
Abstract
Background:
Mobile health (mHealth) technology that addresses diabetes mellitus in pregnancy has the potential to improve maternal and child health while diminishing socioeconomic and racial disparities. Little is known about health literacy, electronic health literacy, or patient characteristics that contribute to increased mHealth use. In this pilot study, we aimed to examine patient factors associated with user engagement with a novel app for diabetes support during pregnancy.
Method:
Low-income pregnant individuals with gestational or type 2 diabetes mellitus were recruited for a 2-week usability assessment of a novel mHealth smartphone application, “SweetMama,” designed to improve diabetes care. This analysis of user characteristics was a pilot assessment of data from the usability study phase. Participants completed assessments of patient health literacy, electronic health literacy, diabetes self-efficacy, and activation. User metrics (eg, sessions and total duration of use) were evaluated by participant characteristics. Descriptive analyses were conducted to assess outcomes with respect to patient’s clinical history, health literacy, electronic health literacy, diabetes self-efficacy, and activation.
Results:
Twenty-two diverse, low-income pregnant patients with either gestational or type 2 diabetes engaged with SweetMama for 14 days. Participants with gestational diabetes had greater mean minutes of use per session and mean total duration of use than those with type 2 diabetes. Participants with greater electronic health literacy, lower patient activation, and greater self-efficacy demonstrated greater total duration of use. No user metrics differed significantly by participant general health literacy.
Conclusions:
Findings of this pilot study suggest engagement with a novel mHealth app for diabetes support during pregnancy varied by baseline behavioral and clinical characteristics. Results could indicate that digital health literacy better differentiates engagement patterns than general health literacy.
Keywords
Introduction
Gestational diabetes mellitus (GDM) and type 2 diabetes mellitus (T2DM) affect over 7% of pregnant individuals in the United States (US), incurring significant individual, medical, financial and societal costs. 1 This burden disproportionately falls on low-income people and people of color relative to their higher income and white peers.2-4 Interventions that address diabetes mellitus in pregnancy can improve maternal and child health while diminishing socioeconomic and racial disparities.5-7 In addition to nutrition therapy and medication, management of diabetes during pregnancy involves patient education, behavior change support, patient activation, and ability to navigate barriers to health.8,9 Despite the prevalence and consequences of GDM and T2DM during pregnancy, few interventions have successfully supported pregnant individuals with diabetes care and self-management to reduce potential complications of diabetes and improve overall health.8,9
Mobile health (“mHealth”) tools, commonly referred to as smartphone applications, that connect individuals with tailored health resources and represent a promising means to impact behavior change and improve health.9-11 As over 70% of low-income adults in the United States have a smartphone, interactive “apps” have the potential to equitably equip pregnant individuals with health tools. 12 New, innovative, technology-forward approaches to health promotion are relatively low cost and accessible to pregnant people along the socioeconomic continuum.8,11 Increasingly, researchers have developed mHealth tools specifically targeted at improving health outcomes in pregnancy with mixed results. 10 Only a few phone applications focus on diabetes in pregnancy,13,14 and none have yet designed their interface to engage low-income populations and integrate with the U.S. health system. 10 These mHealth applications coordinate complex care, provide tools and organization systems to address health needs, monitor health metrics, and provide feedback as patients manage their diabetes over time.15,16
However, the existence of a high-quality app is insufficient to result in health improvement; the success of these programs depends on digital connectivity, 17 application adoption, and educational retention. Furthermore, the potential of such interventions to reduce disparities may only be realized if implementation accounts for barriers that uniquely impact disenfranchised communities. 18 Interventions implemented without attention to equity, usability, and user preferences can inadvertently widen the racial and socioeconomic healthcare and outcome gaps, especially when their use in marginalized communities is not investigated. 19
Understanding patient behavior and patterns of mHealth intervention engagement is foundational to successful implementation of mHealth interventions and optimally applying behavior change theory for maternal diabetes management and to ensuring that mHealth interventions reduce health inequities. As a component of a pilot-phase usability trial, we aimed to examine patient factors associated with use of a novel smartphone app for diabetes support and health modification during pregnancy.
