
Abstract
Background:
Rapid expansion of mobile technology has resulted in the development of many mobile health (“mHealth”) platforms for health monitoring and support. However, applicability, desirability, and extent of tailoring of these platforms for pregnant women, particularly in populations who experience the greatest health inequities—such as women with diabetes mellitus (DM) and/or those with greater socioeconomic barriers—remains unknown. The objective is to understand low-income pregnant women’s experiences and preferences for mHealth tools to support DM health and improve DM self-management during pregnancy.
Methods:
Low-income pregnant and postpartum women were included in individual interviews or focus groups; women with type 2 DM, gestational DM, or no DM were included. Analysis was performed with the constant comparison method.
Results:
In this population of 45 (N=37 with DM) low-income, largely minority, pregnant and postpartum women, 100% reported access to smartphones and prior experience with apps. Interest in mHealth to support health and engagement during pregnancy was high. Preferences for general mHealth features included education that reduces uncertainty, support communities, visualizing progress, convenient access to information, and support for better management of pregnancy-related tasks. Preferred design elements included personalization, interactive features, and integrated graphics. Women with DM expressed multiple additional DM-specific needs, including support tools for DM self-management and self-regulation tasks.
Conclusion:
Pregnant and postpartum women, especially those with DM, desire mHealth technology to support engagement and to adapt lifestyle guidelines and treatment requirements for a healthy pregnancy. Further work to develop mHealth interventions tailored for target populations remains a key step in reducing health inequities and promoting access to evidence-based perinatal health interventions.
Introduction
The antenatal period is a time of increased learning requirements and health behavior change, especially among women with gestational diabetes mellitus (GDM) or type 2 diabetes mellitus (T2DM).1–3 Studies have noted knowledge gaps among pregnant women, which may negatively affect pregnancy outcomes,4-9 making antenatal education and support an important consideration in prenatal care.10,11 However, disparities still exist to prenatal care access, more specifically to quality prenatal care and education among minority and low-income pregnant women. 12 Studies of pregnant women’s experiences indicate that interventions which support comprehensive, personalized education and behavior change could be beneficial.12–16 Such interventions may be especially impactful for low-income and minority women who experience greater barriers to high-quality care.
Mobile health (mHealth) has been used successfully in a variety of populations—including pregnant women—to promote behavior change.17–24 Mobile phones are widely accessible among low-income populations,25,26 and studies indicate that pregnant women have both access to and interest in mHealth interventions,14,15,27-29 supporting these tools as attractive options for antenatal and postpartum health interventions. However, more research is needed to optimize mHealth interventions for pregnancy. Interactions with mobile technology and trust in information from mobile or internet sources vary by race and socioeconomic status.30–32 With regard to those with DM, individuals are provided principles for treatment to activate self-care and make everyday decisions for their DM. In a pregnancy complicated by DM, the utilization of a mHealth intervention could assist with these decisions for rapid behavioral change. Relevant and meaningful use of mHealth may also generate health behaviors that can provide benefit both during pregnancy and for future health. Yet, despite increased requirements for health behavior change necessary in a pregnancy complicated by DM,3,33-35 little is known about the effect of mHealth interventions for pregnant women with DM. 20
Thus, our goal was to conduct an in-depth qualitative investigation to understand the experiences and preferences of low-income pregnant women with DM regarding the use of mHealth apps to support pregnancy and reduce inequities in healthcare and health outcomes. In order to understand the compounded barriers that low-income pregnant women with DM face, we specifically investigated how mHealth platforms may be used to improve DM self-management.
Methods
This qualitative study investigated the mHealth preferences of a diverse group pregnant women with and without GDM or T2DM. Data for this analysis were compiled from a multiphase investigation of a novel motivational and educational mHealth application for use by women with DM during pregnancy. 36 All study activities were approved by the Northwestern University Institutional Review Board. All participants provided written, informed consent and were compensated with gift cards.
