
Abstract
Background:
Early worsening of diabetic retinopathy (EWDR) was observed in the intensively treated arm of the Diabetes Control and Complications Trial (DCCT) before long-term benefits accrued. We sought to assess whether there may be an increased risk of EWDR in high-risk individuals following intermittent-scanning continuous glucose monitoring (iscCGM) commencement.
Methods:
An observational study of 139 individuals with type 1 diabetes ≥5 years duration and with baseline HbA1c >75 mmol/mol (9.0%). This cohort was stratified by subsequent HbA1c response to iscCGM (best responders and non-responders). Pan-retinal photocoagulation (PRP), worsening retinopathy status and new development of retinopathy were compared between groups.
Results:
HbA1c change was -23 mmol/mol (IQR -32 to -19) (-2.1% [-2.9 to -1.8]) in responders and +6 mmol/mol (2-12) (+0.6 [0.2-1.1]) in non-responders (P < .001). There was no difference in subsequent PRP between responders (14.1%) and non-responders (10.3%, P = .340). Baseline HbA1c (HR 1.052 per mmol/mol, P = .002) but not response category (HR 1.244, P = .664) was independently associated with the risk of requiring PRP. Worsening of retinopathy was not different between responders (16.9%) and non-responders (20.6%, P = .577), and the same was true with respect to new development of retinopathy (33.3% vs 31.8%, P = .919).
Conclusions:
In a cohort enriched for risk of diabetic retinopathy, reduction in HbA1c did not result in an increased risk of PRP, worsening retinopathy, or new development of retinopathy. These findings offer reassurance that substantial reduction in HbA1c is not independently associated with early worsening of diabetic eye disease in iscCGM users.
Introduction
Intensive glycemic control substantially reduces the long-term risk of diabetic retinopathy in type 1 diabetes. 1 This was established conclusively by the landmark Diabetes Control and Complications Trial (DCCT) several decades ago. 2 However, DCCT participants assigned to intensive control were also noted to have a significant early worsening of diabetic retinopathy (EWDR) prior to longer term risk reduction. 3 Consequently, many clinicians exercise caution, aiming to avoid rapid reductions in HbA1c and consider more frequent monitoring in situations where this occurs (eg, commencement of new therapies). In recent years, intermittent-scanning continuous glucose monitoring (iscCGM) has been introduced at scale for people with type 1 diabetes across the United Kingdom (over 50% within our center). This technology provides users with an interstitial glucose value only upon scanning a reader device or compatible mobile phone. In many respects, it is similar to real-time continuous glucose monitoring (rtCGM) but without constant access to glucose data or alarm functions. 4 We have previously shown that iscCGM is associated with substantial reduction in Hemoglobin A1c (HbA1c) in people with above target HbA1c.5,6 We hypothesized that due to the potentially lower risks of hypoglycemia and reduced glucose variability associated with iscCGM, 7 the risk of EWDR may be attenuated or absent compared to historical approaches to glucose lowering. We have previously shown that in an unselected cohort of people with type 1 diabetes, comprising the first 589 iscCGM users in a single clinic, there was no independent association with extent of glucose lowering and EWDR (including the need for pan-retinal photocoagulation [PRP], macular laser or anti-vascular endothelial growth factor [VEGF] therapy). 8 However, it remains possible that those at high risk for microvascular complications may have a specific susceptibility to substantial reduction in HbA1c. To test this, we identified a cohort of individuals with high baseline HbA1c and long duration of diabetes and created two groups based on their initial HbA1c response to iscCGM: best responders, with a large decrease in HbA1c and non-responders, with no change or an increase in HbA1c. We sought to assess difference in rates of PRP, worsening of retinopathy, and new development of retinopathy between best responders and non-responders.
Participants and Methods
Study Design and Participants
We conducted an observational study of adults with type 1 diabetes who collected a National Health Service (NHS) prescription for Freestyle Libre sensors (Abbott, Witney, UK) between February 2018 (when NHS funding was approved in our center) and February 2019 within NHS Lothian. As described previously, 6 this cohort originally included 1800 individuals with paired (pre- and post-iscCGM) HbA1c data. The cohort for the current study was derived from the population of individuals with HbA1c >75 mmol/mol (9.0%) prior to iscCGM commencement (n = 342). The details of how the cohort was selected and the follow-up schedule are described in detail in Supplemental Figure 1. All individuals with duration of diabetes less than five years were excluded. Subsequently, we stratified individuals by HbA1c response following iscCGM commencement: HbA1c best responders—80 individuals with the greatest fall in HbA1c following iscCGM, and HbA1c non-responders—the first 80 individuals with either no change or a rise in HbA1c following iscCGM (Supplemental Figure 2). Nine individuals in the best responders group and 12 in the non-responders group were excluded due to incomplete baseline eye data, leaving a final cohort of 71 responders and 68 non-responders for analysis. This project did not involve deviation from usual clinical care or access to data beyond our usual clinical IT systems, and ethical approval was not required.
