
Abstract
Objective:
The objective of this study is to assess the safety and effectiveness of an electronic glucose monitoring system (eGMS) versus paper-based protocols (PBPs) to manage diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar syndrome (HHS) within the VA setting.
Methods:
This study is a retrospective chart review of patients on an insulin drip, treated in the emergency department (ED) or intensive care unit (ICU) at Veteran Health Indiana for DKA or HHS. The primary outcome was evaluating the percentage of patients with hypoglycemia (blood glucose [BG] level <70 mg/dL) in patients admitted with DKA and HHS comparing an eGMS versus a PBP. A total of 168 patients were included in the analysis, with 84 patients in each group.
Results:
The primary outcome comparing rates of hypoglycemia in the eGMS group versus the PBP group showed a lower rate of hypoglycemia in the eGMS group (0.024%) compared with the PBP group (0.060%); however, this difference was not found to be statistically significant (P = .90). Statistically significant secondary outcomes include the percentage of glucose checks drawn within the protocol recommendation (80.7% vs 52.6%, P = .02).
Conclusions:
While the primary endpoint of decreased hypoglycemia was not found to be statistically significant, it did reduce the overall number of hypoglycemia events in the eGMS group compared with the PBP group which may be clinically significant. This demonstrates that eGMS use has the potential to minimize hypoglycemia and glycemic variability in a critically-ill Veteran population by individualizing insulin drip titration based on a variety of patient-specific factors and providing reminders for staff to obtain BG checks in a timely manner.
Introduction
Managing diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar syndrome (HHS) safely and effectively in patients in the emergency department (ED) and intensive care unit (ICU) is a dynamic, complex task due to stress and a variety of patient-specific factors. Although various studies suggest electronic glucose monitoring system (eGMS) utilization provides superior DKA/HHS management, no validation has been performed within the VA setting. A diagnosis of diabetes mellitus can lead to potentially life-threatening complications for many patients. Hyperglycemic emergencies, such as DKA and HHS, as well as hypoglycemic emergencies, are among the most serious and life-threatening acute complications due to inadequate management of diabetes mellitus. 1 Diabetes mellitus is indicated on the medical record for 12.1% of emergency room (ER) visits, with 224 000 visits due to hyperglycemic crisis each year. Approximately 90.6% of these visits are due to DKA and the remaining 9.4% are due to HHS. 2 The inappropriate or mismanagement of DKA and HHS treatment can lead to increased duration of hyperglycemia or an increased rate of hypoglycemia. 1
Hospitalized patients with persistently uncontrolled blood glucose (BG) levels tend to experience increased ICU stays, increased rates of infection, more days on a ventilator, and increased mortality rates compared with patients with well-controlled BG levels. Studies have shown that hyperglycemia can add up to one day of additional hospital stay and hypoglycemia can increase the length of stay by two and a half days. 3 Historically, paper-based protocols (PBPs) were utilized to determine insulin drip rates and rate changes as needed for glucose emergencies. Paper-based protocols use weight-based dosing to determine the initial insulin drip rate. The insulin drip rate would be adjusted based on the most recent BG level and the difference between the current BG level and the last BG level. Paper-based protocols also dictated when to recheck BG based on current BG levels, which ranged from 30 to 90 minutes depending on the level and risk for hypoglycemia. With PBPs, nurses determined the timing of the next BG check and were in charge of setting their own alarm or reminder.
