
Abstract
Background:
Of adults with type 2 diabetes, 84% take antihyperglycemic medication. Successful treatment requires active monitoring and medication dose adjustment by health providers. The objective of this study was to determine how a mobile-phone-based coaching system for diabetes management influences physician prescribing behavior.
Method:
This secondary data analysis is based on a cluster randomized clinical trial that reported patients provided with mobile self-management had reduction in glycated hemoglobin (HbA1c) of 1.9% over 1 year, compared to 0.7% in control patients (P < .001). Participants were primary care patients with type 2 diabetes randomized at physician practice level into a control group (n = 55) and intervention group (n = 62). Main study measures were patients’ medication records (medication, dose, frequency, start and end date) abstracted at baseline and study end. Antihyperglycemic medications, including sulfonylureas or thiazolidinediones, and antihypertensive and antilipemic medications were analyzed.
Results:
A higher percentage of patients in the intervention group had modification and intensification of incretin mimetics during the 1-year study period (9.7% vs 0.0% and 8.1% vs 0.0%, both P = .008). A higher percentage of patients in the intervention group had modification and intensification of metformin (24.2% vs 7.3%, P = .033). The overall difference in physician prescribing of oral antihyperglycemic medications was not statistically significant.
Conclusions:
Our results suggest mobile diabetes interventions can encourage physicians to modify and intensify antihyperglycemic medications in patients with type 2 diabetes. Differences in physician prescribing behavior were modest, and do not appear to be large enough to explain a 1.2% decrease in HbA1c.
Of adults with diagnosed type 2 diabetes, 84% take insulin or oral antihyperglycemic medication. 1 Successful treatment requires active monitoring and medication dose adjustment by health care providers. Despite evidence that punctilious medication management can lead to improved glycemic control and prevent microvascular complications in patients with diabetes,2-6 there is often a delay in medication initiation or intensification by providers.7,8 Interventions that enhance the management of diabetic hyperglycemia could lead to improved health outcomes. 9
One challenge in the successful co-management of diabetes by the patient and provider is the sharing of information, including information about medications and changes in the patient’s glucose values and self-care behaviors. Since higher levels of communication competence are associated with improved glycemic control, 10 it is important that patients and providers share information more effectively. One new, convenient mode of communication is via mobile phones.
Mobile phones are increasingly used to provide behavioral interventions in health care.11,12 They have been used to facilitate smoking cessation13,14 and weight loss, 15 increase physical activity, 16 and manage specific diseases, particularly diabetes.17-19 Mobile phones are attractive for delivery of health care because of their widespread use across socioeconomic groups and their technical capabilities, including text messaging, Internet access, applications, and the ability to connect to sensing devices. Many individuals carry mobile phones everywhere, allowing mobile phone health interventions to be an integral part of the individual’s routine.
Data from the Mobile Diabetes Intervention Study show that patients provided with a mobile self-management coaching system and provider decision support had a reduction in glycated hemoglobin (HbA1c) of 1.9% over 1 year, compared to 0.7% in patients who did not receive these interventions (P < .001). 20 The coaching system involved patients using mobile phones to record information about their diabetes self-management. Patients received real-time (automatic) and personalized coaching feedback consistent with their treatment plans. Physicians could review patient-recorded data accessible through the provider Internet portal and received quarterly facsimile reports that included diabetes treatment recommendations. Since medication management is a key component of diabetes care, the goal of the present study was to investigate the effect of this coaching system on physician prescribing behavior.
Method
Study Overview
Detailed descriptions of the Mobile Diabetes Intervention Study design have been previously reported.20,21 Secondary analyses presented here were specified a priori in the protocol.
Patients
Patients were considered eligible for the study if they had type 2 diabetes that had been diagnosed by a physician at least 6 months prior to enrollment in the study, had an HbA1c level ≥ 7.5% within the past 3 months, and were 18 to 64 years old.
Patients were considered ineligible for the study if they were beneficiaries of Medicare or Medicaid, had no health insurance, used an insulin pump, were pregnant, had actively abused substances, including alcohol and drugs, within the past year, sought treatment for psychosis or schizophrenia, had uncorrected, severe impairment in hearing or vision, did not have an email address or access to the Internet.
