
Abstract
Background:
People with impaired awareness of hypoglycemia (IAH) are at elevated risk of severe, potentially hazardous, hypoglycemia and would benefit from a device alerting to hypoglycemia. Heart rate variability (HRV) changes with hypoglycemia due to sympathetic activity. Since IAH is associated with suppressed sympathetic activity, we investigated whether hypoglycemia elicits a measurable change in HRV in patients with T1D and IAH.
Method:
Eligible participants underwent a modified hyperinsulinemic euglycemic hypoglycemic clamp (glucose nadir, 43.1 ± 0.90 mg/dl), while HRV was measured by a VitalConnect HealthPatch. Measurements of HRV included Root Mean Square of the Successive Differences (RMSSD) and low to high frequency (LF:HF) ratio. Wilcoxon rank-sum test was used for testing within-subject HRV changes.
Results:
We included 12 participants (8 female, mean age 57 ± 12 years, mean HbA1c 57 ± 5 mmol/mol (7.4 ± 0.4%)). Symptoms increased from 4.0 (1.5-7.0) at euglycemia to 7.5 (5.0-11.0) during hypoglycemia (P = .003). In response to hypoglycemia, the LF:HF ratio and RMSSD increased when normalized for data obtained during euglycemia (both P < .01). The LF:HF ratio increased in 6 participants (50%) and declined in one other participant (8%). The RMSSD decreased in 3 (25%) and increased in 4 (33%) participants. In 2 patients, no change in HRV could be detected in response to hypoglycemia.
Conclusions:
This study reveals that hypoglycemia-induced changes in HRV are retained in the majority of people with T1D and IAH, and that these changes can be detected by a wearable device. Real-time HRV seems usable for detection of hypoglycemia in patients with IAH.
Keywords
Introduction
Hypoglycemic events are the principal barrier for strict glucose management and occur on average twice weekly in patients with type 1 diabetes.1,2 When recurrent, hypoglycemia may induce a process of habituation leading to suppression of counterregulatory responses to and symptomatic awareness of subsequent hypoglycemia, ultimately leading to impaired awareness of hypoglycemia (IAH). Using validated questionnaires, about 25% of people with type 1 diabetes 3 and 10% of those with type 2 diabetes can be classified as having impaired awareness of hypoglycemia. 4 Patients with IAH have lost the capacity to detect the onset of impending hypoglycemia, creating a 6- to 17-fold higher risk for severe hypoglycemia, 3 defined as an event with cognitive decline of such a magnitude that it requires third-party assistance for recovery. 5
Severe hypoglycemia is associated with decreased quality of life and increased cardiovascular morbidity and mortality. 6 Devices that alert for hypoglycemia early would allow for timely correction of low glucose values before potentially life threatening hazardous severe hypoglycemia ensues. Use of continuous glucose monitoring has been shown to reduce the frequency of severe hypoglycemia in people with type 1 diabetes and IAH. 7 However, although strict avoidance of hypoglycemia is of critical importance to reverse the process of impaired awareness, 8 glucose sensors have not been shown to restore awareness of hypoglycemia in these people. 9 Also, accuracy of continuous glucose monitoring in the lower glucose range remains a matter of concern and the devices are costly, limiting their access for the larger population. Finally, overwhelming amount of data, disruptiveness of alarms, and physical discomfort have all been reported as limitations associated with glucose sensor therapy. 10
Continuous measurement of heart rate variability (HRV) is potentially useable for early detection of hypoglycemia because hypoglycemia causes sympathetic nervous system hyperactivity. HRV is a measure of beat-to-beat variability in consecutive R-R intervals on an electrocardiogram, reflecting the balance between the sympathetic and parasympathetic nervous system. 11 Hypoglycemia-induced activation of the sympathetic nervous system has been shown to cause specific changes in HRV.12,13 HRV was traditionally measured by Holter or 12-lead ECG devices, but due to improved technology real-time wearable devices have become available that are suitable for daily use. These devices monitor heart rate with high accuracy and a sufficient sample rate. 14 In a previous study, we demonstrated that developing hypoglycemia causes changes in HRV that can be detected by a wearable device in ambulant patients with type 1 diabetes. 15
Whether hypoglycemia causes detectable changes in HRV in people with IAH has not been investigated. The counterregulatory response to hypoglycemia is in large part mediated through the sympathetic nervous system. The absence of symptoms in people with IAH reflects suppression of sympathetic nervous system activation, 16 but the presence of an, albeit blunted, adrenaline response in most persons affected by IAH indicates that this suppression is not complete. The aim of the study was therefore to examine whether hypoglycemia can elicit measurable HRV changes, using a wearable device, in people with type 1 diabetes and IAH.