In recent years, many hospitals in the United States have gone away from PBPs in favor of eGMS for the treatment and management of DKA and HHS. Electronic glucose monitoring system automates the process of managing and adjusting insulin dosing by utilizing a personalized medicine approach. Electronic glucose monitoring system adjusts insulin doses by considering different patient factors including height, weight, age, sex, serum creatinine, steroid dosing, renal function, diabetes status (type 1 and type 2), response to insulin, and estimated residual extracellular insulin.3,4 Studies have shown that eGMS use has resulted in tighter, faster, and less variable BG control, in addition to fewer hypoglycemic episodes. 5 With the ability to utilize more patient-specific factors in an automated fashion, eGMS showcases a higher potential for safety and efficacy than current PBPs.4,5
While there are many brands and versions of eGMS available on the market, EndoTool® was the specific eGMS investigated in this study. It is currently used by more than 300 hospitals across the United States. 3 It is advertised to help patients reach target glucose ranges faster and reduce episodes of hypoglycemia and hyperglycemia. 4 It has demonstrated a 0.009% rate of hypoglycemia readings less than 40 mg/dL and a 0.36% rate of hypoglycemic readings less than 70 mg/dL. 3 It has also been shown to reduce hyperglycemic episodes by 45% to 57%. 4 It determines the initial insulin drip rate by utilizing various patient-specific factors, including height, weight, diabetes status, and more. Nurses input BG levels into the eGMS, which determines if the insulin drip rate needs to be adjusted. It determines the timing of the next BG check based on the previous BG readings. It is equipped with an alarm to alert nursing staff when the next BG check is due. Once the patient is stable, it will also alert the medical staff when to switch the patient to subcutaneous insulin. 3 These data suggest that patients will not only reach BG goals and be taken off continuous insulin faster, but also increase safety for the patient.3-5
Overall, the use of eGMS has demonstrated an increase in efficacy and safety in the treatment and management of DKA and HHS in various clinical trials and studies. There have been limited studies conducted concerning the use of eGMS in a Veteran population with a variety of disease states. Veterans have a much higher rate of diabetes at 25% than the general population at 10%, showing a possible higher prevalence and incidence of hyperglycemic emergencies, such as DKA and HHS. 6 Understanding the risks and benefits of an eGMS in a broad and diverse patient population can lead to high-quality and safer patient care for more patients with DKA and HHS. Data from this study will be used to better understand how Veteran Health Indiana can better manage Veterans with DKA and HHS, reduce adverse events related to insulin therapy, and improve overall hospital-related outcomes. The hypothesis is that the use of eGMS will reduce the overall rate of hypoglycemia compared with the use of a PBP.
Methods
The study site was Veteran Health Indiana in Indianapolis, Indiana. It serves as a level 1a, tertiary care facility and provides a large range of health care services for the US Veteran population. This medical center is a 159-bed facility that offers specialized inpatient and outpatient services such as mental health clinic, polytrauma center, medical ICU, surgical ICU, and an ED. In 2019, Richard L. Roudebush VAMC had approximately 13 000 ED visits and 4200 patients admitted to the inpatient wards.
This study was approved by the Indiana University/Richard L. Roudebush VA Medical Center System Institutional Review Board. This is a single-center, retrospective electronic chart review of patients who were on an insulin drip who presented to the ED or were admitted to the ICU for DKA or HHS between October 1, 2017, and October 1, 2020. There were a total of 168 patients included in the study in a 1:1 ratio for PBP and the eGMS. The PBP group (n = 84) data study dates ranged from October 1, 2017, through May 1, 2019, and the eGMS group (n = 84) had study dates that ranged from October 1, 2019, through October 1, 2020. All eligible patients from the PBP group treated during the pre-established time frame were included in data analysis. Data were collected from the eGMS population until 84 eligible patients had been treated in order for each treatment group to be equal. All of the patients were treated during their respective time frames for DKA or HHS at Veteran Health Indiana. The eGMS was implemented on May 1, 2019, and a five-month buffer was given to allow for training and increasing familiarity with the system to minimize data variability from any kind of learning curve. The inclusion criteria consisted of any patient admitted to the ICU or who presented to the ED with a diagnosis of DKA or HHS. The exclusion criteria consisted of any patient who switched between PBP and the eGMS during the same hospital stay as well as any patient with an admitting diagnosis of hyperglycemia or hypertriglyceridemia.
The objective of this study is to evaluate and compare the safety and efficacy of the PBP and the eGMS in the management of DKA and HHS in a VA setting. The primary outcome evaluated was the percentage of patients with hypoglycemia (BG <70 mg/dL) in patients admitted with DKA and HHS managed with a PBP compared with the eGMS. The secondary outcomes compared the duration of treatment on insulin in hours, length of hospital stay in days, rates of hyperglycemia (BG ≥200 mg/dL), percentage of time within the target range (BG 140-180 mg/dL), time to anion gap closure in hours (<15 mEq/L), and the percentage of BG checks within protocol.
