
Abstract
Background:
Previous systematic reviews have aimed to clarify the effect of telemedicine on diabetes. However, such reviews often have a narrow focus, which calls for a more comprehensive systematic review within the field. Hence, the objective of the present systematic review, meta-analysis, and meta-regression is to evaluate the effectiveness of telemedicine solutions versus any comparator without the use of telemedicine on diabetes-related outcomes among adult patients with type 2 diabetes (T2D).
Methods:
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We considered telemedicine randomized controlled trials (RCT) including adults (≥18 years) diagnosed with T2D. Change in glycated hemoglobin (HbA1c, %) was the primary outcome. PubMed, EMBASE, and the Cochrane Library Central Register of Controlled Trials (CENTRAL) were searched on October 14, 2020. An overall treatment effect was estimated using a meta-analysis performed on the pool of included studies based on the mean difference (MD). The revised Cochrane risk-of-bias tool was applied and the certainty of evidence was graded using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach.
Results:
The final sample of papers included a total of 246, of which 168 had sufficient information to calculate the effect of HbA1c%. The results favored telemedicine, with an MD of −0.415% (95% confidence interval [CI] = −0.482% to −0.348%). The heterogeneity was great (I2 = 93.05%). A monitoring component gave rise to the higher effects of telemedicine.
Conclusions:
In conclusion, telemedicine may serve as a valuable supplement to usual care for patients with T2D. The inclusion of a telemonitoring component seems to increase the effect of telemedicine.
Introduction
Diabetes is one of the most common chronic diseases and a major health care problem worldwide.1,2 In 2017, an estimated 8.4% of the adult global population had diabetes, which is expected to increase to approximately 9.9% (700 million) in 2045, primarily due to an increase in unhealthy dietary habits, obesity, and sedentary lifestyle.1,2 The global prevalence is predicted to increase mostly in low- and middle-income countries. 3 The economic impact of diabetes is considerable, spans health care services, and affects individuals, families, and national productivity.1,4
Type 2 diabetes (T2D) constitutes approximately 90% to 95% of diabetes cases.1,5 The T2D is a progressive disease associated with significant premature mortality, morbidity, and several complications, such as cardiovascular disease, nephropathy, neuropathy, and retinopathy.6,7 Diabetes patient care is a multifaceted and complex process, mainly aimed at attaining optimal glycemic control to prevent and control diabetes-related complications. 8 However, sustaining optimal glycemic control for people with diabetes is both demanding and challenging because it requires numerous daily self-management decisions and care activities. 9 These challenges include estimating the appropriate diabetes medication dosage to avoid hypoglycemic and hyperglycemic events and adherence to obstacles in terms of following the recommended guidelines.8,9 Adherence to the complex T2D treatment regimen is difficult to maintain 10 and medial adherence rates have been reported to range from 36% to 93%. 11
Self-management strategies are considered an essential part of diabetes treatment and are associated with improvements in health-related outcomes. 9 A potential solution to support ongoing diabetes self-management support is the use of telemedicine, 12 which has been suggested as a promising but unproven approach to support people with diabetes in the management of their disease. 13 Telemedicine can be defined as the delivery of health care services over a distance using information and communication technologies. 14 However, no definitive definition exists. 14 Telemedicine solutions may include a variety of different technologies and various delivery forms, including monitoring, education, consultative services, coaching, and counseling tasks.13,15-17 Telemedicine interventions constitute different constellations, such as simple reminders via text messaging, video consultation, and transmission of patient data (eg, blood glucose, blood pressure, dietary and medication intake, and physical activity) with feedback from health care professionals via web portals or via telephone.13,15,16 As diabetes predominantly needs to be managed outside health care facilities and to a large extent requires self-management, telemedicine holds the potential to provide sufficient self-management support to people with T2D.18,19
Previous systematic reviews have aimed to clarify the effect of telemedicine on diabetes.15-17,20-28 However, these previous reviews have often focused on a specific type of telemedicine, a specific outcome, and/or a specific comparator, which calls for a more comprehensive and inclusive systematic review seeking to compare and synthesize findings for treatment outcomes while adjusting for different study characteristics. In addition, the field of telemedicine is developing rapidly; thus, a large number of studies likely have been published recently, calling for an updated review. 29 Hence, the objective of the present systematic review, meta-analysis, and meta-regression was to evaluate the effectiveness of telemedicine solutions versus any comparator without the use of telemedicine on diabetes-related outcomes among adult patients with T2D.