Outcomes
The primary outcome was an assessment of whether fall in HbA1c, following iscCGM commencement, was independently associated with the need for PRP (as determined by a consultant ophthalmologist). In addition, new onset of retinopathy (in those with no retinopathy at baseline), new onset of maculopathy, and worsening of retinopathy were assessed. Retinopathy was classified as none, mild background, intermediate (any eye disease more severe than mild non-proliferative retinopathy but not proliferative retinopathy), or proliferative. Worsening retinopathy was defined as at least one step up through these categories, with the most advanced category being recorded for individuals when a discrepancy existed between eyes. Retinopathy and maculopathy data were obtained from the national diabetic retinopathy screening program, 9 which is accessible via our national clinic database system, SCI-Diabetes (https://www.sci-diabetes.scot.nhs.uk). In individuals attending specialist eye clinics, data on severity of eye disease and treatments administered were obtained from our hospital’s electronic health records. All individuals had an eye assessment prior to commencement of iscCGM and an eye assessment no less than two months after iscCGM commencement, designated the “next eye assessment.” In addition, a further eye assessment was available in 60/139 (35.5%). Final eye outcomes were reported as a combination of the next eye assessment after iscCGM or, in those where it was available, their further eye assessment (Supplemental Figure 1). Baseline HbA1c was the last available result from 2017, and the difference in HbA1c, following iscCGM, was calculated using the next available HbA1c (either from 2018 or 2019 and at least two months since iscCGM commenced). We also report the last available HbA1c up to May 2020 when data collection ended. We sought to include as many potential predictors of HbA1c response as possible, including Scottish Index of Multiple Deprivation 2016 (SIMD) rank and quintile (https://www2.gov.scot/Topics/Statistics/SIMD). The structured education program offered in our center is Dose Adjustment for Normal Eating (DAFNE), and previous participation was discerned from SCI-Diabetes. Mode of insulin delivery (multiple daily injection [MDI] or continuous subcutaneous insulin infusion [CSII]), last available blood pressure measurement, urinary microalbumin status, smoking status, and body mass index were also obtained from SCI-Diabetes. iscCGM data were available in a minority of individuals (58/139, 34.3%) who had linked their data to our clinic via the LibreView portal (www.libreview.com). iscCGM data from LibreView were captured as a snapshot in May 2020.
Statistical Analysis
Data were largely non-normally distributed (as determined by Shapiro-Wilk test) and are presented as median and inter-quartile range. Unpaired data were analyzed by Mann-Whitney-U-test. Categorical data were analyzed by Chi-square or by Fisher’s exact test when assumptions for Chi-square were not met. Logistic regression analysis was performed to identify associations with development or worsening of eye disease. Univariate analysis of the need for PRP was assessed by Log-rank test. Independent predictors of the need for PRP were assessed by Cox proportional-hazard model. Significance was accepted at P < .05. All analyses were performed using R Studio version 1.0.153.
Results
Participant Characteristics
Clinical characteristics of the cohort are described in Table 1. Those belonging to the HbA1c best responder category were younger (37 years [31-50] vs 49 years [35-55], P = .027) but with similar diabetes duration and age at diagnosis (Table 1). Baseline HbA1c was higher in the HbA1c best responder group (88 mmol/mol [82-97] vs 82 [77-88], P < .001) and, by definition, HbA1c change following iscCGM was significantly different (−23 mmol/mol [-32 to -19] vs +6 [2-12], P < .001). The only other significant difference was a higher percentage of individuals having completed the DAFNE course in the HbA1c best responder group (38.0%) compared to non-responders (19.1%, P = .014). There were no significant differences between groups with respect to presence or severity of eye disease (Table 1). The prevalence of PRP at baseline was similar (Table 1), and the same was true of macular laser therapy (two in best responder group vs three in non-responder group) and anti-VEGF therapy (two vs one).
Clinical Characteristics Comparing HbA1c Best Responders and Non-Responders.
