
Abstract
Background:
Management of diabetes mellitus (DM) during pregnancy is burdensome given the intensity of required patient engagement and skills, especially for women with greater social disadvantage. Mobile health (mHealth) technology is a promising avenue for DM health promotion, but few evidence-based mHealth tools exist for pregnancy. Thus, we designed a theory-driven mHealth tool called SweetMama, and planned a priori to gather usability and acceptability feedback from patients and providers to ensure a user-centered design.
Methods:
In this qualitative assessment, we solicited patient and provider feedback on this novel educational and motivational mobile application for low-income pregnant women with type 2 or gestational DM. Patients and providers participated in separate focus groups. Participants shared feedback regarding SweetMama’s visual appeal, architecture, and content. SweetMama modifications were made in an iterative manner. Transcripts were analyzed using the constant comparative technique.
Results:
Patient (N = 16) and provider (N = 29) feedback was organized as positive feedback, negative feedback, or additional desired features. Within each category, themes addressed SweetMama visual features, information, or functional features. The majority of negative feedback was addressed and multiple desired features were implemented via iterative application development, resulting in a user-friendly, efficient, and potentially impactful mHealth app designed to support the unique needs of this population.
Conclusions:
SweetMama users had largely positive feedback about the mHealth tool’s appeal, content, and functionality. Suggested improvements were incorporated in preparation for further evaluation steps, which include longitudinal usability testing, feasibility trials, and larger trials to determine the efficacy of SweetMama use for improving perinatal outcomes.
Keywords
Introduction
Diabetes mellitus (DM) during pregnancy is an increasingly prevalent public health problem, driven by the growing obesity epidemic.1-7 Both gestational diabetes mellitus (GDM) and type 2 diabetes mellitus (T2DM) pose risks to the health of the pregnant woman and her fetus, such as cesarean delivery, hypertensive disorders, macrosomia, and neonatal metabolic complications.8,9 Moreover, racial, ethnic, and socioeconomic disparities related to DM during pregnancy exist, with minority and low-income women at greater risk of GDM, T2DM, and recurrence of GDM.2,7-17
Treatment of abnormal glucose homeostasis during pregnancy reduces the risk of adverse outcomes.18,19 However, logistical, social, financial, informational, access-related, and attitudinal challenges to DM management exist.20-27 Furthermore, given the complexity and intensity of perinatal DM management, women must be equipped with a multitude of communication, literacy, numeracy, problem-solving, and organizational skills to optimize outcomes.20,21 Thus, DM self-management during pregnancy is burdensome and challenging, particularly for women with greater social disadvantage. 25 Although traditional DM behavior support interventions such as in-person coaching can be effective for nonpregnant adults, 28 such interventions have been less commonly studied in pregnancy and scalable interventions that promote sustainable behavior change, address disparities, and are specific to pregnancy are needed.29,30
Mobile health (mHealth) technology is a promising avenue for promoting sustainable behavior change, addressing disparities, and promoting self-efficacy. 30 mHealth technology has been effective in supporting DM management in nonpregnant populations. 31 Furthermore, work by Alqudah et al indicates that women are willing to utilize mHealth technology to remotely manage their pregnancy, under management by healthcare staff, suggesting potential acceptability of various mHealth tools. 32 However, many programs lack rigorous evidence-based or user-centered design, 33 and DM-specific perinatal mHealth interventions, particularly for low-income populations, are absent. 34 Additionally, although some commercial mHealth products are designed to enhance glucose logging or track personal progress, interventions largely fail to promote the skills required for sustainable and successful DM self-management during pregnancy.35-37
To fill this gap, we initiated a multiphase project to develop a mHealth intervention to support pregnant women with DM, with particular attention to low-income women. In prior work we developed a model of barriers to self-care and mitigating factors, which served as a foundation for a text message-based mHealth intervention designed to facilitate DM self-management during pregnancy.25-27,38 Feedback from this text messaging phase indicated that although the curriculum was well received, users desired a more extensive and interactive platform. We subsequently developed SweetMama, a mobile-friendly web-based application. SweetMama delivers a comprehensive educational and motivational DM-focused curriculum tailored for low-income pregnant women with GDM or T2DM with the long-term goal to improve perinatal DM-related outcomes. Adopting a user-centered design approach, the objective of this study was to gather SweetMama feedback from patients and healthcare providers, which informed the iterative modifications necessary to enhance the application’s usability, functionality, and accessibility. This analysis reports on this feedback and modification phase.
Methods
Overview
This prospective, qualitative study was designed to elicit feedback from patients and healthcare providers regarding usability of the SweetMama prototype. Data from this phase represent participants’ first exposure to SweetMama. Patient and healthcare provider participants were recruited from the Prentice Ambulatory Care practice at Northwestern Memorial Hospital, a large academic medical center in Chicago, Illinois, from August 2017 to March 2019. The first phase (August 2017 to July 2018) focused on patient users and the second phase (December 2018 to March 2019) focused on providers. All participants provided written informed consent. This study was approved by the Northwestern University Institutional Review Board.
Participants
Patients were eligible for study participation if they were at least 18 years old, diagnosed with GDM or T2DM, spoke English as a first language, and received public insurance for prenatal care. Patients were recruited during routine clinical care in the DM-focused clinic within this practice. Test smartphones were provided for patient focus groups so that smartphone access was not a barrier to participation. Patient focus groups were conducted separately from provider focus groups.
Any provider with experience treating or educating pregnant women with DM was eligible for participation. Eligible providers included physicians, nurses, medical assistants, and health educators. All providers were over age 18 and English-speaking. Provider participants were recruited by conducting a review of the institution’s clinical personnel records. Provider focus groups were intentionally composed of providers of different types. All providers used their own smartphones for participation.
Focus Group Conduct
Participants were organized into focus groups of three to seven individuals. Focus groups were conducted by a trained research assistant using a semi-structured interview guide to facilitate open-ended conversation. The e-Health “User-Task-Context” (UTC) usability framework was used to develop the interview guide and frame the direction of probes; the UTC helps clarify user requirements and preferences during development stages of novel eHealth/mHealth programs. 39 During focus groups, participants were presented with an early, minimally functional SweetMama prototype and were instructed to think aloud as they interacted with the prototype. The “Think Aloud” protocol is a common approach to usability testing where participants verbalize their thoughts as they perform a certain task. 40 This approach permits investigators to evaluate the ease of learning the system and provides first-hand information about design problems. 41 In this case, participants were asked to familiarize themselves with SweetMama and use it how they would in a real-world setting. Development of the application occurred iteratively such that different participants were not always presented with the same version of the application (ie, prototypes often reflected modifications not featured in prior versions). No at-home use of SweetMama was included. Focus groups lasted 60-75 minutes and were recorded on a digital audio recorder. All participants were compensated with gift cards.