Statistical Analysis
Descriptive statistics, including mean, standard deviations, ranges, and percentages, were utilized to display baseline characteristics of the study population. Student’s t tests were used to analyze primary and secondary endpoints of continuous variables between the two groups, and chi-square tests were used for categorical variables. A P-value of <.05 and a 95% confidence interval were considered significant. With a sample size of 84 patients from each group, the study has 80% power at a two-sided 5% significance level to detect a 15% difference in the percentage of patients with hypoglycemia (20% vs 5%), based on a chi-square test and a two-sample t test with standard deviation 20%, respectively. In order to reach statistical significance for 80% power at a two-sided 5% significance level, 75 patients are required in each treatment arm for a total of 150 patients.
Results
Baseline Characteristics
A total of 168 patients were included in the analysis, 84 in the PBP group and 84 in the eGMS group. Demographics are summarized in Table 1. The groups were evenly matched based on diagnosis (DKA vs HHS), age, race, body mass index (BMI), diabetes status (type 1 vs type 2), non-insulin diabetic medication use at admission, and insulin use at admission. Non-insulin diabetic medications included metformin, sulfonylureas, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, thiazolidinediones, and sodium-glucose cotransporter-2 (SGLT-2) inhibitors. Only one patient was taking an SGLT-2 inhibitor in the PBP group at admission and three patients in the eGMS group were taking an SGLT-2 inhibitor at admission. Mean HbA1c was 10.72% in the PBP group and 11.8% in the eGMS group (P = .022).
Baseline Characteristics.
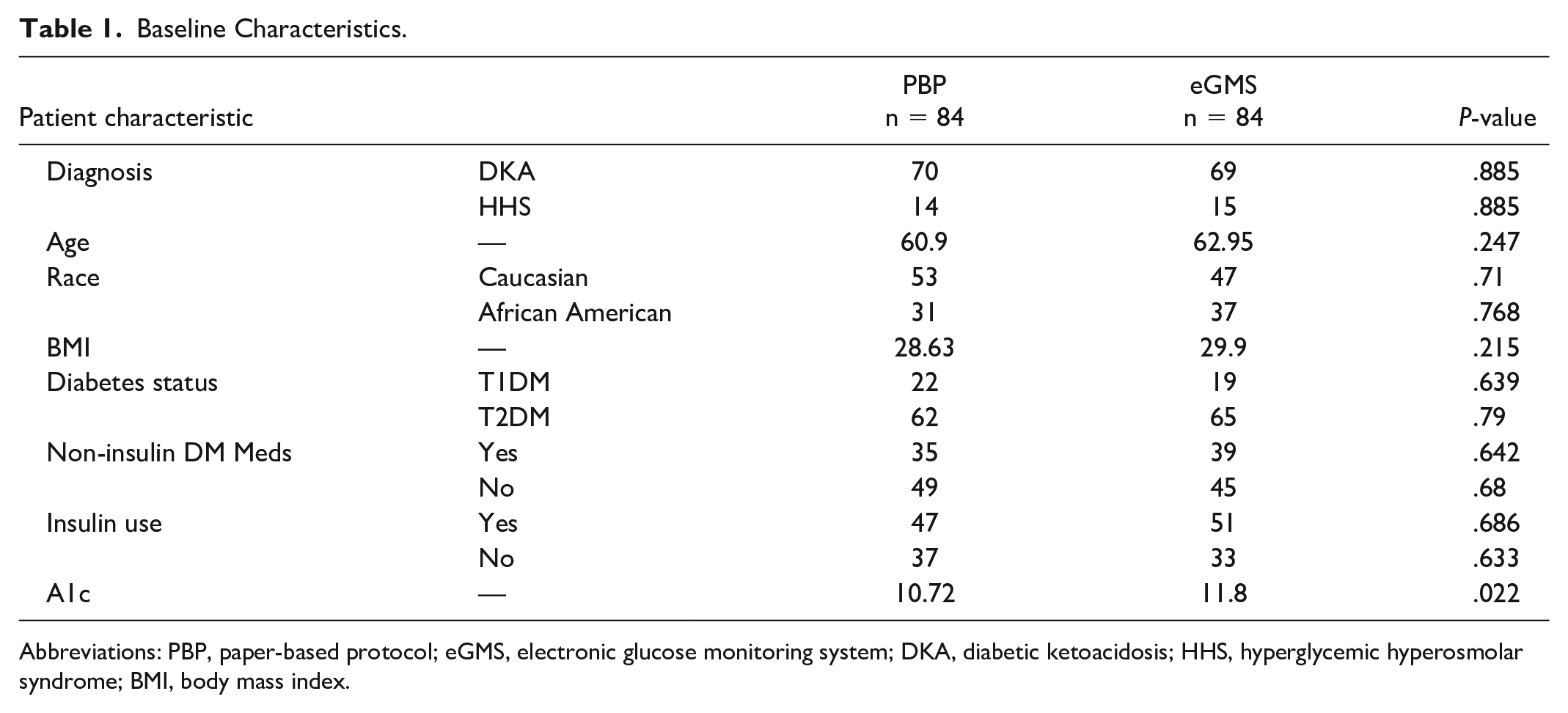
Abbreviations: PBP, paper-based protocol; eGMS, electronic glucose monitoring system; DKA, diabetic ketoacidosis; HHS, hyperglycemic hyperosmolar syndrome; BMI, body mass index.