Methods
Study Design
This systematic review, meta-analysis, and meta-regression was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 30 A comprehensive search protocol was published elsewhere 31 and PROSPERO-registered with identification CRD42020123565 on April 2020. The search was part of a comprehensive search that included T2D as well as type 1 diabetes (T1D) and gestational diabetes 31 , which will be reported separately.
Eligibility Criteria
Studies were considered if they included adults (≥18 years) diagnosed with T2D. Studies that included mixed populations (eg, T1D and T2D) were only included if the data for the T2D population were reported separately. Studies were excluded if only participants at risk of diabetes or participants with prediabetes were included. Furthermore, the studies must have included telemedicine interventions that were substituted for usual practice or served as an alternative to usual practice. The telemedicine interventions had to include remote feedback/communication between a patient and health care professional(s). Alternatively, feedback/communication could occur between the patient and a trained peer. Telemedicine interventions that were wholly automatic were also considered.
Studies that reported on any relevant patient diabetes-related outcome were included. The primary outcome was change in glycated hemoglobin (HbA1c, %).
We only considered randomized controlled trials (RCTs)—both parallel and crossover designs. Studies published in English, Danish, Norwegian, and Swedish as peer-reviewed full-text papers were included. All studies published before October 14, 2020, were considered.
Information Sources
The search was performed in PubMed, EMBASE, the Cochrane Library Central Register of Controlled Trials (CENTRAL), and CINAHL. Two authors performed the database searches (S.H.L. and S.H.). A research librarian assisted. Additional citation searches were performed in the Web of Science, SCOPUS, and Google Scholar.
Search Strategy
Initially, an unstructured search was performed in PubMed, CINAHL, and Google Scholar to identify relevant search terms and thus qualify the systematic search. The systematic search followed the initial search. The search strategy was adapted for each database. The search terms included various synonyms, near-synonyms, acronyms, and spellings for all keywords and index terms. A variety of search functions were applied, including thesaurus, Boolean operators, abstract/title/keywords, phrase, truncation, free text, and advanced search. Citation searches were applied to identify additional studies.
Selection Process
First, all of the identified papers were uploaded into RefWorks (ProQuest RefWorks 2.0, 2010). Second, duplicates were removed using the functions Exact duplicates and Close duplicates. Third, titles and abstracts were screened by two authors with respect to the eligibility criteria of the review (S.H. and S.H.L.). Fourth, the remaining studies underwent full review by three authors with respect to the eligibility criteria of the review (S.H., S.H.L., and J.D.A.). Disagreement between the authors was resolved through discussion by the three authors alone or by inclusion of other authors. During the full review, the reasons for exclusion of studies were recorded, and afterward, a final sample of papers was identified.
Data Extraction
Data were extracted by three independent authors (S.H., S.H.L., and J.D.A.) using a standardized sheet in Microsoft Excel (2016). Extracted data included trial characteristics (author, publication year, country, sample size, and study duration), patient characteristics (age, sex, and body mass index [BMI]), and HbA1c outcomes. In addition, the characteristics of the telemedicine interventions were extracted, including the frequency of contact, implementation setting (primary care, hospital, specialized outpatient clinic, university, community or cross-sectional), peripherals (eg, glucometers, pedometers, blood pressure monitors, and scales), and the general purpose of intervention components (monitoring, consultation, counseling, coaching, education, mentoring, and reminding). Disagreements between the authors were resolved through discussion. Additional authors were included in the discussions when necessary.
Risk of Bias Assessment
The revised Cochrane risk-of-bias tool was applied. 32 Four reviewers (J.D.A., S.H., T.K., and F.W.U.) assessed the included studies independently and resolved potential disagreements by discussion.