SweetMama Features and Development
Original SweetMama features, developed based on established health behavior theories as well as feedback from a prior text message-only phase, involved SweetMama users receiving three motivational and/or informational tip messages, and one individualized goal message, per week.25-27,38,42-45 Messages are designed to promote self-efficacy, healthcare engagement, and health knowledge.46-48 Message content addresses knowledge regarding DM and pregnancy and provides information tailored for the needs of low-income individuals, such as inclusion of regional resources like local food banks and community centers, while also ensuring culturally competent content. Messages were tested in prior phases of work and adapted as needed. 38 Given that low health literacy has been identified to be a barrier to DM self-management in this population, content was also delivered via simple and straightforward language, tailored such that the majority of content was at a sixth grade reading level or less. Individualized goals, based on the goals for DM self-management by the American Association of Diabetes Educators, are set by patients and providers together during routine healthcare, and are delivered weekly via SweetMama to serve as a reminder and benchmark for goal-oriented behaviors.46,47 The motivational, tip, and goal messages allow users to either exit the message or press a button taking them to more detailed information related to the message (Figure 1a and b). In the original version of SweetMama, these messages appeared on a home screen, but based on patient’s feedback (discussed below), later versions experienced by patient and provider participants housed messages in a message center (Figure 2). The home screen (Figure 3a–c) in later versions was reserved for personalized information, including the participant’s first name, gestational age, next appointment, and a technical support request portal.
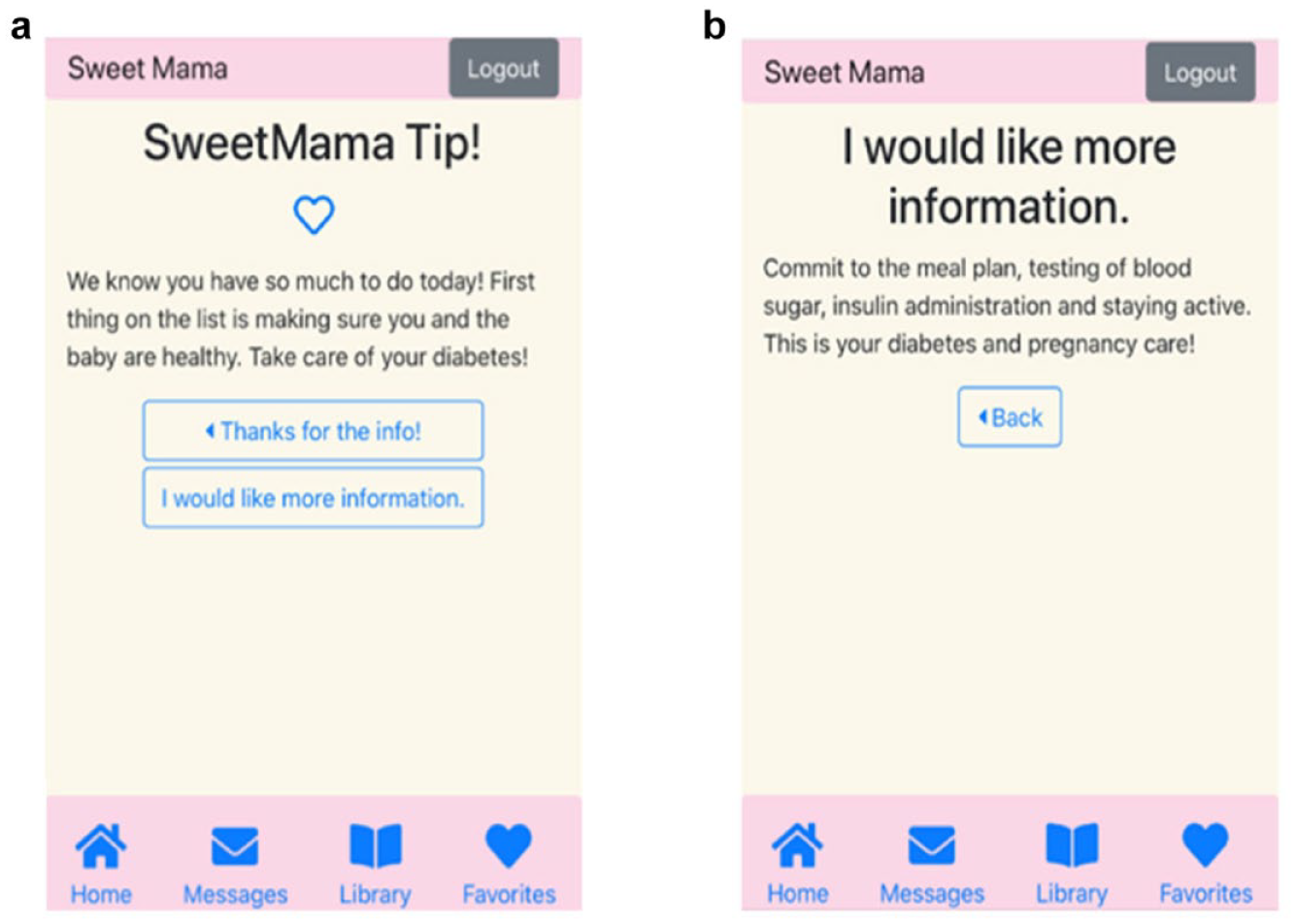
Example of SweetMama motivational message.
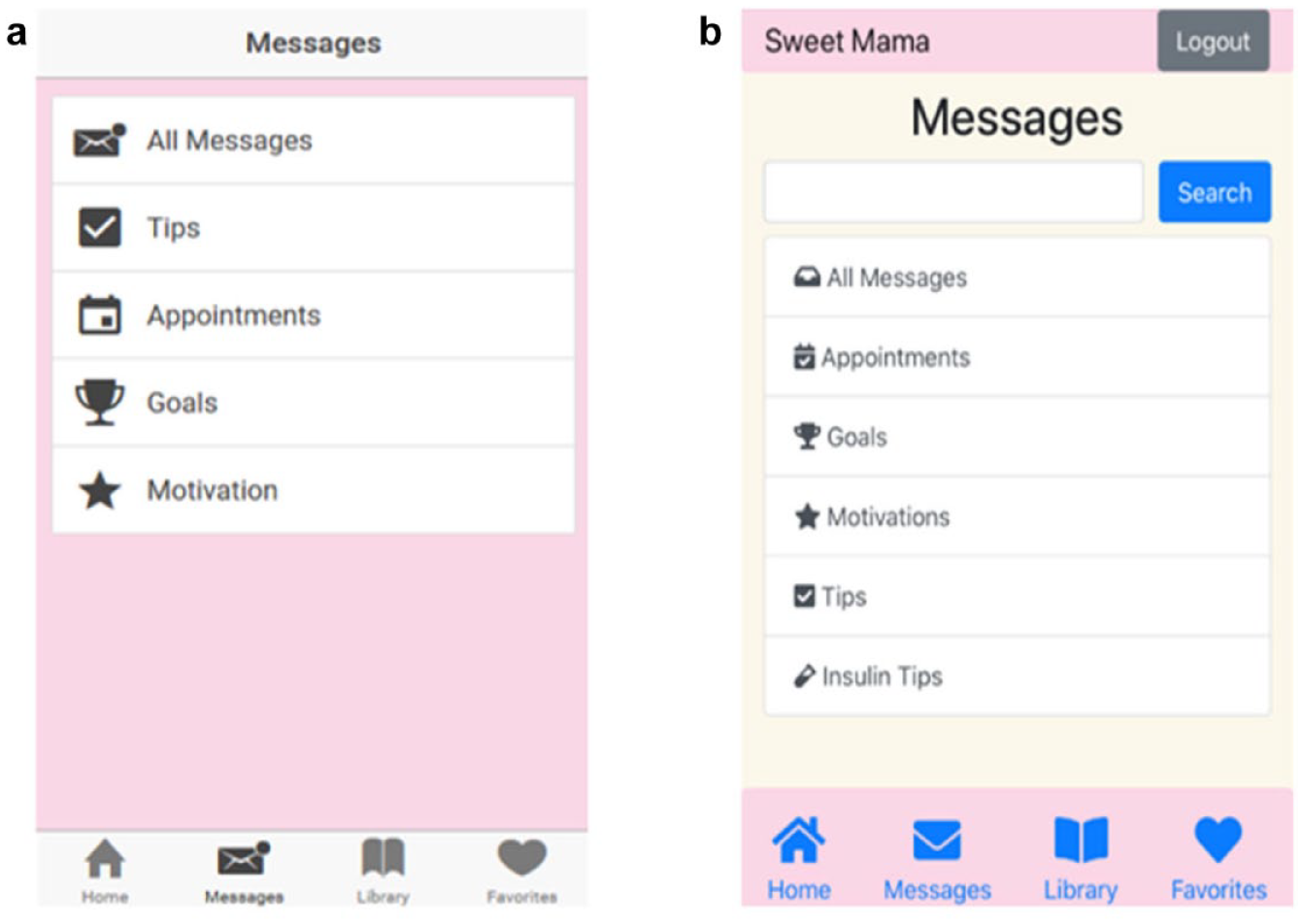
Example of early and current SweetMama message center home page.