Patients with type 2 diabetes were recruited into the Mobile Diabetes Intervention Study as previously reported. 21 Each patient was randomized at the physician practice level to 1 of 4 groups: the usual care group (n = 56), the coach only group (n = 23); the coach-primary care provider (PCP)-portal group (n = 22), or the coach-PCP-portal with decision support group (n = 62). We used data from the usual care (henceforth “control”) and decision support (henceforth “intervention”) groups for the current analysis, excluding the coach only and coach-PCP-portal groups from the analysis because they were prespecified as ancillary in the study design. 21 One patient from the control group was excluded from the analysis because medications were not recorded at baseline. Therefore, for this analysis, the control group n = 55.
The following baseline characteristics of patients were collected: demographics, health history, diabetes health status, current medications, risk factors for complications of poorly controlled diabetes, and self-management and lifestyle activities (exercise, eating behavior, glucose monitoring). Descriptions of prescribed medications were abstracted from the medical chart. All patients in the study received a One Touch Ultra 2™ glucose meter and a 1-year supply of blood glucose testing materials. 21
Patients in the control group were cared for as usual. This care included their physicians reviewing their blood glucose meter readings and blood glucose logbooks, when the patients made these records available, 21 and providing care accordingly.
Intervention
Patients in the intervention group received an intervention consisting of 3 components. The first component was diabetes management by the patient, using a mobile phone to communicate information and receiving real-time (automatic) or personalized coaching feedback. Patients selected 1 of 2 mobile phone models, a 1-year unlimited mobile phone data and service plan, and coaching software on their mobile phones. Using the software, patients entered into their mobile phones their blood glucose levels, carbohydrates consumed, diabetes medications taken, and any comments about their diabetes self-care, all of which were recorded in real time in a web-based logbook. They received messages containing feedback based on the data they had entered, trends in recently entered data, and their physicians’ individualized medication instructions. 21
The second component of the intervention was that their physicians had access to a HIPPA-compliant, password-protected web portal containing the patients’ logbooks of unanalyzed data. The physicians received training on how to use this web portal. 21
The third component was that physicians received via facsimile or email quarterly (or, if necessary, more frequently) reports on patient-entered data, generated by automated, proprietary analytical models. Each report summarized the patient’s glycemic and metabolic profile (eg, blood pressure and lipids), self-management skills, adherence to prescribed medication, and other aspects of health care, such as vaccinations and eye examinations. The report also contained individualized recommendations for medication regimens, based on patient-entered data 21 and evidence-based care guidelines of professional organizations.22-24
Physicians
Physicians practicing primary care, family practice, or internal medicine were recruited from four regions of Maryland, including urban, suburban, and rural settings. Physicians practicing in academic institutions were not included in the study to keep the intervention congruent with care in the community. All physicians at a particular practice were randomized to the same study group, to avoid contaminating the study intervention. 21 Randomization of practices occurred after agreement to enroll in the study to avoid bias in recruiting practices more likely to carry out health behavior change in the intervention practices. Study patients followed the randomization assignment of their enrolled physician.
The following baseline characteristics of physicians were collected: demographics, years in practice, and descriptions of their practice. 21
Physicians in the intervention group were informed that their patients received a mobile phone preloaded with the Diabetes Manager™. 21 All physicians in both groups received the American Diabetes Association (ADA) guidelines for diabetes care23,24 and were reimbursed $250 per enrolled patient for work performed by their practices in the study. 21
Medications and Physician Prescribing Behavior
Medication records from patients’ charts at the primary care site were abstracted at baseline and at the end of the study. Information included medication name, dose, frequency, start date, end date, and any dose change during the study period. Subsequently, all antihyperglycemic, antihypertensive, and antilipemic medications for each patient were individually analyzed by an endocrinology fellow (PLS). The antihyperglycemic medications were further separated into the following subclasses: sulfonylureas, thiazolidinediones, metformin, incretin mimetics, DPP4 inhibitors, and insulin (mealtime and basal).