Participants were recruited from two obstetrics and gynecology practices at Northwestern Memorial Hospital in Chicago, Illinois, from April 2018 to August 2019. Individuals were eligible for participation if they were at least 18 years old, were able to participate in English, were low-income (defined below), and were pregnant or recently postpartum (within 6 weeks of delivery). Patients with and without GDM or T2DM were eligible to participate, although the focus of investigation, and thus recruitment, was on women with DM. Low-income status was defined as having public insurance or total household income less than 200% of the federal poverty line (as identified via assessment from social work personnel). In order to recruit individuals with DM, research personnel conducted targeted screening of the patient census at these practices and approached all individuals who appeared to meet eligibility criteria. For recruitment of individuals without DM, a convenience sample of individuals meeting eligibility criteria was recruited from the inpatient antepartum and postpartum hospital census. Although the primary objective of the study was to understand mHealth preferences among pregnant women with DM, this sample was included to investigate generalized mHealth experiences and preferences that may support low-income women during pregnancy. Trained research personnel conducted focus groups and individual interviews, depending on the investigation phase. Semistructured interview guides encouraged candid conversations. The goal of the primary study was to test early phases of the novel mHealth tool; this analysis addresses broader mHealth preferences, based on participants’ actual experiences and/or general “wish list” features, that were probed during each phase of study.
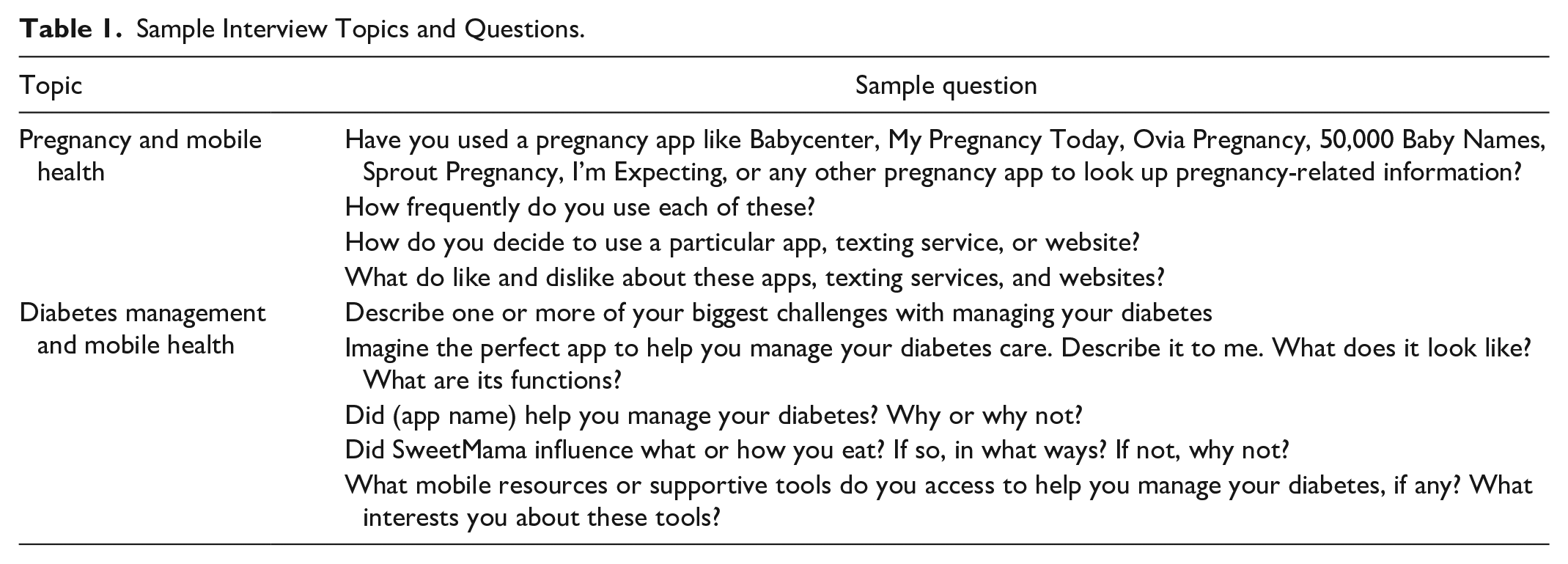
Interview guides featured questions on general mHealth desires, familiarity with mHealth technology, and perspectives on DM-specific mHealth features and preferences (when applicable). Queries focused both on the specific mobile application under investigation as well as general preferences and desires for mHealth applications. Sample questions can be found in Table 1. Interviews lasted 30 to 60 minutes and were digitally recorded, transcribed verbatim, and uploaded to a secure qualitative data storage platform (dedoose.com). Transcripts were analyzed using the constant comparative method. 37 Two independent research assistants iteratively read half of the transcripts and noted recurring concepts called subthemes. All subthemes were discussed with the larger team and were organized into overarching themes. Themes and subthemes were compiled into a codebook, which was utilized to code all remaining transcripts after assuring agreement among team members. A Dedoose “Training Center” test was conducted to determine the Pooled Cohen’s Kappa coefficient, a value summarizing agreement between the test-takers across a selected sample of codes.