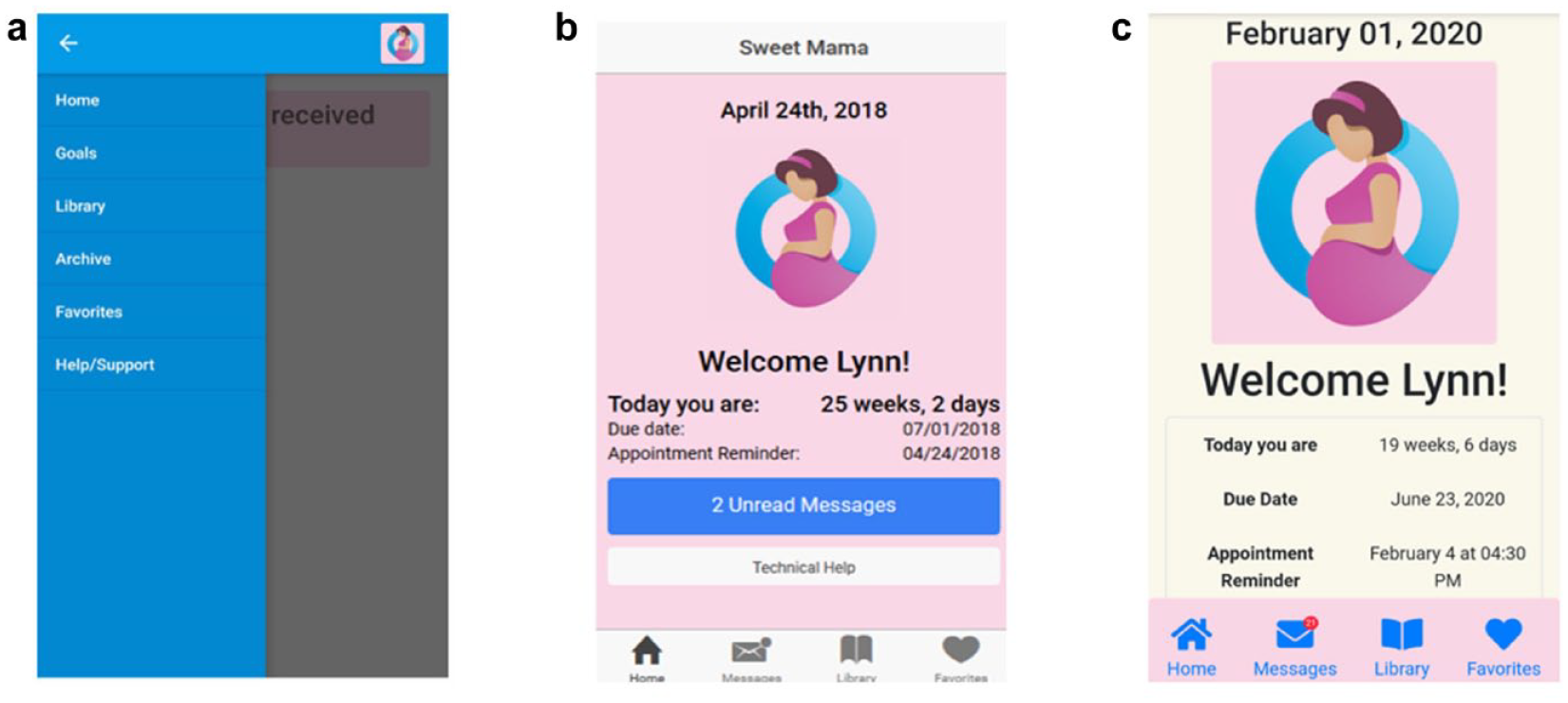
Progression of SweetMama home menu and home screen design.
Also based on early patient user requests, the versions of SweetMama experienced by later patient focus groups and all provider focus groups included a library component. The library consisted of: (1) trusted online educational materials from reputable sources such as the American Diabetes Association and other culturally tailored diabetes-specific resources, (2) clinic-based resources consisting of DM-focused handouts provided to patients in face-to-face care at this site, and (3) a recipe repository. While messages were used to convey quick tips and motivations, the library resources are intended for in-depth education. Users can “Favorite” preferred messages and library resources for later viewing.
Analysis
Interviews were professionally transcribed and uploaded to a secure, qualitative data-organizing platform (www.dedoose.com). Transcripts were analyzed using the constant comparative method.49,50 In this method, transcripts are read line-by-line and are coded for recurring concepts called subthemes. Trained research assistants independently coded transcripts and met regularly to review, negate, and modify subthemes, and eventually collapse subthemes into broad, overarching themes. Analysis was focused around the central goal of improving SweetMama to optimize the user experience before proceeding to subsequent stages of testing. We planned to undergo iterative thematic saturation analysis throughout the investigation in order to determine appropriate sample size. Recruitment of new participants ceased at saturation, or the point at which the dataset captured a wide range of responses, analyses of transcripts yielded redundant themes, and recruitment of additional participants would likely not yield novel results. Results presented below reflect the themes and subthemes in the context of their user type, stage of research, and the actions taken in response to the feedback.
Results
During the study period, 16 patients and 29 providers participated in focus groups (Table 1). Patients were largely non-Hispanic black (88%). Half had T2DM and half had GDM. Patient focus groups were discontinued after 16 participants were enrolled when thematic analysis demonstrated full saturation and provided sufficient information to move SweetMama development forward. In contrast, more than this number of healthcare provider interviews were required before saturation was reached due to the diversity of their perspectives. Providers largely identified as female and included a diverse range of professional backgrounds (Table 1).
Participant Demographic Characteristics.