For each patient’s class or subclass of medication, the following descriptions for physician prescribing behavior were applied: preexisting (entered study on medication at baseline), added, stopped, dose increased, or dose decreased. Afterward, these descriptions were summarized into two outcomes: any modification (vs none) and intensification (medication added and/or dose increased) within the medication class (vs no intensification). Intensification is a subset of any modification. For each of the drug classes, the number of patients who had medications decreased or stopped was very small. For the analysis we chose to look at any modification or intensification.
Patient data were analyzed according to the original cluster-randomized assignment of physician practices (ie, intention-to-treat analyses were performed). Important to this study, physicians and patients were not required to have experience using technology (patients needed to have access to the Internet or email).
Study Oversight
The Institutional Review Board of the University of Maryland Baltimore approved this study. A Data and Safety Monitoring Board was appointed to review the study procedures and adverse events. After study enrollment was closed, errors in consent form completion were found on audit. To ensure that we obtained the appropriate signatures, the Institutional Review Board asked us to repeat our consent procedures, which we did for 163 patient participants and all 39 physician participants. We were unable to contact patients not reconsented. They did not significantly differ (P > .10) at baseline from included patients in age, gender, or baseline HbA1c.
Statistical Analyses
We calculated the following descriptive statistics for patient-, practice-, and physician-level variables: means and standard deviations for continuous variables, and frequencies and proportions for categorical variables. Differences in demographic data between groups were analyzed using Fisher’s exact test, in the case of categorical variables, and t tests, in the case of continuous variables. Differences between the groups’ prescription behavior were calculated using a generalized linear mixed model that included practice level clustering. Certain medication analyses had very sparse cell sizes. Due to sparse data for some outcomes, the analyses were run at a practice level instead of at the patient level. These Wilcoxon rank-sum analyses rank order practices by the proportion of their patients with versus without a change/intensification of the specified medication to draw inferences, instead of drawing inferences from direct patient counts. For these variables, a practice-level Wilcoxon rank-sum test was utilized to account for practice clustering. 25 All tests were unadjusted for baseline medication usage. SAS 9.2 (SAS Institute, Cary, NC) was used to perform all statistical analyses. P < .05 was considered statistically significant.
Results
The baseline characteristics of study patients are shown in Table 1. Two statistically significant differences out of 20 comparisons between the groups were found. Patients from the control group had an average HbA1c of 9.1%, compared to 9.9% in the intervention group (P = .025). Also noted was a different distribution of smoking status between the intervention and control groups (P = .032). The control group had a higher proportion of current smokers than the intervention (20.0% vs 12.9%), but the intervention group had a higher proportion of former smokers (14.5% vs 1.8%). Since the patients from the 2 groups were treated by different providers, we evaluated the baseline characteristics of physicians and practices, as shown in Tables 2 and 3. There was one statistically significant difference of 11 comparisons. The control practices had a higher percentage of male physicians (90.9% vs 36.4%, P = .023). Physicians assigned to the intervention group were younger, spent fewer hours in clinic per week, and had fewer years of experiences, but these differences were not statistically significant. There were no physician dropouts after training on use of the physician web portal, which contained study participant blood glucose logs and patient self-reported information.
Baseline Characteristics of Patients.