Methods
Objectives
In this analysis of data from a small pilot study designed to explore to explore mHealth adoption, we aimed to examine baseline clinical and behavioral characteristics associated with engagement in the personal use of a novel diabetes mHealth application “SweetMama.” The overarching goal of the SweetMama study is to improve T2DM and GDM self-management and health care, thereby aiming to improve diabetes-related health outcomes for low-income pregnant individuals.15,16,20
Population
We enrolled low-income pregnant individuals with GDM or T2DM in this pilot phase investigation between February 2019 and August 2019. This analysis was one component of a multiphase usability evaluation of the SweetMama application.15,16,20 The study was conducted within 3 academic obstetrics and gynecology practices at a large tertiary care center. The target sample size was 20 participants based on the goals of usability research, in which the goals are to obtain sufficient user experience with the novel intervention in order to adapt it successfully for future longitudinal and more in-depth investigation. Written informed consent was obtained from all participants prior to participation and the study was approved by the Northwestern Institutional Review Board.
Eligible participants were pregnant individuals who were age 18 and greater, English-speaking, low income (ie, public insurance or household income <200% of the poverty line), and smartphone owners (with access to WIFI). All individuals had either GDM (ie, a diagnosis of glucose intolerance first recognized in pregnancy) or a T2DM diagnosed pre-pregnancy. As this phase of investigation was focused on assessing characteristics associated with SweetMama adoption and use, rather than clinical outcomes, individuals at all gestational ages were eligible for inclusion once an intrauterine pregnancy was confirmed.
Intervention
SweetMama is a smartphone application designed to provide pregnant individuals with educational, motivational, and goal-setting content on diet, exercise, medication management, glucose monitoring, behavioral coaching, motivation, and other health behaviors to support DM management during pregnancy. A combination of behavior change theory, obstetric diabetes literature, and expert experience informed app development and content. Behavior change theory as it relates mHealth supports the effectiveness of customizable features like favoriting, a dynamic library of information, goal setting support, technical support, instructional videos, and appointment reminders, all of which were incorporated into SweetMama.21,22 Each feature allowed participants to interact with, save, and iterate on their preferred SweetMama content.
In addition to providing regular delivery of content, the intervention provides appointment reminders, recipes, support for logistical details (such as local food resources), and a library of educational materials, including digital versions of the health education materials that are provided in counseling sessions at in-person appointments. Content is delivered via messages tailored to gestational age, sent three or more times per week, and with the ability to interact with content to obtain more in-depth information, as well as a static repository of health library information. The application also provides goal-based messages customized to the user with accompanying graphics and multiple mechanisms for users to interact with goal messages. All participants were provided a standardized orientation, video instructional resources, and contact information for technical difficulties. The SweetMama features followed key principles of behavior change including acceptability of use, goal setting with real-time feedback, and multifaceted, diverse behavior change techniques such as customizability and tailored content. In aggregate, the content aimed to facilitate an individualized connection between the participants and SweetMama and engender self-efficacy and motivation for sustainable behavior change, while also promoting the development of a scalable clinical tool.21,22
All participants were enrolled to use SweetMama on their own Apple or Android-based phones for 14 days.
Metrics and Outcomes
Upon enrollment, we collected participant demographic, clinical, and behavioral characteristics. Participants completed baseline surveys to evaluate:
General health literacy, defined as the ability to obtain and process health information (NVS: Newest Vital Sign);23-25
Electronic health literacy, defined as computer literacy as related to health information (eHEALS: eHealth Literacy Scale); 26
Diabetes self-efficacy, defined as the psychosocial self-efficacy of individuals with diabetes (DES-SF: Diabetes Empowerment Scale–Short Form);27,28
Patient activation, defined as patient engagement in the healthcare process (PAM: Patient Activation Measure). 29
Participants were also informed that their usage of SweetMama would be recorded. Use of the application was collected via monitoring each user interaction with the app, including all log-ins, viewed messages, and clicked links or library information. Outcomes included user metrics such as application sessions (ie, number of separate log-ins), mean number of minutes of use per session, days of actual use during the study period, and total duration of use (minutes). User metrics were collected in real time as participants used the application through the online SweetMama research platform.
