
Abstract
Background:
School-aged children often participate in type 1 diabetes (T1D) self-care tasks. Despite widespread discussion about the importance of developing self-care skills in childhood, few explain how the health care team should assess the skills of children with T1D when performing insulin injections.
Objective:
We sought to assess content validity evidence in two checklists regarding injection technique performed by children.
Methods:
Two checklists were designed based on a systematic review of the insulin injection technique. Experts in pediatric diabetes, health literacy, and diabetes education assessed the checklists regarding their clarity, objectivity, and relevance. Content validity was assessed using the content validity ratio (CVR).
Results:
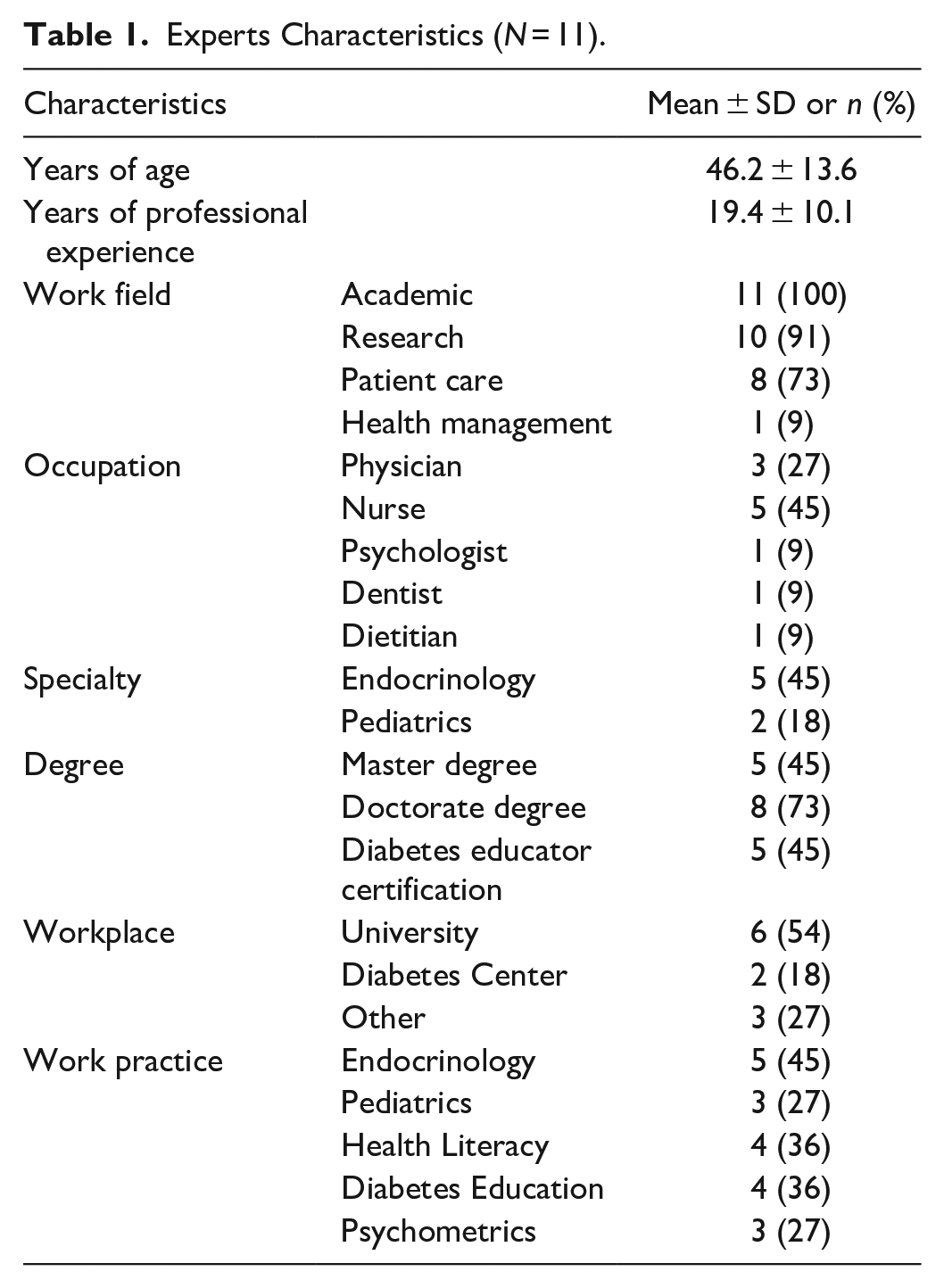
Eleven providers (72% nurses or physicians, professional experience 19.4 ± 10.1 years, 45% of specialists in endocrinology, and 18% in pediatrics) participated in the assessment. Experts considered items containing the word homogeneity inappropriate. Items related to the needle insertion angle and the skin fold did not reach the CVR critical value. The final version of the checklist for syringe injection comprised 22 items with CVR = 0.91, and the checklist for pen injection comprised 18 items with CVR = 0.87.