Sample Interview Topics and Questions.
Results include themes and subthemes regarding the preferences, experiences, and knowledge about mHealth among low-income pregnant women, including those with DM.
Results
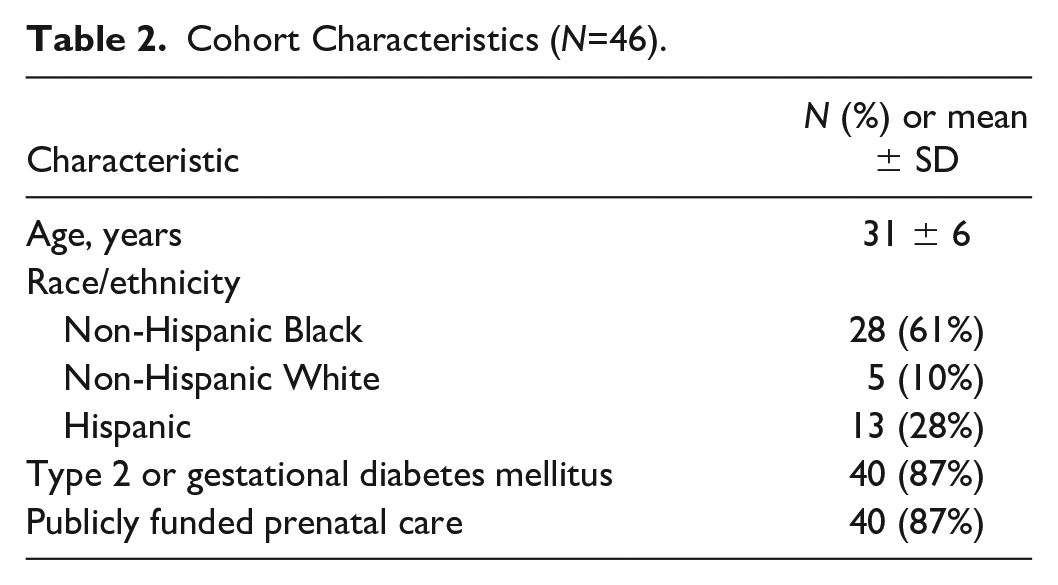
During this study period, 46 women consented to participate. Participants were majority non-Hispanic Black (N=28, 61%) and N=40 (87%) received public insurance. Eighty-seven percent (N=40) had T2DM or GDM (Table 2). All participants reported smartphone access and familiarity with apps. After thematic analysis, the resulting Pooled Cohen’s Kappa coefficient was 0.91 from a sample of 2 to 4 code applications per subtheme (44 excerpts total), indicating high interrater reliability.
Cohort Characteristics (N=46).