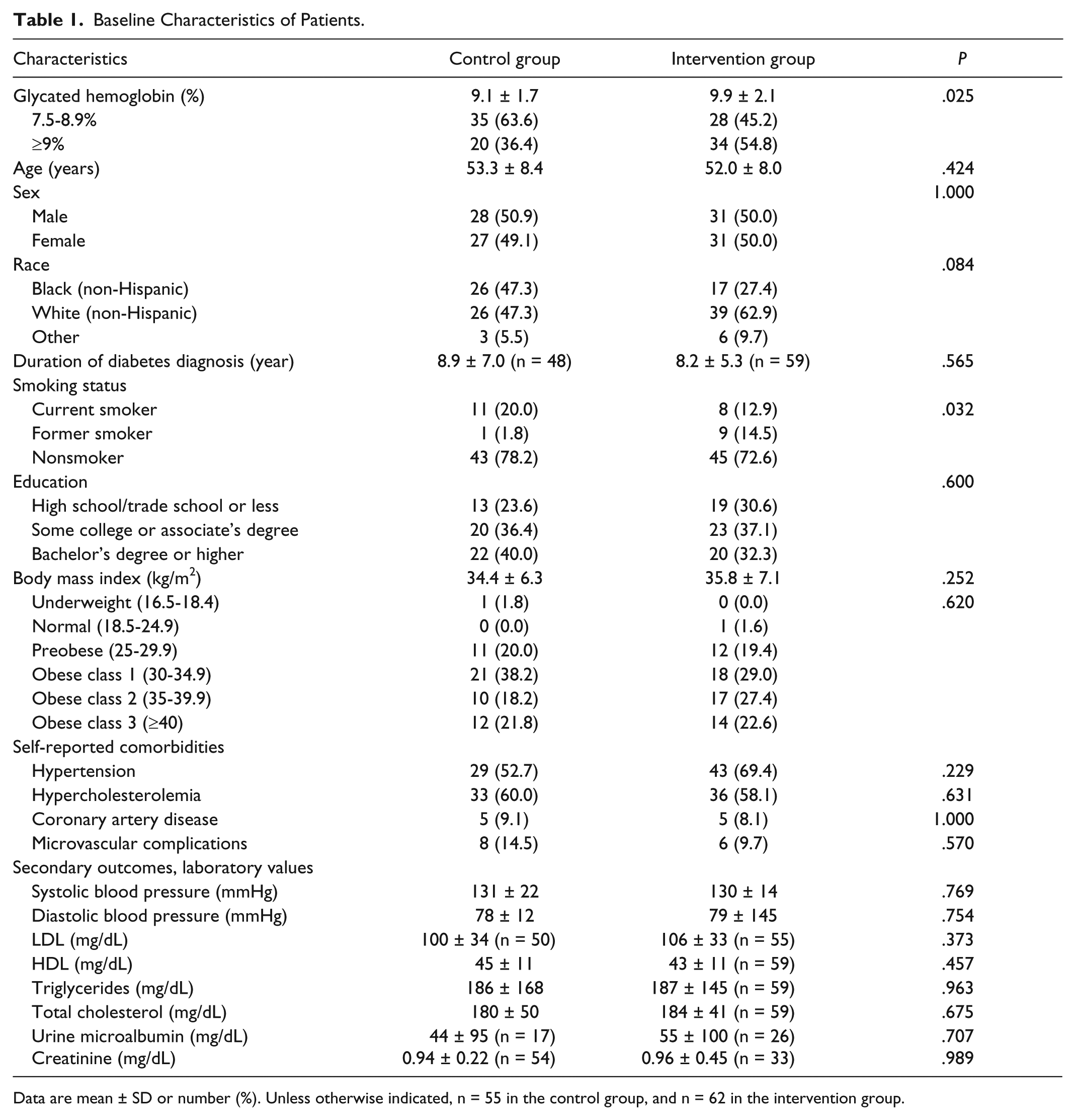
Data are mean ± SD or number (%). Unless otherwise indicated, n = 55 in the control group, and n = 62 in the intervention group.
Baseline Characteristics of Physicians.
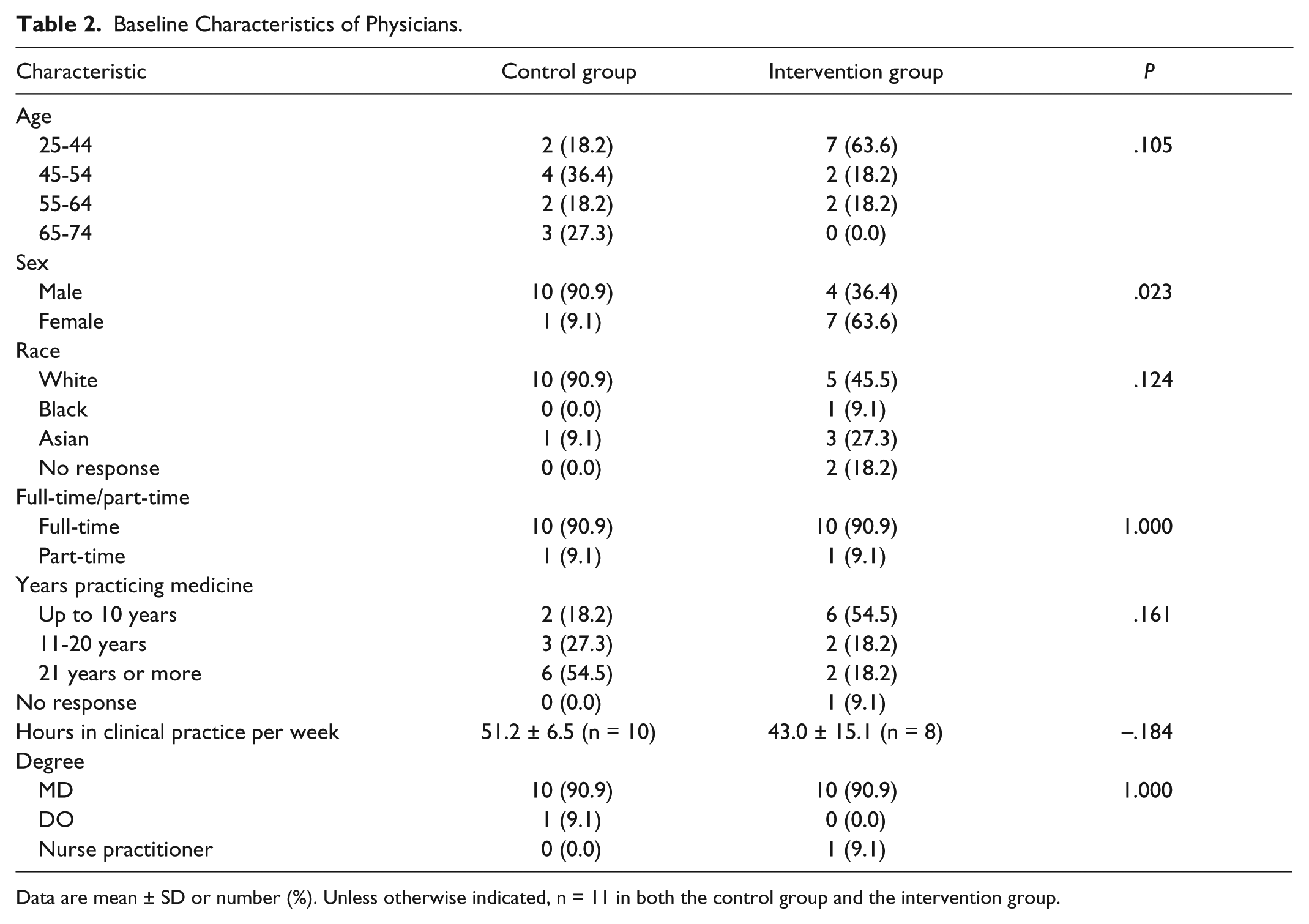