Conclusions:
The checklists presented clear, objective, and relevant content that assesses the skills of children with T1D for insulin injection. The checklists formally present the order of the technique and all the steps for insulin injection and allow a quantitative assessment of the operational skills of children. The developed instruments offer providers the possibility of continuous assessment of the progress of the pediatric clientele until they reach independence in diabetes self-care.
Introduction
For more than 25 years, the prescription of intensive regimens which consist of at least three insulin injections per day has been considered the gold standard in type 1 diabetes (T1D) management. 1 However, intensive treatment can be a major challenge for the clinical care of children with diabetes. First, because injection administration is related to emotional factors such as fear and anxiety, it can occasionally make the self-injection difficult for young people.2,3 Second, because insulin administration is a high-risk procedure due to insulin being a high-alert medication, meaning it can cause serious harm if misused. These errors can occur at any stage in the process of medication use; however, most of them occur in the administration of the injection.4,5 Thus, it is important to teach the correct steps for performing an insulin injection safely, enabling young people to perform injections independently and effectively.6,7
It is crucial to recognize which steps in the technique the child knows and masters, as well as those that need support and supervision until they reach a higher age, ensuring excellent clinical care focused on the specific needs of the pediatric population. The subcutaneous injection technique is described in guidelines set forth by various diabetes organizations,8-10 in literature reviews,11-13 as well as in recommendations from pediatric specialists.6,14
In search of evidence-based recommendations, experts from 54 countries summarized the results of a systematic review of the subcutaneous insulin injection technique to provide a new, practical, and comprehensive set of guidelines for patients and practitioners throughout the world. These recommendations include the particularities of the injection technique in the pediatric population and guide worldwide actions on insulin injections. 12
Although expert consensus highlights the uniqueness that differentiates children injections from adult injections, there are no recommendations as to which technique steps should be delegated to the child nor at what age the health care provider can introduce new concepts and expect complex steps to be taken by the youth. Experts from the American Diabetes Association propose a division of priorities in the management of T1D, according to young people’s developmental stage, which indicates school age as the opportune phase for stimulating cognitive skills and flexibility in the insulin regimen that may lead to more injections per day. 15
Given the importance of assessing diabetes self-care skills, several instruments are available to measure adolescent and adult diabetes self-management practices.16-18 However, to our knowledge, there are no instruments available for self-care assessment in children with T1D with regard to their skills for administering insulin injections. Thus, this study aimed to develop and validate two checklists on the syringe and pen injection technique to assess the skills of children with T1D.
Methods
Design
This is a psychometric study that sought evidence of the content validity of two checklist instruments. This type of instrument is used when the order of steps is important for performing a task. In the health context, checklists are mainly employed during a sterile procedure, which does not allow the substitution of one step for another. 19 Both checklists are observer report instruments that, through direct observation of the procedure, aim to measure the skills of children with T1D during a subcutaneous insulin injection.
Study reporting was consistent with the EQUATOR guidelines, using the STrengthening the Reporting of OBservational studies in Epidemiology, the STROBE checklist (Supplementary File). The study was approved by the Research Ethics Committee of a public university under report no. 313/2017.
Developing the Initial Pool of Items and the Response Scale
The checklists were developed for clinical use by health care professionals who evaluate and oversee the competency of insulin injection technique performed by children with T1D. Therefore, providers and educators can use the checklists as a method for data collection based on direct observation of the insulin injection procedure. Children’s performance assessed by the injection checklists may be considered a quantitative data helpful in setting up goals for diabetes educational sessions.
For the construction of instrument items, all information described in the consensus of experts 12 regarding the injection technique with syringe and insulin pen were included. In order to divide the technique into steps, the checklist items were organized into three domains: preparation procedures, application procedures, and finishing procedures. The first version of the syringe checklist contained 24 items, and the pen checklist contained 20 items, which included steps on injecting only one type of insulin.