Primary Outcome
The primary outcome comparing the percentage of patients with hypoglycemia in the eGMS group versus the PBP group was not found to be statistically significant with a rate of 0.024% in the eGMS group and a rate of 0.060% in the PBP group (P = .90; Table 2). The eGMS group had two total events of hypoglycemia compared with 10 total events in the PBP group. In the eGMS group, the two hypoglycemia events happened in different patients. In the PBP group, the ten hypoglycemia events happened in five unique patients. In the eGMS group, neither reading was classified as severe hypoglycemia, BG <54 mg/dL. The PBP group had three readings of severe hypoglycemia with BG readings <54 mg/dL.
Primary Outcome.

Abbreviations: PBP, paper-based protocol; eGMS, electronic glucose monitoring system; BG, blood glucose.
Secondary Outcomes
Results for the secondary outcomes are summarized in Table 3. The percentage of BG checks drawn within the protocol recommendation was also statistically significant, with 80.7% of the eGMS checks being drawn within an appropriate time frame and 52.6% of PBP readings being drawn within the protocol recommendation (P = .02). The remaining secondary endpoints were not found to be statistically significant. Patients on an insulin drip using the eGMS experienced a similar duration of treatment when compared with the PBP group (24.1 hours vs 23.9 hours, P = .96). The eGMS patients also experienced similar rates of hyperglycemia when compared with those in the PBP group (46.0% vs 55.7%, P = .34). The eGMS group showed a higher percentage of values within target range (BG 140-180 mg/dL) at 26.1% when compared with the PBP group at 16.3% (P = .13); however, this difference was not statistically significant. Both groups had similar lengths of hospital stay (4.6 days vs 4.6 days, P = .96) and time to anion gap closing (17.4 hours vs 16.0 hours, P = .64).
Secondary Outcomes.