Data Synthesis
All statistical analyses were performed in Stata 16 (Stata Statistical Software: Release 16, StataCorp 2019.; StataCorp LLC, College Station, Texas). Reported medians, interquartile ranges, ranges, and confidence intervals were transformed to means and standard deviations by traditional methods33,34 and scaled to HbA1c% when relevant (eg, if outcome was reported as mmol/mol). An overall treatment effect was estimated with a meta-analysis of the pool of included studies based on the mean difference (MD). Heterogeneity was assessed statistically using I2 tests. The results were combined with a random-effects model (due to heterogeneity, ie, an I2 statistic > 50%). Univariate a priori subgroup analyses based on meta-regression of the telemedicine characteristics were conducted and combined with post hoc analyses of the association of study and patient characteristics with the treatment effect of telemedicine. Publication bias was evaluated using visual inspection of the funnel plot and Egger test.
Certainty Assessment
The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was applied. A summary of findings (SoF) table was created using GRADEPro GDT 2015 (McMaster University, Ontario, Canada),35,36 which presents the absolute risks for the groups (treatment and control), estimates of relative risk, and ranking of the quality of the evidence, which is based on the risk of bias, 37 indirectness, 38 imprecision, 39 inconsistency, 40 and risk of publication bias. 41
Results
The flowchart in Figure 1 describes our selection of studies. In the literature search, 16 309 studies were found and 1125 eligible studies were assessed by full-text reading after screening titles and abstracts. After full-text assessment, 246 articles met our inclusion criteria.
Flowchart.
The characteristics of the individual studies are presented in Table 1. One study was multinational, 88 articles were conducted in North America (36%), 84 in Asia (35%), 44 in Europe (18%), 16 in Australia/New Zealand (7%), five in Africa (2%), and five in South America (5%). Four studies were published before 2000 (2%), 50 in the 2000s (21%), 165 in the 2010s (68%), and 24 (10%) in 2020. Sample sizes ranged from 17 to 4078, with an average of 251 participants per study. The study duration ranged from one to 96 months, with a study average of 8.5 months. Across studies, the mean proportion of men was 50.4% (range = 15%-100%), the average age at baseline was 57 (range = 37-73) years, and the baseline mean BMI was 30 (range = 22-40). The average baseline HbA1c% levels ranged from 5.70% to 11.05%, with an average of 8.33%.
Study and Participant Characteristics.

Abbreviations: BMI, body mass index; HbA1c, glycated hemoglobin; NA, not available.
Table 2 illustrates the telemedicine technologies implemented across studies. Seventy-one studies (29%) were conducted in a hospital setting, 58 studies (24%) in the primary care sector, 37 in communities (15%), 34 in specialized outpatient clinics (14%), 14 in a university setting (6%), and four in cross-sectorial implementations (2%). The frequency of contact with patients across studies was daily (30 studies, 12%), weekly (83 studies, 34%), every two weeks (26 studies, 11%), monthly (40 studies, 16%), and more rarely (12 studies, 5%). Twenty-four (10%) of the studies reported a “tailored” number of contacts with participants (10%). Across studies, the explicitly reported peripherals were scales (13 studies, 5%), glucometers (45 studies, 19%), blood pressure monitors (19 studies, 8%), and pedometers (16 studies, 7%).
Telemedicine Intervention Characteristics.
Abbreviation: BP, blood pressure.
The final sample included 86 studies (35%) with a monitoring component in the telemedicine intervention, 22 studies with a consultation opportunity (9%), 53 studies with a counseling purpose (22%), 63 studies with an opportunity for patients to receive coaching (26%), 81 studies with a patient education component (33%), and eight studies with the possibility of mentoring (3%). Furthermore, 38 studies were able to send reminders (16%).
The evaluation of risk of bias is described for each study in Online Appendix 1 and across studies in Figure 2. Overall, there was a high risk of bias in 45% of the included studies, a moderate risk in 38% and a low risk in 17%. This result was largely attributed to two factors. First were missing outcomes at follow-up, where a high proportion of studies (43%) only reported results of a complete case or per-protocol analysis without appropriate consideration of the relationship with covariates and missingness (ie, tests for missing completely at random or an assumption of missing at random with imputation and/or tests for association with baseline variables and missingness and/or adjusted analyses). Second, there were some concerns regarding the risk of selecting published results, especially due to a lack of registered or published research protocols in the majority of studies (72%).