The response scale was built with yes, no, and not applicable options. The not applicable option is justified by the fact that an injection technique can be modified according to the material available and the indication of its use. For example, keeping the insulin vials or the insulin pen at room temperature or refrigerated after opening is optional, provided that the local temperature does not exceed 30 °C (86 °F). The injection using a 4 mm needle does not require skin fold; however, it is known that many children only have access to needles longer than 4 mm. 20
Panel of Experts’ Selection
Content validity indicates that items of an instrument were selected from a systematic sampling after the assessment of experts in the field—the expert panel. 21
The potential panelists were selected in August 2018, after consulting a Brazilian researchers’ database—Plataforma Lattes (https://www.lattes.cnpq.br) and Google Scholar Citations (https://scholar.google.com/citations), by subject, on the basis of doctors and other researchers according to their academic background/degree.
Professionals who educate children on T1D self-care, health literacy specialists, and specialists in psychometrics experienced in developing measuring instruments were invited. Eight professional specialists in T1D, 15 health literacy specialists, and six psychometrists were approached by invitation letter via e-mail. The invitation letter explained the purpose of participating in the study and contained a Uniform Resource Locator link that directed them to the Survey Monkey Online platform. Through this platform, potential participants had access to the consent form and, upon accepting to participate in the research, completed a characterization questionnaire constructed by the first author and previously evaluated by a psychometrist (FR) and two pediatric nurses (ROLB and WAA) members of the research team. Responses were anonymous, and in order to have the records included for analysis, all sections of the online assessment needed to be complete.
Content Validity
To search for content validity of the checklists, a brief explanation of insulin injection recommendations that guided the construction of the items were provided to the expert panel. Next, the preliminary versions of the checklists were presented, and the experts evaluated all items of both instruments for its relevance, objectivity, and clarity according to the following definitions:
Relevance: The checklist item concerns the subject. The item is related to the child’s performance regarding the insulin injection technique.
Objectivity: The checklist item achieves what it is intended to achieve, and it is objective.
Clarity: The checklist item is clear. It is intelligibly expressed, or it is easily understood.
Other aspects evaluated about the content of the instruments, called general aspects, included format and clarity of the response scale, adequacy of the language used, number of items in each instrument, and whether the instrument measures what it intends to measure. Finally, an open-ended question asked the expert to make a general assessment of the checklists.
Statistical Analysis
Expert panel characterization data were analyzed using means, SDs of continuous variables, and frequencies of categorical variables.
The content validity of checklists was assessed using the content validity ratio (CVR).22,23 The formula for CVR calculation is CVR = (Ne – N/2)/(N/2), where Ne is the number of experts that indicates “I agree” option and N is the total number of experts. Thus, we calculated the CVR of the items in each checklist (CVR-I), as well as the total CVR of the instrument (CVR-S). The CVR-S demonstrates the validity of the entire scale, and it is based on the average CVR values found per item. In addition, by using the CVR we aimed at reducing the risk of bias related to the expert panel size since the CVR critical value depends on the number of experts included.23,24 Moreover, the CVR is a strong psychometric tool able to provide the best content validity assessment. 25
Results
Thirteen professionals assessed the checklists in September and October 2018. Two professionals were excluded for not completing the full evaluation. The characteristics of the 11 participating experts are presented in Table 1. The checklist assessment completion lasted about 45 minutes.
Experts Characteristics (N = 11).
The critical value established for cut-off was 0.63, which is in line with the number of panelists. 26 The evaluation of the general aspects of the instruments presented CVR = 0.90 for the syringe checklist and 0.86 for the pen checklist. Tables 2 and 3 show all checklist items and CVR-I values. The highlighted values correspond to items that did not reach the critical value in the CVR-I calculation.
Checklist for Insulin Syringe Injection: Content Assessment per Item.