Analysis
Descriptive analyses were conducted to assess outcomes with respect to patient’s clinical history, eHEALS, NVS, DES-SF, and PAM scores. Although trends were assessed, p-values were not calculated given the small sample size and preliminary nature of the data.
Results
Participants
Of 24 total participants consented to participate in this small-scale pilot to explore to explore mHealth adoption (Table 1), 22 participants provided user metrics during their 14-day usability trial. The average age of participants was 32.1 years (± 5.3) and a majority of participants represented diverse self-identified racial and ethnic backgrounds (45.8% black, 37.5% Latinx, 16.7% white). A majority (62.5%) had publicly-funded prenatal care and most (79.2%) did not have a college degree. Half of participants had GDM and the other half T2DM.
SweetMama Participant Demographics.
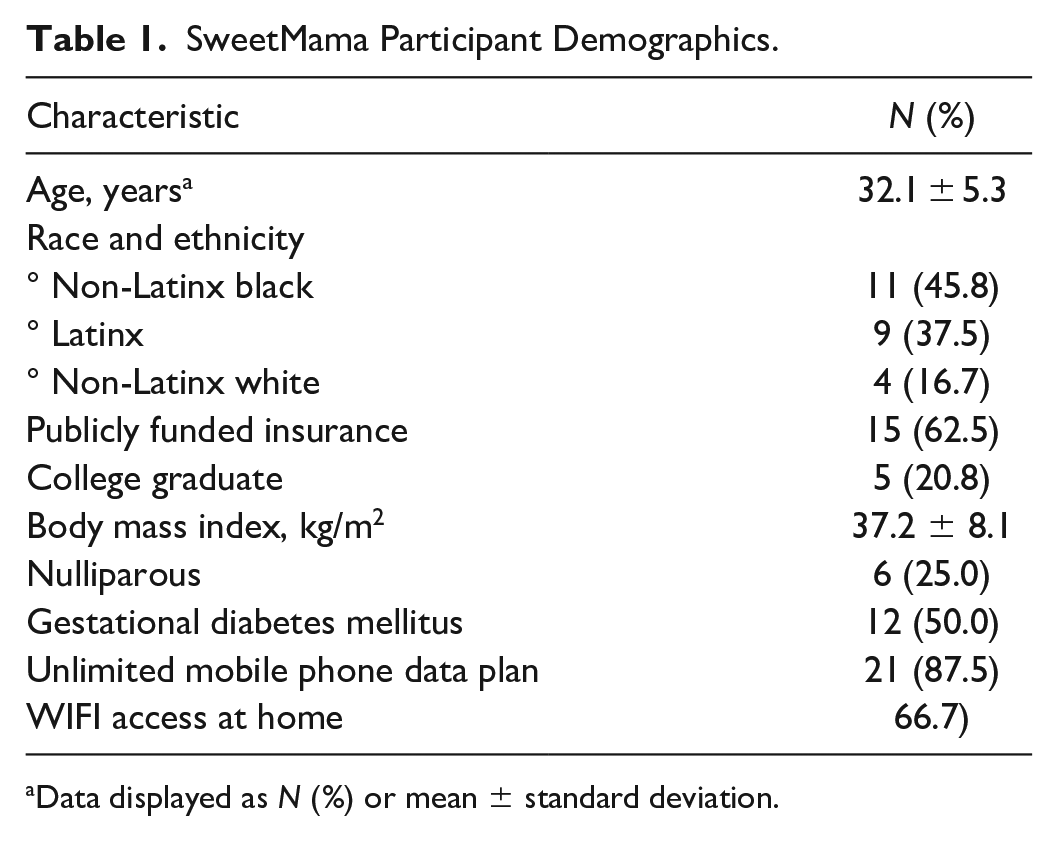
Data displayed as N (%) or mean ± standard deviation.
Participants with GDM had greater mean number of minutes of use per session (4.0 ± 2.9 vs 2.5 ± 0.9 minutes) and mean total duration of use (28.1 ± 17.0 vs 18.2 ± 12.3 minutes) than participants with T2DM (Table 2). No difference was seen between participants with GDM and those with T2DM with respect to days of actual use (approximately 12 days median use for both). Participants with GDM differed from those with T2DM with regards in their behavioral characteristics. Participants with GDM trended towards greater eHEALS scores (median 87.50 [IQR 82.50, 100.00] vs 82.50 [IQR 70.00 vs 100.00]), but were more likely to have a low diabetes self-efficacy score (54.6% vs 36.4%) than those with T2DM. Health literacy trends were similar, with a greater proportion of participants with GDM having inadequate general health literacy (54.6% among GDM and 36.4% among T2DM with inadequate health literacy). Patient activation was similar by diabetes type (81.8% among GDM and 90.0% among T2DM with highest-level activation).
