference; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; RCT, randomized controlled trial; SMS, short message service; SoF, summary of findings; T1D, type 1 diabetes; T2D, type 2 diabetes; WHO, World Health Organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is an independent manuscript commissioned and jointly funded by the Steno Diabetes Center North Denmark and Aalborg University.
Data Sharing
No additional data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.