Summary of risk of bias assessment.
Effect on HbA1c%
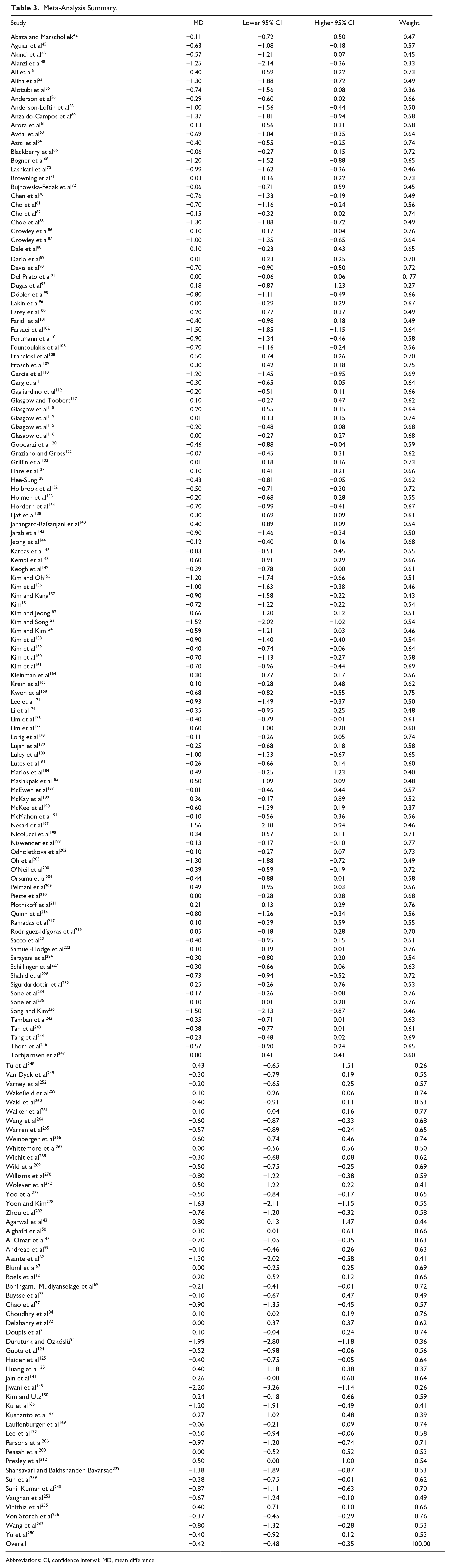
Of the 243 studies, 168 had sufficient information to calculate an MD with standard errors for the effect on HbA1c% and reported treatment effects of telemedicine from one to 96 months. Figure 3 and Table 3 present the results from the individual studies and the meta-analysis. Overall, the results favored telemedicine, with an MD of −0.415%, which was statistically significant (95% confidence interval [CI] = −0.482% to −0.348%). The heterogeneity was great (I2 = 93.05%).
Forest plot of the meta-analysis (magenta line is effect size difference of 0).
Meta-Analysis Summary.
Abbreviations: CI, confidence interval; MD, mean difference.