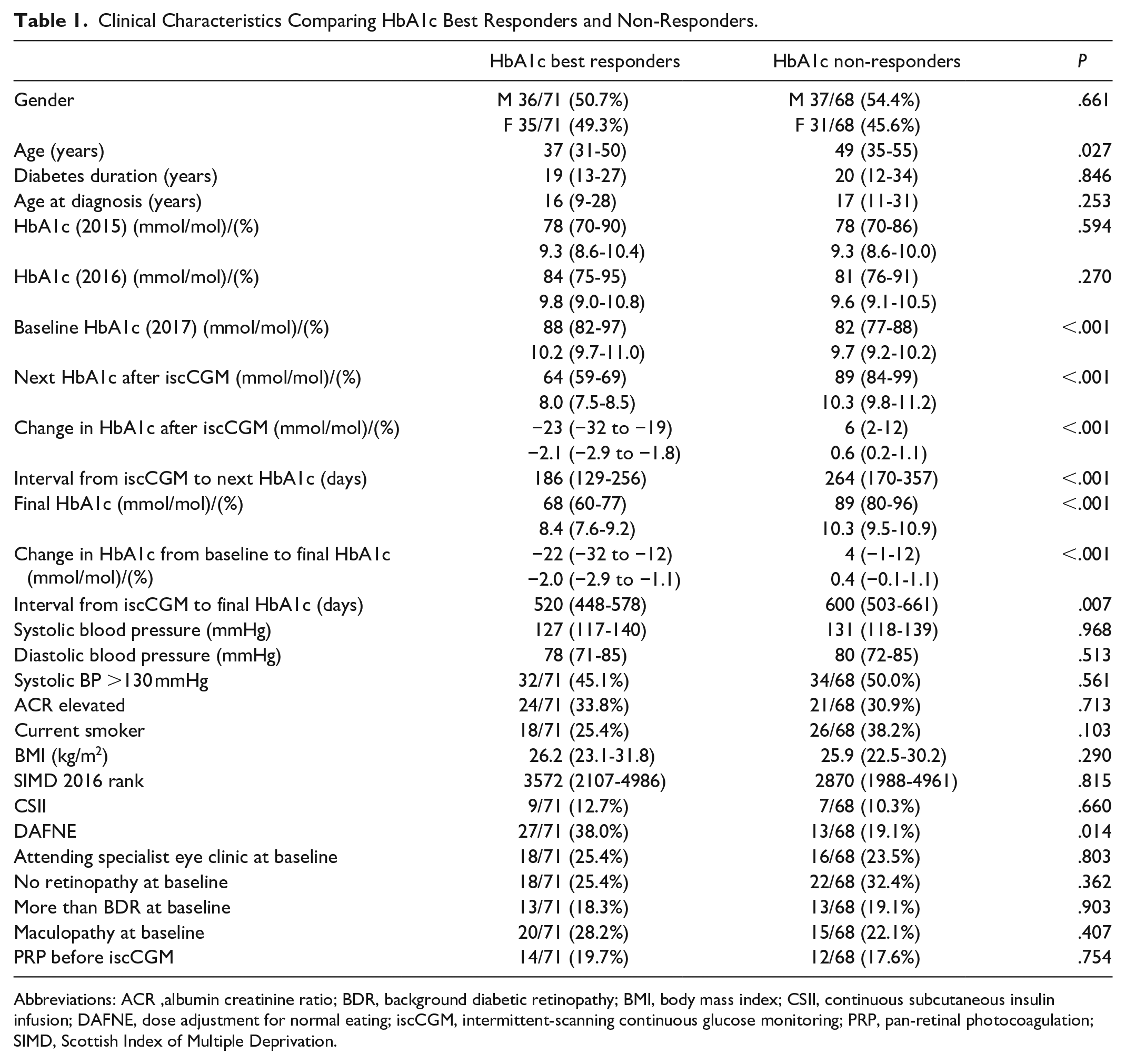
Abbreviations: ACR, albumin creatinine ratio; BDR, background diabetic retinopathy; BMI, body mass index; CSII, continuous subcutaneous insulin infusion; DAFNE, dose adjustment for normal eating; iscCGM, intermittent-scanning continuous glucose monitoring; PRP, pan-retinal photocoagulation; SIMD, Scottish Index of Multiple Deprivation.
Snapshot iscCGM data from May 2020 showed significantly lower average glucose (10.2 mM [9.1-11.7] vs 13.5 [11.9-14.8], P < .001), greater percentage time in range (48% [33-57] vs 29 [23-36], P < .001), lower standard deviation (4.0 mM [3.6-5.0] vs 5.5 [4.3-6.1], P = .001) and more sensor scans per day (9 [6-12] vs 6 [4-9]) in the HbA1c best responder group (Supplemental Table 1).
PRP
Prior to iscCGM commencement, 26/139 (18.7%) had received PRP, with no significant difference between subsequent best responders (14/71 [19.7%]) and non-responders (12/68 [17.6%], P = .754). Following commencement of iscCGM, over a median 425 days (255-559) follow-up, 10/71 (14.1%) best responders and 7/68 (10.3%) non-responders received PRP. There was no significant difference in subsequent PRP between best responders and non-responders as presented in Figure 1 (P = .340). Baseline HbA1c (HR 1.052 per mmol/mol [95% CI 1.019-1.086], P = .002), but not HbA1c response category (HR 1.244 [95% CI 0.465-3.325], P = .664), was independently associated with risk of PRP following iscCGM (Figure 2). Seven individuals had a first episode of PRP following iscCGM commencement (5/71 in the best responder group and 2/68 in the non-responder group, P = .442). Three of the first ever PRP episodes were in women during pregnancy, all of whom were in the best responder cohort. Only two individuals received a first course of anti-VEGF therapy after iscCGM commencement, and only one individual received a first episode of macular laser therapy.