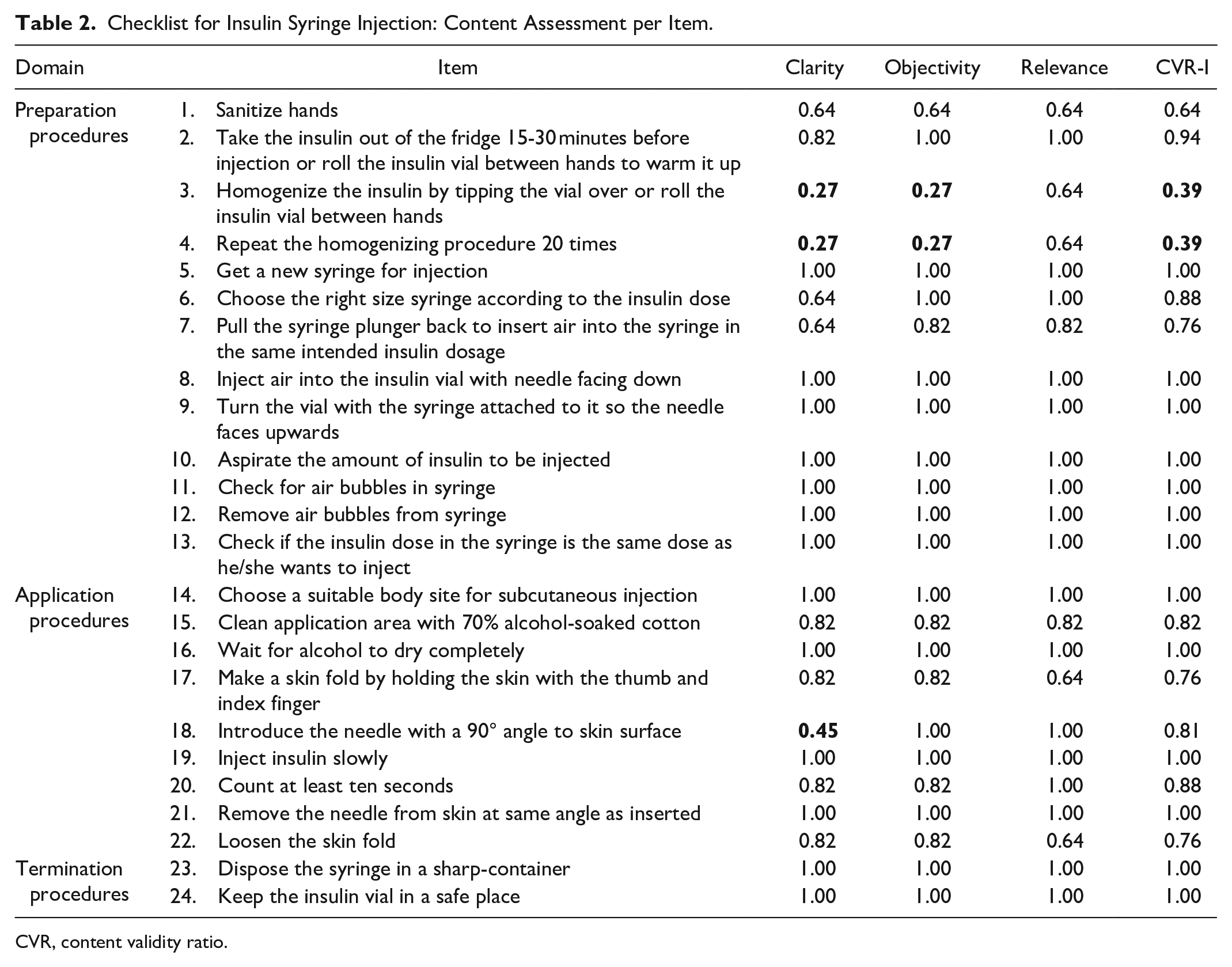
CVR, content validity ratio.
Checklist for Insulin Pen Injection: Content Assessment per Item.