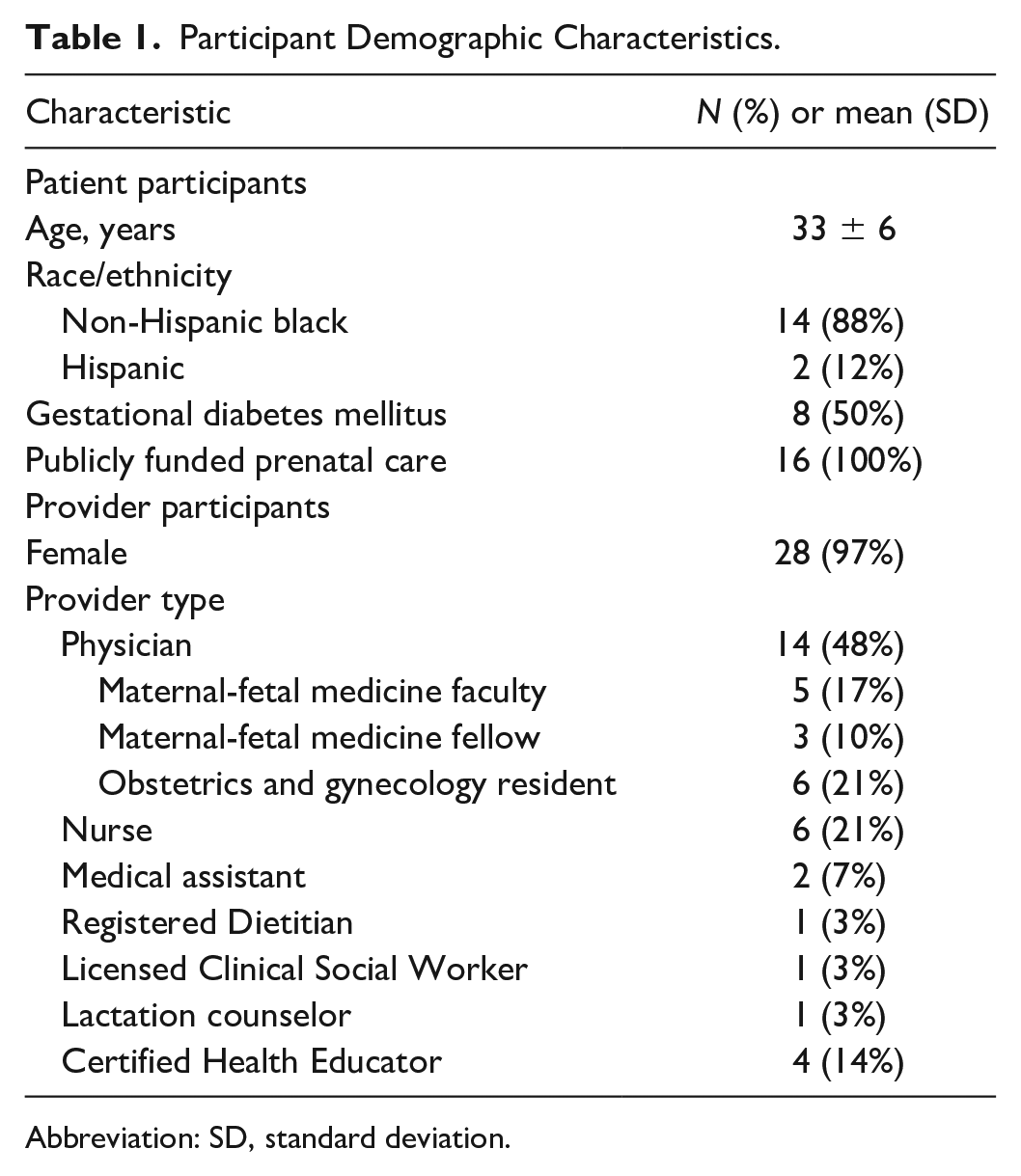
Abbreviation: SD, standard deviation.
Based on thematic analysis, data were organized into three overarching categories: positive feedback, negative feedback, and additional desired features for SweetMama. Within each category, we further organized data into themes based on whether they referred to visual features, information, or functional features. Each theme contained specific subthemes, described below.
Positive Feedback
First, participants expressed satisfaction with multiple SweetMama visual features, including personalization, aesthetic appeal, and content organization (Table 2). Regarding personalization, participants (N = 9 patients; N = 6 providers) viewing later versions (after SweetMama was modified based on early user feedback) liked the personalized home screen, which featured a welcome message with the user’s name, gestational age, and estimated due date (Figure 3b). The more developed home screen also included the patient’s next appointment (Figure 3c). Aesthetic appeal was also high; patient participants (N = 11) reported enjoying the SweetMama icon and the color scheme. Notably, patients enjoyed the pastel color theme, which was described as “fun” and reminiscent of “cotton candy.” Finally, a majority of patient participants (N = 11 patients) described liking the content organization, which included the separation of contents between tabs, the ability to see all messages on a single page, and the ability to navigate to each tab from the home screen.
Provider and Patient Positive Feedback on SweetMama.
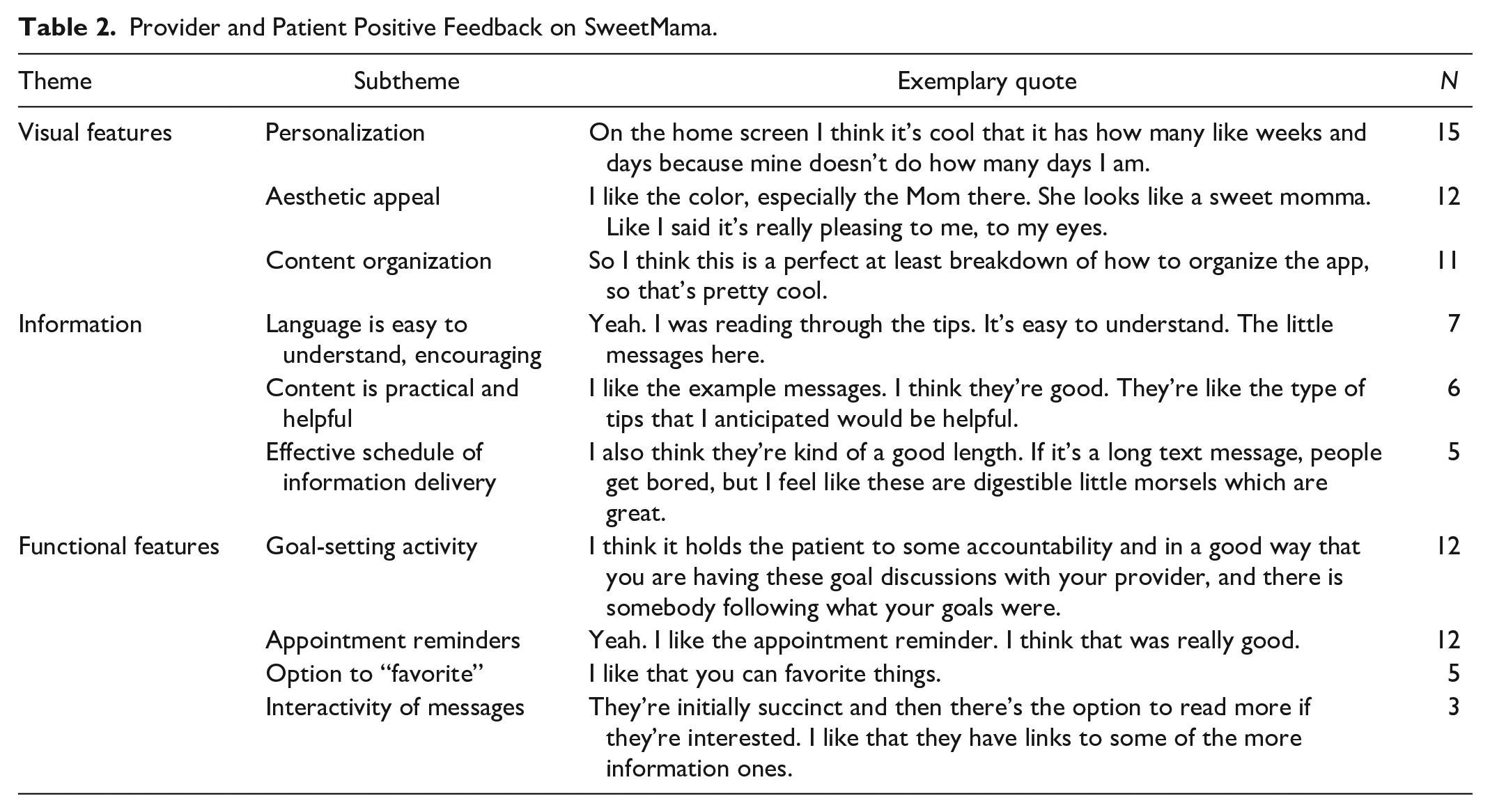
Second, both patients and providers expressed satisfaction with the information in SweetMama and its presentation (Table 2). Predominantly provider participants noted that the language used in goal and motivation messages was easy to understand and had a “positive” and “upbeat” tone. One provider commented on the lighthearted language of the messages, saying, “It’s. . .not like someone is trying to lecture you,” while a patient, after reading a motivational message, stated, “. . . that is what will be a little more helpful in the messages.” Another provider said, “I like the language you mentioned like, ‘I’m still working on this goal,’” language that was seen as having an encouraging effect on those who fell short of achieving their goal. Patient (N = 2) and provider (N = 4) participants also stated that the SweetMama content was practical and helpful. One resident physician said, “They all seemed really practical. . . they seem easy to integrate but also all things that I wanna know. And I really like how tailored ‘I would like more information’ stuff is to our clinic, to Chicago. . .” The schedule of information delivery was seen as an effective way to present information to users without being overwhelming or overly frequent. One provider said, “. . .these are coming in over time too so it’s not just a ton of information you get all at once. . .one tip at a time you actually can read the whole tip, digest it and then be ready for more information at a different time.”