Trends in Use of a Novel Health Tool During Pregnancy by Patient Behavioral Characteristics and Diabetes Type.
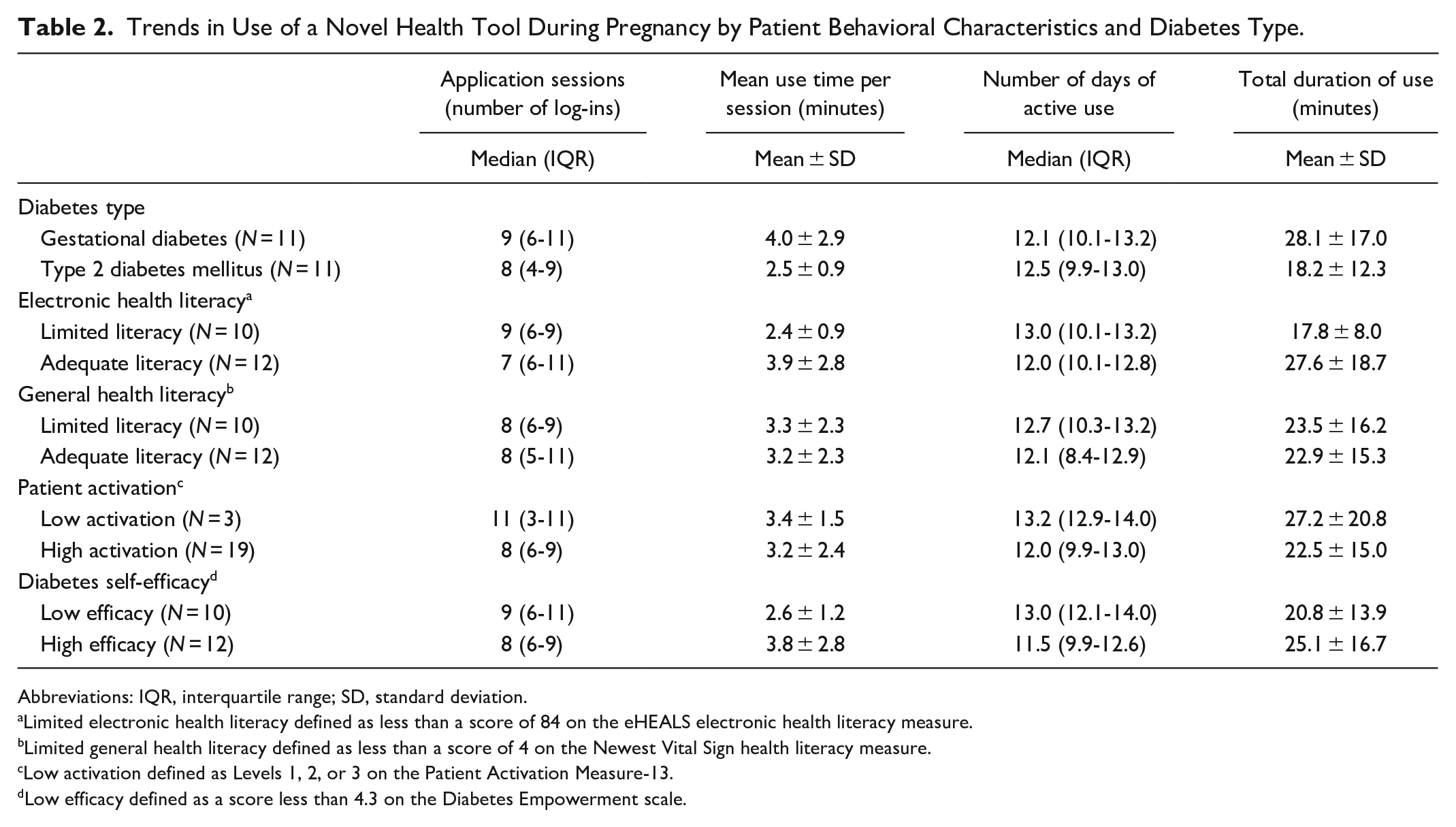
Abbreviations: IQR, interquartile range; SD, standard deviation.