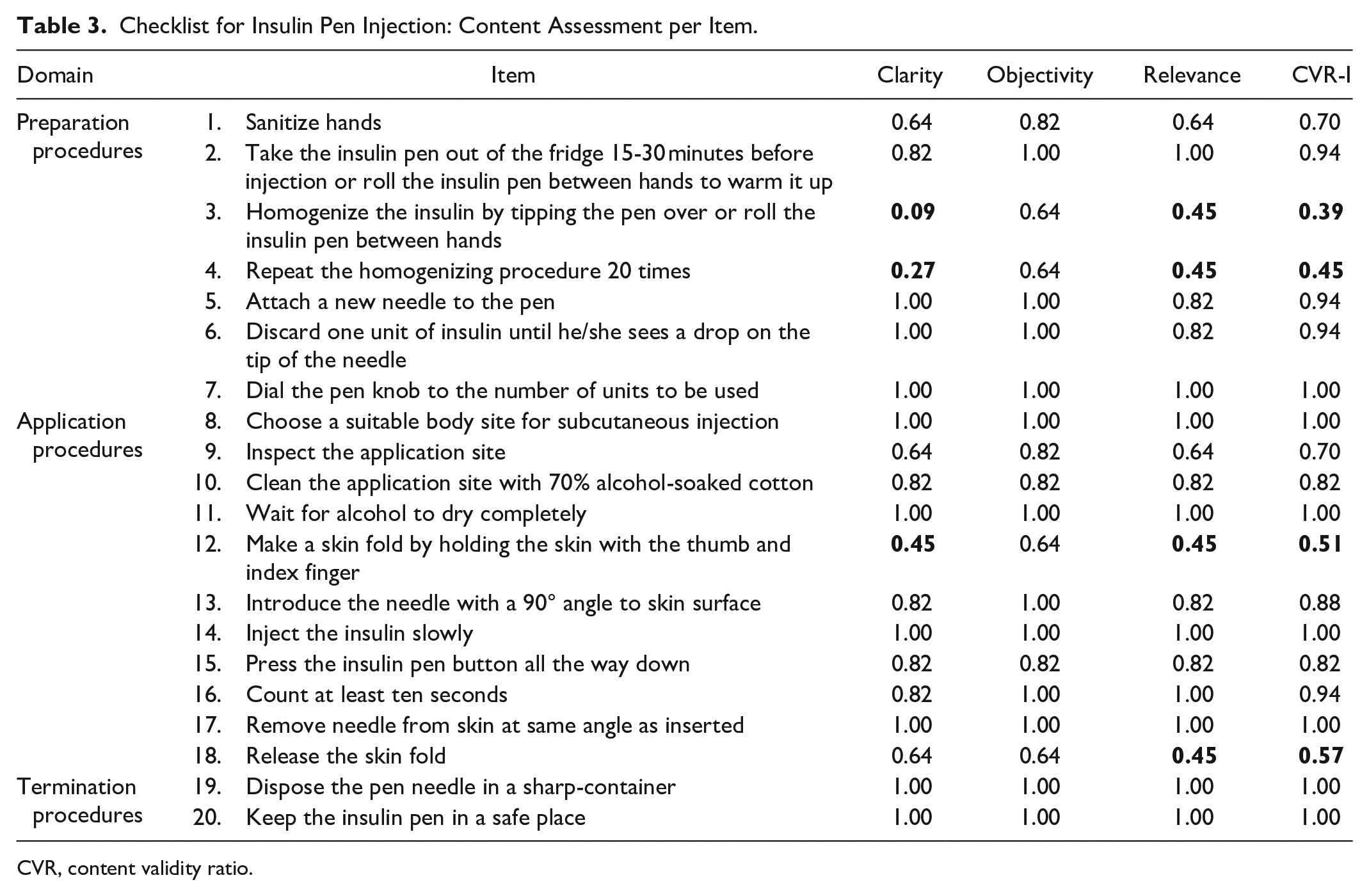
CVR, content validity ratio.
The checklist items that contained the word homogeneity were considered inappropriate by the experts, as it is a word that is difficult to understand. The other items that did not reach the critical value referred to two particularities of the injection technique: the needle insertion angle and the skin fold. In these, the specialists pointed out that performing the insertion angle and the skin fold depends on the size of the needle used and, therefore, should be considered only when the child uses needles longer than 4 mm. Thus, these items were kept in the final version of the checklists because the response scale allows the provider to check as “not applicable” when there is no need for injection angulation or skinfold.
As items containing the word homogenization were considered inadequate in both checklist assessments, they were removed from the instruments. In addition, the homogenization procedure is indicated only when using NPH insulin, which has a higher risk for hypoglycemia, weight gain, and poorer glycemic control, when compared with insulin analogs of a prolonged or intermediate acting profile. 9 In this sense, we understand that NPH is an outdated insulin for T1D treatment. Therefore, the final version of the checklists did not include the items regarding the homogenization procedure.
The answers to the open question revealed that the experts considered the instruments appropriate, with potential for clinical evaluation of the insulin injection technique due to the adequate description of the items. As weaknesses, they indicated the language used in the wording of the items such as the word “homogenize,” as well as the impossibility of evaluating the syringe injection technique using pre-mixed insulin. The comments below exemplify the findings of the open question inserted in the online assessment:
I found the arrangement of both instruments very good. Because they are children, I think the idea of [the answer scale] being yes, no and not applicable can work better. (Expert 2)
Both checklists address the proposed objective, being important only to review the points placed in the observations. I understand that the most common issues were considered, and I think it is important that these points are discussed by the researchers (Expert 6)
The instrument will be very useful for health care teams, but it should be adapted to the actual use of insulin and other suggested details. (Expert 11)
After removing items 3 and 4 from the preliminary version of both checklists, the CVR-S was calculated. Both checklists had CVR-S values above the critical value of 0.63 (Table 4).