Methods
Setting and Study Population
Data were obtained from 12 individuals with type 1 diabetes and IAH, who had participated in either of two studies, conducted to investigate the effect of a glucagon-like peptide-1 (GLP-1) receptor agonist 17 or a sodium glucose cotransport-2 (SGLT-2) inhibitor on IAH (NCT03556033). Participants had been recruited from the Radboud University Medical Center outpatient diabetes clinic. They were potentially eligible if they had an HbA1c below 75 mmol/mol (9%) and could be classified as having IAH on basis of a score of ≥3 out of 5 on the Dutch modified version of the Clarke questionnaire.18,19 Exclusion criteria were cardiac arrhythmias and use of antiarrhythmic agents. The research protocol was approved by the institutional review board and all patients provided written informed consent.
Procedure
Patients were invited to the research facility at 8.00 AM to undergo a hyperinsulinemic euglycemic hypoglycemic glucose clamp after overnight fasting and abstinence of alcohol and caffeine containing substances for 24 hours, as described previously. 17 Briefly, intravenous catheters were inserted into the antecubital vein of one forearm and into a dorsal hand vein of the opposite arm in retrograde fashion. The latter arm was placed into a heated box (55°C) for frequent blood sampling of arterialized venous blood at 5-minute intervals. The catheter in the other arm was used for infusion of glucose 20% (Baxter B.V., Deerfield, IL, USA) and insulin (insulin aspart; Novo Nordisk, Bagsvaerd, Denmark). Glucose levels were determined using Biosen C-Line (EKF Diagnostics, Cardiff, UK). After obtaining baseline variables, insulin was infused at a rate of 60 mU m-2 min-1 and glucose 20% at a variable rate to achieve and maintain euglycemia targeted at 90 mg/dl for 30 minutes, after which plasma glucose was allowed to fall to hypoglycemic levels and maintained there for another 45 minutes. Additional blood was sampled periodically for the measurement of adrenaline and noradrenaline at the same time as symptoms were scored using a translated version of the Edinburgh hypoglycemia questionnaire, containing generic, neuroglycopenic, and autonomic symptoms. A HealthPatch (VitalConnect, San Jose, CA) was placed on the chest during the whole procedure. The HealthPatch continuously measured heart rate with 125 Hz via single lead ECG recording, which was then transmitted via Bluetooth device (Apple Inc, Cupertino, CA). The unfiltered high-sampled data were used for data processing.
Data Analysis and Calculations
Continuous outcome measurements of HRV in the time domain analysis included standard deviation of the R-R intervals (SDNN) and root mean square of the successive differences (RMSSD). Frequency domain analysis was performed by Fast Fourier transformation and included low to high frequency ratio (LF:HF) with the use of Python 3.7. These HRV measures were chosen for comparability reasons and because they are according to standard guidelines 20 and have been validated. A 1-min-rolling 6-minute window was used for optimal frequency and temporal resolution. Missed and premature beats were corrected. Windows with artifacts were excluded. The data obtained during the 30 minutes of euglycemia were compared with those obtained during the 45 minutes of hypoglycemia (Figure 1).
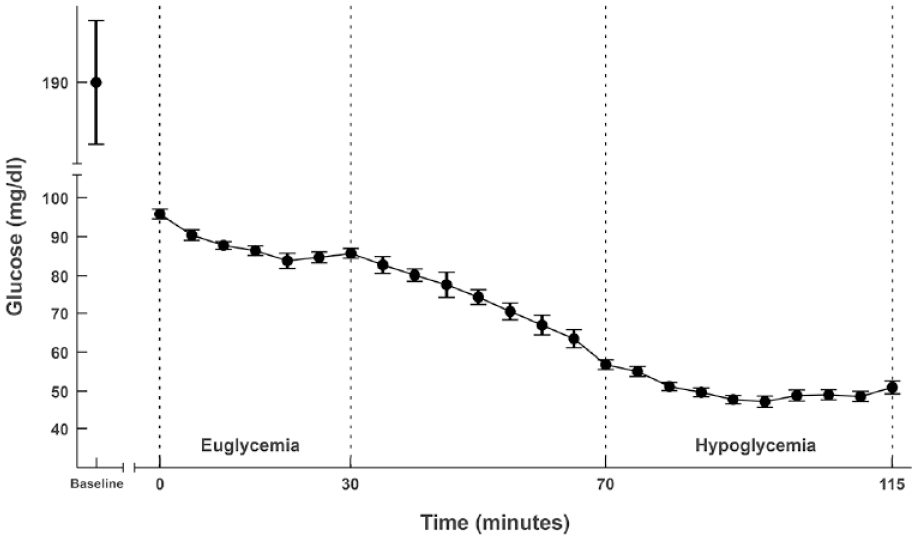
Glucose levels during the clamp.