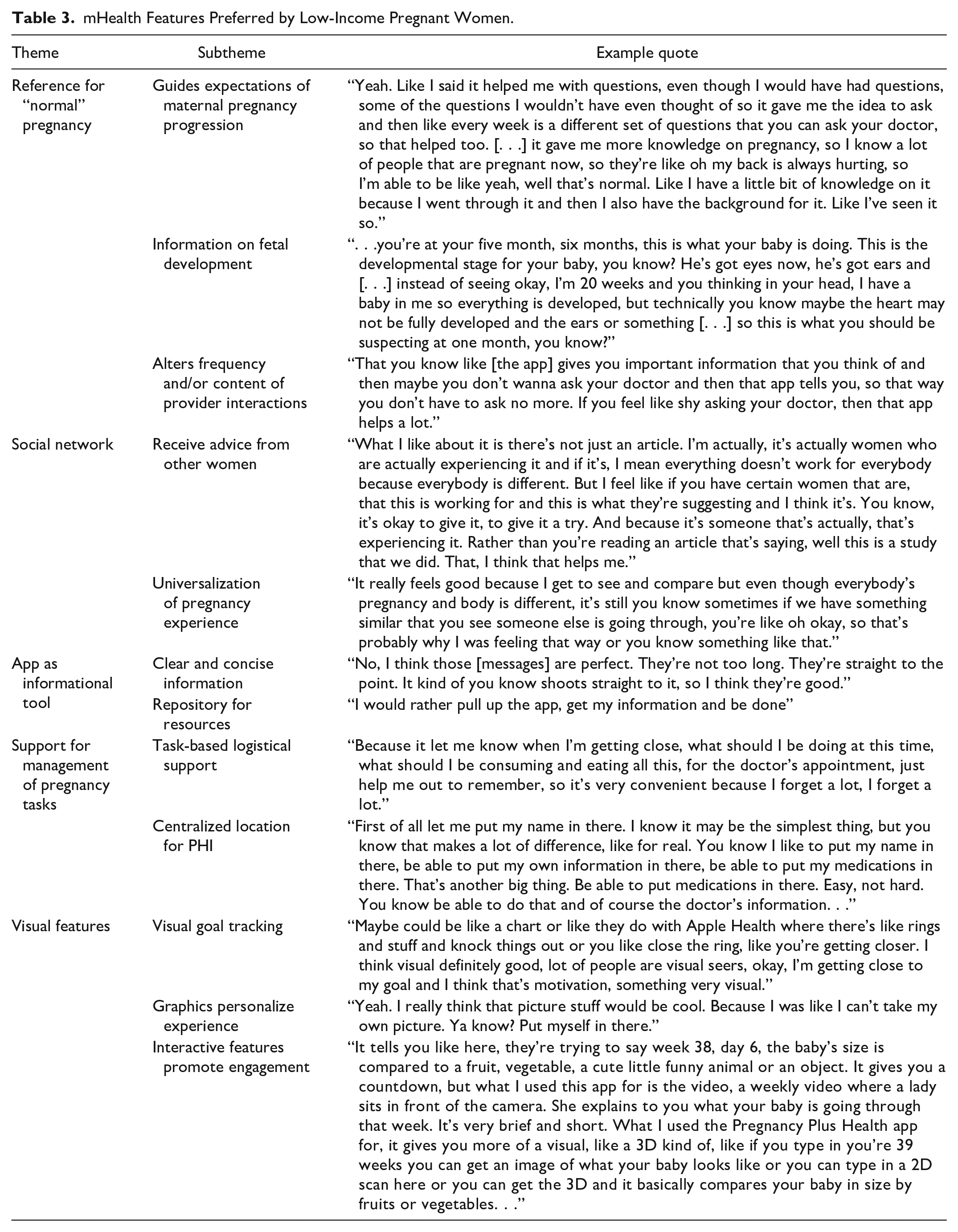
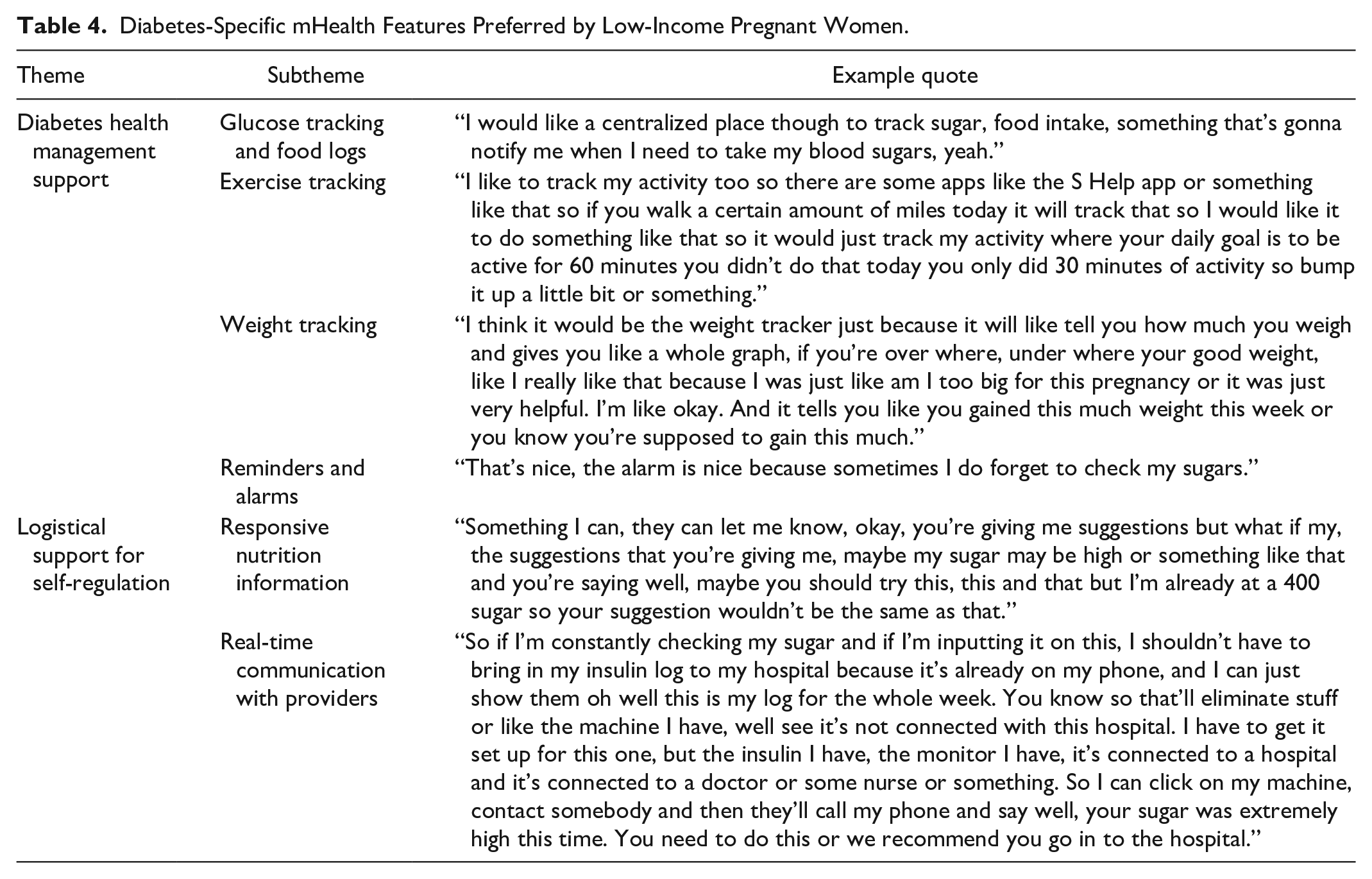
Themes regarding pregnant participants’ mHealth preferences were categorized based on whether the theme was unique to DM. The mHealth preferences related specifically to DM management were noted to be in addition to the general pregnancy mHealth preferences, and participants overwhelmingly reported that combining general pregnancy features with diabetes-specific features would be most responsive to their needs. Results are described below; exemplary quotations are found in Tables 3 and 4.
mHealth Features Preferred by Low-Income Pregnant Women.
Diabetes-Specific mHealth Features Preferred by Low-Income Pregnant Women.
General mHealth Preferences
App as Reference for “Normal” Pregnancy
Guides expectations of maternal pregnancy progression to reduce uncertainty
When queried about their favorite features of pregnancy apps, many participants reported using the app as a reference for a typical pregnancy. Participants expressed uncertainty about expectations during pregnancy and found apps to be helpful resources. As one participant said, “I just go in there and look up 32 weeks and then it be like you’ll start feeling back pain and all that, so it’s a really helpful app.” Apps reassured users about physical changes and emotional fluctuations during pregnancy, and provided a source of information to individuals with diminished access to care and other support systems.