Data are mean ± SD or number (%). Unless otherwise indicated, n = 11 in both the control group and the intervention group.
Baseline Characteristics of Practices.
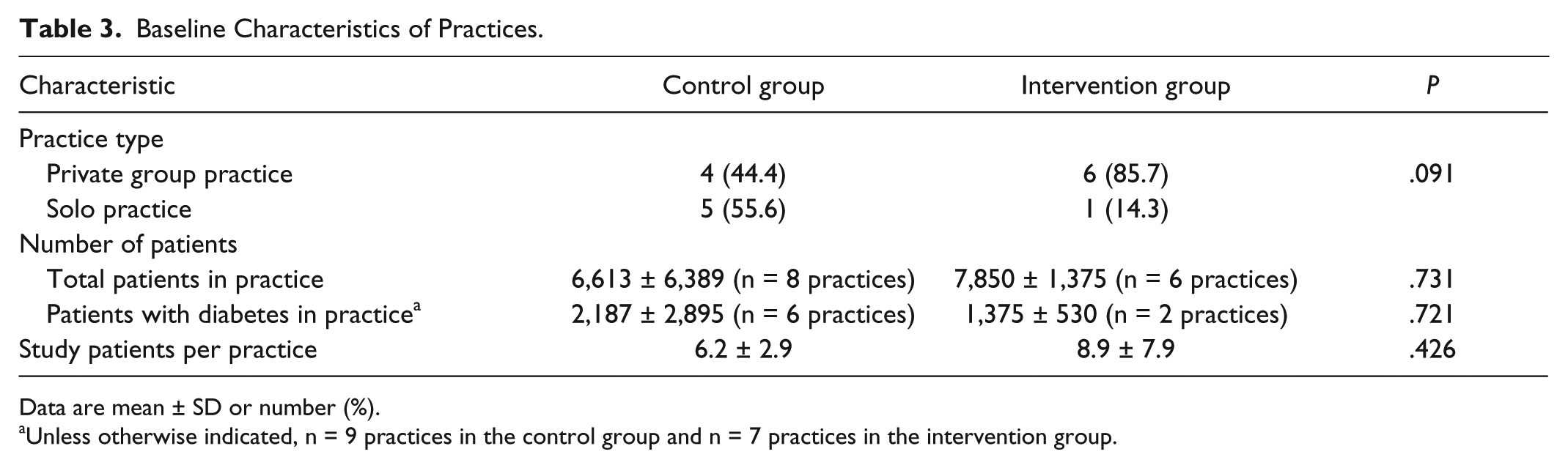
Data are mean ± SD or number (%).