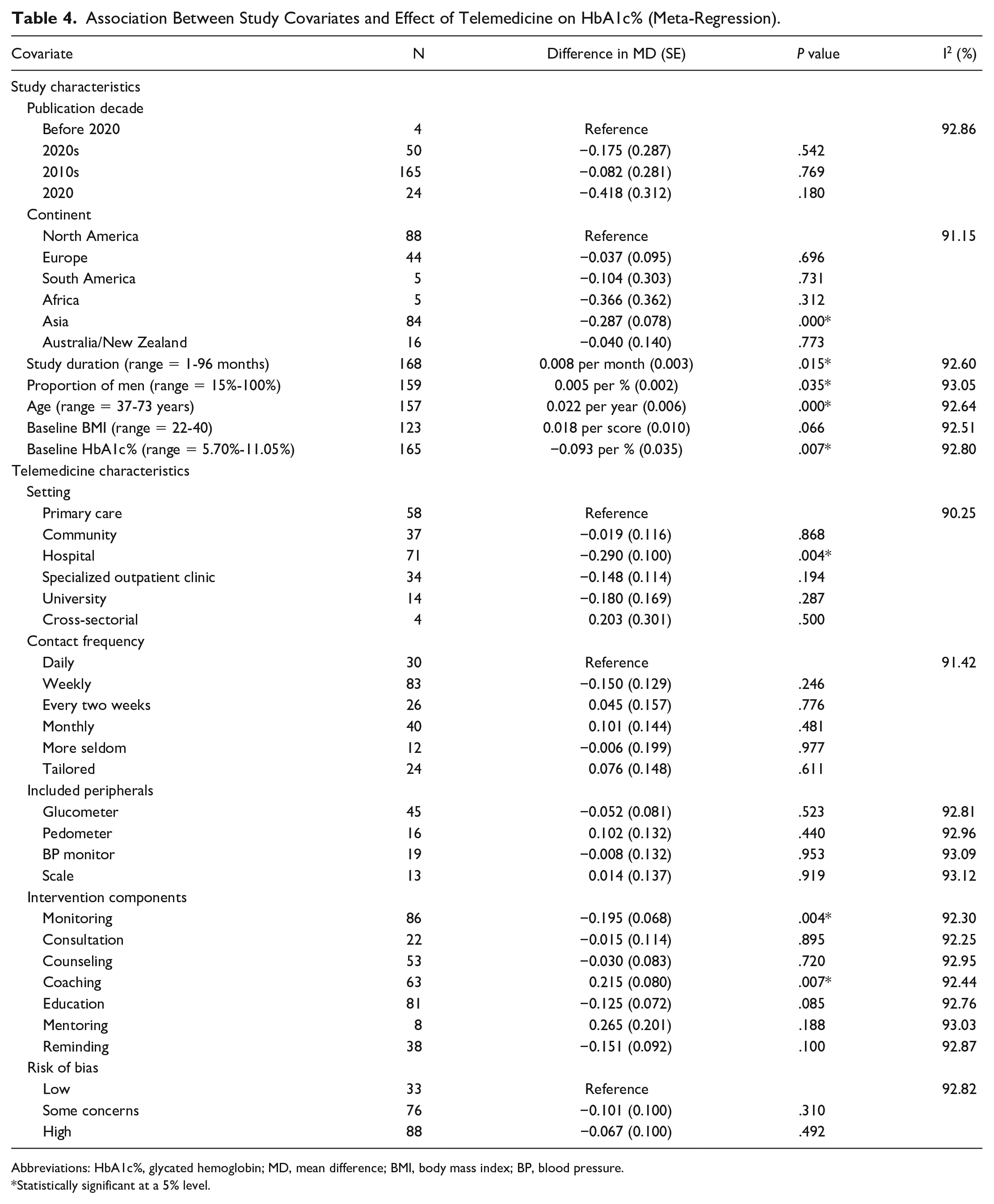
A series of univariate meta-regressions are illustrated in Table 4 and were assessed with a 5% significance level. Compared with North American studies (the reference), Asian studies reported larger effects of telemedicine (difference in MD = −0.287, P = .000), as did studies with higher baseline HbA1c% levels (difference in MD = −0.086 per %, P = .008). Compared with primary care settings (reference), hospital settings were also associated with an increase in the effect of telemedicine (difference in MD = −0.290, P = .004). Furthermore, a monitoring component gave rise to greater effects of telemedicine (difference in MD = −0.195, P = .004). Treatment effects of telemedicine were lesser for studies with longer duration (difference in MD = 0.008 per month, P = .015) and for studies with higher proportions of men (difference in MD = 0.005 per %, P = .035) and higher age (difference in MD = 0.022 per year, P = .000). A coaching component led to a lower effect (difference in MD = 0.215, P = .007). There were no statistically significant associations between the effect of telemedicine on HbA1c% levels and publication date, baseline BMI, contact frequency, the included peripherals, or risk of bias.
Association Between Study Covariates and Effect of Telemedicine on HbA1c% (Meta-Regression).