Information on fetal development
Apps were used as a reference for the expected progression of fetal development, which was perceived to be engaging and educational. For example, apps reported fetal milestones, such as the development of a heart. One participant said, “The app basically it goes week by week with pregnancy [. . .] you have like videos of what to expect [. . .] Like if your baby is growing its ears or whatever the case may be. . .”
Alter frequency and content of provider interactions
Using apps to find information to avoid or delay the next prenatal appointment, or to augment information already given, was a prominent theme. When access to providers was inadequate, participants reported using apps to fill the gap. One participant reported, “. . .for a good month I wasn’t able to go to the doctor and like I had the app to you know keep me walking through it.” Participants reported finding that information on apps shortened appointment times and in some cases it “save[d] [them] a lot of doctors’ appointments.” Some used apps to clarify information, find questions to ask during appointments, and learn what would happen at each appointment. Notably, many participants did not consider apps an adequate alternative to appointments. In most cases, women felt the information they found needed to be corroborated by a healthcare professional.
Social Network
Receive advice from other women
The potential for social interaction and crowdsourced answers within mHealth platforms was widely appreciated in our cohort. In prior experiences with mHealth related to pregnancy, women asked and/or answered questions in forums, joined “birth month clubs,” participated in polls, and sometimes read responses rather than interacting directly. Participants appreciated the opportunity to know “what other moms think,” often in cases of concern about bodily changes (eg, stretch marks), or when trying different remedies for pregnancy symptoms (eg, lemons for nausea). Quicker response times and more diverse opinions were benefits of crowdsourced information. Notably, some participants reported that these forums or polls motivated their daily interaction with apps.
Universalization of experience
Social interaction through apps also provided support and validation during pregnancy, particularly during perceived stressful experiences. Women often sought evidence that “it’s not just me” or that they weren’t “crazy.” Participants reported being comforted by stories of “real” women, particularly for other women experiencing complications such as DM. For example, one participant said, “It felt good ‘cause I’m like okay, so I’m not the only one experiencing this. . .”
App as Informational Tool
Clear and concise information
Our cohort appreciated when information provided in apps was given in non-academic terms, was presented clearly, and was engaging. One participant described an app she used: “It’ll give me tips on. . . like the baby is the size of an orange this week. The doctor wouldn’t. . . put it in those words or give me that type of visual description.” Information provided by apps was described as “plain and simple” while interactions with healthcare professionals were recounted differently; “sometimes the doctors, they’re giving you all these big words and you’re just like oh okay. Can you put it into English now?” Apps also made video or visual learning options available. As one participant reported, “if you don’t wanna read it. . . it’s a woman literally explaining it to you and basically reading it to you.”
Repository for resources
One significant benefit of apps was their accessibility. Apps were described as “easy” and “straightforward,” often in contrast to the internet. One participant noted that mobile apps “just narrows it down,” while Google resulted in “a bunch of different links and a bunch of different information.” Our cohort not only appreciated the simplicity of finding information on apps, but also their potential as a centralized source of pregnancy- or DM-related educational materials. Ideally, many expressed, they wanted “everything in one app.”
Support for Management of Pregnancy Tasks
Task-based logistical support
Participants reported that they valued apps that supported pregnancy- and DM-related tasks. For example, women appreciated alerts for doctor’s appointments and medication timing, as well as reminders about when to come fasting to appointments or when to make recommended dietary changes. Women described reminder functions as “helpful” and like a “backup brain.” Women also appreciated practical support with tasks such as exercising during pregnancy or selecting a pediatrician.
Centralized location for PHI
Our cohort appreciated that apps could serve as a repository for personal health information (PHI) in addition to being pregnancy resources. For example, women liked having a centralized location for information about their medications, doctors, tests completed throughout pregnancy, and gestational age. Some favored using pregnancy apps to access PHI and message health care providers over health portals provided by their hospital. As one participant expressed, “. . .you can go into the portal too, but I don’t wanna have to do that. I would rather pull up the app, get my information and be done.”