Unless otherwise indicated, n = 9 practices in the control group and n = 7 practices in the intervention group.
Table 4 compares the prescription behavior between the groups for each class of medications. Nearly all patients included in the analysis were on antihyperglycemic medications at the start of the study. Although not statistically significant, a majority of patients in the intervention group had modifications to their medications versus a minority in the control group during the study period (56.5% vs 36.4%, P = .121), modifications in insulin and/or oral antihyperglycemics (46.8% vs 27.3%, P = .094), and intensification of oral antihyperglycemics (37.1% vs 16.4%, P = .053).
Prescription Medications.
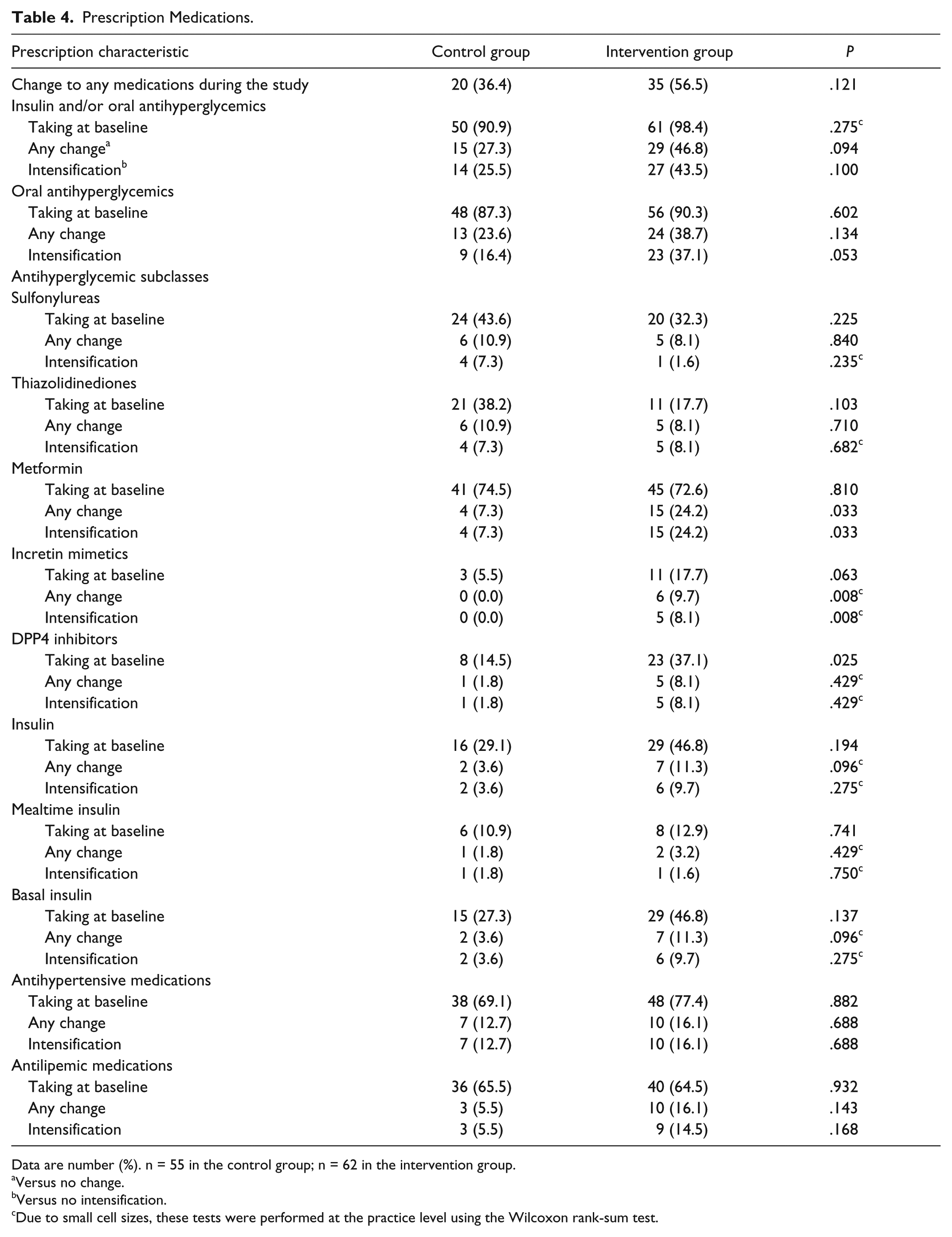
Data are number (%). n = 55 in the control group; n = 62 in the intervention group.
Versus no change.
Versus no intensification.
Due to small cell sizes, these tests were performed at the practice level using the Wilcoxon rank-sum test.
A higher percentage of patients in the intervention group than in the control group had intensification of metformin (24.2% vs 7.3%, P = .033). A higher percentage of patients in the intervention group had modifications and intensifications in incretin mimetics (9.7% vs 0.0%, P = .008, and 8.1% vs 0.0%, P = .008 respectively). There were no statistically significant differences between the groups in the percentages of patients with modifications or intensifications of sulfonylureas, thiazolidinediones, DPP4 inhibitors, or insulin. It is important to note that liraglutide was not on the market during the study period (FDA approved January, 2010), and no study patients were prescribed liraglutide. There were also no appreciable differences in the percentages of patients with modifications of or intensification of antihypertensive or antilipemic medications. The primary study reported no significant difference in blood pressure or lipids between the two study groups. 20
An intensification of medication resulting in improved HbA1c may result in increased frequency and severity of hypoglycemia. Hypoglycemic events, hospitalizations, and emergency room visits were infrequent in all groups.