Abbreviations: HbA1c%, glycated hemoglobin; MD, mean difference; BMI, body mass index; BP, blood pressure.
Statistically significant at a 5% level.
Certainty of the Evidence
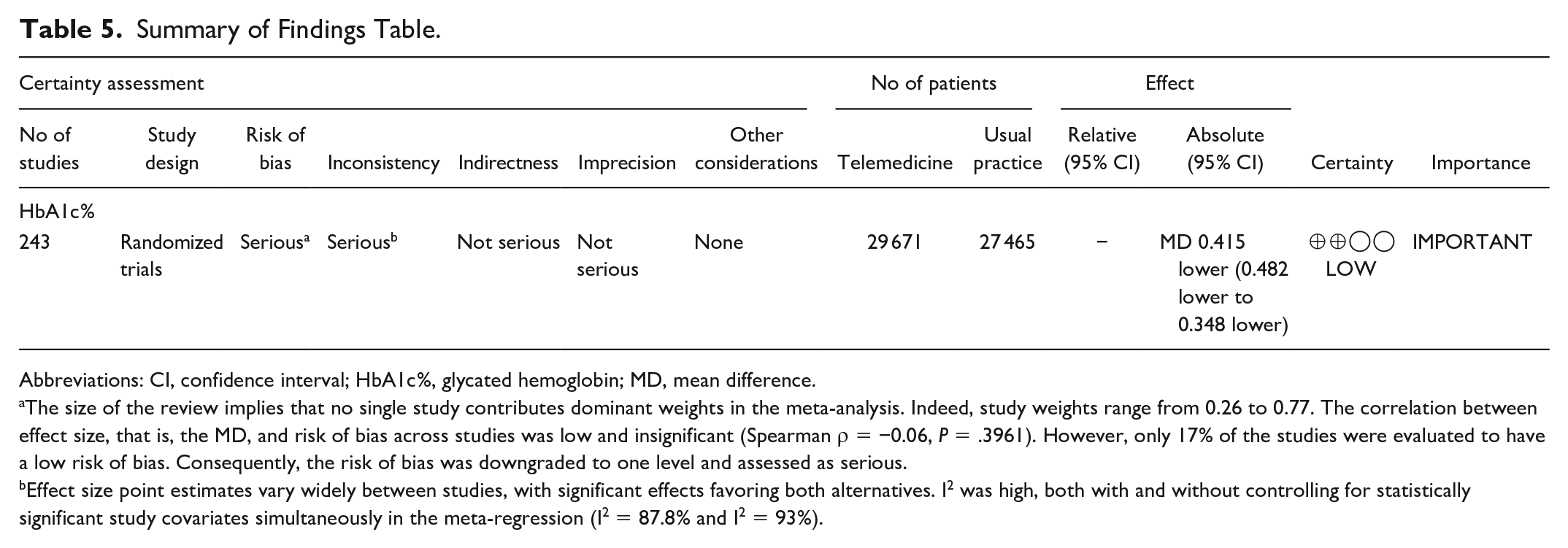
Table 5 summarizes the findings. Overall, the certainty of evidence of the calculated effect on HbA1c% was judged as low due to serious problems with the risk of bias and inconsistency.
Summary of Findings Table.
Abbreviations: CI, confidence interval; HbA1c%, glycated hemoglobin; MD, mean difference.
The size of the review implies that no single study contributes dominant weights in the meta-analysis. Indeed, study weights range from 0.26 to 0.77. The correlation between effect size, that is, the MD, and risk of bias across studies was low and insignificant (Spearman ρ = −0.06, P = .3961). However, only 17% of the studies were evaluated to have a low risk of bias. Consequently, the risk of bias was downgraded to one level and assessed as serious.
Effect size point estimates vary widely between studies, with significant effects favoring both alternatives. I2 was high, both with and without controlling for statistically significant study covariates simultaneously in the meta-regression (I2 = 87.8% and I2 = 93%).