Visual Features
Visual goal tracking
Participants expressed a desire for visual goal tracking and encouragement to provide positive reinforcement for health behavior changes. As one woman said, “. . .if I’m on track, shoot me up a little happy face emoji or something. . .to just encourage me along.” Our cohort desired support through visual goal tracking between appointments; as one participant put it:
“I wish that I could log in my own personal trends and be able to see it on a graph for my blood sugars, I feel like having it be more interactive, less reading maybe . . .and more interactive options.”
Some participants favored visual encouragement catered at their goal of a health pregnancy:
I think for goals, maybe instead of a trophy, something to do with pregnancy, maybe baby shoes. . .My goal is healthy babies. . ..So maybe changing that. . ..just remind ourselves this is what we’re working for. Babies out of our tummies and healthy.
Using graphics to personalize experience
Participants’ preferences for personalization were diverse. Many desired the ability to add images of themselves or their ultrasound images to pregnancy apps; others desired the ability to reorganize app sections and menus. Cultural representation in pregnancy application icons was a concern. One participant described her feelings about an app icon:
“I mean like she’s a pale brown-haired woman. I’m not pale and I’m not brown haired, so it’s like okay that’s not me at all. . .I think it’s always hard when you pick a picture of a woman because we look all so different. . .if I saw that in. . .the app store, like that little icon, I wouldn’t probably pick it.”
Interactive features promote engagement
Visually interesting graphics and interactive features were favored among our cohort and were described as drivers of engagement with apps. Participants reported interest in bright colors with high-quality graphics, describing these features as ones that make applications “more personable” and “less sterile.” Video content, as opposed to text, was often preferred and deemed “easier to absorb.” Participants enjoyed features such as group polling, question boards, and mini-quizzes. Additionally, many women who used apps for pregnancy liked graphically seeing fetal growth compared to common objects, reporting that these visuals were often the reason they checked their pregnancy app daily.
Diabetes-Specific mHealth Preferences
Logistical Support for Diabetes Management
Glucose tracking and food/carbohydrate logs
Members of our cohort with DM preferred apps that could help with glucose tracking, carbohydrate intake, and food logging. Participants desired an app to track blood sugar so they would “not have to worry about carrying a book around or finding a pen,” and so they could add notes about meals or incidents related to abnormal blood sugars. Many also felt that apps could help them understand and track their daily carbohydrate intake. They reported difficulty understanding daily “limits,” and preferred their phones as easy record-keepers: “it was good to have it right on my phone [ rather than] to have it in my brain.” Desires for food logging were more varied; while some participants preferred apps with food logging, others found it too time-intensive.
Weight and exercise tracking
While less commonly discussed, some participants appreciated features for tracking exercise and weight, which they found encouraging. Similar to other health tracking features, participants wanted to have a comprehensive log available on their phones to show healthcare providers.
Reminders and alarms
Members of our cohort with DM were vocal about preferring an app that would help them track and remember DM management tasks. Centralization was a common request; participants wanted an app that “gives you everything,” and “would love it if [apps] could do everything in one spot” rather than visiting separate apps, portals, or web-based resources. Desired features included automated reminders to take insulin, check glucose, and eat meals/snacks, as well as the ability to add personalized alarms and reminders, and desired complex management reminders. For example, one participant said, “I would like for it to be able to remind me. . .if your [glucose] level is this, remember you can do this and you can do that.”
Logistical Support for Self-Regulation
Responsive nutrition information
Participants with DM wanted information about healthy foods during pregnancy, ideas for recipes and snacks, and personalized feedback on their food choices. Our cohort preferred responsive technology that could help them “notice trends” about food intake and blood sugar, indicate whether they had been “on track” for the day, and offer suggestions if not. Personalization requests included suggestions for “dealing with the cravings,” making child-friendly recipes, and providing culturally diverse recipes that incorporate DM guidelines for medical nutritional therapy.