CVR-S According to the Type of Content Assessment Performed.
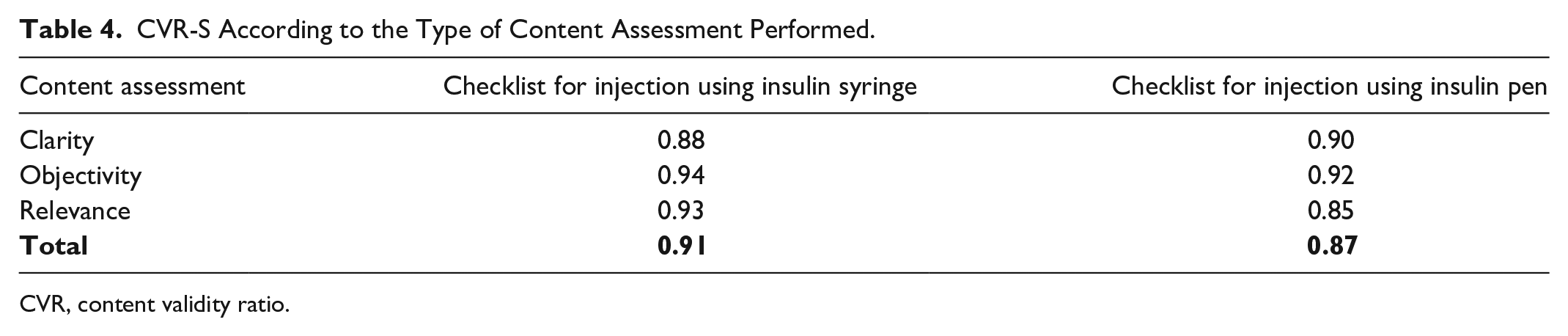
CVR, content validity ratio.
The final versions of the syringe checklist and the pen checklist are in the Appendices of this article and were revised by three nurses (ROLB, WAA, and LCN) and one psychometric expert (FR) member of the research team.
The total checklist score should be calculated by the formula N/(n – NA) × 100, in which N is the sum of items marked as yes, n is the number of checklist items, and NA is the total number of items considered as not applicable. When using the checklists, the provider must evaluate in advance how many items will be scored as NA, which will vary according to the available material, and then observe the child performing the injection. The final calculation will result in a score of 0-100 on each checklist, in which the higher scores indicate a child’s greater ability to perform the insulin injection technique.
Discussion
The assessment of skills for administration of insulin via injection of children with T1D by the multidisciplinary team is critical, especially by nurses who are professionals with expertise in injections and health education. 27 Prior studies presented proposals for assessing the knowledge of young people with diabetes about insulin dosage 28 or their knowledge about the preparation and application of insulin. 29 Therefore, this is the first proposal of a syringe and a pen injection checklist, whose content will enable providers and diabetes educators to assess the skills of school-aged children with type 1 diabetes on self-injections.
In this study, the expert panel that evaluated the checklists was composed of a majority of nurses, as well as medical, psychometric, and nutrition professionals. The multidisciplinary composition of the panel of experts ensured a comprehensive technical assessment, similar to other tools used for diabetes self-care assessment.16-18 The qualification of the panelists showed a high educational level. The various areas of expertise and reported experience of over 5 years ensured the checklists were evaluated by professionals with different backgrounds and work experience. These characteristics guarantee the methodological rigor in validation studies, especially those used for clinical assessment. 30
With regard to the item selection, the authors followed the recommendations of a systematic review and organized each checklist into three domains. The CVR-I results show that the items presented what they intended to measure and were clear and objective, except for those concerning insulin homogenization. The option to remove this step from the final version of the checklists limits the use of these instruments for insulin types that do not require homogenization. It is evident that advances in insulin therapy have led to the growing use of insulin analogs in pediatric diabetes management. However, insulin analogs are substantially expensive and scarce in low-income resource countries.31-33 Thus, the development of instruments that evaluate the insulin injection technique that requires homogenization is a gap to be addressed in future research.