Limited electronic health literacy defined as less than a score of 84 on the eHEALS electronic health literacy measure.
Limited general health literacy defined as less than a score of 4 on the Newest Vital Sign health literacy measure.
Low activation defined as Levels 1, 2, or 3 on the Patient Activation Measure-13.
Low efficacy defined as a score less than 4.3 on the Diabetes Empowerment scale.
The median eHEALS score for all participantss was 83.75 (interquartile range (IQR) 76.25-100.00), indicating overall high facility with electronic health resources. Although individuals with electronic health literacy above the median trended towards fewer days using SweetMama and fewer sessions, their overall duration of use was on average nearly 10 minutes longer than those with low electronic health literacy. In contrast to electronic health literacy, no user metrics differed significantly by participant general health literacy.
Participants with low-level patient activation (defined as Levels 1, 2, or 3 on the PAM) had more frequent sessions (median 11 [IQR 3-11] vs 8 [IQR 6-9]) and greater number of days of use (median 13.2 [IQR 12.9-14.0] vs 12.0 [IQR 9.9-13.0]). Additionally, they trended towards greater duration of overall SweetMama use compared to their high-level activation counterparts.
The median DES score for participants was 4.37 out of 8.00 (IQR 4.00-4.88), indicating moderate diabetes self-efficacy. Although those with higher self-efficacy tended towards fewer days of SweetMama use, each of their sessions had a longer duration and their overall time on SweetMama was nearly 5 minutes longer on average.
Discussion
Early-phase findings in this pilot study demonstrate that use of a novel mHealth app for diabetes support during pregnancy may vary by diabetes disease type and baseline behavioral characteristics. We note that in this diverse population, individual use patterns also varied by electronic health literacy and patient activation, which is considered a reflection of motivation and engagement in health care. Individuals with greater diabetes self-efficacy had greater overall use of the intervention. Interestingly, individuals with lower patient activation demonstrated slightly greater use of this novel intervention, suggesting this population may be particularly more likely to benefit from interventions such as SweetMama.
Our results suggest that electronic health literacy may be more informative than general health literacy in predicting application engagement. An increasing body of literature differentiates between general and electronic health literacy, and calls for greater evaluation of the role of electronic health literacy, especially as it pertains to health equity. 18 Electronic health literacy incorporates many of the principles of general health literacy, but additionally covers access to and effective engagement with digital health tools like SweetMama. It comprises a crucial component of Digital Connectivity, the ability and capacity of individuals to engage with digital health platforms like SweetMama. 17 Previous studies have raised concerns that disparities in electronic health literacy will fall along similar axes to those in general health literacy, disproportionately limiting access to and the utility of digital resources for low income and minority communities. 19 Although the literature supports high mobile technology use among these populations especially in reproductive years, attention to access disparities and technology gaps will be critical to ensuring equity. SweetMama differs from previous mHealth applications for pregnancy with several unique features including tailoring for low-income and largely minority users, the inclusion of tools that address social determinants of health, and the use of behavioral theories to guide goal achievement.10,15,16 Additionally, it differs from other applications in that it was designed to be a scalable adjunct to clinical care, rather than a digital tool for communication of glucose results, which exists in many extant commercial products and are commonly not tailored to the needs of low-income users. We aimed to improve electronic health literacy as specifically related to SweetMama by providing individualized, interactive orientations to the application as well as an introductory video. However, despite this orientation to SweetMama, we still found that use patterns appear to vary by electronic health literacy.