Discussion
To our knowledge, this is the first randomized study of a mobile diabetes intervention that links patient communications with physician actions. Our study is one of the first to describe physician prescribing behavior for mobile diabetes management. Medication intensification was not the only such behavior that we examined; we also examined whether a particular medication had been stopped or a dose had been decreased. Nevertheless, the main differences in prescription behavior between the two groups were intensification related: a higher percentage of patients in the intervention group than in the control group had intensification of oral antihyperglycemic medications, metformin therapy most often.
Both metformin therapy and intensification of antihyperglycemic medications are part of the standard of care for treating hyperglycemia in type 2 diabetes patients. The ADA and the European Association for the Study of Diabetes recommend that patients start metformin therapy and lifestyle changes (eg, exercise) at the time of diagnosis, and that their medication be periodically intensified to achieve optimal glycemic control (HbA1c < 7% for most patients).23,26 In a 2009 study, intensification of oral antihyperglycemic medications or insulin did in fact significantly improve glycemic control, by 0.49% HbA1c. 27
Despite the benefits of intensifying medications in patients with type 2 diabetes, physicians often fail to do so.7,8 For example, in one study, only 40.4% of patients with high HbA1c levels underwent changes in their medication regimens. 7 In another study, less than half of such patients underwent medication intensification, regardless of physician specialty. 28 Our results suggest that the mobile diabetes intervention may be a way to encourage physicians to intensify antihyperglycemic medications in patients with type 2 diabetes. Furthermore, our analysis provides a framework for evaluating commonly prescribed antihyperglycemic medications over a 1-year period.