Third, multiple functional features were favorably reviewed by participants. In particular, participants positively reviewed the app’s goal-setting activity, which patients (N = 4) and providers (N = 8) felt helped focus patients’ efforts during pregnancy. One provider stated, I think it helps to actually have [goals] written down because I think sometimes when you tell people stuff. . .they tend to glaze over after a while and it’s clear you’re just totally overwhelming them and so I think having something concrete and specific that they can do every week, I like that.
This sentiment was echoed by a patient, who said, “I like goals, period. It makes you challenge yourself and then it makes you look forward to what you got going on.” Participants also praised the appointment reminders feature that was added in response to prior feedback. Patient (N = 3) and provider (N = 2) participants viewed the option to “favorite” content favorably, which saves preferred materials in a designated folder and allows users to easily access the contents at a later time. Additionally, patient (N = 1) and provider (N = 2) participants mentioned the interactivity of messages, specifically the ability to view more content after the initial message or to favorite content, as being beneficial features.
Negative Feedback
Participant opinions of SweetMama’s shortcomings also encompassed themes of visual features, information, and functional features. Development of the app occurred concurrently with ongoing evaluation and many suggestions for improvement were addressed (Table 3) throughout the process of iterative app development. The majority of negative feedback came from providers.
Provider and Patient Negative Feedback on SweetMama and Subsequent Improvements.
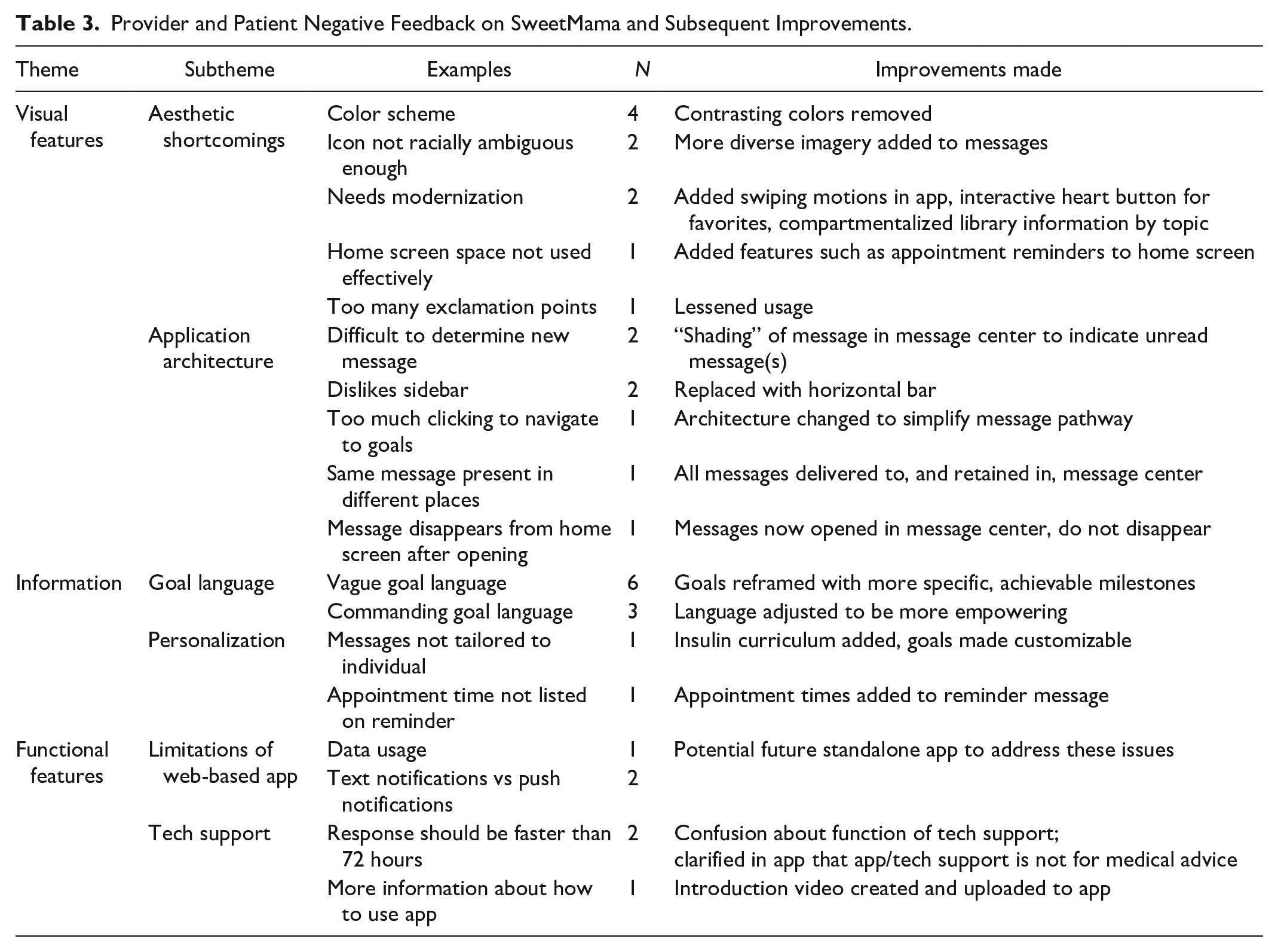
Early focus groups indicated that the app’s aesthetic features needed improvement. For example, one patient user viewed the original colors in the message notifications as “boring”; these colors were replaced with ones that complemented the color scheme selected by patient participants. Later, multiple providers (N = 3) commented on the pastel color scheme: “I feel a little weird about it being pink. . . it just seems weird that so many apps targeted toward women are pink and we like other colors too.” However, due to the almost entirely positive feedback regarding the color scheme from patient focus groups and because patient users had selected the colors, we opted to retain the color scheme. Providers (N = 2) also expressed concerns about the presentation of the SweetMama icon, a graphic profile of a pregnant person that used colors and shapes chosen to suit the topic and population (Figure 3c). Though the icon was designed to be racially ambiguous, providers were concerned that our objective may not have been achieved and that the icon could be refined to enhance application to a diverse group. However, patient participants did not comment on this issue. Additionally, later iterations of SweetMama featured improvements requested by users such as a modernized interface, more images, alterations in background colors, more effective use of the home screen via inclusion of appointment reminders, messages featuring more professional punctuation, and compartmentalized library information organized by topic.