Statistical Analysis
Normally distributed continuous variables are described using mean and standard error (SE) unless otherwise stated. Median and interquartile values are shown for variables that are not normally distributed. The qualitative or categorical variables, that is, baseline parameters, are described using frequencies and percentages. Wilcoxon rank-sum test was performed to determine significant difference within a participant by comparing HRV outcome measurements during euglycemia to those obtained during hypoglycemia with the use of SPSS 26 (IBM Corp., Armonk, NY). All hypoglycemic HRV measurements of each participant are normalized for the euglycemic measurements for that same participants, which we call euglycemic-normalized, and compared as one group. One Sample t test was used to evaluate euglycemia-normalized HRV measurements.
Results
Detailed characteristics of the participants are shown in Table 1. Eight persons were examined while on placebo treatment, whereas 4 were treated with the investigational compound (GLP-1 agonist, n = 2; SGLT-2 inhibitor, n = 2).
Baseline Characteristics.

Data are shown as number or means ± SD.
Glucose Clamp
During the clamp, plasma glucose averaged 87.9 ± 0.72 mg/dl during the euglycemic phase and reached a nadir of 43.1 ± 0.90 mg/dl during the hypoglycemic phase (Figure 1). In response to hypoglycemia, plasma adrenaline levels increased from 0.16 nmol/L (0.13-0.21) to 0.36 nmol/L (0.30-1.30, P = .002) (Supplementary Figure 1) and noradrenaline increased from 1.43 nmol/L (1.21-1.70) to 1.84 nmol/L (1.61-2.21, P = .002). Symptoms at euglycemia were 4.0 (1.5-7.0) and increased to 7.5 (5.0-11.0, P = .003) during hypoglycemia (Supplementary Figure 2).
Analysis of Heart Rate Variability
Supplementary Figure 3 shows an example of LF:HF measurements during the clamp procedure. The absolute LF:HF ratio increased from 1.33 (1.30-1.38) during euglycemia to 1.48 (1.44-1.52) during hypoglycemia (P < 0.001). The euglycemia-normalized LF:HF ratio increase during hypoglycemia averaged 1.09 (95% CI: 1.07-1.11, P < .001). Absolute RMSSD decreased from 26.1 ms (24.8-27.5) to 24.7 ms (23.7-25.7) during hypoglycemia (P = 0.198). The euglycemia-normalized RMSSD increase during hypoglycemia averaged 1.03 (95% CI: 1.01-1.06, P = 0.009).
Hypoglycemia caused a significant increase in LF:HF ratio in 6 of the 12 participants of which 3 also had a significant decrease in RMSSD. Four participants had a significant increase in RMSSD, of which one showed a decrease in LF:HF ratio (Figure 2). Only 2 of the 12 participants did not show any response in either of the 2 HRV measures. These 2 participants had no or a minimal change in symptom scores in response to hypoglycemia (+0 and +1), although adrenaline level increases (+0.23 and +0.32 nmol/l) were about average.

Effect of hypoglycemia on change of LF:HF ratio (y-axis) and change of RMSSD (x-axis). Every symbol represents one participant.
Discussion
In our study, symptom score and adrenaline responses to hypoglycemia were clearly attenuated in the participants, when compared to data published earlier in people with normal awareness of hypoglycemia, 21 reflecting suppressed sympathetic nervous system activity and confirming IAH. Nevertheless, hypoglycemia still caused HRV to change, as reflected by a significant increase in absolute LF:HF ratio and a non-significant decrease in absolute RMSSD. On the individual level, hypoglycemia-induced changes in HRV were retained in the majority of the participants, albeit not always with the typical response. Finally, we showed that the changes in HRV can be detected by a wearable device, which provides promise for future clinical application.
Our data are in line with previous studies demonstrating changes in HRV during experimental hypoglycemia in people with type 1 diabetes and healthy individuals13,22 and extend these to the population of people with type 1 diabetes and IAH. Also, the finding that the typical response of increased LF:HF ratio and decreased RMSSD, as reflection of increased sympathetic and decreased parasympathetic activity, respectively, was often absent in the population studied, corroborates previous observations. In a study among outpatients with type 1 diabetes in whom HRV was monitored for a week, we found that hypoglycemia caused typical HRV changes in 55% of the hypoglycemic events and no or an ambiguous response in 18%. 15
IAH is a clinical diagnosis, characterized by absence of timely perception of hypoglycemia by the affected person—although family members often retain recognition of its symptoms—and suppression of sympathetic nervous system activation as its underlying mechanism. Our finding that most participants with IAH had a measurable HRV response during hypoglycemia indicates first that such suppression is seldomly complete and second that even (very) low levels of sympathetic activation are sufficient for HRV to change. Analogously, Cichosz et al. showed reduced, but not lost, sympathetic nervous system activation in patients with type 1 diabetes and cardiac autonomic neuropathy. 23 The absence of a symptom response in the 2 participants in whom no HRV response to hypoglycemia could be detected may reflect the lowest level of sympathetic nervous system activation required to elicit a change in HRV. Whether lower levels of hypoglycemia would have provoked an HRV response in these participants remains speculative.