Discussion
This review aimed to evaluate the effectiveness of telemedicine solutions among adult patients with T2D. Overall, the results favored telemedicine. Asian studies, studies with higher baseline HbA1c% levels, and studies in hospital settings reported larger effects of telemedicine. Moreover, inclusion of a monitoring component in the telemedicine solution gave rise to a higher effect of telemedicine, whereas inclusion of a coaching component led to a lower effect. The results reflect the findings from previous systematic reviews, which have found significant reductions in HbA1c favoring telemedicine.13,22,283,284 In line with our findings, Faruque et al and Wu et al found a larger effect among studies with a higher baseline HbA1c.13,283 In contrast to our findings, Faruque et al found a larger effect in studies that used web portals or text messaging. 13 In terms of telemonitoring, Hanlon et al found improved glycemic control in studies that included telemonitoring with feedback 17 and Jaana et al found significantly reduced HbA1 through telemonitoring. 22 Hence, the ideal telemedicine setup remains to be determined, although the inclusion of a telemonitoring component seems advisable.
The heterogeneity of the included studies was large (I2 = 93.05%), which is often seen in reviews of telemedicine.13,15,284-286 In the before-mentioned systematic review by Faruque et al, the heterogeneity (I2) ranged from 58% to 75% depending on the time point Hba1c was measured. 13 A systematic review and meta-analysis by Tchero found a heterogeneity (I2) of 99% in studies comparing telemedicine with usual care in T2D. 284 Hence, the large heterogeneity found in the present review is not unusually large when compared with similar reviews. The large heterogeneity found in the present review may be explained by differences in the inclusion criteria and context of studies that vary greatly in terms of patient subgroup, provider, technology, organization, communication frequency, outcome, and so on. Moreover, the inclusion of studies from the 1990s and 2000s may have added to the heterogeneity. Telemedicine interventions in diabetes have evolved significantly during the last decades due to technological advances and differences in the interventions are thus expected to have affected heterogeneity. However, the inclusion of studies from the 1990s and 2000s has maintained the broad and inclusive scope that was intended for the present review.
The certainty of the evidence was judged as poor. First, most of the evidence (45%) stems from studies with a high risk of bias and only 17% stems from studies with a low risk of bias. However, the size of the review implies that no single study contributed dominant weights in the meta-analysis, where study weights ranged from 0.26 to 0.77. The correlation between effect size, that is, the MD, and risk of bias across studies was low and nonsignificant (Spearman ρ = −0.06, P = .3961). Taken together, the certainty of evidence was downgraded one level due to risk of bias. Second, imprecision was assessed as not serious, as the effect size was statistically significant, and the MD and lower confidence limit (MD = −0.415, 95% CI = −0.482% to −0.348%) were both clinically relevant, and all were comparable with expected effects for other quality improvement strategies, 287 which is also why no upgrading due to large effects was conducted. The total number of patients (N = 57 136) included in the review was also much higher than the optimal information size threshold (the OIS criterion). Third, inconsistency was assessed as serious. Although confidence intervals overlap considerably, effect size point estimates vary widely between studies, with significant effects favoring both alternatives. I2 was high both with and without controlling for statistically significant study covariates simultaneously in the meta-regression (I2 = 87.8% and I2 = 93%). Fourth, indirectness was not serious in this review, as all included studies were head-to-head experimental trials assessing the same outcome, and the inclusion criteria for both the population and type of intervention were broad. Fifth, although publication bias cannot be rejected with high confidence, the risk of publication bias was evaluated as undetected. Less than 100 participants were included in 35% of the studies. The Egger test for small-study effects was statistically significant (P < .000) and the funnel plot in Figure 4 reveals studies reporting both significant and insignificant positive and negative effects. The funnel plot is somewhat asymmetrical, with more studies demonstrating significant effects favoring telemedicine than negative effects. Of the 243 included studies, 32 reported industry sponsorship and 44 studies did not report whether there were sponsorships or other relevant conflicts of interest. However, the relationship between disclosed industry sponsorship and/or undisclosed relationships with both study size (above/below 100 participants) and MD (above/below mean effect across studies) was statistically nonsignificant (Fisher exact test = 0.31 and 0.11, respectively). Finally, no dose-response gradient was detected, as the contact frequency was insignificant in the meta-regression (Table 4).