Participants also suggested improvements to SweetMama’s application architecture. For example, two participants (N = 1 patient) stated that it was difficult to determine the most recently delivered message; in subsequent prototypes, messages were organized chronologically, message badges with the number of unread messages appeared in the message center and navigation bar, and new messages were shaded blue to indicate which ones were unread. Similarly, early patient participants expressed frustration with having to “click through” too many pages to view a message, seeing the same message on the home screen and in the message center, and having a message disappear from the home screen after interacting with it. These complaints were addressed by changing SweetMama’s message pathway; instead of delivering messages to the home screen, users navigate to the message center to view messages (Figure 2). After interacting with a message, it does not disappear (though it changes color to indicate it has been read) and users may navigate back to other screens.
Provider participants were critical of certain aspects of information presentation in SweetMama (Table 3). Although the overall goal concept was well received (see above), some providers (N = 6) felt that the goal language lacked specific, achievable goals. For example, one provider commented: [quoting goal message] ‘During my pregnancy I will try to maintain an active lifestyle to support diabetes control.’ It’s very broad and I would easily just put a checkmark by that at like week 12. . . I’m just saying. . . ‘I need to do 30 minutes of exercise three days a week’ [would be better].
Additionally, providers (N = 3) commented that the nature of some goal messages may be too harsh, saying, “To me it sounds like a little harsh to say [a statement such as], ‘During my pregnancy I will take my medication as prescribed.’ It seems a little cold or removed rather than saying, ‘My goal is to take my medication without missed doses’. . .”
Because provider focus groups were initiated later than patient focus groups, only providers, and not patients, viewed a more advanced SweetMama prototype containing specific goal messages. Upon review of the motivational curriculum, goal messages were revised to include specific goals with empowering language.
Other suggested areas of information weakness in the early stages of evaluation included the lack of personalization of information, specifically, the desire for messages that were tailored to the individual, information about the individual’s gestational age, and appointment reminders that included the appointment time. One patient stated, “. . . like with someone who is not on insulin how do you tailor that to just her specifically in the app and then for somebody like me who has been on insulin since the beginning.”
Improvements in personalization, such as the customized home screen containing specific appointment reminders, were reviewed positively in subsequent groups (discussed above). To address the desire for medically tailored information while balancing the need for a scalable intervention, we developed a set of 12 messages for women with an insulin regimen, which contains insulin-specific tips and motivations. This curriculum can be activated whenever the woman initiates insulin therapy.
Third, participants noted the limitations of SweetMama’s functionality. For example, one provider noted that users could incur excessive data charges when not using WiFi. Additionally, two patient participants commented on their preference for push notifications, as opposed to the text message-based notification system SweetMama currently uses. Participants also voiced qualms about SweetMama’s technological support. Two patient participants mistakenly assumed that the “Tech support” page within SweetMama extended to medical advice, despite the disclaimer that it did not, and desired a response. In subsequent versions, it was further clarified that technological support encompassed app problems only (Figure 4). Finally, in response to feedback (N = 1 patient) that not enough information was provided on how to use SweetMama and the team’s desire to create a streamlined introduction to SweetMama, we created an introduction video that plays when a user opens SweetMama for the first time and explains the app’s main features.
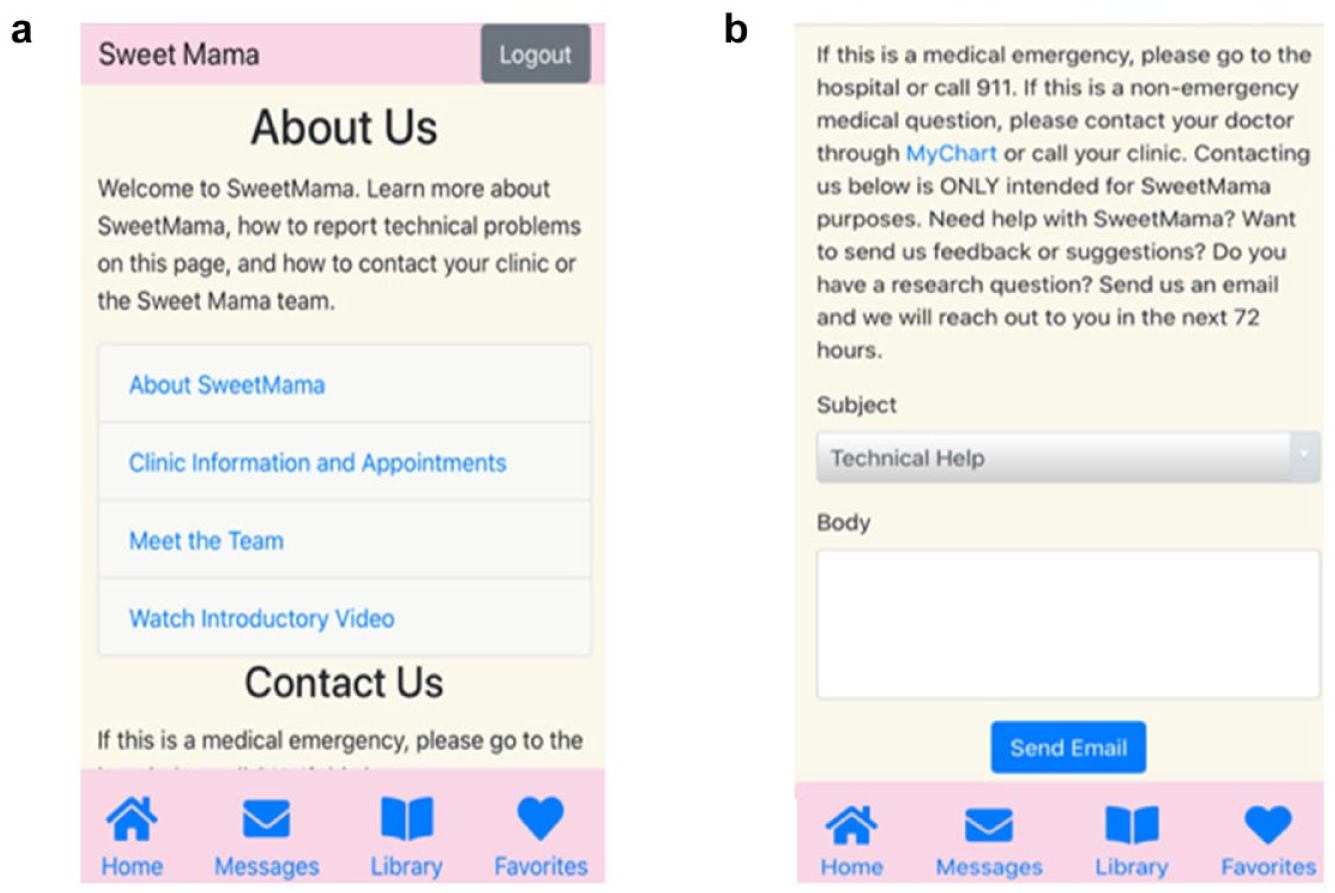
SweetMama “Contact us” page.