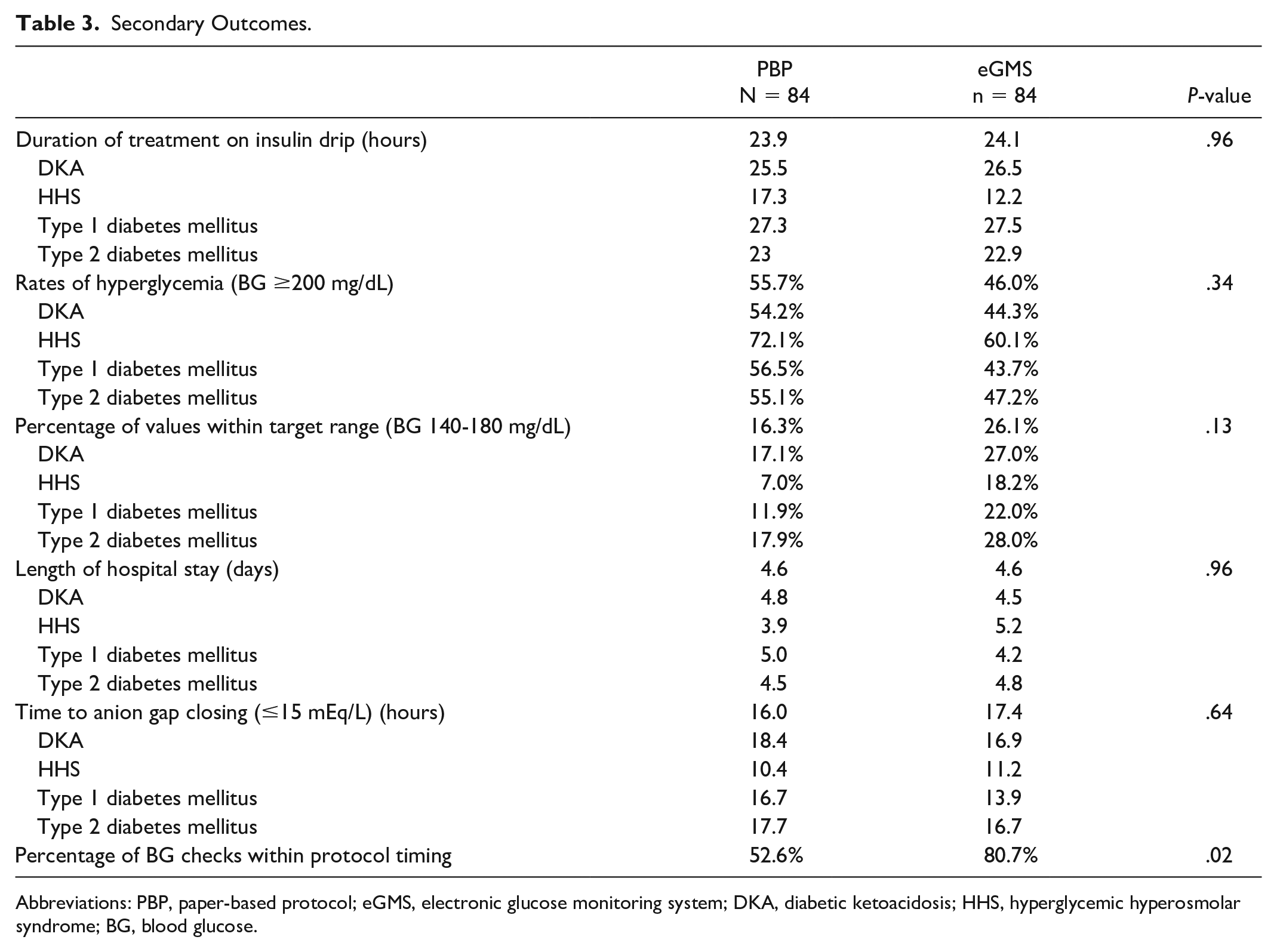
Abbreviations: PBP, paper-based protocol; eGMS, electronic glucose monitoring system; DKA, diabetic ketoacidosis; HHS, hyperglycemic hyperosmolar syndrome; BG, blood glucose.
Discussion and Conclusions
Discussion
The eGMS study population showed a lower rate of patients with hypoglycemia when compared with the PBP group; however, that rate was not statistically significant. Although the difference was not statistically significant, it can be considered to be clinically significant. Decreased rates of hypoglycemia can reduce pharmacy costs related to treating hypoglycemia and reduce nursing staff burden as well. The nonsignificance could be correlated to conservative eGMS settings as these data were collected during the initial use phase. There are current plans to change some of the treatment parameters, in particular in the ER. Similar results were seen in the study by John et al with trends toward decreased hypoglycemia and hyperglycemia in the eGMS group. 4 No study has been conducted comparing the use of an eGMS to PBP in a Veteran population. This study showed increased safety and effectiveness in the management of DKA and HHS in a critically-ill Veteran population.