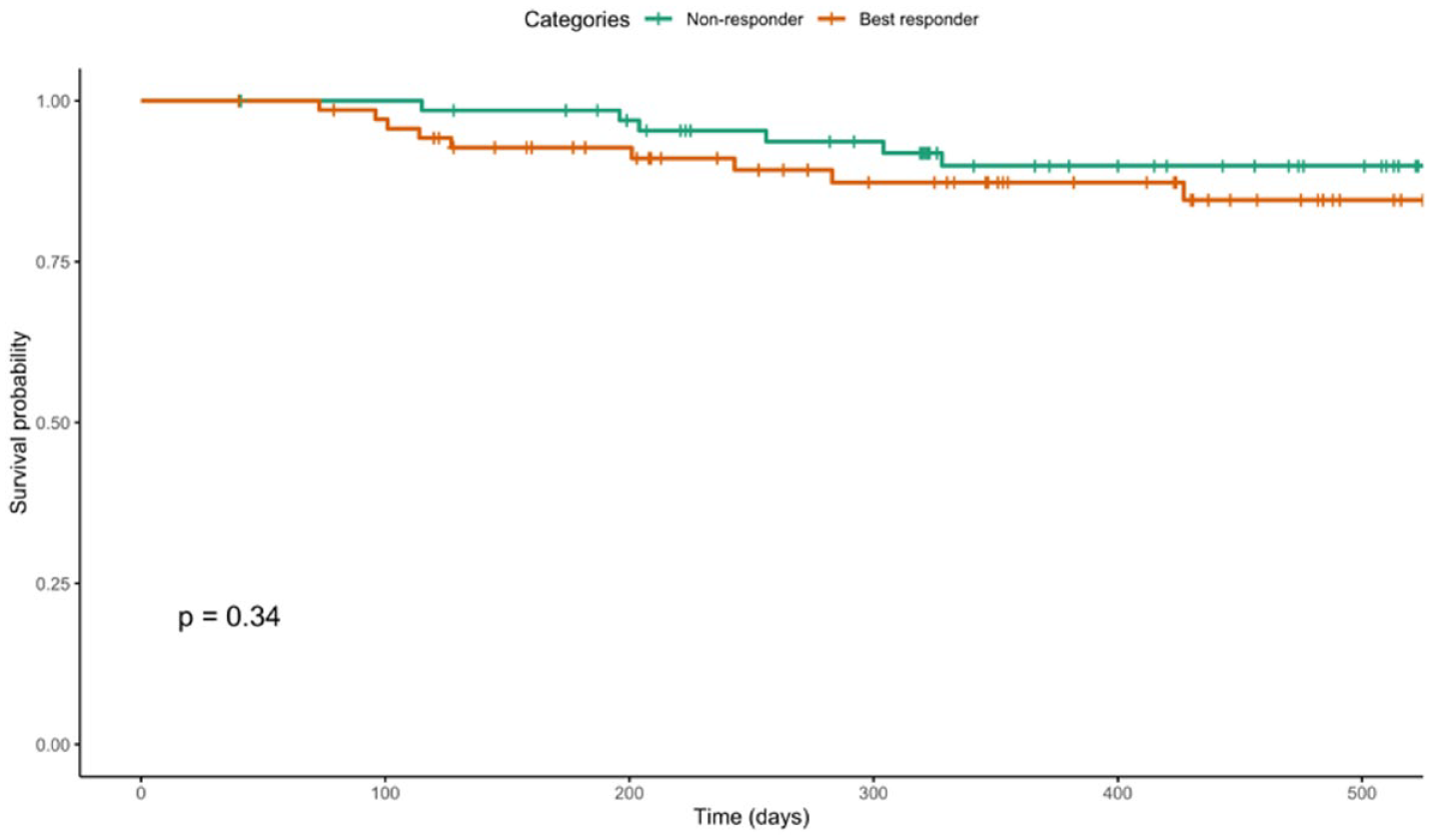
Survival curve for PRP following iscCGM comparing HbA1c best responders (orange line) and non-responders (green line). Log rank test P = .340. Abbreviations: iscCGM, intermittent-scanning continuous glucose monitoring; PRP, pan-retinal photocoagulation.