Additional Desired Features
Participants suggested additional novel features for SweetMama (Table 4). Multiple subthemes within visual improvements were identified; for example, both patient (N = 7) and provider (N = 3) participants desired a customizable homepage. This included being able to upload one’s own picture or ultrasound images or being able to create a customizable avatar to replace the SweetMama icon. Patients also desired the ability to customize the greeting on the home page with a specified baby name. Participants’ desire for customization included being able to control notification topics and frequency (N = 3 patients; N = 3 providers). One participant said, “I think that an ideal app would give you the option to decide what you want to be alerted for.” Participants also voiced their desire for a greater number, and improved quality, of graphics and videos within the app. Mostly provider participants desired the ability to “declutter” messages, that is, to delete or file them away according to topic after interacting with them.
Additional Desired SweetMama Features by Participant Type.
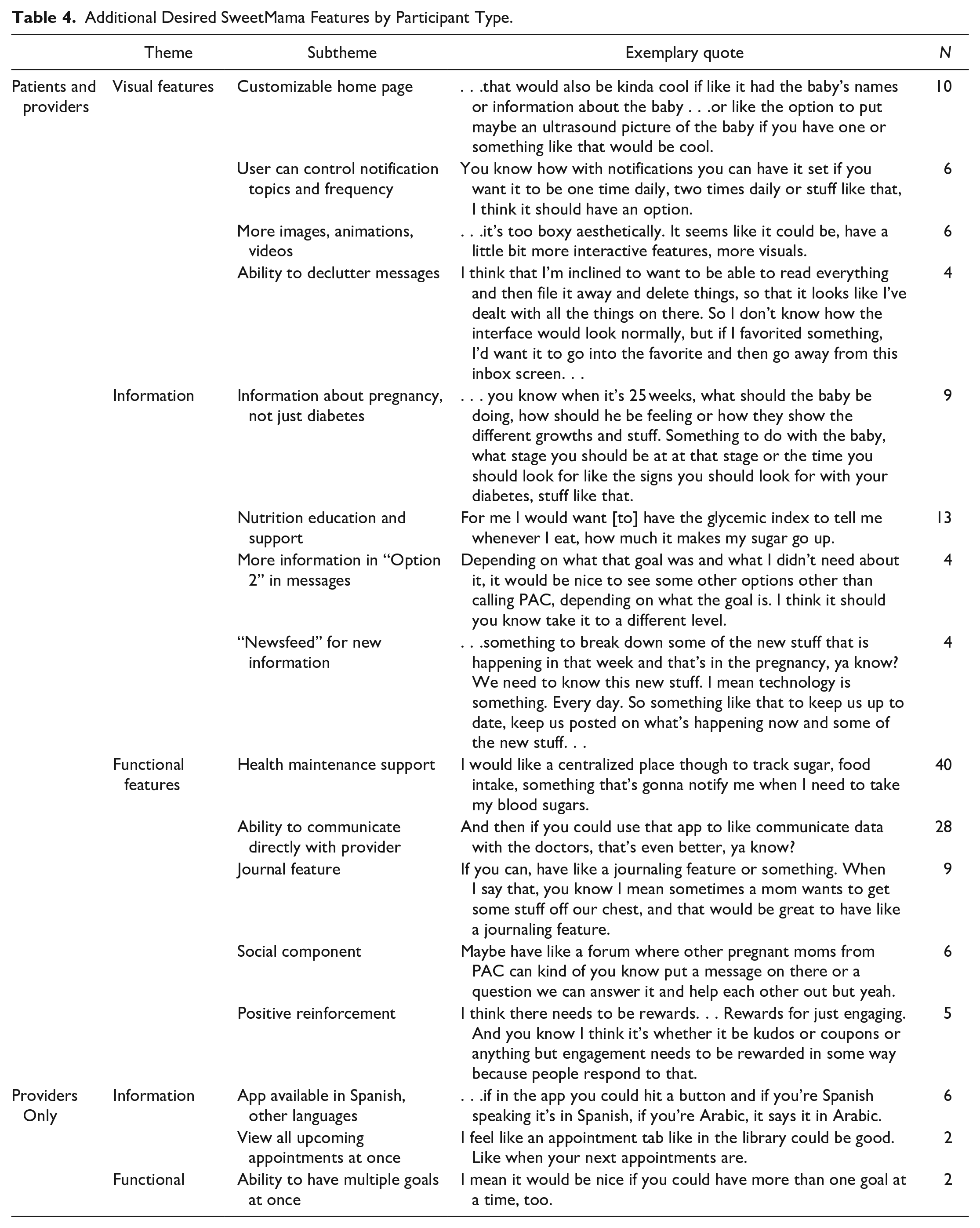
Second, suggestions related to SweetMama’s general and DM-specific pregnancy education information were made. Patient participants especially desired general pregnancy information in addition to the DM-focused health information and motivational messaging. One patient stated, . . .it needs more information pertaining to pregnancy. . . I’m 24 weeks and what should I expect at 24 weeks? . . . How big should the baby be? How should I be feeling? What are some of the things that studies show that a woman that’s a diabetic at 21 weeks pregnant, what should she be expecting or feeling like?
Participants (N = 6 patients; N = 7 providers) also desired nutrition education and support, for example, in the form of a glycemic index, suggestions of what to eat, and recipe support. One resident stated, Or just like a how would I use this [ingredient] if I’m going to the grocery store? I think when you tell people to buy fruits and vegetables, they’re like great, now what do I do with them? Like if you tell somebody to buy salad and kale and that is not incorporated in their diet . . . what the hell are you gonna do with the kale?
In addition, participants (N = 3 patients; N = 1 provider) voiced their desire for more specific information and targeted suggestions within the follow-up content area of tips, motivation, and goals messages. Some participants felt that certain content was not specific enough; for example, one patient said: So with this one, ‘Start a friendship with fiber’ tip message thing, it says ‘I would like more information,’ which is good, but I think this would be good to say okay, show me some recipes or something because . . . it’s like okay, well what can I make with beans?
Similarly, some patient participants desired a “newsfeed” within SweetMama that would display articles related to DM and pregnancy; it was perceived that this feature would help users remain current with DM information.