IAH in people with type 1 or type 2 diabetes is associated with several-fold higher risk for severe hypoglycemic events. 3 These patients would obviously benefit from an early warning device to prevent such events. Although there is a longstanding interest in clinical applications of HRV, 21 whether HRV monitoring can be used for the detection of hypoglycemia in people at increased risk of severe hypoglycemia requires further study. This is in part because of the large variability in HRV as it is determined by individual characteristics such as age and sex, as well as situational factors like mood and physical activity.24,25 Given that the intraindividual variation in HRV is much smaller,26,27 improved data analysis and deep machine learning techniques should be further validated and precisely applied before the potential of HRV monitoring for hypoglycemia detection can be fully appreciated and implemented. Even with limited specificity but high sensitivity, use of HRV could be beneficial to alert patients for potential hypoglycemia and expedite necessary actions, and would even better in addition to existing additional diagnostics.
A strength of the study is the glucose clamp setting in which frequent blood sampling offers the potential to investigate the time related effect of hypoglycemia on HRV changes. Using validated measures with state-of-the-art methods with 1-minute-rolling 6-minute windows instead of the superseded subsequent 5-minute windows ensured high frequency resolution on a small time scale and small data losses due to artefacts and enabled investigation of HRV changes in IAH compared to other T1D studies. The study also has limitations. Because data were derived from 2 trials on GLP-1 receptor agonists or SGLT-2 inhibitors, some participants were on either of these agents during data collection. However, although treatment with GLP-1 receptor agonists can increase resting heart rate, they have not been found to affect HRV in general or under hypoglycemic conditions in particular. 28 Similarly, SGLT-2 inhibitors have not been found to alter HRV in people with type 1 diabetes, albeit in the absence of concurrent hypoglycemia. 29 The results did not materially change after exclusion of participants using these medications. Another limitation is that we performed a one-step hypoglycemic clamp, so that we are unable to determine a glucose threshold level below which HRV starts to change. However, this was not the purpose of the study and we would posit such thresholds to be highly variable, depending on prior exposure to hypoglycemia. One may also criticize the lack of a control group consisting of people with diabetes and intact awareness of hypoglycemia. However, we aimed to examine the appearance of an HRV response per se rather than the magnitude of such a response, which obviates the need for a control group.
Conclusions
In conclusion, hypoglycemia-induced changes in HRV are retained in the majority of people with type 1 diabetes and IAH, despite almost complete blunting of symptomatic perception of hypoglycemia, and that these changes in HRV can be detected by a wearable device. Considering developments in wearable devices and data analytics, real-time HRV seems usable for detection of hypoglycemia in patients with IAH.
Supplemental Material
sj-png-1-dst-10.1177_19322968211007485 – Supplemental material for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia
Supplemental material, sj-png-1-dst-10.1177_19322968211007485 for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia by Mats Koeneman, Marleen Olde Bekkink, Lian van Meijel, Sebastian Bredie and Bastiaan de Galan in Journal of Diabetes Science and Technology
Supplemental Material
sj-png-2-dst-10.1177_19322968211007485 – Supplemental material for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia
Supplemental material, sj-png-2-dst-10.1177_19322968211007485 for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia by Mats Koeneman, Marleen Olde Bekkink, Lian van Meijel, Sebastian Bredie and Bastiaan de Galan in Journal of Diabetes Science and Technology
Supplemental Material
sj-png-3-dst-10.1177_19322968211007485 – Supplemental material for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia
Supplemental material, sj-png-3-dst-10.1177_19322968211007485 for Effect of Hypoglycemia on Heart Rate Variability in People with Type 1 Diabetes and Impaired Awareness of Hypoglycemia by Mats Koeneman, Marleen Olde Bekkink, Lian van Meijel, Sebastian Bredie and Bastiaan de Galan in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
We are indebted to the willingness of all patients who took part in this study.
Abbreviations
GLP-1, glucagon-like peptide-1; HRV, heart rate variability; LF:HF, low to high frequency; IAH, impaired awareness of hypoglycemia; RMSSD, root mean square of the successive differences; SGLT-2, sodium glucose cotransport-2; SDNN, standard deviation of the R-R intervals; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant 2016.30.004 from the Dutch Diabetes Research Foundation. The study on the effect of a GLP-1 receptor agonist on IAH was supported by AstraZeneca, but the sponsor was not involved in the present analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.