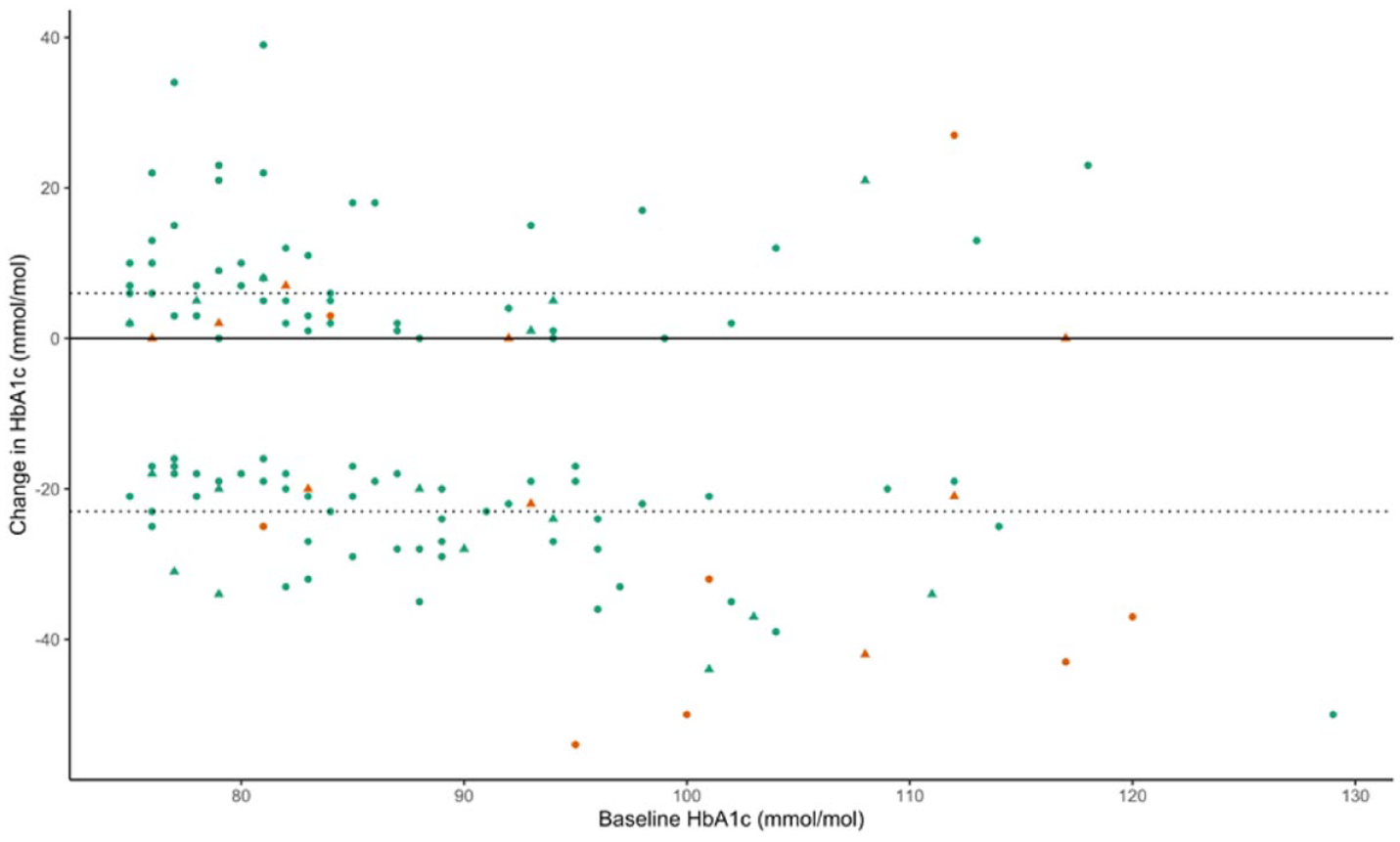
Relationship between baseline HbA1c and change in HbA1c, categorized by subsequent need for PRP. Orange represents individuals who received PRP after iscCGM commencement, and green represents those who did not. Triangles represent individuals with any PRP prior to iscCGM, and circles represent those with no prior history of PRP. The two individuals with the largest fall in HbA1c, who received PRP after iscCGM, were pregnant at the time of treatment. Abbreviations: iscCGM, intermittent-scanning continuous glucose monitoring; PRP, pan-retinal photocoagulation.
Changes in Diabetic Eye Disease
Retinopathy categories at baseline, next assessment, and final assessment are summarized in Table 2. At the next eye assessment following iscCGM commencement, there was no significant difference between best responders and non-responders with respect to progression of retinopathy stage (16.9% vs 20.6%, P = .577) or development of new retinopathy in those with none at baseline (33.3% vs 31.8%, P = .919). The same was true when analyzing the final eye assessment data (P = .442 and P = .622, respectively) (Table 2). At next assessment following iscCGM, there was no difference in those with a new diagnosis of maculopathy (7/71 in best responders [9.9%] vs 4/68 [5.9%] in non-responders, P = .385). Univariate analysis identified only shorter diabetes duration (15 years [10-23] vs 21 [13-32], P = 0.037) and higher HbA1c in 2015 (83 [75-88] vs 76 [69-87], P = 0.036) as being associated with worsening retinopathy (Supplemental Table 2). Logistic regression identified baseline HbA1c (OR 1.054 per mmol/mol [95% CI 1.017-1.094], P = .005) but not HbA1c response category (OR 0.53 [95% CI 0.20-1.33], P = .183) or diabetes duration (OR 0.963 per year [95% CI 0.917-1.003], P = .096) as independently predictive of retinopathy progression at next eye assessment after iscCGM. There was no difference in the number of individuals newly referred to specialist ophthalmology clinics following iscCGM commencement based on response category (6/71 [8.5%] best responders vs 7/68 [10.3%] non-responders, P = .709).
Retinopathy Categories at Baseline, Next Assessment Following iscCGM, and Final Assessment.