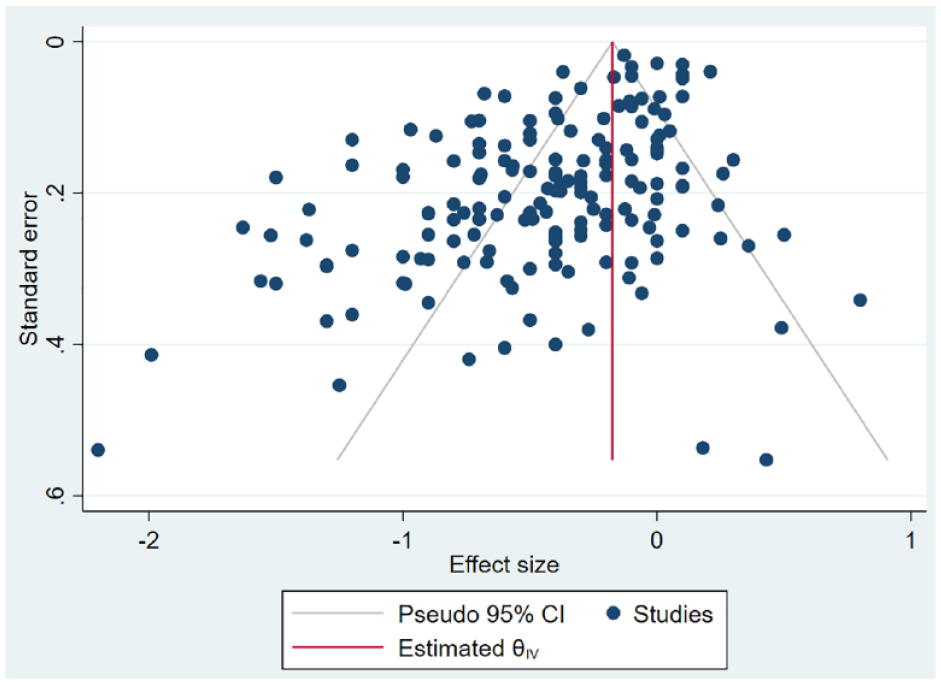
Funnel plot.
The present systematic review has some limitations. First, more baseline data, such as diabetes years, blood pressure, cholesterol levels, and medication, could have been extracted. However, due to differences in reporting style, such an extraction would have resulted in a high proportion of missing data in the analysis. Second, we could have contacted the authors of the individual studies to minimize the amount of missing HbA1c data. However, due to the large sample of included papers, such a search for data was deemed too time-consuming. Third, relevant studies may have been overlooked. Although a very broad search was conducted, the search was still limited to English and Scandinavian.
Conclusion
Telemedicine may serve as an effective supplement to usual care for patients with T2D. The inclusion of a telemonitoring component seems to increase the effect of telemedicine. It seems that those with a higher HbA1c are more likely to benefit from telemedicine. Patients with poor glycemic control may benefit more from telemedicine interventions, as a high HbA1c level leaves further room for improvement. However, the ideal glycemic target group for telemedicine in T2D remains to be determined.
Supplemental Material
sj-docx-1-dst-10.1177_19322968211064633 – Supplemental material for The Effectiveness of Telemedicine Solutions for the Management of Type 2 Diabetes: A Systematic Review, Meta-Analysis, and Meta-Regression
Supplemental material, sj-docx-1-dst-10.1177_19322968211064633 for The Effectiveness of Telemedicine Solutions for the Management of Type 2 Diabetes: A Systematic Review, Meta-Analysis, and Meta-Regression by Stine Hangaard, Sisse H. Laursen, Jonas D. Andersen, Thomas Kronborg, Peter Vestergaard, Ole Hejlesen and Flemming W. Udsen in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors would like to thank the research librarian Connie Skrubbeltrang, who assisted in the literature search.
Abbreviations
GRADE, The Grading of Recommendations, Assessment, Development and Evaluation; HbA1c, glycated hemoglobin A1c; MD, mean difference; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is an independent manuscript commissioned and jointly funded by the Steno Diabetes Center North Denmark and Aalborg University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.