Another aspect highlighted in the evaluation of the specialists that deserves attention is keeping the not applicable option in the response scale, indicated by the experts as fundamental due to the difficulties in accessing the appropriate material. A response scale in a clinical assessment instrument must include clear options for the professional who will use it. In this case, the evaluation of the insulin injection technique will depend on what is shown by the child and on other factors, such as the needles and syringes available and the professional’s own control over the procedure.34,35
In the overall content evaluation, measured in this study by CVR-S, both checklists obtained excellent evaluation, which affirms the relevance of the instruments for clinical practice. The answers to the open-ended question reinforce the importance of the syringe and the pen injection checklists in assessing the skills of children with T1D, benefiting the evidence-based practice.
Limitations and Strengths
There are some limitations to this study. First, the expert panel was composed of Brazilian professionals with expertise in instrument development, pediatrics, and diabetes. Ultimately, both checklists need to be tested within other Portuguese speaking settings to confirm its cross-cultural validity. Nonetheless, aspects that demonstrate methodological rigor to the instruments proposed in this study need to be highlighted, primarily due to the use of a strong content validity index such as the CVR. The checklists formally present the order of the technique and all the steps for insulin injection, previously described in guidelines and literature reviews in different ways, which may lead to differences in procedure accuracy. In addition, the checklists allow a quantitative assessment of the operational ability of children with T1D, offering providers the possibility of continuous assessment of the progress of this clientele until they reach independence in self-care. This study, therefore, favors diabetes care and education specialists’ practices regarding teaching, research, and care for children with T1D.
Implications for Practice
Correct training on insulin injection technique is crucial. It is possible to find patients who have never received formal instruction from their health care providers on injection technique, even after many years of insulin therapy. 36 Thus, the validation of instruments that formalize and order the steps of insulin injection, such as checklists, encourages a commitment to optimize injection practices and to assess a child’s ability as early as possible.
It is important to highlight that measurement tools such as the developed injection checklists do not replace clinical judgment and experience. The diabetes care and education specialists must use the checklist findings as a complement to the various clinical assessments performed during the encounter. By using the checklists to assess pediatric skills on injection technique, providers may quantify what steps in injection self-care need require training and education, along with advice on site care, injection site rotation, alleviation of pain, and psychological approach to managing pediatric patients. 20 By using an instrument with satisfactory content validity, the child’s health is preserved, and complications are avoided. 37