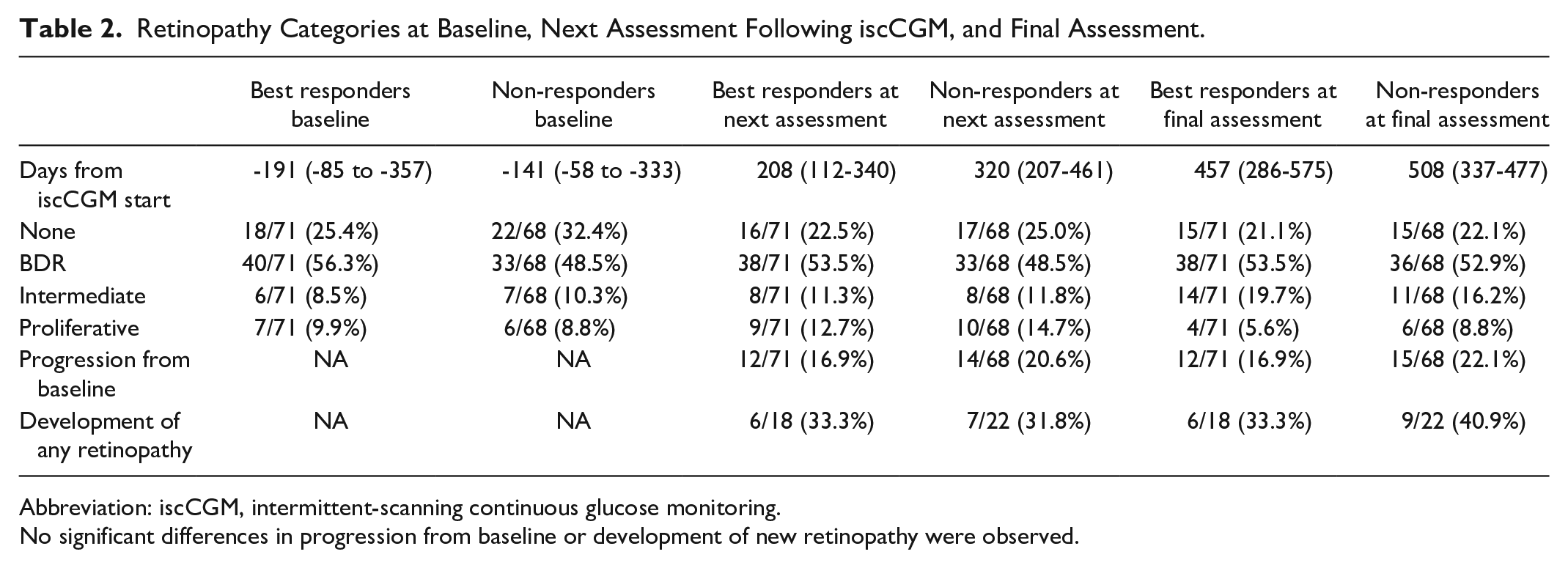
Abbreviation: iscCGM, intermittent-scanning continuous glucose monitoring.
No significant differences in progression from baseline or development of new retinopathy were observed.
Snapshot iscCGM data from May 2020 showed only fewer daily iscCGM sensor scans and lower percentage data capture as being significantly associated with worsening retinopathy stage following iscCGM commencement. Specific glucose metrics were not significantly different although there was a trend to greater glucose variability as indicated by higher coefficient of variation (CV) and standard deviation (Table 3). Logistic regression identified standard deviation (OR 2.4 per mM [95% CI 1.2-5.5], P = .027) but not average glucose (OR 0.8 per mM [95% CI 0.6-1.2], P = .320) as independently associated with worsening final retinopathy status.
iscCGM Parameters (Recorded in May 2020) Comparing Those With Worsening Retinopathy and Those Without Worsening Retinopathy Following Commencement of iscCGM.