Real-time communication with providers
A mainstay of perinatal DM therapy is regular communication with providers about glucose monitoring results and other aspects of perinatal DM care. Many participants expressed that they had more frequent questions and concerns than their appointments were spaced to handle, making app-facilitated timely communication with providers appealing. Real-time provider feedback on diet and blood sugars was also favored. One participant desired a way to share her glucose readings in real time with her provider so that “they can reach out to you and be like [. . .] let’s schedule a visit a little bit earlier so you can come in and I can help you get back on track. . .”
Discussion
Few studies have investigated mHealth preferences among pregnant women who experience increased burdens of care—such as those with DM—or preferences of women with increased barriers to care—such as those with low income. This study provides a novel perspective regarding women’s experiences with apps during pregnancy, as well as their preferences for future directions in pregnancy- and DM-specific app development. As has been seen previously,20,22,27,28,38-41 this cohort found apps to be accessible and acceptable sources of information about pregnancy and DM. Participants expressed a preference for apps over other sources of information, including internet sites and provider visits, highlighting the need for apps to include reliable educational information. Suggestions included the use of interactive, simple features to support the health behavior needs of patients with and without DM. Additionally, participants identified the importance of combining general pregnancy mHealth features with diabetes-specific features. They expressed a strong preference for a comprehensive app to support pregnancy, and addressing general pregnancy health in addition to diabetes-specific health was felt to be essential.
These findings provide useful patient-centered feedback for the development of DM-specific pregnancy apps. Specific DM features may include goal-setting, relevant self-care tasks, and strategies to boost motivation and self-efficacy. For example, pregnancy apps may include interactive features to engage women in learning about and monitoring their pregnancies, which may be particularly helpful in complex learning or high maternal health need states, such as DM. Future apps should consider how to ensure that presentation of content promotes increased health literacy and engagement, including straightforward language, videos, and graphics. Such consideration is necessary to maximize the potential of apps as tools to decrease inequities in access to high-quality prenatal care and improve health outcomes. 42
A strength of our study is the inclusion of a diverse patient population from a large urban medical center. Additionally, our study design allowed us to investigate patient mHealth preferences in women with and without a DM diagnosis in order to examine a broad range of mHealth experiences and preferences, including DM-specific topics, with the intention to elevate overall perinatal health. This study is limited in its generalizability due to inclusion of participants from a single center. However, the strengths of qualitative work allow for richer, in-depth descriptions of patients’ lived experiences that can offer insight into the characteristics that render mHealth apps useful, and qualitative data are intended to be hypothesis-generating rather than widely generalizable. Additionally, participant lack of comment on a certain topic may not indicate an absence of an opinion and may instead indicate a lack of an explicit query.
Conclusions
The adoption of evidence-based mHealth technology to support the health of low-income pregnant women with DM may be one novel approach to reduce disparities in DM-related perinatal outcomes. In this study, participants expressed desires for an engaging and personally tailored mHealth app to assist with pregnancy tasks, educate on healthy pregnancy progression, and connect with others. DM-specific preferences which align with DM self-management skills necessary to optimize glycemic control in pregnancy include blood glucose monitoring, meal planning, and weight tracking. Other features include support for managing appointments, medications, and other DM tasks. Future work should center on mHealth preferences, particularly those of women with increased barriers to care access, in order to create effective interventions to support pregnancy and improve DM self-management.
Footnotes
Abbreviations
app, application; DM, diabetes mellitus; GDM, gestational diabetes mellitus; mHealth, mobile health; T2DM, type 2 diabetes mellitus.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Contribution Statement
KL and EB jointly conceived the scientific design, performed the data analysis, and wrote the manuscript. JJ and AS supported the research design, performed the interviews, assisted with analysis, and edited the manuscript. CN supported the scientific design, provided clinical and technical knowledge for the analysis, and edited the manuscript. LMY wrote the grants that funded this work, conceived the scientific design, supervised with data analysis, provided the technical knowledge for the manuscript, and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lynn M. Yee was supported by the NICHD K12 HD050121-11 at the time of the study. Additionally, this work was supported by the NICHD R21 HD094271 and the Friends of Prentice Grants Initiative (FY2019).