Finally, several functional features were desired. The most ubiquitous desire was for health maintenance support within the app. Both patients and providers envisioned a SweetMama feature where patients could log blood glucose readings, record insulin administrations, track meals and exercise, and set alarms and reminders. Some participants wanted SweetMama to display trends, such as graphical blood glucose results in conjunction with dietary information input. This desired feature was commonly described in tandem with the request to have the ability to communicate directly with providers; some participants wanted their health data to be accessible to providers, allowing providers to give personalized feedback to each patient. Interestingly, providers (N = 6) also desired such a feature but noted that it was time intensive and likely not feasible. Other patients desired a more automatic approach, that is, if a patient inputted a blood glucose level not within target, the system itself would provide tips accordingly. Participants desired this “all-in-one” functionality as it could ease the burden of daily DM tasks. Participants (N = 8 patients; N = 1 provider) also desired a feature within SweetMama that would act as a journal, which would allow patients to record their experiences, reasons for skipping meals, medication names, and/or what they ate during the day. Participants also desired a social component to share personal anecdotes, ask questions in a forum-like setting, and read others’ success stories regarding DM during pregnancy. Similarly, patients and providers recognized the importance of positive reinforcement in SweetMama. Though the app featured messages with strong words of encouragement, providers suggested gamifying certain aspects of the app, for example, with goal tallying, although patients did not request gamification.
Provider participants suggested additional improvements to SweetMama beyond those they had in common with patient participants. Encompassed by the theme of information, providers cited the urgent need for health materials and mobile apps to be available in Spanish and other languages. Providers also desired a way for patients to be able to view all of their appointments at once. Finally, some providers believed SweetMama should give patients the option of having multiple goals at once.
Discussion
Diabetes is the most common metabolic pregnancy complication and poses short- and long-term health risks to both the mother and fetus, and disproportionately affects low-income and minority women.8,9 Pregnancy is also a critical window for improving women’s long-term health 51 ; thus, improving DM skills and outcomes during pregnancy may confer lifelong benefits. Yet, managing DM during pregnancy requires complex skills and greater engagement, motivation, and action than outside of pregnancy, placing burdens on women with lower health literacy or fewer resources.25,26,52 Patient-centered behavioral interventions designed to support pregnant women with DM are limited. For this reason, we developed SweetMama, which was designed to enhance self-efficacy, health literacy, and patient engagement, while also supporting barrier reduction in this high-risk population.
In the present study, we conducted patient and provider focus groups over a period of 15 months in order to gather feedback on our novel mHealth intervention. Participants approved of visual features such as the application’s aesthetic appeal, customizable features, and intuitive content organization. Participants valued SweetMama’s accessible language, practical content, and manageable content delivery schedule. Participants also approved of SweetMama’s goal-setting activity and appointment reminders, as well as its user-friendly interface, ability to interact with messages, and ability to select favorites. Despite these positive reviews, participants were critical of some features, including certain aesthetic shortcomings and organizational features that were resolved with more streamlined prototypes. Participants also noted vague goal language, messages that could be more customized, and the limitations of a web-based app. While there was much concordance between patients’ and providers’ preferences, suggestions were not always identical between groups; however, addressing both patient and provider viewpoints allowed the SweetMama team to consider all aspects of the application’s design. Most importantly, participants offered suggestions on improving the app, guiding its future development.
Other studies have utilized patient and/or provider feedback to ensure user-centered design for applications made for users with DM, though few have focused on pregnancy. Though most of these applications primarily aimed to provide blood glucose tracking support, many participant responses remain relevant to the development of SweetMama. A Norwegian group developing a GDM app, Pregnant+, identified the importance of an easy and intuitive interface, 53 a commonly praised feature of SweetMama. However, the application lacks the active, regular delivery of motivational content, does not have customization options for women requiring insulin, and requires users to input appointments manually—all of which are popular SweetMama features. In assessment of the Pregnant+ app, women with GDM appreciated the availability of reliable information in the app; in our study, women also desired more information with greater detail. 54 Some Pregnant+ participants reported being discouraged by viewing negative blood glucose trends within the app, underscoring the importance of delivering motivational content in SweetMama. Another app, GDm-Health, was designed to facilitate blood glucose monitoring management and real-time provider review of these data and demonstrates promising findings; however, this application similarly lacked the regular delivery of motivational and literacy-matched education materials—a critical gap in our patient population.55,56 Theis et al analyzed the failed adoption of an app intended to support management of DM in a nonpregnant population, in which patient and provider interviews revealed the poor adoption was due to clinical providers having to toggle between internal and external platforms during patient visits, an unreimbursed activity that took time away from the provision of healthcare. 57 These data support the self-contained structure of SweetMama, which requires minimal provider interactivity aside from routine goal setting and does not ask providers to monitor or communicate with patients via SweetMama. Participants in the Theis et al study also reported being initially confused by the app because of inadequate orientation, which was also noted in our data and supports our creation of an introduction video.
Though some patient participants voiced their desire for SweetMama to include basic health maintenance support tools, such as blood glucose and fitness trackers, our team opted against implementing such features due to redundancy with existing technology. With the advent of downloadable blood glucose meters with smartscreen capabilities, well-developed and free commercial nutrition tracking apps, and Android/iPhone-native step counters, as well as a mobile app for the electronic health record patient portal, our team’s focus remained on addressing the unmet need for education and motivation for lifestyle behavior change in this population and less on creating a “do-all” mobile app that replicates existing technology. However, recognizing the need to curate web-based information for a low health literacy population and for the specific needs of low-income users, SweetMama content in the latest iteration does include reputable resources that assist with DM-specific health maintenance needs.
One design strength of this study was its iterative input from both patients and providers. By focusing on the target population, we ensured a user-centered design and identified feature improvements that may be particularly important to this population. Not only do no other pregnancy and DM mHealth applications specifically designed for low-income women exist, but SweetMama was also rooted in strong conceptual frameworks and evidence for health behavior support. Additionally, by including providers with a wide range of professional backgrounds, we were able to consider various issues that may have been apparent to some provider types and not others. However, a weakness in this study is its inclusion of participants from a single medical center, which may limit generalizability. Importantly, this study was limited to English-speaking women, and thus the majority of the patient population was non-Hispanic black; future work needs to be performed to incorporate the perspectives of Hispanic women. Additional limitations of our approach include the inherent drawbacks of the “Think Aloud” methodology; for example, few providers commented on the aesthetic appeal subtheme, yet the lack of comment does not necessarily indicate negative opinions, but may instead simply indicate the absence of an overt query. Finally, the sequential nature of investigation means that an additional limitation is that patients did not experience the most up-to-date version of SweetMama, and patients and providers did not participate in combined focus groups; however, we feel this limitation is acceptable given the importance of incorporating user perspectives in an iterative fashion, and future work will continue to focus on patient perspectives.
Future work by the SweetMama development team will continue addressing numerous participant requests, for example, more images, information, customization, and positive reinforcement. Building on provider feedback that SweetMama was user-friendly, the SweetMama team will continue investigating acceptability and usability of more advanced SweetMama prototypes. The iterative development process that occurred in this phase was essential to creating a user-friendly, efficient app that will have a greater chance of diverse patient engagement and use. Next steps include both longitudinal usability testing and subsequent feasibility trials. A future randomized controlled trial of the SweetMama app in clinical settings will determine the efficacy of supportive, longitudinal continued education and motivation to sustain lifestyle behavior change for DM via SweetMama to improve perinatal outcomes.
Conclusion
SweetMama, a novel educational and motivational mHealth tool for pregnancy with diabetes, was perceived to be a helpful and user-friendly educational tool by low-income women during a two-week usability trial. Future work will address SweetMama’s longitudinal utility in improving perinatal outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LMY was supported by the NICHD K12 HD050121-11 at the time of the study. Additionally, this work was supported by the NICHD 1R21 HD094271-01 and the Friends of Prentice Grants Initiative (FY2019). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This work was also supported by the Northwestern University Academic Year Undergraduate Research Grant (2018-2019) to KL.