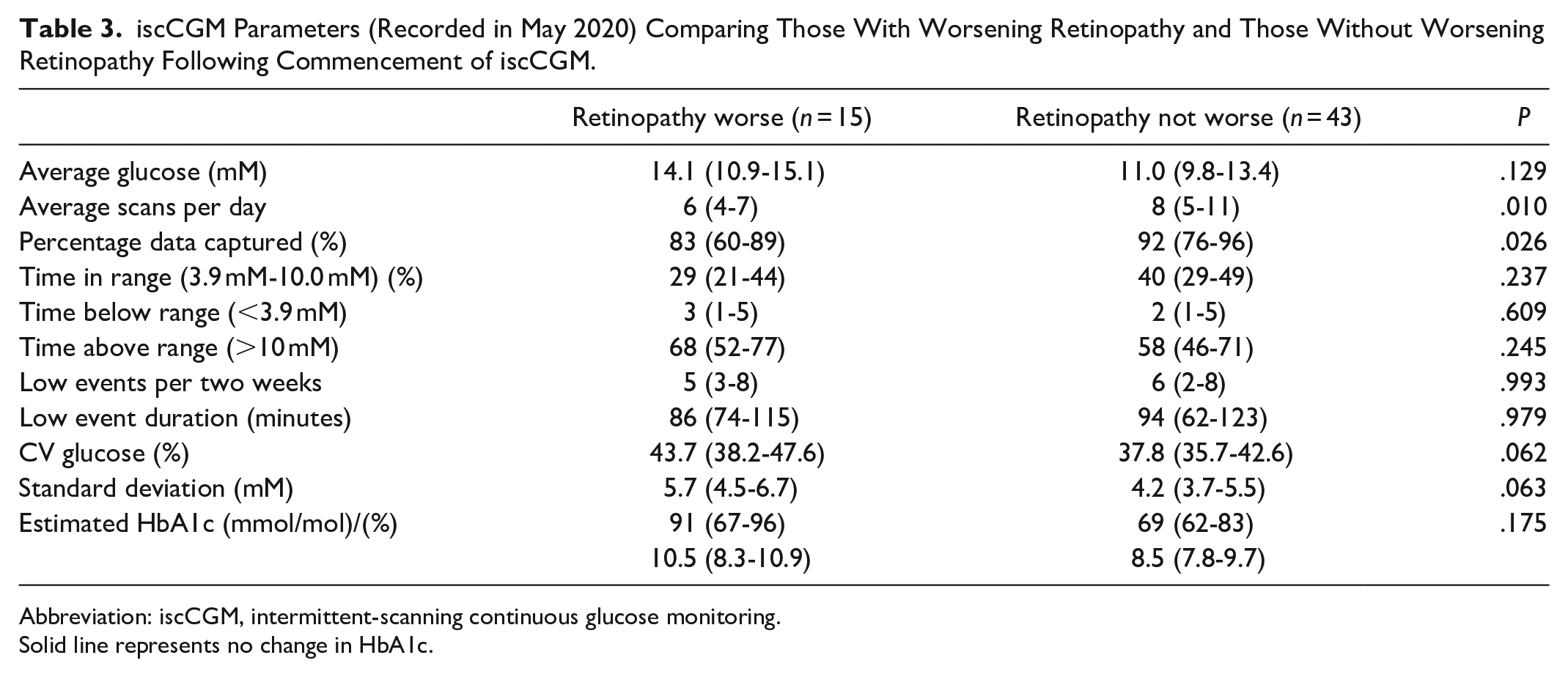
Abbreviation: iscCGM, intermittent-scanning continuous glucose monitoring.
Solid line represents no change in HbA1c.
Discussion
We have demonstrated that large improvements in HbA1c, in people with persistently high HbA1c and long duration of diabetes, are not significantly associated with clinically important early worsening of diabetic retinopathy. Baseline HbA1c, but not diabetes duration or change in HbA1c, was associated with the need for PRP. Similar associations were noted with respect to worsening of retinopathy. This assessment of individuals at high risk of microvascular complications (high HbA1c and long diabetes duration) accords with our earlier findings in an unselected group of individuals who commenced iscCGM within a single clinic in our center. 8
It has been conclusively proven that intensification of glycemic control results in long-term reduction in the development and progression of diabetic retinopathy.2,10,11 However, in the DCCT, those randomized to intensive control experienced a transient early worsening of retinopathy prior to subsequent risk reduction (13.1% vs 7.6% in the conventional arm). 3 It remains unclear what pathophysiological mechanisms underpin EWDR, although changes in the somatotropic axis and increased retinal concentration of angiogenic factors have been advanced as potential explanations. 12 We hypothesized that intensification in the modern era may not be associated with the same risk of early worsening due to potential benefits offered by iscCGM, as well as the multifaceted approach to complication prevention, which developed following DCCT. Historically, intensification of therapy was associated with a substantial increase in severe hypoglycemia (threefold in DCCT). We have previously reported no increased frequency of severe hypoglycemia following the introduction of iscCGM. 5 The largest RCT of iscCGM demonstrated reduced glucose variability and hypoglycemia, 7 and a recent large observational study suggested lower rates of severe hypoglycemia in iscCGM users. 13 rtCGM has been associated with an attenuation of hypoglycemia risk as HbA1c levels fall, compared to individuals using self-monitoring of blood glucose, 14 although these data cannot necessarily be extrapolated to iscCGM. Islet15,16 and pancreas 17 transplantation are both associated with less glucose variability and hypoglycemia and have not been associated with EWDR in the context of HbA1c reduction. Similarly, no significant worsening of retinopathy has been observed in the context of commencing CSII. 18 Although the numbers were limited, our iscCGM data trend toward a more significant influence of glucose variability (standard deviation) than average glucose in relation to worsening retinopathy.