An eGMS considers multiple patient-specific factors to determine insulin infusion rates, such as height, kidney function, diabetes status, estimated extracellular residual insulin, and response to insulin. This demonstrated a more personalized medicine approach as compared with the weight-based PBP dosing recommendations. These findings are consistent with other similar studies comparing PBPs to an eGMS to evaluate the rates of hypoglycemia and resolution of hyperglycemic events. Younis et al 7 demonstrated a statistically significant difference in time to resolution of DKA and hypoglycemic events. Rabinovich et al 5 demonstrated statistically significant decrease in the percentage of days with hypoglycemia and a higher percentage of time in range after eGMS implementation. Ullal et al 8 showed lower rates of hypoglycemia and faster rate of DKA resolution in the eGMS group compared with the PBP group. While done in a non-Veteran population, these studies showed trends toward decreased rates of hypoglycemia and increased glycemic control.
One point of discussion is the frequency of hypoglycemia readings for the primary outcome. Five patients from PBP group experienced a total of 10 hypoglycemia readings as opposed to two total readings from the two patients in the eGMS group. This demonstrates that some patients had multiple hypoglycemic readings in the PBP group. As patients experience hypoglycemia, the monitoring requirements for BG checks become more frequent in order to normalize BG levels at an appropriate rate. This increased monitoring can lead to multiple hypoglycemia readings in order to ensure that the patient’s BG level is rising. The PBP group also experienced two readings of severe hypoglycemia with BG readings <54 mg/dL. The eGMS group did not have any severe hypoglycemia readings. This can also be clinically significant as severe hypoglycemia tends to require more pharmacy and nursing resources in order to return to a normal BG level.
Rates of SGLT-2 inhibitor use were analyzed in both the PBP and the eGMS groups as euglycemic DKA is listed as a warning for SGLT-2 inhibitors. Only one patient was taking an SGLT-2 inhibitor in the PBP group at admission and three patients in the eGMS group were taking an SGLT-2 inhibitor at admission. Only patients with type 2 diabetes mellitus were using SGLT-2 inhibitors in this study.
Another point of discussion is the number of BG checks performed by the nursing staff in each group. In the PBP group, there were 1078 BG readings performed on the 84 patients and 1373 readings performed on the 84 patients in the eGMS group. This equates to an average of an additional 3.5 BG checks per patient in the eGMS group. As the eGMS group had more readings, it is important to consider the increased burden on nursing staff to perform these checks. It also can lead to higher rates of hypoglycemia readings, readings in range, and hyperglycemia readings. In this particular study, the eGMS showed a lower rate of hypoglycemia compared to PBP. It also showed an increased rate of readings in range, with 358 readings in range (26.1%) compared to 176 readings (16.3%) in the PBP protocol. It is difficult to determine if this is driven by the increased number of BG checks. Rates of hyperglycemia were different between the two groups, with the eGMS group having 632 readings (46.0%) >200 mg/dL and the PBP group with 600 readings (55.7%).
Limitations
There are several limitations with this study including the retrospective nature and heterogenicity of the patient population. This study relied on manual chart review, so data collection was reliant on correct documentation in the charts. The study population for this study was mostly white males from a single study site, so results might not be generalizable to all medical institutions.
Conclusions
In conclusion, the use of an eGMS for the management of DKA and HHS has potential to increase safety and effectiveness of glycemic control. In a critically-ill Veteran population, the eGMS demonstrated decreased rates of hypoglycemia when compared with a PBP. It also showed higher rates of readings in range and lower rates of hyperglycemia, although neither of these differences from the PBP were statistically significant. The alarm feature of the eGMS assisted with an increased compliance to BG checks per protocol, although it did result in a slightly higher occurrence of BG checks, thus increasing nursing workload. Overall, the use of the eGMS minimized hypoglycemia and glycemic variability by individualizing insulin drip titration based on a variety of patient-specific factors. The use of eGMS in the management of DKA and HHS will need further evaluations in order to confirm the findings of this study.
Footnotes
Abbreviations
BG, blood glucose; DKA, diabetic ketoacidosis; DPP-4, dipeptidyl peptidase-4; ED, emergency department; eGMS, electronic glucose monitoring system; GLP-1, glucagon-like peptide-1; HHS, hyperglycemic hyperosmolar syndrome; ICU, intensive care unit; PBPs, paper-based protocols; SGLT-2, sodium-glucose cotransporter-2.
Authors’ Note
This material is the result of work supported with resources and the use of facilities at Veteran Health Indiana. The contents do not represent the views of the US Department of Veterans Affairs or the United States Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of the US Government or any of its agencies.