One of the subclasses of antihyperglycemic medications that we studied was thiazolidinediones (TZDs). In 2007, a safety alert was issued for 1 type of TZD, rosiglitazone, leading to this drug being discontinued among 53.5% of users and another TZD, pioglitazone, being discontinued among 21.4% of users, according to a 2011 study. 29 We did not see any differences between the 2 treatment groups in terms of changes in TZD prescriptions; the safety alerts either did not affect whether the study physicians prescribed TZDs or affected both groups similarly.
Another subclass of antihyperglycemics that we studied, incretin mimetics, was used by a higher percentage of patients in the intervention group than in the control group at baseline (17.7% vs 5.5%, P = .063). Furthermore, modifications to and intensifications of incretin mimetics prescriptions occurred in a significantly higher percentage of patients in the intervention group than in the control group (9.7% vs 0%, P = .008). These differences may have been due to the fact that physicians in the intervention group tended to be younger. Younger physicians may be more inclined to prescribe incretin mimetics, a newly available pharmaceutical.
We reported previously that the mobile phone-based intervention improved HbA1c levels by 1.9% in 1 year, while usual care only improved them by 0.7%. 20 We aimed to assess the effect of the intervention on physician prescribing practices because previous research has shown that medication-based management of diabetes relates to lower HbA1c.5,6 Changes in medication are only one hypothesized mechanism through which the mobile diabetes intervention may have reduced HbA1c. Other possible mechanisms include lifestyle guidance and self-management support.
One reason we undertook the analysis in the present study was to determine whether medication changes explained the improvement in HbA1c. The overall difference in physician prescribing of oral antihyperglycemic medications was not statistically significant between the two groups. However, we found that metformin and incretin mimetics prescribing were significantly higher in the intervention group than the usual care group. The estimated differences were modest and do not appear to be large enough to explain a 1.2% decrease in HbA1c. Hence, replication of these findings is warranted.
We advise caution in generalizing our results. This study was not powered to detect changes in physician prescribing behavior, and small group size was a limitation. Generalizability is limited to commercially insured persons. In addition, we did not attempt to record patient adherence to prescribed medications. Patients play a critical role in the choice to adhere to medications. Patients may be influenced by a view of medication initiation as evidence of personal failure, or medication intensification as related to risk for diabetes-related complications. 30 Actual changes to insulin dosing may not be completely reflected in medical chart abstraction. Even with electronic medical records, documentation of actual insulin self-dose (based on physician suggestion) may not exist in the medical record. Patients also play a critical role in choices of lifestyles by, for example, exercising, eating well, and learning about and implementing other ways of self-managing their diabetes. 31 When patients choose lifestyle improvements favorable to their diabetes, outcomes may not require medication intensification. Mobile technology, such as that used for the intervention in our study, may help patients work more closely with providers on self-care behaviors in addition to medication changes.
Conclusions
Our study underscores the key role of patient–physician communication. The results suggest that mobile communication may be effective in improving a physician’s access to both information and support for decision making regarding treatment changes. The results also suggest that more timely feedback to providers prescribing medications may improve short-term diabetes outcomes, such as HbA1c levels. We are currently studying what specific messages and feedback improve engagement and communication between patients and their physicians. Future work will examine effectiveness of the mobile phone intervention in other populations, including older adults.
Footnotes
Acknowledgements
We thank Michelle Jones, PhD, ELS, for her assistance in writing and editing this article.
Abbreviations
ADA, American Diabetes Association; DPP4, dipeptidyl peptidase; HbA1c, glycated hemoglobin; HIPPA, Health Insurance Privacy and Portability Act; M, measurement; PCP, primary care provider; Yr, year.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through a contract between the University of Maryland Baltimore and WellDoc, and by study-related contributions to the University of Maryland Baltimore from CareFirst Blue Cross/Blue Shield of Maryland, LifeScan, and Sprint. Additional funding was provided by the University of Maryland’s Maryland Industrial Partnerships Program, an initiative of the A. James Clark School of Engineering’s Maryland Technology Enterprise Institute. The funders of the study did not contribute to the design and conduct of the study, or to the collection, management, analysis, and interpretation of the data. They also did not contribute to the preparation of the article, except that WellDoc contributed to the description of the software coaching system that it provided. WellDoc did not have veto power over, or a say in, any other article text. Dr. Ram Miller served as the Data Safety Monitoring Board.