Our preliminary results demonstrated potential differences between those with GDM and T2DM both in their baseline characteristics and in their SweetMama use. These differences in SweetMama use may reflect the different baseline characteristics of pregnant individuals affected by GDM vs T2DM. Given the novelty of a diabetes diagnosis to individuals with GDM, these findings may also point to the importance of interventions that capture patients around their time of diagnosis, when they may be most motivated to participate in behavior change activities and interact with mHealth. It is possible individuals with T2DM experience intervention fatigue and a different framework of behavior change would better serve their needs, while also capitalizing on the enhanced engagement and activation that occurs with pregnancy and the postpartum period. 30 Qualitative literature demonstrates that pregnant people with GDM trust information provided through mHealth tools and have specific preferences regarding application content. 31 Similar qualitative examinations of pregnant patients with T2DM could inform more effective mHealth tools. Mixed-methods research that incorporates information about pregnant patients with both GDM and T2DM, like this study, will play a critical role in supporting them through a safe pregnancy and improving their diabetes control.
Digital inclusion, a framework for implementing and evaluating electronic health tools, connects technology, access, equity and justice. 32 Achieving digital inclusion necessitates an understanding of the electronic health literacy of underrepresented populations and the factors that impact their technology engagement To reach and improve health practice of all patients, the nuances of behavior change theory in mHealth as it applies to diverse populations and different characteristic phenotypes will need to be explored. This bears particular relevance to pregnant individuals, who are often neglected in research and health intervention development, 33 and who may particularly experience the consequences of the digital divide. Our finding of the relative importance of electronic health literacy offers new insight into a technology use for a unique, understudied population and may contribute to digital inclusion for pregnant patients with diabetes. Future research will need to focus on how to enhance electronic health literacy and address digital connectivity in pregnancy, a crucial window for health interventions.
Although low patient activation is generally thought to be indicative of low engagement in healthcare, individuals in this study with low activation actually had greater engagement with SweetMama, suggesting a potential key role for mHealth interventions in supporting patient care. It is possible that individuals with low activation engage differently with digital tools than with other resources in the healthcare ecosystem. These differences reinforce the importance of principles such as flexibility, customizability, and tailored content that are inherent in behavior change theory and critical to effective diabetes interventions.21,22 Given those with low activation may also experience differences in diabetes-related perinatal outcomes, digital connectivity may represent an important and novel mechanism to their improve health outcomes. Determining how behavior change theory and app development applies to individuals of different baseline characteristics and those typically marginalized by health systems could present a meaningful area of future study. Further studies are needed to investigate how mHealth tools impact the health of low activation patients and others who have been disengaged with traditional health resources.
This study has several limitations. This small pilot phase was designed as a preliminary investigation of usability with a small sample size. Although trends in the findings may present an interesting starting point for further investigation, findings must be interpreted with caution and replicated in larger studies. Significance testing could not be completed due to this small sample size, and thus the data represent hypothesis-generating exploratory findings on this topic. In addition, as these data were generated during a usability assessment of SweetMama that was designed to be 14 days, the exposure of participants to SweetMama was short. The results therefore cannot be generalized to long-term effects and may reflect a novelty period or a time during which participant had only begun familiarizing themselves with SweetMama. Future work will need to explore whether these use patterns persist over the duration of pregnancy. Limitations with the study tools and metrics have been described previously and apply to this study.23-29
Conclusion
To ensure smartphone applications for the support of diabetes-related health benefit all users, those with baseline characteristics associated with less intervention engagement may need additional support and resources. Although the study sample size is small, this initial experience with a novel intervention could critically inform how apps such as SweetMama or other interventions targeting similar populations are distributed and implemented. The study focuses on a historically disenfranchised population and contributes to a larger effort to improve digital inclusion. The benefit of mHealth applications depends, in part, on an iterative development process that accounts for differences between users and optimizes application features and ancillary support such that the product maximizes impact.
Footnotes
Abbreviations
DES-SF, Diabetes Empowerment Scale–Short Form; eHEALS, eHealth Literacy Scale; GDM, gestational diabetes mellitus; IQR, interquartile range; mHealth, mobile health; NVS, Newest Vital Sign; PAM, Patient Activation Measure; T2DM, type 2 diabetes mellitus; US, United States.
Authors’ Note
Presented at the 41st Annual meeting of the Society for Maternal-Fetal Medicine (virtual, January 2021) as a poster presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NICHD R21 HD094271 and the Friends of Prentice FY2019 Women’s Health Grants Initiative. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.