In addition to differences related to modern diabetes management, our cohort differs substantially from that of the DCCT in terms of older age (42 vs 27 years), longer duration of diabetes (20 vs six years), higher prevalence of prior PRP (18.7% vs none in DCCT) and higher baseline HbA1c (84 mmol/mol vs 76 mmol/mol [9.8% vs 9.1%]). This was our intention, as we selected a cohort perceived to be at greatest possible risk for development or deterioration of retinopathy. To that end, this cohort is likely to be generalizable to populations of individuals with long-standing high HbA1c, although we have previously reported that even with NHS funding, those with greatest socioeconomic deprivation are less likely to be iscCGM users.5,6
The study is susceptible to the typical criticisms of observational methodology particularly in relation to the potential influence of unmeasured confounders. As a “real-world” assessment, the timing of HbA1c measurement and eye examinations was not standardized but simply reflected usual clinical practice. This has the potential to introduce biases, and there are differences in some follow-up intervals between best responders and non-responders. However, there is no significant difference in the interval from baseline eye assessment to iscCGM commencement and, critically, between iscCGM commencement and final eye assessment. In addition, univariate and multivariate analysis of the primary endpoint accounted for differences in follow-up duration. A key strength of a “real-world” approach is the inclusion of individuals with type 1 diabetes who would often be excluded from RCTs or, if eligible, less likely to participate. In that respect, this cohort is likely to be similar (and therefore generalizable) to populations of iscCGM users with high baseline HbA1c across the United Kingdom and beyond. The decision to create two groups at the extreme ends of the HbA1c response spectrum was taken to address the specific issue of whether magnitude of change in HbA1c was independently associated with eye disease progression. Critically, there was no difference in diabetes duration (although non-responders were older) and baseline HbA1c was higher (6 mmol/mol [0.6%]) which, if anything, would increase the likelihood of events in the best responder group. That absence of difference in adverse outcomes is even more striking when considering the higher baseline HbA1c, which was both statistically significant and clinically relevant. As a real-world assessment, we did not have access to Gold Standard evaluation of retinopathy grade, typically considered to be the Early Treatment Diabetic Retinopathy Study (ETDRS) classification system. 19 This is a significant limitation, as the results from our national screening program and electronic health record entries from specialist clinics do not provide the same level of detail as ETDRS. However, in mitigation, using real clinical data means that it is very unlikely that we have missed clinically important changes in retinopathy. As well as changes in retinopathy status, we report PRP which is an unambiguous, hard clinical endpoint. The interval between iscCGM commencement and next eye assessment may have limited the opportunity to observe extremely early retinal changes in this study. Furthermore, we cannot address the issue of whether rapidity of glucose lowering is a specific risk factor for eye disease progression, although self-management changes are likely to occur early following iscCGM commencement. 7 The number of PRP events in this study were relatively small, and it remains possible that we have missed significant differences between best responders and non-responders, which would be evident in a larger cohort. However, associations with PRP were not close to statistical significance and, at final assessment, development and progression of retinopathy were non-significantly lower in best responders. Three of seven individuals requiring a first ever episode of PRP were pregnant (a recognized independent risk factor for retinopathy progression).
Conclusions
These findings offer some reassurance that, even in a group at significant risk of microvascular complications, there does not appear to be a significant effect of marked HbA1c reduction upon worsening retinopathy. This stands in contrast to the findings of the DCCT and will require verification in larger multicenter datasets and RCTs of novel glucose lowering therapies. However, as we enter the era of closed-loop insulin delivery, our findings suggest grounds for optimism regarding the potential risks associated with rapid reduction in HbA1c.
Supplemental Material
sj-docx-1-dst-10.1177_1932296821994091 – Supplemental material for Substantial HbA1c Reduction Following Intermittent-Scanning Continuous Glucose Monitoring Was Not Associated With Early Worsening of Retinopathy in Type 1 Diabetes
Supplemental material, sj-docx-1-dst-10.1177_1932296821994091 for Substantial HbA1c Reduction Following Intermittent-Scanning Continuous Glucose Monitoring Was Not Associated With Early Worsening of Retinopathy in Type 1 Diabetes by Kathryn Linton, Roland H. Stimson, Anna R. Dover, Shareen Forbes, Karen Madill, Roxanne Annoh, Mark W. J. Strachan, J. A. McKnight, Rohana J. Wright and Fraser W. Gibb in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
BDR, background diabetic retinopathy; BMI, body mass index; CSII, continuous subcutaneous insulin infusion; CV, coefficient of variation; DAFNE, dose adjustment for normal eating; DCCT, Diabetes Control and Complications Trial; ETDRS, Early Treatment Diabetic Retinopathy Study; EWDR, early worsening of diabetic retinopathy; HbA1c, Hemoglobin A1c; IQR, inter-quartile range; iscCGM, intermittent-scanning continuous glucose monitoring; MDI, multiple daily injections; NHS, National Health Service; PRP, pan-retinal photocoagulation; rtCGM, real-time continuous glucose monitoring; SIMD, Scottish Index of Multiple Deprivation; VEGF, vascular endothelial growth factor.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FWG has received speaker fees from Abbott Diabetes Care. ARD has received speaker fees from Abbott Diabetes Care.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.