Conclusion
The syringe injection checklist and insulin pen injection checklist were assessed as relevant, clear, and objective. Both checklists were considered by the expert panel as potential instruments for assessing the operational skills of children with T1D. Therefore, the checklists are suitable as a one-time screening tool or can be used with a given individual longitudinally to monitor changes in their proficiency and assess the needs for potential training and education over time.
Supplemental Material
sj-pdf-1-dst-10.1177_1932296820984771 – Supplemental material for Checklists for Assessing Skills of Children With Type 1 Diabetes on Insulin Injection Technique
Supplemental material, sj-pdf-1-dst-10.1177_1932296820984771 for Checklists for Assessing Skills of Children With Type 1 Diabetes on Insulin Injection Technique by Rebecca Ortiz La Banca, Flávio Rebustini, Willyane A. Alvarenga, Emilia C. de Carvalho, Mayara Lopes, Kerry Milaszewski and Lucila C. Nascimento in Journal of Diabetes Science and Technology
Footnotes
Appendix
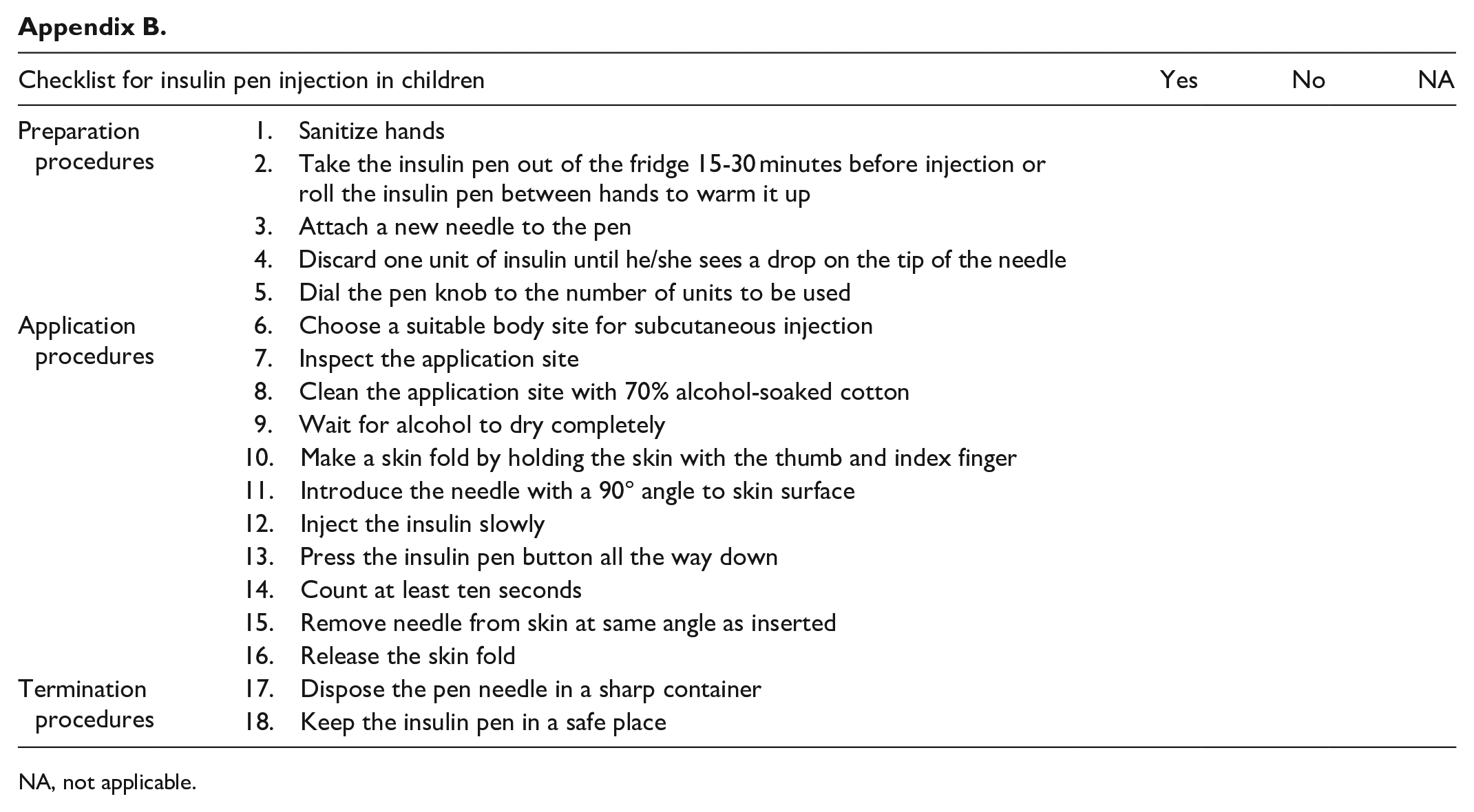
| Checklist for insulin pen injection in children | Yes | No | NA | |
|---|---|---|---|---|
| Preparation procedures | 1. Sanitize hands | |||
| 2. Take the insulin pen out of the fridge 15-30 minutes before injection or roll the insulin pen between hands to warm it up | ||||
| 3. Attach a new needle to the pen | ||||
| 4. Discard one unit of insulin until he/she sees a drop on the tip of the needle | ||||
| 5. Dial the pen knob to the number of units to be used | ||||
| Application procedures | 6. Choose a suitable body site for subcutaneous injection | |||
| 7. Inspect the application site | ||||
| 8. Clean the application site with 70% alcohol-soaked cotton | ||||
| 9. Wait for alcohol to dry completely | ||||
| 10. Make a skin fold by holding the skin with the thumb and index finger | ||||
| 11. Introduce the needle with a 90° angle to skin surface | ||||
| 12. Inject the insulin slowly | ||||
| 13. Press the insulin pen button all the way down | ||||
| 14. Count at least ten seconds | ||||
| 15. Remove needle from skin at same angle as inserted | ||||
| 16. Release the skin fold | ||||
| Termination procedures | 17. Dispose the pen needle in a sharp container | |||
| 18. Keep the insulin pen in a safe place | ||||
NA, not applicable.
Abbreviations
CVR, Content Validity Ratio; T1D, Type 1 Diabetes.
Authors’ Note
Portions of this article were presented as an abstract at the 22nd Brazilian Diabetes Society Congress in 2019, Natal, RN, Brazil.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CAPES Foundation within the Ministry of Education, Brazil - Finance Code 001 and partially by a Mary K. Iacocca Research Fellowship provided by the Iacocca Family Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.